
Abstract
A 15-y-old, castrated male domestic shorthair cat was presented with a 3-d history of lethargy, inappetence, and significant weight loss. Clinical findings included moderate non-regenerative anemia, granular lymphocytes in a blood smear, and abdominal ultrasonographic abnormalities, including splenic mottling and lymphadenomegaly. Atypical lymphocytes that contained engulfed erythrocytes were found on cytologic evaluation of peritoneal fluid and splenic and lymph node aspirates. Despite supportive treatment, the patient rapidly declined and was euthanized. Histologically, neoplastic round cells were centered on blood vessels throughout lungs, liver, spleen, kidneys, and brain. Immunohistochemistry confirmed CD3-positive cells, and PCR revealed a clonal T-cell receptor gene, establishing a diagnosis of angiocentric T-cell lymphoma. Neoplastic infiltration of the myenteric plexus likely caused chronic intestinal pseudo-obstruction, explaining the gastrointestinal signs. Lymphoma should be considered in cases of disseminated vasculopathy.
A 15-y-old, castrated male domestic shorthair cat was presented because of a 3-d history of lethargy and inappetence. The patient had a history of upper airway infections, which had been treated with antibiotics, but were not a concern at presentation. The patient lost 1.2 kg (21% of body weight) over 1 mo and had diffuse muscle atrophy. Given the patient’s fractious temperament, a limited physical examination was performed, which revealed no other abnormalities. The patient was sedated with dexmedetomidine and butorphanol to facilitate blood sample collection for analysis.
A moderate non-regenerative anemia (hematocrit: 0.23 L/L, RI: 0.28–0.49 L/L; reticulocytes: 34 × 109 cells/L, RI: <60 × 109 cells/L) was found on CBC. All other measurands were within RIs, including the WBC concentration (8.4 × 109 cells/L; RI: 4.2–13 × 109 cells/L). In the blood film, ~5% of the leukocytes were intermediate-to-large granular lymphocytes. These 12–15-µm lymphocytes had 8–10-µm round-to-indented eccentrically placed nuclei with clumped chromatin and indistinct nucleoli. The cytoplasm was moderate in volume, light-to-medium blue, and contained a few magenta granules, which were often in small aggregates adjacent to the nucleus.
Mild hypocalcemia (tCa: 2.08 mmol/L, RI: 2.22–2.78 mmol/L)—presumed to be the result of mild hypoalbuminemia (albumin: 29 g/L, RI: 30–44 g/L)—and mild hyperbilirubinemia (total bilirubin: 8.6 µmol/L, RI: 0–4 µmol/L) were the only abnormalities on serum biochemistry.
An abdominal ultrasound was performed. The spleen was diffusely mottled with lobular irregular margins. A 1.48-cm ovoid nodule was present adjacent to the liver and was presumed to be an enlarged abdominal lymph node. Mild nonspecific peritoneal effusion was also present. Decreased corticomedullary distinction and left renal atrophy were consistent with chronic bilateral nonspecific nephropathy. No significant findings were identified in other organs. Aspirates were performed of the free peritoneal fluid, spleen, and the presumed irregular abdominal lymph node.
Cytologic evaluation of the peritoneal fluid, splenic aspirate, and abdominal lymph node aspirate all revealed low numbers of atypical lymphocytes, which had cytomorphologic features similar to those seen in the peripheral blood ( Fig. 1A ). The highest percentage of these lymphocytes (~50% of the total nucleated cell population) was seen in the peritoneal fluid, which was interpreted as a low cellularity effusion with atypical lymphocytes.
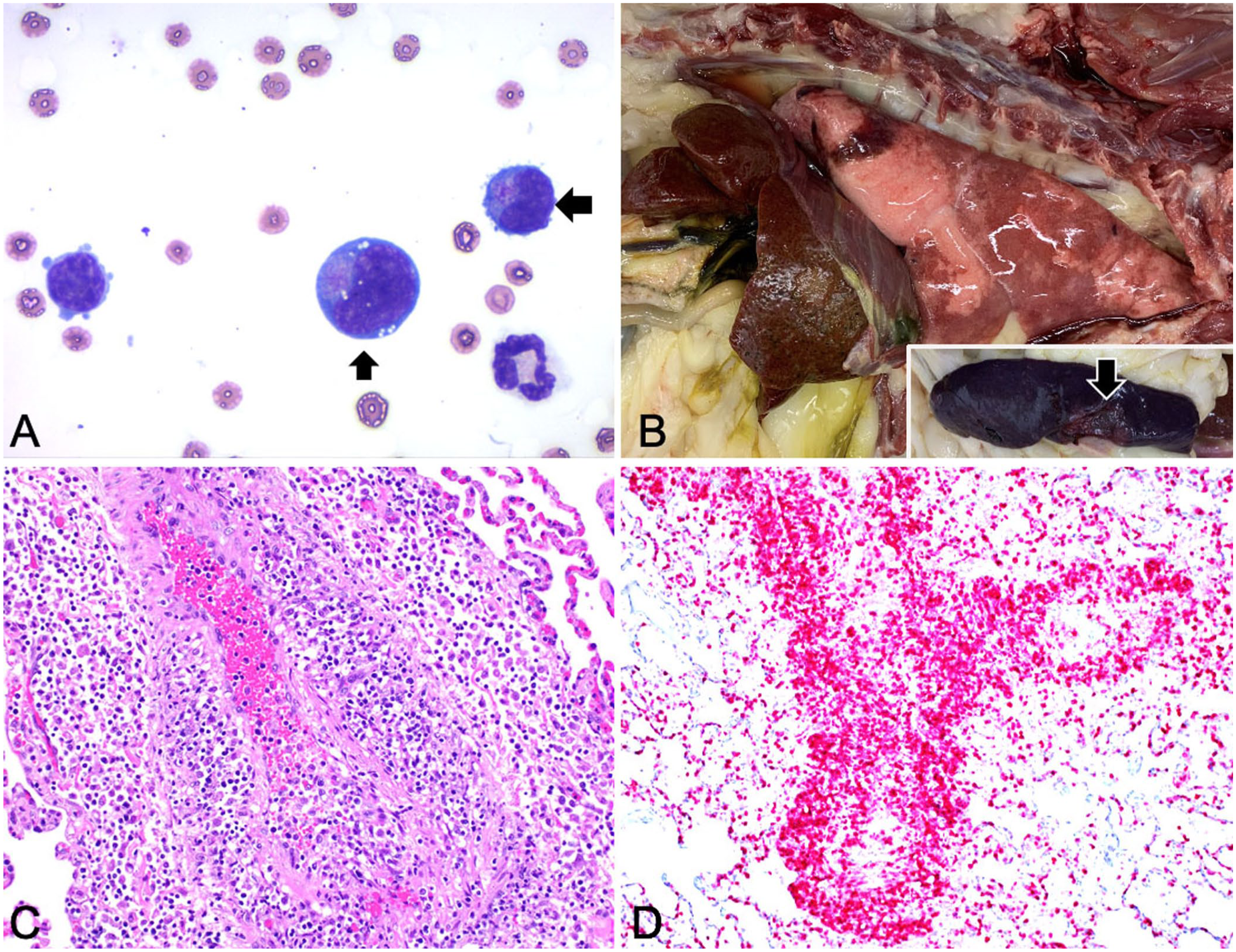
Angiocentric T-cell lymphoma in a cat.
The splenic and lymph node aspirates contained a heterogeneous population of lymphocytes with lower percentages of the atypical lymphocytes; atypical lymphocytes were occasionally observed engulfing erythrocytes. Additionally, erythrophagocytic macrophages were noted. Given the heterogeneity of the lymphocyte population, a reactive or inflammatory process was favored over a lymphoid neoplasm, although lymphoid neoplasia was a strong consideration.
The patient was stable and discharged from the clinic with a working diagnosis of neoplasia, with strong suspicions of gastrointestinal lymphoma. Supportive treatment included maropitant (2.7 mg/kg PO q24h), gabapentin (10 mg/kg PO q8h, as needed), and prednisolone (2 mg/kg PO q12h). Over the following 3 d, the patient steadily declined, becoming laterally recumbent and dyspneic. The owner elected euthanasia.
At postmortem examination, the lungs were mottled red and slightly firm, and ~5 mL of fluid was found in the thorax. The liver was pale, with a rough surface and increased reticular pattern. The spleen was covered with a thin film of blood, moderately enlarged, and had a 2-cm white depressed area in the hilus ( Fig. 1B ). The gastrointestinal tract had no obvious gross abnormalities.
Histologically, in H&E-stained sections of lung, liver, spleen, kidneys, lymph node, myenteric plexus, mesenteric vessels of the small intestine, and brain, we found numerous atypical round cells centered on blood vessels ( Fig. 1C ). These cells had a moderate amount of eosinophilic cytoplasm, round-to-polyhedral nuclei 1.5–2 times the size of an RBC, with 1 prominent nucleolus. These cells also partially to totally occluded the lumens of many blood vessels, aggregating in the intima in clusters and extending transmurally into the adventitia. Mitotic figures were seen in occasional intravascular neoplastic cells. In the lung, infiltrates thickened the alveolar septa; increased numbers of foamy macrophages and moderate edema were in alveoli. Significant erythrophagocytosis by macrophages was noted in the lumen of vessels and in the red pulp of the spleen, with infarcts. Focal necrosis was also noted in the brain and liver, and multiple thrombi were detected in numerous internal organs. The portal vasculature was markedly hypercellular, and hepatic sinusoids were frequently filled with atypical cells, often engulfing RBCs.
Based on the histologic findings, immunohistochemistry testing for CD3, CD79a, and IBA1 was performed following the standard operating procedures of the Virginia Tech Animal Laboratory (Blacksburg, VA, USA). Most of the suspected neoplastic cells had strong cytoplasmic immunoreactivity for CD3 ( Fig. 1D ). To confirm a T-cell lymphoma diagnosis, lung tissue scrolls were submitted to the Clinical Hemopathology Laboratory at Colorado State University (Fort Collins, CO, USA) for PCR for antigen receptor rearrangement. Polyclonal immunoglobulin and clonal T-cell receptor genes were revealed. Given the accumulation of neoplastic cells in the vasculature, angiocentric T-cell lymphoma was diagnosed. Intravascular lymphoma was ruled out, given the invasion of vessel walls and surrounding tissue by the neoplastic lymphocytes.
Lymphoma associated with the vasculature can be broadly characterized as either intravascular lymphoma or angiocentric (sometimes referred to as angioinvasive or angiodestructive) lymphoma; differentiation of the 2 forms relies on the location of the lymphocytes with respect to the blood vessel. In intravascular lymphoma, neoplastic lymphocytes are present within blood vessels. Blood vessels are often occluded and distended, but the endothelium is still visible and the lymphocytes do not infiltrate the vessel walls. 15 In angiocentric lymphoma, neoplastic lymphocytes surround the blood vessel, often compress the vessel lumen, and may invade the vessel lumen. 15 We considered intravascular lymphoma in our case, given the large aggregates of cells within multiple vessel lumens, but invasion of the vessel wall by neoplastic cells made the diagnosis of angiocentric lymphoma more appropriate.
Angiocentric T-cell lymphoma is a rare disease. Although rarely reported in cats, angiocentric T-cell lymphoma has been reported in other species, including dogs and people. Angioinvasive T-cell lymphoma originating in the skin and ocular tissues has been reported in dogs, although lung lesions are most common. 9 Angiocentric T-cell lymphoma is also rare in humans, often resulting in lung or disseminated disease, with diagnosis made at autopsy.7,10,13 In humans, the nasal and upper respiratory tract variants account for ~20% of angiocentric or angioinvasive lymphoma cases. 14 In all species, prognosis is poor.
In 2 reported cases of angioinvasive T-cell lymphoma in feline patients, skin nodules were the initial clinical presentation, and lesions were present in lung, eyes, lymph nodes, liver, and spleen.2,12 A case of angioinvasive T-cell lymphoma of the tympanic bulla was reported in a FeLV-positive cat, with postmortem lesions also found in the liver and spleen. 13 Similar to our case, all of the cats in these case reports were euthanized or died shortly after diagnosis.2,12,13 The most common treatment of alimentary large-cell lymphoma and other lymphomas in cats is a combination of prednisolone and chlorambucil, which can prolong survival times. 11 Our case was started on prednisolone after diagnostic testing was performed; however, the response to treatment was poor, and the cat was euthanized. In retrospect, had the cat been started on prednisolone and chlorambucil, the clinical signs may have improved. However, given the severity of the postmortem findings, that improvement seems unlikely.
The clinical signs in our case were nonspecific but were explained by postmortem findings. The moderate non-regenerative anemia was most likely secondary to destruction of RBCs by the neoplastic lymphocytes and erythrophagocytosis by macrophages, which is well described in the literature. 3 Anemia of chronic diseases should also be considered. 3 Rather than gastrointestinal lymphoma, the signs of weight loss and inappetence may have been the result of invasion of the myenteric plexus by neoplastic cells. Lack of peristalsis in the intestinal tract could have led to pseudo-obstruction.
Chronic intestinal pseudo-obstruction (
A diagnosis in our case was only reached after postmortem examination, although neoplasia was suspected based on cytologic and hematologic findings of atypical lymphocytes. Based on the clinical signs and subsequent diagnostic testing, angiocentric or intravascular lymphoma should be considered in patients with nonspecific clinical signs in which antemortem diagnosis cannot be reached definitively. Although angiocentric lymphoma is a rare condition, various primary sites have been documented, and the gastrointestinal system should be considered as a primary site for cats with gastrointestinal clinical signs and granular lymphocytes in the peripheral blood. Angiocentric lymphoma may be underdiagnosed in practice, given the nonspecific clinical signs and laboratory findings and lack of autopsy follow-up.
Footnotes
Acknowledgements
We thank Jinhua Zhang and Daren Lewis from Virginia Tech Animal Laboratory Services for their assistance with histopathology and immunohistochemistry.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.