
Abstract
Introduction:
Domestic violence against women (DVAW) is a global health issue, particularly in areas with patriarchal norms and a lack of culturally relevant assessment tools. We developed a culturally adapted questionnaire to measure community attitudes toward DVAW in Saudi Arabia.
Methods:
We conducted a cross-sectional study involving expert review, exploratory factor analysis (EFA), and assessments of internal consistency. The study included a convenience sample of 831 adult participants, comprising 417 males and 414 females.
Results:
The adapted instrument showed excellent psychometric properties (Cronbach’s alpha = 0.93) and strong validity across demographic groups. Although excluding acceptance-oriented items narrowed the conceptual scope, the remaining items effectively measure key dimensions of DVAW rejection, reflecting community attitudes and their mental health implications.
Discussion:
This reliable instrument measures community attitudes toward DVAW. Future work may explore cognitive neuroscience methods to study attitude change and the long-term effects of culturally adapted interventions on mental health.
Introduction
Domestic violence against women (DVAW) is a pervasive global health concern and a profound violation of human rights. Women experience physical or sexual violence in their lifetime, with prevalence estimates reaching 31% in the Eastern Mediterranean Region, surpassing the global average of 27% (Sardinha et al., 2022). DVAW encompasses physical, sexual, and psychological harm, as well as coercion, threats, and the deprivation of liberty, and may occur in private or public domains (Office of the High Commissioner for Human Rights [OHCHR], 1993). Its consequences are extensive, ranging from physical injuries and chronic pain to mental health conditions, including depression, posttraumatic stress disorder (PTSD), and substance use disorders (Wessells & Kostelny, 2022). DVAW is further associated with long-term sequelae such as reproductive health complications, suicidality, and elevated risk of homicide perpetrated by intimate partners, who account for 38% to 50% of female homicides worldwide (Stöckl et al., 2013). Children exposed to DVAW may also suffer immediate and enduring adverse health outcomes, perpetuating intergenerational cycles of violence (Jewkes & Machisa, 2024). Moreover, established links between DVAW and infant morbidity and mortality underscore its far-reaching public health implications (Sardinha et al., 2022; World Health Organization [WHO], 2021).
A complex interplay of individual, relational, community, and societal factors underpins the perpetration of DVAW (Stockman et al., 2015). Individual-level contributors include childhood trauma, substance misuse, mental health disorders, and lower educational attainment, while relational factors may encompass marital dissatisfaction or infidelity (Mazza et al., 2021). Socioeconomic determinants, such as poverty and unemployment, further compound vulnerability (Yakubovich et al., 2018). Critically, entrenched cultural norms and patriarchal traditions often elevate men’s status over women, exclude women from decision-making, and justify violence as a means of control, thereby reinforcing harmful attitudes that normalize DVAW (McKinley et al., 2021; UN Women, 2023). Multiple studies estimated that DVAW in Saudi Arabia ranged between 34%-43%(Alquaiz et al., 2017; Fageeh, 2014; Sinha et al., 2012). Enhanced female decision-making power has been shown to reduce the likelihood of abuse, illustrating the pivotal role of societal and cultural structures in shaping these outcomes (Manna et al., 2024).
Cultural beliefs and collective social norms are thus central in either perpetuating or challenging violence against women (Childress et al., 2023; Lomazzi, 2023). Attitudes toward DVAW can be broadly categorized as acceptance or rejection, in which acceptance by victims or the wider community contributes to normalization, increased perpetration, and justification (Gracia et al., 2020; Karlsson et al., 2022). Against this backdrop, social norms theory provides a robust conceptual foundation for understanding these attitudinal dynamics. This theory suggests that individuals’ perceptions of what is considered acceptable or normative within their reference group shape their own beliefs and behaviors (Bicchieri, 2017; Cialdini et al., 1991). When applied to DVAW, such norms can either entrench acceptance and justification or promote widespread condemnation and intervention (Berkowitz et al., 2022; Jewkes et al., 2015).
Anchoring the current study in Social Norms Theory acknowledges that attitudes toward DVAW emerge from complex interplays of cultural traditions, power disparities, and communal values rather than being confined to individual predispositions. Attitudes and social norms, as central constructs in this study, are underpinned by cognitive and emotional processes that align with cognitive neuroscience principles. Understanding these processes is vital for designing effective, culturally adapted interventions. This framework thereby guides the interpretation of the findings and informs the design of culturally sensitive, community-driven interventions aimed at shifting harmful norms—an approach endorsed by the WHO and international human rights bodies committed to eliminating violence against women (Office of the High Commissioner for Human Rights [OHCHR],1993; WHO, 2009).
Although numerous studies have highlighted the complexity of DVAW and its multifaceted determinants, few have developed validated, culturally relevant instruments to measure community attitudes toward this violence (Copp et al., 2019; Pérez-Vázquez & Bonilla-Campos, 2023; Villanueva-Blasco et al., 2024). Often derived from Western populations, existing scales may lack cross-cultural applicability or fail to undergo rigorous psychometric evaluation. This gap hinders the development of robust, evidence-based strategies tailored to specific cultural environments, such as those in Arab-majority countries.
In alignment with global initiatives, including the WHO’s call for region-specific instruments and the United Nations Sustainable Development Goal 5 to eliminate all forms of violence against women, this study aimed to develop and psychometrically validate a culturally adapted tool to measure attitudes toward DVAW in Saudi Arabia. Recognizing the sensitivity and potential challenges inherent in capturing the acceptance and justification of violence, we employed a theory-informed process to ensure the instrument’s cultural relevance and methodological soundness. This developed measure can serve as a valuable resource for Arab researchers and public health professionals, informing community-level interventions, facilitating cross-cultural comparisons, and ultimately contributing to reducing DVAW through context-specific, evidence-based strategies. Hence, the current study aimed to develop a culturally adapted questionnaire to measure community attitudes toward DVAW in Saudi Arabia.
Method
Ethical Considerations
Expedited approval of the study was obtained from the University Research Center’s institutional review board (IRB number: H-01-R-005) before data collection. Research assistants explained the purpose and nature of the study privately to each potential participant to obtain their written informed consent. The investigators took all measures to ensure confidentiality and the voluntary nature of participation, adhering to ethical standards in research involving human participants. The researchers used anonymous self-administered written surveys to protect participant confidentiality and anonymity. The consent form was placed on the survey’s first page. Participants completed surveys, folded their response sheets, and put them in a locked box. Completed surveys were transferred to the university research facility and placed in a safe, locked cabinet. Every survey had a unique research code, and the data were fed to a computer secured with a password. To minimize social desirability bias, participants completed the surveys anonymously. Furthermore, the investigators used indirect questioning techniques and neutral phrasing to reduce the likelihood of socially biased responses. Where necessary, trained research assistants provided reading support to participants who were unable to read or write, but they were instructed not to influence responses. All questionnaires were self-administered in a private setting to promote privacy and confidentiality.
Study Design
The study utilized psychometric analysis and a cross-sectional approach aimed at developing and validating a culturally adapted instrument for assessing attitudes toward domestic violence against women (DVAW) in Saudi Arabia. The current study asks the following research question: What is the reliability and validity of the DVAW scale across diverse participants’ demographics? The methodological approach adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines to ensure transparency, rigor, and reproducibility (von Elm et al., 2007).
Sample
We planned to recruit a minimum of 1,000 participants to achieve construct validity for the DVAW attitude questionnaire, guided by Comrey and Lee’s criteria (100 = poor, 200 = medium, 300 = good, 500 = very good, ≥1,000 = excellent) (Comrey & Lee, 2013). Participants included Saudi men and women aged 18 years or older, recruited through convenience sampling. No restrictions were placed on participants’ socioeconomic or educational backgrounds. To enable subgroup analyses, participants were stratified by gender, age, education, and living standards. Of the 2,000 questionnaires distributed, 1,100 were returned, and 831 were deemed complete and included in the analysis, yielding a response rate of 55% (Table 1).
Socio-Demographic Characteristics of the Participants.
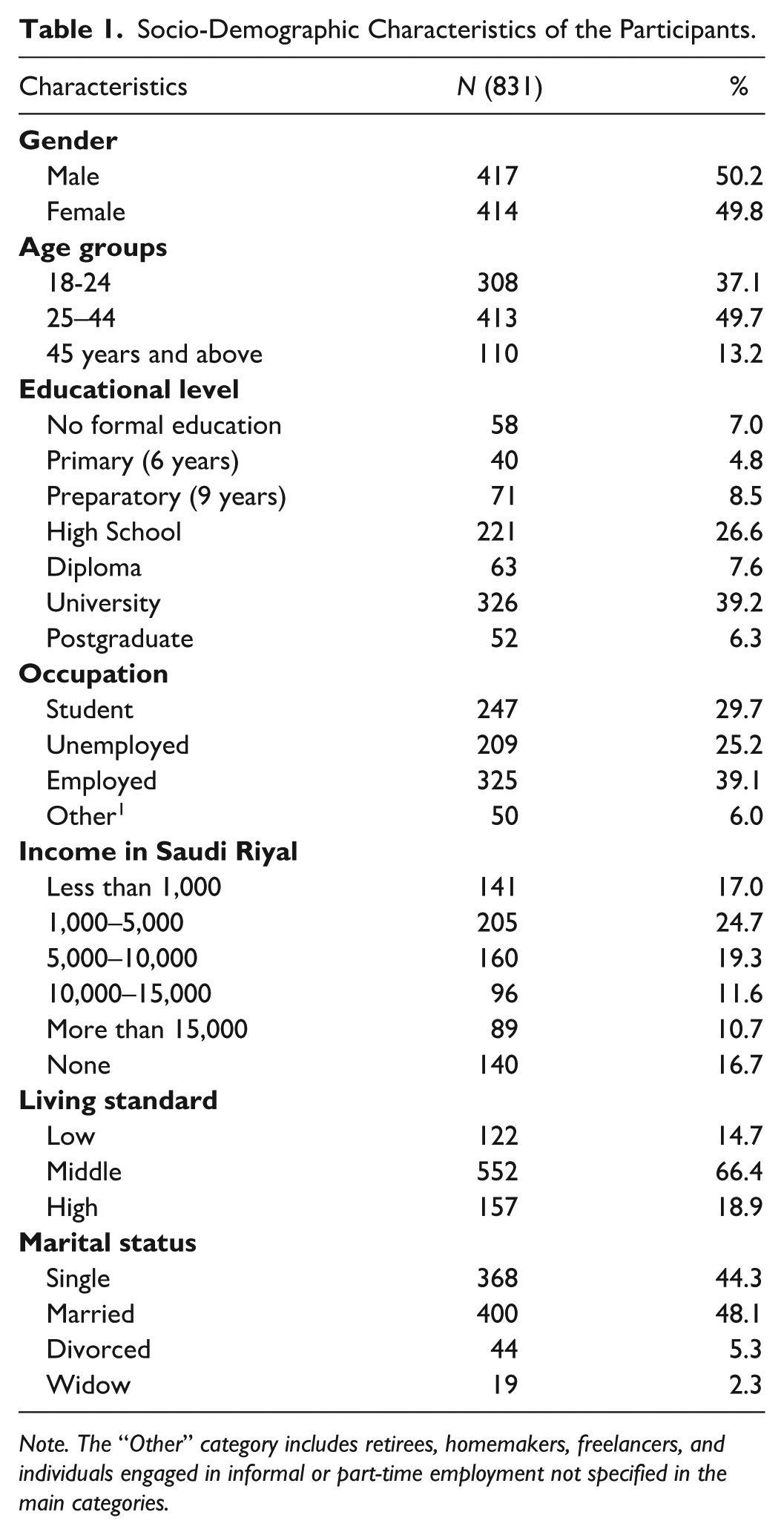
Note. The “Other” category includes retirees, homemakers, freelancers, and individuals engaged in informal or part-time employment not specified in the main categories.
Recruitment and Data Collection
Research assistants collected the data during health promotion campaigns in public venues such as shopping malls, markets, and parks. These campaigns offered health screenings (e.g., measurement of body mass index, blood glucose, and blood pressure) and distributed educational materials on chronic disease prevention and management. The research assistants introduced the study to the public using flyers and word of mouth. If participants agreed to participate, they were provided with the informed consent to sign and a hard copy of the survey to complete.
Questionnaire Development and Content Validation
The study employed a paper-based questionnaire comprising socio-demographic variables (gender, age, education, marital status, employment, income, and living standards) and items assessing attitudes toward DVAW. Tool development followed the guidelines described by Boateng et al. (2018). A thorough literature review informed the development of the initial nine-item DVAW attitude questionnaire, ensuring its relevance to Arab and Muslim communities and acknowledging that existing instruments were predominantly Western-centric (Fikree et al., 2005; Gracia et al., 2020). The nine items used a 3-point Likert-type scale (1 = disagree, 2 = neutral, 3 = agree). Items 1, 2, and 3 were revised based on expert feedback for improved clarity and cultural relevance. Items 1 (“Men have the right to practice violence against women”) and 2 (“Domestic violence against women is acceptable”) were reverse-scored (1 = agree, 2 = neutral, 3 = disagree) to ensure that agreement with these statements indicated acceptance of DVAW, opposite to the intended direction of the scale. Reverse scoring thus aligned all items so that higher overall scores reflected a greater rejection of DVAW, enhancing consistency and reducing response bias.
Five experts in the field of domestic violence against women from nursing (psychiatric and mental health and women’s health) and psychiatry disciplines evaluated the questionnaire for content validity, rating item relevance on a 4-point scale (1–4). Items rated 3 or 4 were considered relevant. Expert feedback prompted minor modifications to the wording of Items 1, 2, and 3, ensuring these statements accurately captured the nuances in attitudes toward DVAW. This process maintained the essential conceptual dimensions of acceptance versus rejection of violence.
Translation and Cultural Adaptation
The finalized English questionnaire underwent a systematic translation and cultural adaptation process following the Rome Foundation’s guidelines for scale translation, adaptation, and validation (Rome Foundation, 2021). Two bilingual medical translators (native Arabic speakers) independently conducted forward translations into Arabic. A bilingual researcher then reconciled the two Arabic versions. Subsequently, an independent professional bilingual medical translator (a native English speaker) performed a blind back-translation into English. A committee of translators and one researcher compared the original English and back-translated versions to ensure semantic, experiential, and conceptual equivalence, making minor adjustments to enhance cultural relevance and clarity.
Pilot Testing and Cognitive Debriefing
Before the main data collection, the Arabic version of the questionnaire was piloted with 30 Arabic-speaking individuals who were not included in the final sample. These participants provided feedback on item clarity, comprehension, and cultural sensitivity. Their input informed the further refinement of items 1, 2, and 3, ensuring the questionnaire was understandable and culturally appropriate. Following these adjustments, the final version of the DVAW attitude questionnaire was used for data collection.
Statistical Analysis
Continuous variables were summarized using means and standard deviations, while categorical variables were described using frequencies and percentages. Multivariate normality was assessed via Mardia’s tests for skewness and kurtosis, which indicated non-normality (Mardia’s kurtosis = 41.0, p < .001; Mardia’s skewness = 2,102.1, df = 165, p < .001). Potential multivariate outliers were examined using the Mahalanobis distance. To identify the latent structure of the nine-item scale assessing attitudes toward DVAW, we conducted a common factor analysis with iterated principal axis factoring (PAF). This approach is recommended when the assumption of multivariate normality is unmet (Watkins, 2018). Given the ordinal nature of the 3-point Likert-type responses, a polychoric correlation matrix was employed to provide more accurate estimates of the relationships among items. Bartlett’s test of sphericity confirmed that the correlation matrix was not an identity matrix (Bartlett, 1950), and sampling adequacy was ensured with the Kaiser–Meyer–Olkin (KMO) measure; KMO values >0.50 indicate sufficient common variance for factor analysis (Kaiser, 1970).
Exploratory factor analysis (EFA) criteria included the Kaiser criterion (eigenvalues >1), the percentage of total variance explained (≥60%), and the Scree test to determine factor retention. Given theoretical grounds that factors might be correlated, an oblimin rotation was applied. In social science research, latent constructs are often expected to correlate to some degree. Therefore, we chose oblimin rotation, which allows for correlated factors, as it aligns better with the theoretical expectation in our context (Watkins, 2018). Moreover, our preliminary analysis revealed non-negligible correlations among the extracted factors, justifying the use of an oblique rotation. The EFA supported a single-factor solution with high loadings on Items 4–9, and low loadings on Items 1–3. Consequently, Items 1–3—originally designed to measure acceptance or justification of DVAW—were excluded. The final six-item measure thus reflected community awareness, recognized risk factors, and the perceived need for intervention, rather than direct acceptance constructs.
To further evaluate the questionnaire’s robustness, subgroup analyses were performed by gender, age group, educational attainment, and living standards. Within each subgroup, Cronbach’s alpha values and EFAs were recalculated to assess internal consistency and factor stability, ensuring that the scale’s psychometric properties remained reliable and valid across diverse participant demographics. All statistical analyses were performed using R. The psych package (version 4.0.0) was used for the KMO test, Bartlett’s test, EFA, and Cronbach’s alpha estimations (R Core Team, 2020).
Results
Participant Characteristics
A total of 831 Saudi individuals participated in the study, with an equal representation of men and women. The majority (n = 721) were younger than 45 years, and approximately 80% (n = 662) had attained at least a high school education. Regarding employment, 29.7% were students, 39.1% were employed, and 25.2% were unemployed, while an additional 6.0% were categorized as “Other” (including retirees, homemakers, freelancers, and those engaged in informal or part-time work). More than half (58%, n = 485) reported a monthly income ≥5,000 SAR, and 85% (n = 709) had a living standard classified as middle or high. Detailed demographic characteristics are presented in Table 1.
DVAW Attitude Questionnaire Validity and Reliability
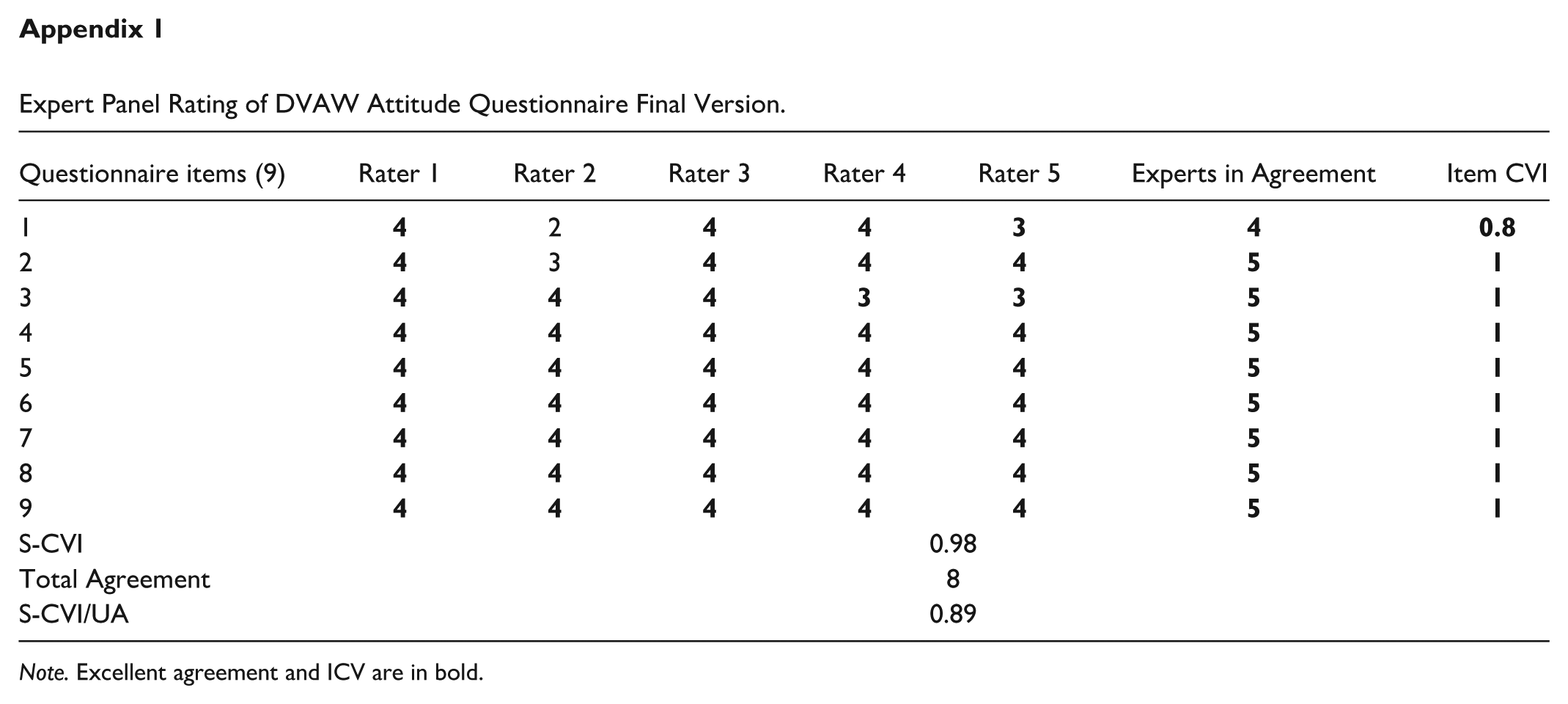
Content validity was assessed by calculating the Item Content Validity Index (I-CVI) and the Scale Content Validity Index (S-CVI). Each of the five experts rated item relevance on a 4-point scale. I-CVI values ranged from 0.8 to 1.0, indicating strong agreement among experts, and the overall S-CVI reached 0.98, with an S-CVI/Universal Agreement (S-CVI/UA) of 0.89 (Appendix 1). These results demonstrate excellent content validity. Based on expert feedback and cognitive debriefing, Items 1, 2, and 3 were refined to enhance clarity, cultural appropriateness, and conceptual integrity.
Table 2 summarizes the descriptive statistics for responses to the nine 3-point Likert-type items (1 = disagree, 2 = neutral, 3 = agree). Notably, 58.6% of respondents disagreed with the statement “Men have the right to practice violence against women” (Item 1), and 49.7% disagreed that “Domestic violence against women is acceptable” (Item 2). In contrast, 61.3% agreed that “Domestic violence is a common problem in Saudi society” (Item 3). Strong agreement was observed for items highlighting the role of child abuse as a risk factor (Item 4; 63.2%), the link between violent homes and violent citizens (Item 5; 64.7%), and the importance of raising community awareness (Item 6; 73.4%). Most participants acknowledged the need for help for perpetrators (Item 7; 70.4%), government involvement in addressing domestic violence (Item 8; 75.1%), and the religious prohibition of domestic violence against women (Item 9; 72.6%). Overall, these findings indicate that while direct acceptance of DVAW was relatively low, there was strong recognition of the problem’s prevalence, underlying risk factors, and the necessity for intervention, prevention, and authoritative action.
Descriptive Statistics of the Responses to DVAW Attitude Questionnaire.
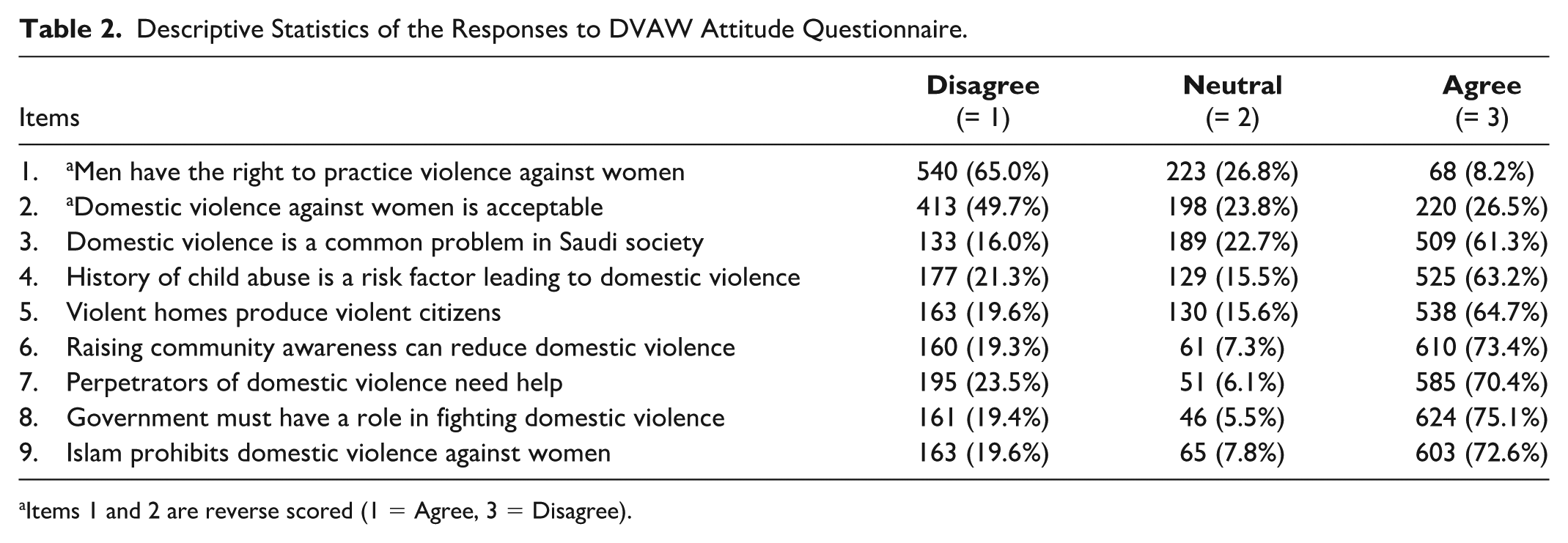
Items 1 and 2 are reverse scored (1 = Agree, 3 = Disagree).
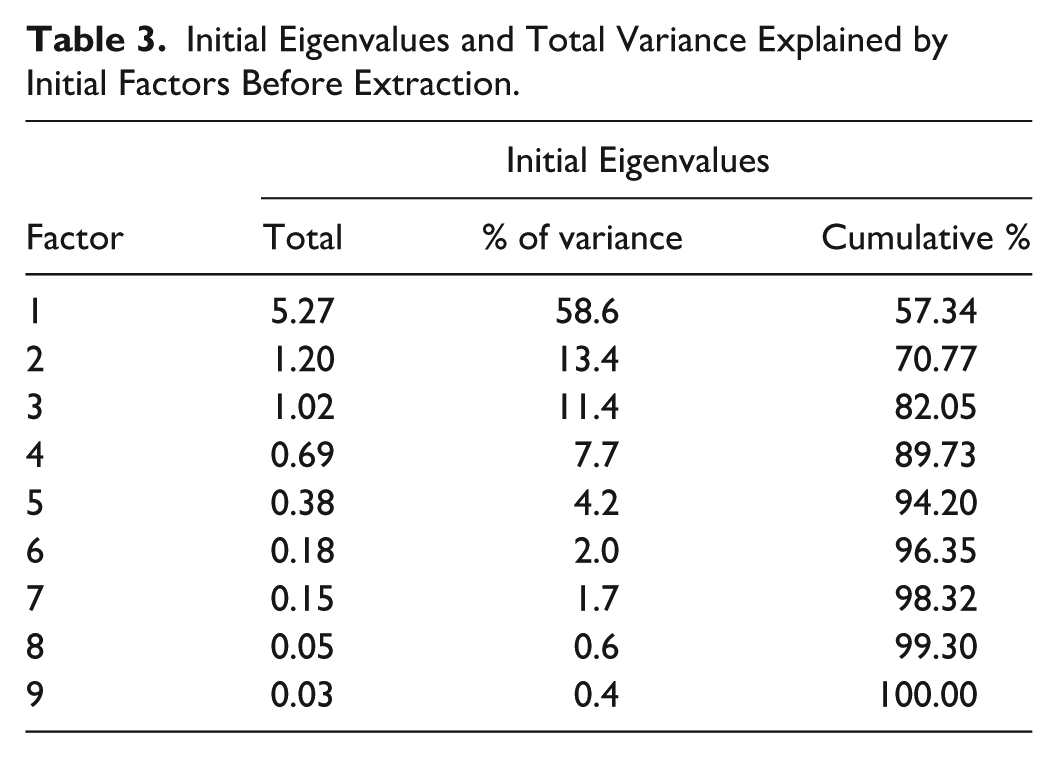
High inter-item correlations were observed among items 4–9, with Pearson’s r values ranging from 0.69 to 0.96 (Figure 1). All 831 respondents provided complete data on the nine-item DVAW attitude questionnaire. Using the Mahalanobis distance, 27 multivariate outliers were identified and excluded from subsequent factor analyses. Bartlett’s test of sphericity confirmed that the correlation matrix did not represent an identity matrix, χ2(36) = 7,382.0, p < .001. Sampling adequacy was supported by a KMO statistic of 0.87, exceeding the recommended minimum threshold for factor analysis. Accordingly, the data were deemed suitable for dimensionality reduction. The initial eigenvalues from the principal component analysis are presented in Table 3.
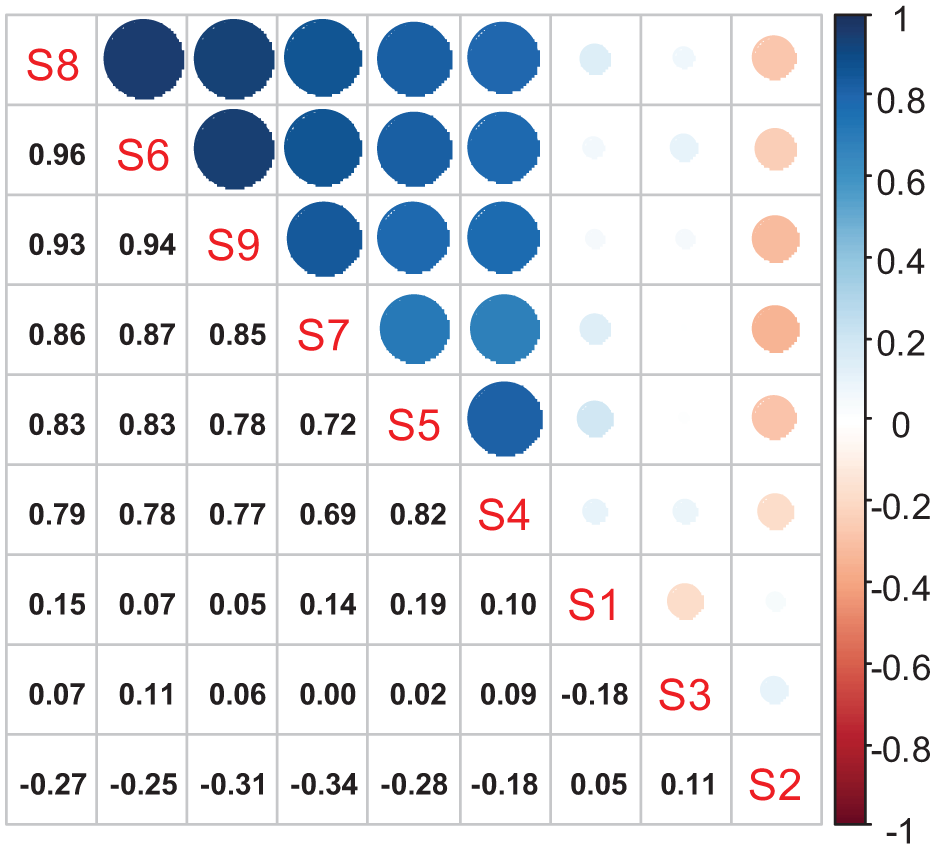
Polychoric Correlation Matrix.
Initial Eigenvalues and Total Variance Explained by Initial Factors Before Extraction.
Extraction of Factors and Item Reduction
Examination of the Scree plot (Figure 2) suggested a one-factor structure, as only a single component exceeded the breakpoint. Although the Kaiser criterion identified three factors with eigenvalues greater than one, the third factor’s eigenvalue barely surpassed this threshold. In addition, a variance-based criterion supported a two-factor solution, with two factors accounting for 70.77% of the total variance. To ensure a robust final model, we evaluated one-, two-, and three-factor solutions.
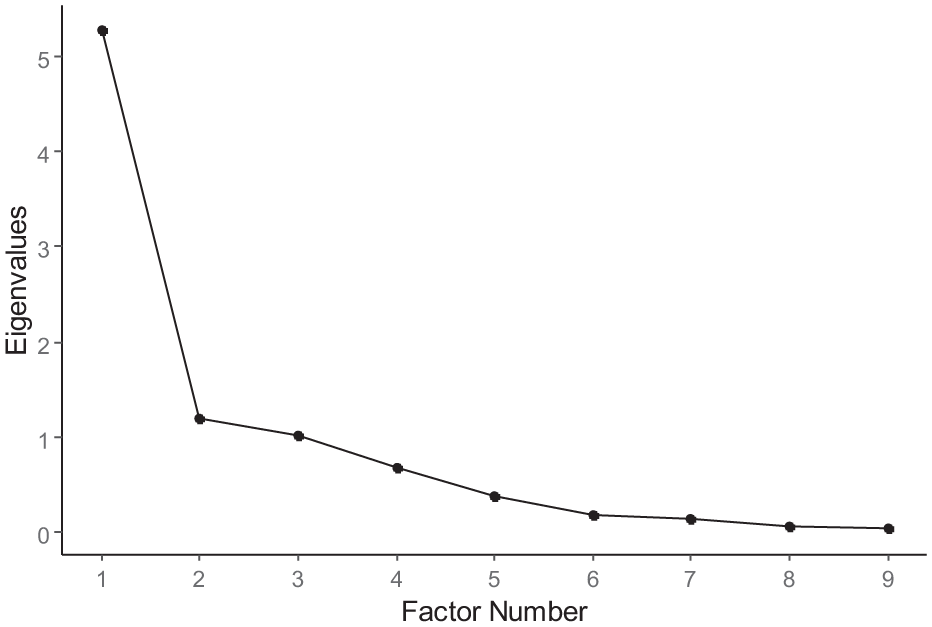
Scree Plot.
Table 4 presents the PAF results, including pattern coefficients and communalities, for each model. Across all solutions, Items 4–9 demonstrated strong loadings on the primary factor, with communalities ranging from 0.7 to 0.9, indicating that these items were well-explained by a single underlying latent dimension. In contrast, Items 1–3 performed inconsistently. Under the three-factor solution, Item 1 loaded only on the second factor, Item 2 on the third factor, and Item 3 showed weak, diffuse loadings across two factors. The two-factor model failed to adequately incorporate Items 1 and 2, and included only Item 3 in the second factor. In the one-factor model, none of Items 1–3 met the 0.4 loading criterion. These findings justified the removal of Items 1–3, which did not coherently align with the latent construct measured by Items 4–9. Retaining Items 4–9 produced a single-factor instrument that captured the core dimension of community attitudes toward DVAW.
Pattern Coefficients (Standardized Factors’ Loadings) and Items’ Communalities for 804 Participants on the Nine Items of the Domestic Violence Against Women Attitudes Questionnaire Using One-, Two-, and Three-Factors Solutions.
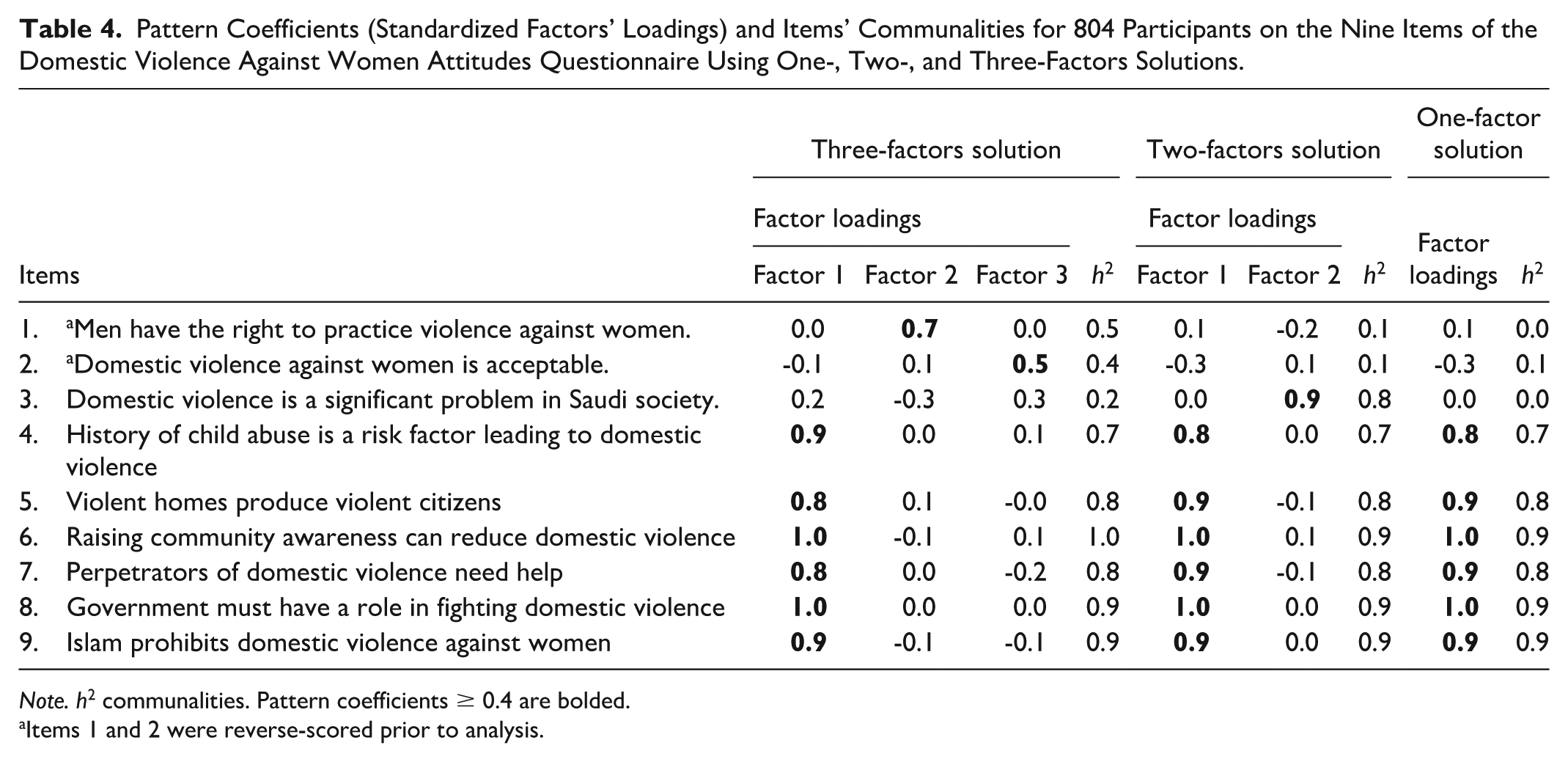
Note. h2 communalities. Pattern coefficients ≥ 0.4 are bolded.
Items 1 and 2 were reverse-scored prior to analysis.
Internal Consistency and Reliability
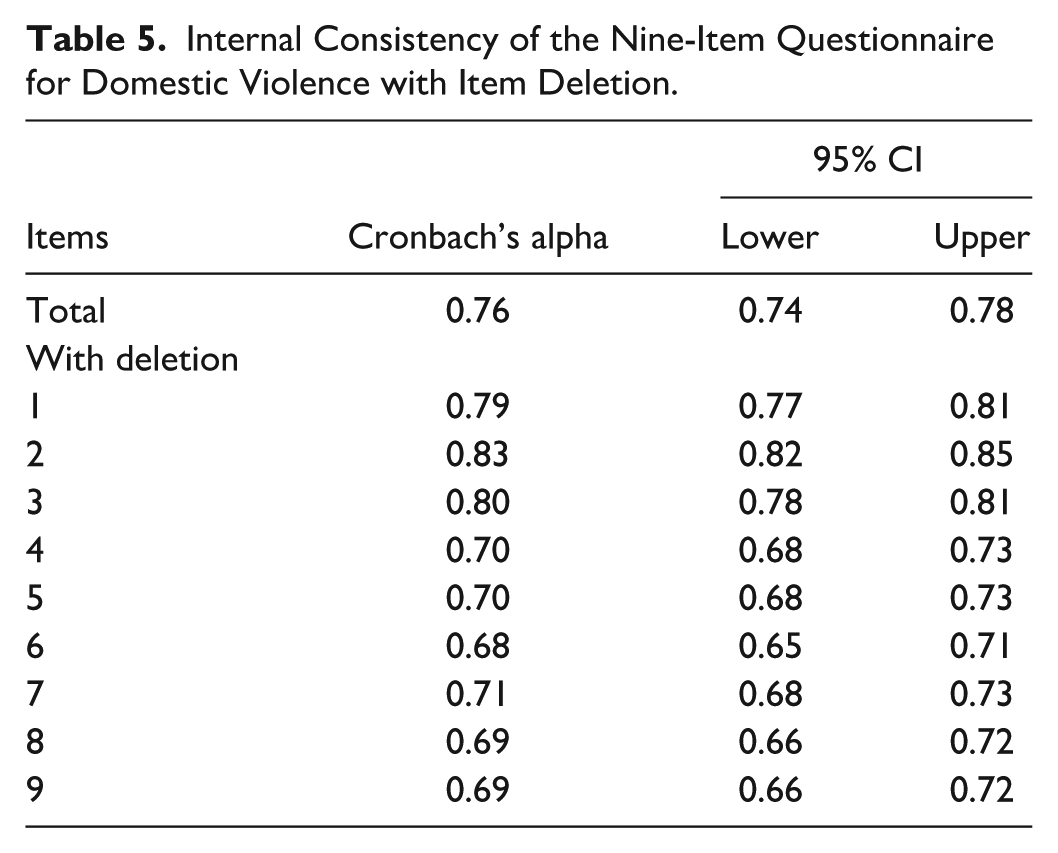
Table 5 summarizes the Cronbach’s alpha coefficients for the original nine-item questionnaire with and without individual item deletions. The overall alpha of .76 (95% CI: 0.74–0.78) indicates acceptable internal consistency. However, Items 1, 2, and 3 appear to diminish reliability; removing any one of these items increases the alpha to between 0.79 and 0.83, suggesting that they may not meaningfully contribute to the scale’s cohesion. In contrast, removal of any item from 4 to 9 reduces the alpha to values between 0.68 and 0.71, underscoring the integral role these items play in the instrument’s internal consistency. Focusing on Items 4–9 alone yields excellent reliability, with a Cronbach’s alpha of 0.93 (95% CI: 0.91–0.94). Thus, while Items 4–9 form a robust core reflecting the latent construct of interest, Items 1–3 warrant reconsideration for potential redundancy, suboptimal phrasing, or limited relevance.
Internal Consistency of the Nine-Item Questionnaire for Domestic Violence with Item Deletion.
Subgroup Analyses
Reliability and validity were further tested across various demographic strata. Cronbach’s alpha remained high within each subgroup, including males (0.91), females (0.93), those under 25 years (0.92), those aged 25–45 years (0.93), and those older than 45 years (0.90). Similarly, strong internal consistency was observed regardless of educational level (≥0.91) or living standards (≥0.90). Exploratory factor analyses conducted within each subgroup supported a single-factor model, confirming that the instrument’s structure and reliability remain stable across diverse participant characteristics.
Discussion
This study developed and validated a culturally sensitive instrument for assessing community attitudes toward domestic violence against women in Saudi Arabia, addressing a critical gap in the literature. By demonstrating strong psychometric properties—including high internal consistency (Cronbach’s alpha = 0.92) and a solid factor structure—the questionnaire emerges as a reliable and valid tool for measuring DVAW-related attitudes across diverse demographic subgroups.
Our findings concur with global research underscoring the profound influence of sociocultural norms on violence against women (Rodelli et al., 2022), which emphasized the role of entrenched social beliefs in perpetuating gender-based violence, and our instrument similarly captures core dimensions that contribute to DVAW, including the justification of violence and acceptance of male dominance. Unlike many Western-oriented scales, however, our tool engages with the unique cultural realities of Saudi Arabia, situating individual attitudes within the region’s specific social, religious, and familial contexts. This work also addresses the gaps highlighted by Badenes–Sastre’s study (Badenes-Sastre et al., 2024), which noted a lack of validated instruments in non-Western settings. By focusing on an underrepresented Arab and Muslim-majority context and incorporating culturally specific factors, the questionnaire extends the existing repertoire of DVAW assessment tools to environments where nuanced measurement approaches have been scarce (Elghossain et al., 2019). Beyond confirming the importance of cultural adaptation advocated by Haddad and colleagues (Haddad et al., 2011), our results reinforce the need for rigorous psychometric validation to ensure that instruments accurately reflect local norms and values.
Notably, Items 1 and 2—reverse-scored to mitigate response bias—showed lower factor loadings, underscoring the challenges of incorporating reverse-scored items in culturally sensitive scales. While reverse scoring can enhance methodological rigor, future work should refine these items to preserve their intended purpose (detecting acceptance of DVAW) without compromising clarity or cultural resonance. Comprehensive tools that account for subtle variations in attitudinal acceptance will remain essential for effective research and intervention design.
Theoretical Discussion
Informed by Social Norms Theory, our findings underscore the centrality of community standards and cultural traditions in shaping attitudes toward DVAW. This theoretical lens emphasizes that individual beliefs are not formed in isolation but rather emerge from shared perceptions of what is deemed acceptable within a given reference group (Bicchieri, 2017; Cialdini et al., 1991). The prominence of items reflecting community awareness, the recognition of violence as a collective problem, and the need for intervention align closely with the theory’s core tenets. Specifically, our results indicate that shifting communal norms—through awareness campaigns, educational programs, and culturally tailored interventions—may be a strategic pathway to reducing the acceptance of DVAW. The validated instrument captures cognitive dimensions such as beliefs and norms, and emotional dimensions like acceptance or rejection of violence. These constructs align with cognitive neuroscience research on how cultural and social factors shape decision-making and emotional regulation. By translating theoretical constructs into a validated, context-specific measure, the present study provides a robust foundation for designing interventions that challenge deeply ingrained norms, guide policy initiatives, and inform culturally sensitive nursing practice. Employing Social Norms Theory as a conceptual anchor thus reinforces the importance of engaging communities as active agents in reshaping attitudes, ultimately fostering environments where violence against women is neither tolerated nor normalized.
Strengths and Limitations
A key strength of this study is its rigorous cultural adaptation and psychometric validation. Using established methodologies and expert feedback, the instrument underwent multiple refinements, showing high internal consistency across demographic groups. The one-factor structure confirmed that items effectively captured essential dimensions of rejection toward DVAW, despite the removal of Items 1 and 2 due to low factor loadings. This removal highlights the study’s focus on rejection and intervention support, limiting the conceptual breadth by excluding attitudes of acceptance or justification. In addition, reliance on self-report data may have introduced social desirability bias, and the use of convenience sampling could limit the external validity, as participants may not fully represent the broader Saudi population.
Implications of Findings
Policymakers, health care providers, and community leaders can utilize the validated tool to identify harmful norms, inform context-specific interventions, and track progress. Such informed, evidence-based approaches align with global efforts to dismantle systemic support for violence and replace it with safety, respect, and gender equity (Ferrer-Perez et al., 2020). The current instrument focuses on Arab and Muslim communities, enabling comparisons between populations and supporting the design of culturally grounded prevention strategies. Furthermore, the tool can be translated into other languages for use in non–Arab Muslim communities. The current study demonstrates the practical application in nursing. Nurses provide culturally adapted education and support, serving as trusted professionals for women affected by domestic violence (O’Dwyer et al., 2019; Palmieri & Valentine., 2021), particularly in environments where cultural norms may hinder disclosure (Alshammari et al., 2018). Nurse educators can integrate these findings into curricula and outreach to identify warning signs and challenge harmful norms (Bacchus et al., 2024; Montesanti, 2023; Rathnayake et al., 2023; Stephenson, 2024).
Conclusion
By capturing locally relevant constructs and demonstrating strong reliability and validity, the tool provides a strategic platform for public health interventions, community education, and policy development. Although further refinement is needed to fully capture acceptance dimensions, the current instrument offers a solid foundation for advancing gender equity and preventing violence against women. Future expansions and adaptations may extend its applicability across diverse cultural settings, ultimately strengthening the global response to DVAW. Overall, such tools can guide nursing research, fostering shifts in attitudes and supporting effective health care policies for violence prevention.
Footnotes
Appendix
Expert Panel Rating of DVAW Attitude Questionnaire Final Version.
| Questionnaire items (9) | Rater 1 | Rater 2 | Rater 3 | Rater 4 | Rater 5 | Experts in Agreement | Item CVI |
|---|---|---|---|---|---|---|---|
| 1 |
|
2 |
|
|
|
|
|
| 2 |
|
3 |
|
|
|
|
|
| 3 |
|
|
|
|
|
|
|
| 4 |
|
|
|
|
|
|
|
| 5 |
|
|
|
|
|
|
|
| 6 |
|
|
|
|
|
|
|
| 7 |
|
|
|
|
|
|
|
| 8 |
|
|
|
|
|
|
|
| 9 |
|
|
|
|
|
|
|
| S-CVI | 0.98 | ||||||
| Total Agreement | 8 | ||||||
| S-CVI/UA | 0.89 | ||||||
Note. Excellent agreement and ICV are in bold.
Acknowledgements
A special thank you to Dr. Ehab Elmongui for his valuable statistical consultation and support.
Author Contributions
Conceptualization and Study Design: AS, AO, RA, SH, AMA, HM, and HAS conceptualized the study, developed the methodology, and defined the research scope and objectives.
Writing—Original Draft: AS, RA, and AO
Writing—Review and Editing: AS, RA, SH, AMA, HM, HAS, and AO critically reviewed and revised the manuscript for intellectual content, ensuring clarity, coherence, and alignment with journal requirements.
Final Approval: All authors (AS, RA, SH, AMA, HAS, HM, and AO) read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Consent to Participate
All participants who responded to the study provided written informed consent before completing the study questionnaire. The data collected were completely anonymous, and the participants ensured that their participation was entirely voluntary.
Data Availability
The data collected for the current study are available and will be provided upon reasonable request. Please contact Dr. Selim for data availability at
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
Institutional Review Board (IRB) approval was secured from King Abdullah International Medical Research Center, Riyadh (IRB number: H-01-R-005)