
Abstract
Objective:
The aim of this study is to evaluate knowledge of and attitudes toward the lumbar puncture procedure among adults in Riyadh region, Saudi Arabia, 2018.
Methods:
This study used a quantitative cross-sectional evaluation of the responses of adults aged ⩾18 years from the Saudi Telecom Company database in the Riyadh region of Saudi Arabia to an online survey between October and December 2018. The questionnaire included questions on knowledge, attitudes, and demography. The questionnaire was pretested and validated (Cronbach’s alpha = 0.701).
Results:
Of 1500 questionnaires, 1223 (81.5%) were returned and included in the analysis. In the study, 57.7% of the participants were aged 18–25 years, and 58.5% of the participants were females. Only 235 (19.2%) participants had an accepted knowledge level of lumbar puncture. The attitudes of the majority of the participants (n = 1151, 94%) to lumbar puncture were acceptable. A multivariate logistic regression test revealed a significant association between an acceptable knowledge level and acceptable attitude level (odds ratio = 2.30, 95% confidence interval = 1.06–5.66). A significant association was also found with ages over 46 years old (odds ratio = 12.99, 95% confidence interval = 4.45–37.9). The attitudes level toward lumbar puncture had a significant negative association among the participants who had a fear of injections in the lumbar region (odds ratio = 0.46, 95% confidence interval = 0.3–0.68).
Conclusion:
There is a lack of appropriate knowledge of the lumbar puncture procedure among the public which predict an unacceptable attitude toward lumbar puncture. Improvements in public education could improve public awareness of the clinical importance/value and complications of lumbar puncture.
Introduction
A lumbar puncture (LP) or spinal tap, which is used to obtain cerebrospinal fluid (CSF), is a commonly used diagnostic procedure to rule out or diagnose various critical neurological conditions.1,2 The procedure may also be performed for therapeutic and anesthetic indications.1–3 It is considered a relatively invasive procedure, with some minor complications, including low back pain, bleeding, and headaches. 2 In rare cases, it may be associated with serious and potentially fatal complications, such as transmission of infections, nerve root injury, and brain herniation. 2 Although serious LP-related complications are infrequent, especially when the procedure is performed by an expert, 2 concern about such complications, along with a lack of awareness about the clinical significance of LPs, is one of the main reasons why patients refuse consent for LPs. 4
Some studies on parents of children with febrile seizures in East Asia reported that the LP refusal rate ranged from 25% to around 28%.5,6 A study conducted with parents in the United Arab Emirates reported a refusal rate of 44%. 7 In contrast, in the United States, the LP refusal rate for patients with Lyme disease was just 5%, 8 and it was just 7% in a Danish study on patients with isolated optic neuritis. 9 Attitudes toward the LP procedure may vary, depending on cultural beliefs, geographical location, and knowledge levels.1,5,10 Patients who refuse consent for LP procedures will be subjected to unwanted hospital admission or an increased hospital stay, both of which are associated with a risk of iatrogenic complications, as well as nosocomial infections.1,7 Such patients may also receive unnecessary empirical antibiotic therapy, which may lead to an increase in antibiotic resistance.4,7 Information on public knowledge of and attitudes toward LPs is needed to develop a suitable strategy to increase the LP consent rate. 10 The latter would result in a reduction in hospitalization cost and burdens on hospitals. Likewise, improving the acceptance level of LPs could reduce unnecessary complications resulting from improper management, thereby leading to a reduction in associated morbidity and mortality. 2 To our knowledge, there is little information in the contemporary literature on LP-related knowledge and attitudes among the Saudi population. Therefore, the purpose of this study was to evaluate LP-related knowledge and attitudes among adults living in Riyadh, Saudi Arabia.
Methods
Study subjects
This study adopted a quantitative cross-section design. It focused on the Riyadh region, which includes Riyadh city and its associated territories in Saudi Arabia, and was conducted in October through December 2018. A randomly selected population (N = 1500) of Saudi adults aged ⩾18 years were invited to take part in an online-based survey. The participants were selected from the Saudi Telecom Company (STC) database, with the aid of a marketing organization. All the participants received an online webpage with an explanation of the purpose of the study, and all potential participants were requested to provide informed consent before they proceeded to the online questionnaire. The participants were encouraged to complete the questionnaire voluntarily at their convenience and within the time interval of the study.
Sample size
According to the Saudi Arabia General Statistical Authority, there were 4,943,447 Saudi adults living in Riyadh in 2018. 11 Using the Epi Info calculator tool of the Centers for Disease Control and Prevention, 12 based on an acceptable error margin equivalent to 4% and the design effect of two together with a confidence interval (CI) of 95%, a sample size of at least 1200 was required. In our study, the total number of respondents included in the analysis was 1223.
Data collection tool
The questionnaire was adapted with the permission of Wan Sulaiman et al. 1 and translated into Arabic. The translation process for the questionnaire included a cross-cultural validation, a review by the translation committee of our institute, and a review by a senior neurologist. Participants were excluded if they had a medical-related degree, as ascertained by a question at the beginning of the questionnaire. Repetition of responses was prevented through the linking of every survey response with an Internet protocol. The Medical College Institutional Review Board, Al-Imam Muhammad Ibn Saud Islamic University, Riyadh, Saudi Arabia approved this study protocol.
Questionnaire
The study employed a self-administrated questionnaire, which included 42 items on LP-related knowledge and attitudes and their associations toward LP procedure. The questionnaire contained multiple-choice questions, which were presented in three main segments: 14 questions on general characteristics, 18 questions on LP-related knowledge, and 10 questions on LP-related attitudes. The general characteristics included demographic variables (age, sex, marital status, level of education, occupation, health insurance, site of residence (i.e. rural or urban), and socioeconomic status). The questionnaire also included questions related to the participants’ previous experience of LP, source of LP-related knowledge, and questions about needle phobias. To ensure the reliability and validity of the questionnaire, a pilot study was carried out with 25 individuals prior to the data collection. Modifications to the questionnaire were made based on this study.
Data analysis
The data were collected and tabulated using Microsoft Excel 2016 and analyzed using SPSS software, version 25 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as frequencies and percentages. Both a univariate chi square analysis and logistic regression tests were conducted to determine the associations between the participants’ knowledge and attitudes and their general characteristics, as well as their attitudes to the accepted level of knowledge, to obtain odds ratios (ORs) for unadjusted and adjusted models. A p value of <0.05 was considered statistically significant.
Scoring system
For LP-related knowledge, a Likert-type scale was used to measure and analyze the responses, where 1 = true, 2 = false, and 3 = I do not know. 13 For each question, a correct response received a score of +1, and an incorrect response received a score of 0. The total achievable score based on the answers to all 18 questions was 18 (100%). The participants’ knowledge level was categorized as “excellent” if they obtained a score of more than 75%, “good” if they obtained a score of between 50% and 75%, and “poor” if they obtained a score of less than 50%. Participants who achieved scores ⩾50% were considered to have an acceptable level of knowledge and used to evaluate the associations in the regression test.
For LP-related attitudes, based on the participants’ response to each question, their attitudes were classified as excellent (a score of +4), good (a score of +3), neutral (a score of +2), bad (a score of +1), or poor (a score of 0). The sum of the scores on all 10 questions provided the final score for each participant, with a total achievable score of 40 (100%). The participants’ attitudes were categorized as “excellent” if they obtained a score of more than 75%, “good” if they obtained a score of between 50% and 75%, and “poor” if they obtained a score of less than 50%. A score of ⩾50% was considered as an acceptable degree of attitude and used to evaluate the associations in the regression test.
Results
Descriptive characteristics
Of the 1500 online questionnaires, 1223 were returned (81.5% response rate). Table 1 presents the demographic data. Most of the participants were aged 18–25 years (n = 706, 57.7%). Females accounted for more than half of the sample (females: n = 716, 58.5%; males: n = 507, 41.5%). The majority of the participants cited “student” as their current occupation (n = 521, 42.2%). Around 800 of the participants were single (65.5%), and 1098 of the participants lived in cities (89.8%). In terms of education levels, among the four listed categories, the majority of the participants said they had a bachelor’s degree (71%). Most of the participants had no health insurance (71.3%), but the majority had a middle-income level (n = 850, 69.5%). Most of the respondents were aware of the LP procedure (62.4%), but the majority had no direct personal experience of LPs (90.8%) or a familial experience of LPs (60.8%). Most of the respondents expressed no fear of injections in the hand (59%), but 83.2% of the participants reported a fear of lumbar injections.
Socio-demographic characteristics of the participants (n = 1223).
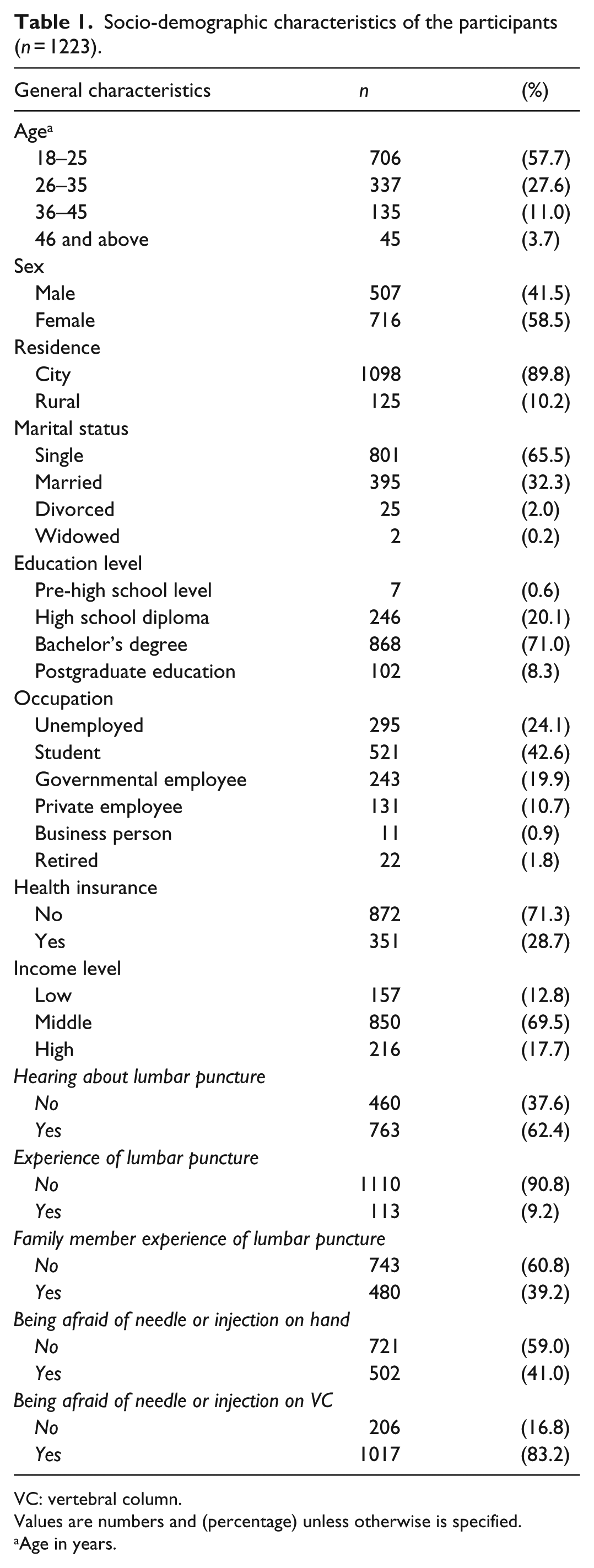
VC: vertebral column.
Values are numbers and (percentage) unless otherwise is specified.
Age in years.
Knowledge and attitude scores
The median score of the participants’ knowledge was 27.7 (interquartile range (IQR): 33.3). Among the respondents, 80.8% of the participants had poor knowledge (<50%), 16.8% had an acceptable moderate knowledge (50% to ⩽75%), and 2.4% had excellent knowledge. On the contrary, the median attitude score of the participants to the LP procedure was 65 (IQR: 15), with 5.9% of the participants having a poor attitude (<50%), 79.2% having an acceptable moderate attitude (50% to ⩽75%), and 14.9% having an excellent attitude (Table 2).
Calculated percentage score for knowledge and attitude toward lumbar puncture.

IQR: interquartile range; Min: minimum; Max: maximum.
Values are numbers and (percentage) unless otherwise is specified.
Tables 3 and 4 show the frequency of correct and incorrect answers to questions about LP-related knowledge and attitude. Question 10 in knowledge section was the most wrongly answered question by the participants (incorrect answers = 46.1%), which asked about severe back pain resulting from the LP procedure. This was followed by general knowledge about LP complications (Question 15) (incorrect answers = 39.6%). In the attitude section, Question 1, which asked about acceptance of the LP procedure in Saudi society, was the most poorly answered questions by the participants (poor answers = 19.6%). Question 9 was the second most poorly answered question (8.5%), in which 104 individuals stated that they would rather go for long time treatment than being diagnosed by LP. The majority of the participants stated that their friends and family members were the source of their LP-related information (32.7%) (Supplemental Figure 1).
Frequency of correct and incorrect answers regarding participants’ knowledge of lumber puncture (LP) (n = 1223).
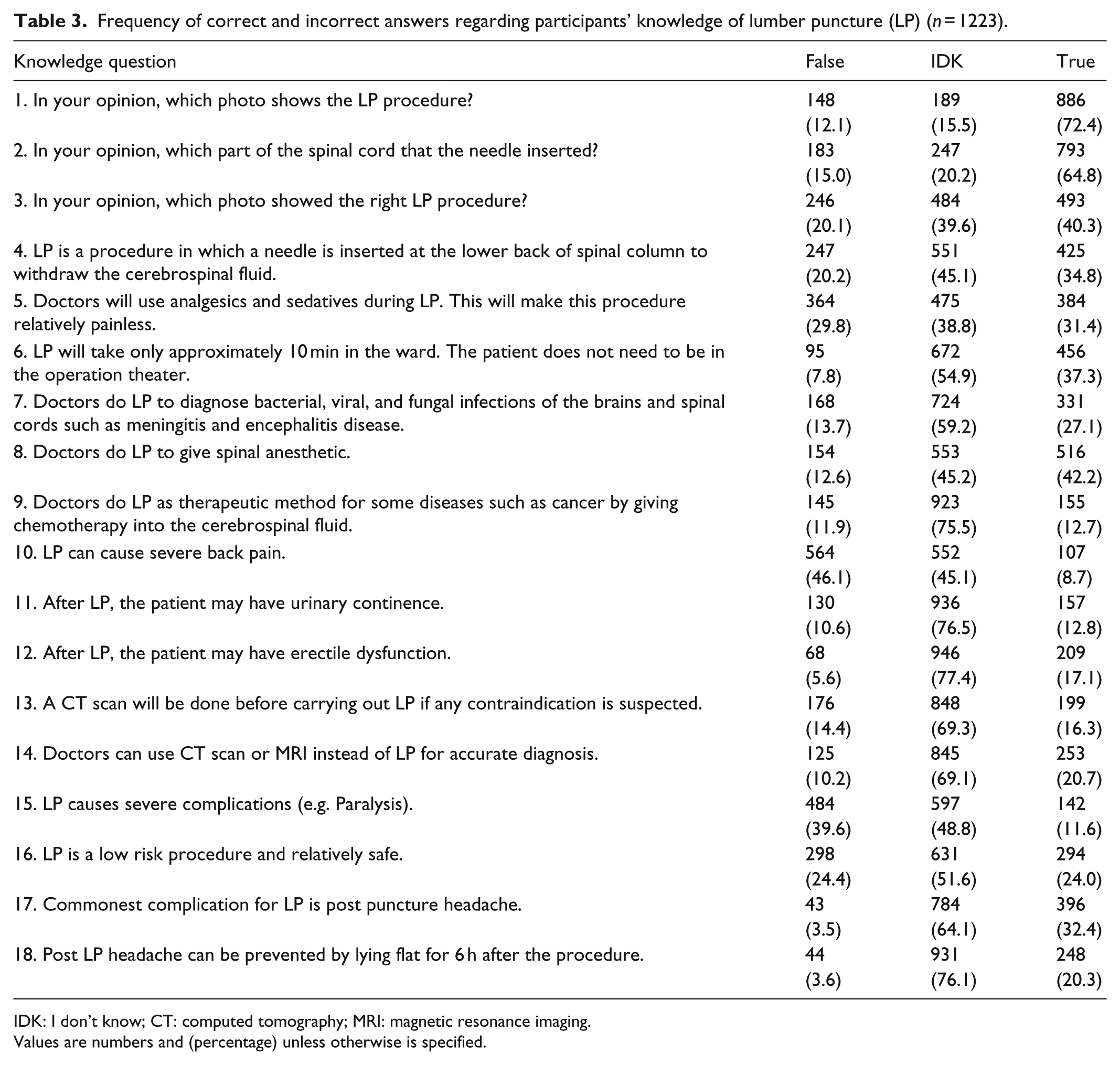
IDK: I don’t know; CT: computed tomography; MRI: magnetic resonance imaging.
Values are numbers and (percentage) unless otherwise is specified.
Distribution of responses regarding participants’ attitude toward lumber puncture (LP) (n = 1223).

Values are numbers and (percentage) unless otherwise is specified.
Relationship between acceptable knowledge scores and other factors
Table 5 shows the association between the acceptable knowledge score and other variables of interest. There was a significant association between older age and greater knowledge scores (p < 0. 001); respondents older than 46 years were approximately 13 times more likely to have a higher level of knowledge than those aged between 18 and 25 years (adjusted OR = 12.99, 95% CI = 4.45–37.9). Marital status was also a significant predictor of the level of knowledge (p < 0. 001), as the LP-related knowledge of the married respondents was more likely to be poor as compared with that of the single respondents (adjusted OR = 0.41, 95% CI = 0.25–0.67). General awareness of LP procedure was another significant predictor of a higher knowledge score (adjusted OR = 5.4, 95% CI = 3.49–8.5). Unlike general awareness, familial-related experience of LP showed a negative correlation with a higher knowledge score (adjusted OR = 0.6, 95% CI = 0.47–0.94). The knowledge scores of the participants who expressed a fear of lumbar injections were lower than those who expressed no such fear (unadjusted OR = 0.45, 95% CI = 0.32–0.63). This relation remained after adjusting for confounders (adjusted OR = 0.46, 95% CI = 0.3–0.68).
Unadjusted and adjusted OR of acceptable knowledge score (⩾50%) across other factor of interests (n = 1223).

OR: odds ratio; CI: confidence interval; VC: vertebral column.
“No health insurance” is the reference group.
p value significance at level 0.05.
Relationship between acceptable attitude scores and other factors
Table 6 describes the association between acceptable attitude scores and other factors of interest. There was a significant association between the acceptable level of knowledge and the acceptable attitude level in both the unadjusted and adjusted analyses (unadjusted OR = 2.73, 95% CI = 1.17–6.38; adjusted OR = 2.30, 95% CI = 1.06–5.66). There was a slight decrease in the acceptable level of attitude of employees when compared with that of unemployed or business people (unadjusted OR = 0.36, 95% CI = 0.17–0.77; adjusted OR = 0.37 95% CI = 0.15–0.93). Some factors such as aged between 36 and 45 years, male sex, and retirement showed a significant association with the acceptable level of knowledge before adjusting for confounders (p < 0.05), but these associations were not maintained after the adjustment. The attitudes of the participants who were aware of the LP procedure were better (approximately two and a half times higher) than those of the participants who had never heard of the procedure. This relation was noted in both the adjusted and unadjusted analyses. The participants who reported previous LP-related experience had poorer attitudes as compared with those of their counterparts (OR = 0.33, 95% CI = 0.13–0.80). A fear of upper arm injections was associated with poorer attitudes in both analyses (OR = 0.54, 95% CI = 0.32–0.91). None of the other variables showed a significant association with acceptable attitude scores (p > 0.05).
Unadjusted and adjusted OR of acceptable attitude score (⩾50%) across other factor of interests (n = 1223).

OR: odds ratio; CI: confidence interval; VC: vertebral column.
“No health insurance” is the reference group.
p value significance at level 0.05.
Discussion
The LP procedure plays an essential diagnostic role, as well as a role in anesthetic and therapeutic indications, in several neurological diseases. Training in procedure conduction and the presence of an optimal laboratory facility play an important role in accurate and safe CSF studies. Patients’ and relatives’ LP misconceptions are one of the main reasons for LP rejection.14,15 To the best of our knowledge, this is the first study to examine public knowledge and attitudes concerning the LP procedure among Saudi adults in Riyadh, Saudi Arabia. Previous studies on this issue in different settings have found that the public lacks an appropriate level of knowledge about, in addition to having poor attitudes toward, LPs. In this study, 80.8% of the respondents were poorly informed (standardized score: <50%) about the LP procedure. Moreover, LP-related attitudes were directly proportional to the participants’ levels of knowledge. Those with greater knowledge levels had better attitudes toward the LP procedure and vice versa. These findings support those of earlier studies by Wan Sulaiman et al., 1 Borhani-Haghighi et al., 16 and Farag et al., 17 which also found a significant relationship between attitudes and knowledge levels (p < 0.0001). In this study, after adjusting for confounders in the logistic regression test, age older than 36 years, an awareness of the LP procedure and previous experience of the procedure were the only factors that showed a positive significant association with an acceptable level of knowledge. In contrast to the results of the study by Borhani-Haghighi et al., 16 level of income, sex, education level, and place of residence (e.g. a city) were not statistically significant in this study, whereas LP-related experience was significant in both studies. Furthermore, Farag et al. 17 illustrated that males were more prone to accepting LP procedures. However, in this study, the logistic regression tests showed no significant differences in the attitudes toward LP.
The findings of this study are in accordance with those of Wan Sulaiman et al., 1 who found a significant negative association between needle injection fear and attitudes toward LP. A fear of needles can range in scale from mild to extreme (needle phobia). The anxiety associated with needle phobia may result in avoidance of medical care, with adverse consequences in terms of health outcomes. According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), the incidence of a psychiatric disorder known as blood-injection-injury phobia 18 affects around 1 in every 10 people.1,19 Both types of fear of injections, either in the upper arm or lumbar regions, showed a significant unadjusted association with poorer attitudes toward LP. Medical providers need to be aware of this condition because of its potential impact on medical management and outcomes. A systematic review illustrated that multiple sessions of exposure-based psychological therapy, imaginal exposure interventions, and applied tension were effective methods of treatment for minimizing fears associated with needles. 20
The majority of the participants in this study failed to comprehend the answer to the knowledge questions and stayed neutral to the attitude questions manifest the decent chance to enhance the attitude of the public toward the LP procedures primarily via education. The bulk of the participants, in common with most sectors of society, did not seem to be aware of the importance of the LP procedure as a diagnostic technique for central nervous system infections, such as meningitis and encephalitis. Aside from the relation of knowledge and attitude, most of the participants expressed an interest in LP-related education, which is an important point that our attitude’s result point out, and this was in support with Borhani-Haghighi et al.’s 16 findings. Educational interventions to evaluate the impact on LP-related knowledge and attitudes should be investigated more closely. With a higher level of knowledge, people will be better equipped to evaluate the risks and benefits of the LP procedure and hopefully be willing to accept the LP procedure. 21
This study addressed the issue of LP rejection and its importance in terms of the serious complications that may ensure due to delayed diagnoses and treatments. The findings demonstrated that the level of LP-related knowledge among the public was relatively low and that this significantly predicted poor attitudes. There is a crucial need for the health ministry and policy makers to raise awareness of the importance of the LP procedure and LP-related complications through social media and health-related campaigns.
Limitations
The limitations of this study include the self-reported nature of the data, which has the potential for misclassification. Second, Cronbach’s alpha was 0.701, which indicated that the questionnaire may have only a moderate level of reliability. In addition, as this study was conducted in a specific region (Riyadh), the findings may not be applicable to other Saudi regions that have different habits, cultures, and beliefs. Furthermore, a single questionnaire is not sufficient to comprehensively cover all aspects of the LP procedure. Likewise, in this study, the STC database was used to select our participants, so there is a probability for old people and those with low education level to be less included, whereas young and people with good education level to be more included. Future studies should assess other factors that could influence public knowledge and attitudes toward LP. Regardless of these limitations, this prefatory study provides baseline information on public awareness and attitudes toward the LP procedure, in addition to information on factors that affect LP-related knowledge and attitudes among the public. As the data are recent, they are more likely to reflect the current status of the population. Further population-based cohort studies, as well as interventional test studies, are needed to verify the results of this study.
Conclusion
This study addressed the issue of LP rejection and its importance in terms of the serious complications that may ensure due to delayed diagnoses and treatments. The findings demonstrated that the level of LP-related knowledge among the public was relatively low and that this significantly predicted poor attitudes. There is a crucial need for the health ministry and policy makers to raise awareness of the importance of the LP procedure and LP-related complications through social media and health-related campaigns.
Supplemental Material
Supplemental_Figure_1 – Supplemental material for Public knowledge and attitude toward lumbar puncture among adults in Riyadh, Saudi Arabia: A cross-sectional study
Supplemental material, Supplemental_Figure_1 for Public knowledge and attitude toward lumbar puncture among adults in Riyadh, Saudi Arabia: A cross-sectional study by Abdulrahman Yousef Aldayel, Muteb Mousa Alharbi, Mohammed Saud Almasri and Saleh Mansoor Alkhonezan in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank all respondents for their time and patience during questionnaire completion.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study’s protocol was approved by the Institutional Review Board (IRB) of Al-Imam Muhammad Ibn Saud Islamic University (IRB no. 0032/03/2018-50).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The informed consent was obtained through a formal online web page from each participant before they completed the questionnaire. All the study’s population were adults 18 years old and above. The written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.