
Abstract
Introduction: When it comes to non-communicable diseases like diabetes, inadequate knowledge, attitude, and practice are often linked to poor health outcomes. This study aims to assess the patients’ knowledge, attitude, and practice (KAP) of diabetes in the outpatient department of a university teaching hospital in Saudi Arabia. Methodology: In this cross-sectional study, diabetes type 2 patients attending outpatient departments at a university teaching hospital, Riyadh, were assessed regarding their knowledge, attitude, and practice toward diabetes using a validated KAP scale. Descriptive and inferential analysis was done to determine the factors associated with KAP score using SPSS version 26.0 software (SPSS Inc., Chicago, IL, U.S.). Results: Males made up 69.7% of the sample (n = 165), while 56.9% were between the ages of 41 and 75. The level of knowledge and practice had “good” in 37.6%, and 47.9%, respectively, but level of attitude had “positive” in 30.9% of patients. The association between knowledge tier and gender (p0.014) and insurance status (p0.008), respectively, was shown to be significant. However, the attitude tier was only significantly associated with gender (P = .003). The practice tier also showed a significant age association (P = .049). As regards, the mean scores for diabetes-related knowledge were higher only among insured participants (P = .03) than for other participants’ sociodemographic factors. Meanwhile, the mean attitude scores were also higher among males (P = .006) than for other sociodemographic characteristics. A comparison of the participants’ sociodemographic characteristics found no statistically significant variations in practice scores. Conclusion: Unfortunately, this study found that outpatient diabetes patients had insufficient knowledge, practice, and a negative attitude toward diabetes type 2. This imposes a great burden on healthcare workers and hence the healthcare system to improve patient scores via diabetes education programs or pharmacist-led patient counseling initiatives.
Educating diabetes patients has been shown to have positive effects on their clinical results and quality of life. Patients and healthcare professionals who could not make lifestyle changes might reduce diabetes-related morbidity and mortality because of a lack of knowledge, attitude, and practice in type 2 diabetes management. The findings of this research cannot be generalized, but they do place significant pressure on healthcare personnel and hence the healthcare system to improve patient scores via diabetes education programs or pharmacist-led patient counseling efforts. Provides an assessment of diabetics’ knowledge, attitudes, and behaviors at a Saudi teaching university hospital where a large number of interns can be seen as a cornerstone of improving health outcomes, particularly for non-communicable diseases such as diabetes mellitus.What do we already know about this topic?
How does your research contribute to the field?
What are your research’s implications toward theory, practice, or policy?
Introduction
Diabetes mellitus (DM) has been more common in developed and developing countries during the last several decades.1–3 According to WHO estimations, Saudi Arabia ranks second in the Middle East and seventh globally for DM prevalence.1,2 According to the International DM Federation (IDF), 463 million people worldwide have DM. Of them, 55 million live in MENA countries, and the number is expected to increase to 108 million by 2045. 4 The prevalence of DM was projected to be 18.3% in Saudi Arabia, 16.3% in the United Arab Emirates (UAE), 17.2% in Egypt, and 12.7% in Jordan. 5
DM is the cardinal reason for death all around the world. 6 Out of 3.7 million deaths connected to blood glucose levels in 2012, DM was the immediate reason for 1.5 million passing worldwide and the extra 2.2 million passing were caused by the growing risk of cardiovascular and other diseases as a consequence of hyperglycemia. It expected for DM to end up the seventh driving reason for death by 2030.6,7 In Saudi Arabia, diabetes mellitus has turned out to be progressively clear in the last two decades because of emotional changes in the way of life. 7
DM and its consequences have grown to be a major public health issue. The majority of diabetes-related morbidity and death is caused by cardiovascular disease. 8 When compared to those without diabetes, people with diabetes have a two- to four-fold higher risk of cardiovascular events. When it comes to diabetes individuals, cardiovascular disease may account for as much as 80% of their early excess mortality. 9
Knowledge of this notably prevalent illness is critical for early diagnosis and management. 10 Patients who knew more about their disease had a positive perspective and practiced healthy habits, which enabled them to present sooner in the course of their illness. Furthermore, patients who were unaware of their disease risk had less control over those predictors. 11
Living with diabetes needs knowledge and experience gained through time. Diabetes patients need to be educated on self-care skills, and this is a prerequisite for effective diabetes control. Insufficient patient education on diabetes and related topics leads to unanswered questions, anxiety, distrust, and anger. Educating diabetes patients has been shown to have positive effects on their clinical results and quality of life. 12 Patients and healthcare professionals who could not make lifestyle changes might reduce diabetes-related morbidity and mortality because of a lack of knowledge, attitude, and practice in type 2 diabetes management. 13
As for Saudi Arabia being one of the countries currently undergoing rapid development, it is faced with the challenge of the increase in the number of diabetic patients. Earlier reports found various factors, such as sociodemographic, knowledge of the disease, and early diagnosis, are thought to influence the prevalence of DM. A recent Saudi study found that most individuals had never monitored their blood glucose levels and one-third of participants thought alternative medicine might manage diabetes. 14 Another Saudi study revealed the positive patient attitude toward the disease was connected with health-related quality of life (HRQoL) and that most respondents felt in charge of their treatment. 15 However, managing or diminishing the incidence of diabetes necessitates assessing the general knowledge, attitude, and behavior of people with diabetes. Thus, it is essential to evaluate DM’s knowledge, attitude, and practice among diabetic outpatients visiting a tertiary hospital. Furthermore, such data is vital to designing public health regulations with specific national implementation. Therefore, we designed this study is to assess the knowledge, attitude, and practice among people with diabetes among outpatients visiting a university teaching hospital in Riyadh, Saudi Arabia.
Materials and Methods
Study Design and Population
A cross- sectional self-administered survey study was conducted at a university teaching hospital, a tertiary teaching hospital in Riyadh, Saudi Arabia, between May and October 2018. The study setting hospital is multi-disciplinary facility with general and subspecialty medical services that provides primary, secondary care, and tertiary care to its patients. It includes a designated outpatient and inpatient facilities with a specialized diabetes clinic. Two well-trained researchers conducted the questionnaire in all instances to guarantee consistency. We included all outpatient diabetics who attended the endocrinology clinic during the study period. Patients aged >18 years and having at least 6 months of type 2 DM history were recruited in the study, while type 1 DM, gestational DM, and mentally ill patients were excluded. Furthermore, prior to data collection, ethical approval was obtained from the College of medicine at university teaching hospital (Research project reference number: E-16-1903). Patients who fulfilled the study’s requirements were recruited with informed consent and assured that their data would be kept private and used only for research reasons.
Design of the Questionnaire
The questionnaire used for this study was prepared based on previous studies published in a similar context as well as including additional questions based on local diabetic attitudes and practices that were deemed relevant.16–18 The questionnaire is composed of 2 sets, the first of which focuses on the patient’s demographics, such as age, gender, employment position, educational attainment, and smoking habits. The second section of the questionnaire was devoted to questions about KAP (knowledge, attitude, and practice). A Knowledge, Attitudes, and Practices (KAP) survey is a quantitative approach for gathering quantitative and qualitative data. KAP survey discloses what was stated, but there may be significant gaps between what was said and what was done. It consists of 20 questionnaires, the first eight items of which are knowledge-wise assessments with multiple options about DM symptoms, complications, treatment plans, blood glucose control, food habits, and foot care problems. Six diabetes-related attitudes were evaluated, including the importance of managing DM symptoms such as glucosuria and ketonuria, as well as achieving and maintaining ideal body weight. Another six diabetes-related practices completed the KAP questionnaire, including the frequency of blood glucose testing, blood pressure monitoring, regular exercise, and, finally, the frequency of participating in DM education programs, are explored.
The questionnaire was translated into Arabic by an independent professional translator, and experts in the field were asked to independently evaluate the questionnaire’s validity by noting the appropriateness of the questions. After that, we validated the questionnaire through a random selection of 10 patients to check for the reliability test. Cronbach’s alpha was found to be .81.
Each knowledge, attitude, and practice question were assigned a point value of one (1) for a correct response and zero (0) for erroneous ones. We established two tiers of either knowledge, attitude, or practice scores depending on participants’ responses:
Good knowledge is shown when patients answer knowledge questions with a mean score higher than or equal to six, while poor knowledgeable patients are those who answer knowledge questions with a mean score of less than six.
Good practice is shown when patients answer practice questions with a mean score higher than or equal to four, while poor practicing patients are those who answer practice questions with a mean score of less than four.
Positive attitude is shown when patients answer attitude questions with a mean score higher than or equal to four, while negative attitude, patients are those who answer attitude questions with a mean score of less than four.
Data Management
Data extraction is a crucial step in the research process and involves careful examination of complete and incomplete answered questionnaires. 19 In the current study, data were checked for accuracy and completeness and any missing, incomplete, or invalid responses were excluded from the study.
Data Analysis
Categorical data are presented as frequency and percentage. Continuous data were presented as medians and interquartile ranges (IQRs) or means and standard deviation (SD). The association between the categorical variables and either knowledge, attitude, or practice tiers was assessed using a chi-square test and analysis of variance (ANOVA) to compare their score means. Statistical significance was determined for all analyses by a P-value less than .05. The data were analyzed using the SPSS version 26.0.
Results
Demographic characteristics of the participants

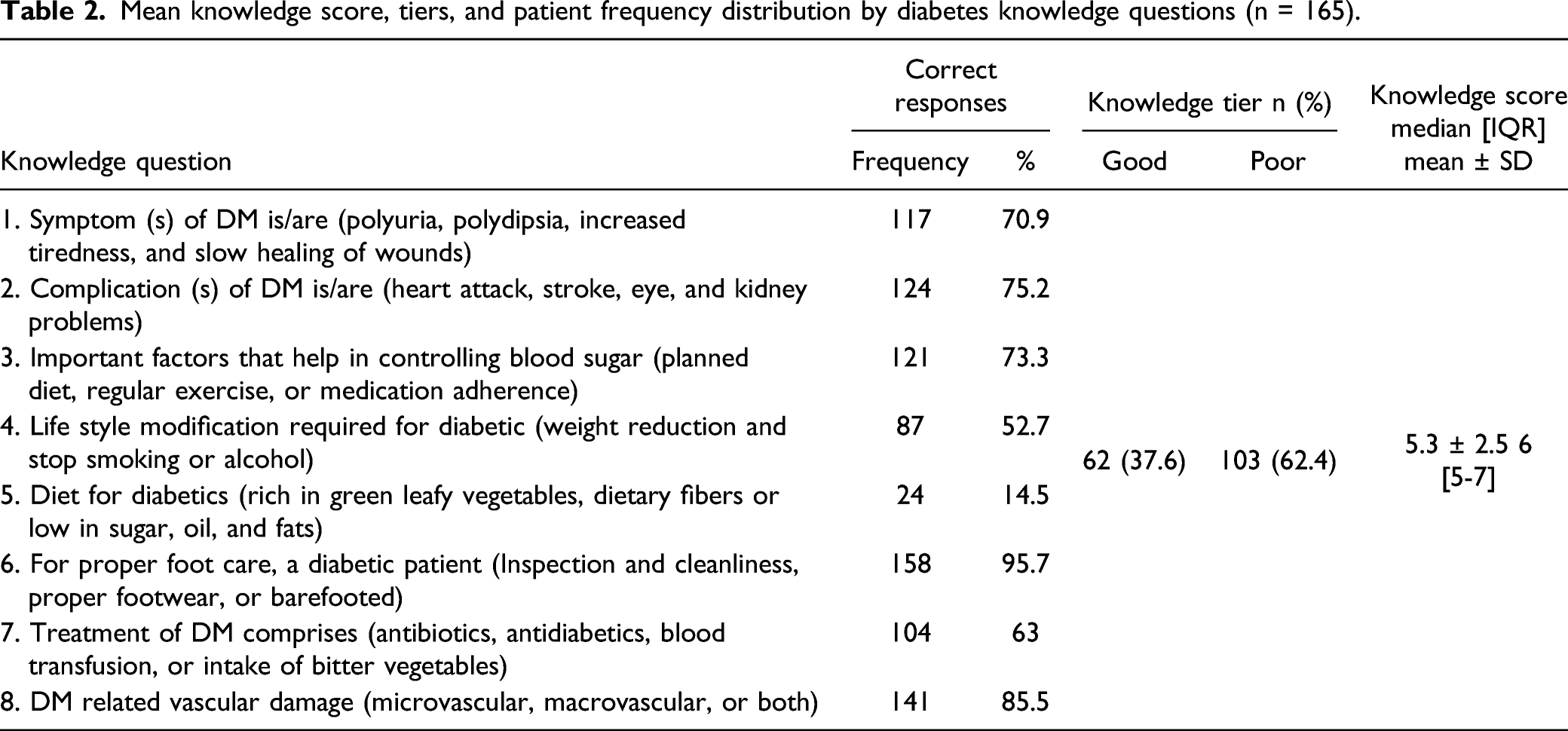
Mean knowledge score, tiers, and patient frequency distribution by diabetes knowledge questions (n = 165).
Mean attitude score, tiers, and patient frequency distribution by diabetes attitude questions (n = 165).

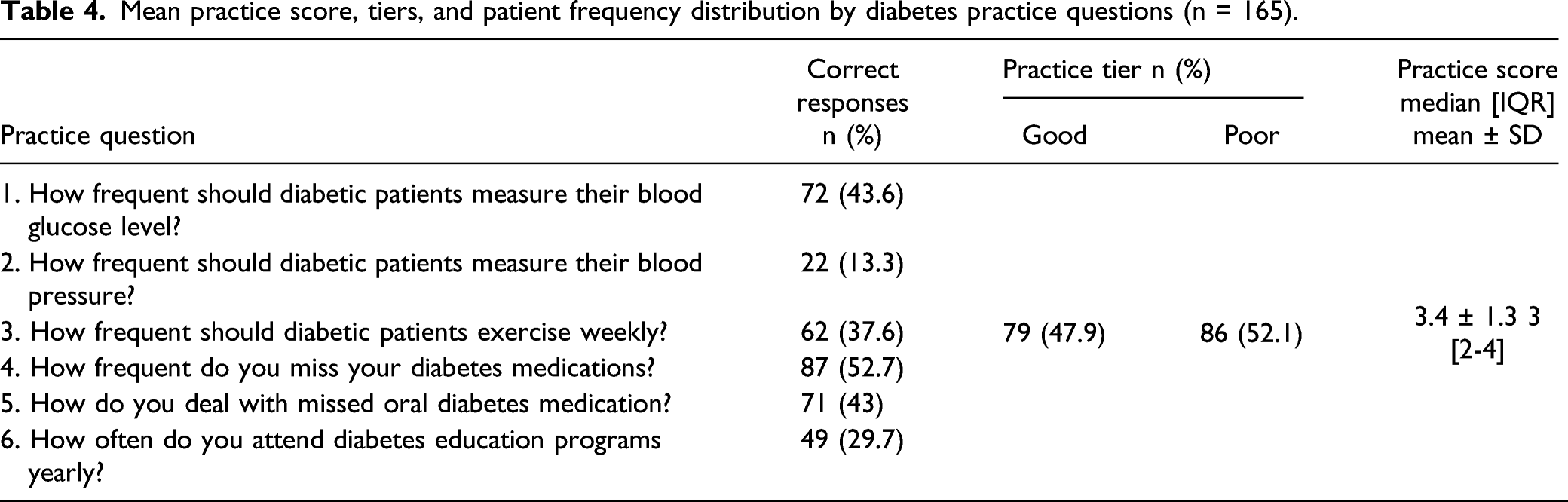
Mean practice score, tiers, and patient frequency distribution by diabetes practice questions (n = 165).
Association of different knowledge, attitude, and practice of DM tiers regards participants’ demographics.

For diabetes knowledge, 103 (6.2.4%) patients had inadequate knowledge. 114 (69.1%) of the cases had negative attitudes, while 86 (52.1%) had poor practices.
one-way ANOVA **Chi-square.
Regarding the distribution of participants' diabetes-related knowledge, attitude, practice, and belief levels, 103 (6.2.4%) cases had poor knowledge scores. In contrast, the majority of the cases, 114 (69.1%), had negative attitude scores, and more than half of the patients, 86 (52.1%), had poor practice scores, as shown in Tables 2, 3, and 4, respectively.
Also, it can be shown in Table 5, the mean scores for diabetes-related knowledge, attitude, and practice were significantly higher only among insured participants (P = .03) than the mean knowledge scores for other participants’' sociodemographic variables. Moreover, the mean scores for diabetes-related knowledge, attitude, and practice were significantly higher only among males (P = .006) than the mean attitude scores for other participants’ sociodemographic variables. Finally, the mean scores for diabetes-related knowledge, attitude, and practice revealed no statistically significant differences in practice scores across various sociodemographic factors of the participants.
Discussion
In this modern era of society, the prevalence of communicable diseases is on the rise, including DM, and when it comes to diabetes prevalence, the WHO has ranked Saudi Arabia the seventh in the world and second in the Middle East.16,20–22 As the American Diabetes Association (ADA) has always said, clinical treatment, self-care behaviors, and patient education are critical to preventing chronic problems associated with this public health issue and managing it effectively. 23
In this study, patients were asked to fulfill questions on several fundamental characteristics of diabetes, such as their knowledge, attitude, and habits toward their disease. 117 (70.9%) of the participants correctly identified diabetes-related symptoms such as frequent urination, increased thirst, hunger, fatigue, and delayed wound healing, which is comparable to Abougalambou et al. 2019’s research where 81% of participants properly identified diabetes symptoms. 24 On the other hand, our study results are better than the one has done among Nepalian diabetics who reported 37.9% of the participants only identified correctly diabetic symptoms. 25 Nevertheless, the median knowledge score of participants in this study was 6 and more than 62% toward the poor tier. The median knowledge score for diabetes was 10 (good knowledge range 9–17), according to Al-Yahya et al. 18 The average knowledge score for DM was good among our participants, which is comparable with another research performed in Fiji by Zibran et al., who found a good level of knowledge with a mean knowledge score of 23.3 out of 30 (SD 3.25). 26 In India, on the other hand, John et al. found that 58% of their sample lacked good knowledge. 11 These discrepancies in knowledge on DM across studies might be explained by changes in the participants’ sociodemographic, their educational level, and the amount of knowledge about diabetes that was available at the time.
In the current research, the majority (75.2%) of the patients knew that DM damages the heart, brain, eye, and kidneys, which is better than the earlier two studies by Bimani et al. and Endale and Teni.27,28 However, these findings were similar to previous findings by Abougalambou et al. who reported 82% of patients identified it correctly. 24 Planned diet, regular exercise, and medication adherence are considered as crucial measures to regulate blood glucose levels by the vast majority of patients (73.7%). Studies in Malaysia and the United Arab Emirates29,30 found that participants had a higher understanding of exercise-related issues, but Hashmi found that only 9% of patients recognized that weight loss is a vital control option. 31 In our research, only 51 patients (30.9%) showed a positive attitude toward diabetes. Srinivasan and his colleagues explored 29.2% of patients with a positive attitude toward diabetes. 11 In contrast, Hussain R et al. reported that 53.8% of diabetics had a positive attitude toward diabetes. 32 When compared to the participants in Hussain’s R et al., Srinivasan et al., and Rani PK et al. were found to have comparable practice patterns in 57.6%, 54.9%, and 48.45% of the participants, respectively.11,32,33
Regrettably, scores of knowledge, attitude, and practice obtained from this study were less than half of the participants. These findings concede with what was concluded by Naheed 34 when he stated that the knowledge, attitude, and practice scores were low in most areas of diabetes care. 34 Nevertheless, many other studies found higher knowledge, attitude, and practice score compared to our results.24,35,36 One reason for the disparity might be the fact that physicians spend less time with their patients, there are less structured diabetes education facilities, and the media has a diminished role.
In this study, one-third of the participants found good knowledge of DM, 37.6%. These results were similar to the previous studies by Binhemd in 1992 and Almalki et al. in 2017 among diabetic patients.37,38 However, the current study results were better than an earlier study by Al-Aboudi et al. who found 14.7% of the participants reported poor DM knowledge. 39 Meanwhile, the knowledge of DM is different with respect to different study populations,40,41 for instance, a previous study by Wajid et al. reported 43.1% of the diabetic knowledge, among pharmacy students, which is better than current study findings. Additionally, a recent study from western region of Saudi Arabia reported lack of knowledge and awareness of DM among Saudi population. 41 Quaresima et al. stated that awareness of gestational diabetes mellitus–related fetal-maternal hazards is critical for optimum compliance among vulnerable mothers. Therefore, they developed a comprehensive post-diagnosis counseling program that addresses GDM incidence, pathogenesis, risk factors, fetal and maternal hazards, and treatment. 42 Patients and the general public benefit significantly from the health education offered by primary healthcare centers (PHCs). Health education must enable and inspire individuals to make educated choices about their healthcare activities. The anticipated impact on public health might pose significant problems to healthcare systems and economies, particularly in quickly emerging nations such as Saudi Arabia. Individuals of reproductive age who have uncontrolled diabetes mellitus may develop long-term complications typically linked with higher morbidity and mortality. Therefore, additional efforts are required to educate patients about the importance of DM management to achieve optimum health outcomes in Saudi Arabia.
Conclusions
Diabetes education is critical for controlling the disease and reducing the incidence of diabetes-related complications, where patient education, awareness of the disease, and importance of regular screening and follow-up will likely increase patient compliance to follow-up visits, which may help in controlling the disease and improving its outcome.
Footnotes
Acknowledgments
The authors of this work would like to acknowledge the Researcher Supporting Project (project number RSP-2021/81) at King Saud University in Saudi Arabia.
Limitation of the Study
Study findings could not be made applicable since glycemic control parameters as HbA1c levels were not accessible to the researchers. Although our study does not reflect a paradigmatic sample of Saudi population, yet it provides an overview of diabetics' knowledge, attitudes, and practices.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.