
Abstract
Neuroglial choristomas are rare in humans and animals. During a routine medical examination, an ovarian mass was found in a 5-y-old female mixed-breed dog. Histologically, the ovarian mass was well-defined, expansile, and composed of large polygonal cells resembling well-differentiated neurons and scattered smaller cells resembling glial cells. Immunohistochemically, the neuron-like cells were positive for neuronal nuclei; the smaller cells were positive for glial fibrillar acidic protein, oligodendrocyte transcription factor 2, and ionized calcium–binding adaptor protein-1. Ovarian neuroglial choristoma was diagnosed.
A choristoma is a tumor-like mass consisting of normal cells in an unusual location. 5 Neuroglial choristoma is a rare ectopic lesion of mature neuroglial tissue that is anatomically not directly associated with the CNS. 17 Various terms used for this entity, such as hamartoma, neuroglial heterotopia, heterotopic brain tissue, teratoma, and glioma, highlight the ongoing uncertainty over its pathogenesis.17,33 No specific syndromic tendencies or etiologic factors have been identified. 9
In humans, neuroglial choristoma has been reported most commonly in extracranial midline structures of the head and neck, including the nose, 31 nasopharynx,4,7 oropharynx,8,18,21,28,37 and tongue.9,11,13 Notably, the incidence of these lesions is 57% in the palatopharyngeal region and 37% in the tongue. 18 Only a few cases have been reported at other sites, such as middle ear,16,23,36 temporal region,19,30 foot, 14 retroperitoneum,12,39 and cervix. 2
In animals, only a few cases of neuroglial choristoma have been reported, including in the pharynx 10 and skin 33 of kittens, the retina 1 and ovary 6 of dogs, and the oropharynx of a newborn harbor seal. 17 Here we describe a rare case of neuroglial choristoma in the ovary of a dog, in which we used a comprehensive panel of immunohistochemical markers to elucidate the probable histogenesis of the proliferating cell types.
A 5-y-old, intact female, mixed-breed dog was presented to a local veterinary hospital due to a mammary mass. CBC, blood chemistry, urinalysis, and radiographic examination were unremarkable. The dog underwent ovariohysterectomy and mastectomy. During the surgery, the right ovary was multinodular and approximately twice as large as its left counterpart (Fig. 1). The ovaries and uterus were submitted for histologic examination.

The right ovary (arrow) was enlarged and multinodular.
The tissues were fixed in 10% neutral-buffered formalin, processed routinely, and sections stained with H&E. Microscopically, the right ovary contained a well-defined, encapsulated, expansile, multilocular, cystic mass that compressed the normal ovarian parenchyma (Fig. 2A). The mass was comprised of large round-to-polygonal cells with a centrally located round nucleus, prominent single nucleolus, and abundant eosinophilic cytoplasm, resembling neurons, as well as many scattered smaller round, polygonal, or rod-shaped cells (Fig. 2B). The background stromal tissue was diffusely eosinophilic and vacuolated with a few capillaries, resembling neuroparenchyma. All cells were well-differentiated, and no mitoses were observed in 2.37 mm2. The variously sized cystic spaces contained serous fluid and cell debris. We found no cell types of endodermal or mesodermal origin in multiple sections of the ovarian mass. No significant microscopic lesions were found in the left ovary or the uterus.
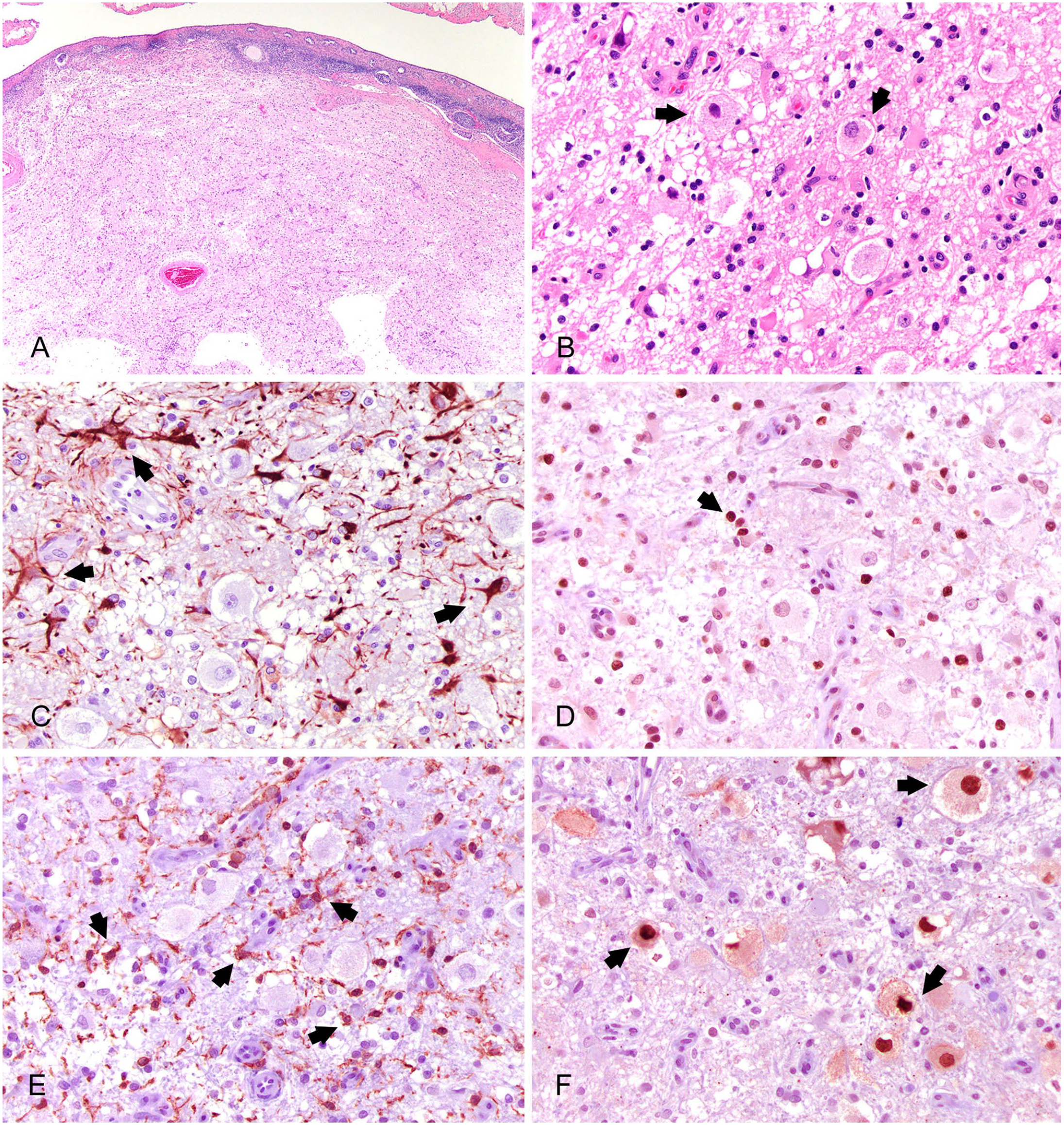
Ovarian neuroglial choristoma in a female dog.
To investigate the origin of the cells comprising the ovarian mass, immunohistochemistry (IHC) was performed with antibodies against glial fibrillary acidic protein (GFAP), oligodendrocyte transcription factor 2 (Olig2), ionized calcium–binding adapter molecule-1 (Iba1), and neuronal nuclei (NeuN; Table 1). All antibodies had been validated for use with canine tissues.20,38
Primary antibodies used for immunohistochemical staining of an ovarian mass.

GFAP = glial fibrillary acidic protein; Iba1 = ionized calcium–binding adapter protein-1; mAb = monoclonal antibody; NeuN = neuronal nuclei; Olig2 = oligodendrocyte transcription factor 2; pAb = polyclonal antibody.
IHC for GFAP revealed strong cytoplasmic staining on intermediate-sized polyangular cells with dendrites, consistent with astrocytes (Fig. 2C). The small round cells with vacuolated cytoplasm had positive nuclear immunostaining for Olig2, suggesting oligodendrocytes (Fig. 2D). Some small, round-to-slender cells with rod-shaped nuclei and short dendrites had cytoplasmic and membranous immunostaining for Iba1, indicating microglia (Fig. 2E). The nuclei and cytoplasm of the large neuron-like cells stained positively with NeuN (Fig. 2F). The IHC results strongly suggested that the ovarian mass originated from CNS tissue.
Ovarian disorders in female dogs are seen infrequently due to the popularity of early-age spaying. 22 The most common ovarian diseases in dogs are ovarian tumors and cysts. 3 There has been a case report of ovarian neuroglial choristoma in a dog. 6
Various terms have been used to denote choristoma, which can complicate the diagnostic process. Hamartoma is a focal disoriented proliferation of mature cells normally located in their typical tissue. On the other hand, choristoma is a mass of normal tissue occurring in ectopic locations. 5 The term heterotopic brain tissue, or neuroglial heterotopia, refers to the presence of normal brain tissue in an atypical location, but it does not indicate that it is an ectopic tissue forming an expanding mass. 24 Neuroglial choristoma also does not fulfill the diagnostic criteria for glioma or teratoma. 5 Teratoma refers to a tumor made up of the cells derived from at least 2 embryonic layers. 6 In a dog, an ovarian teratoma with predominantly nervous tissue has been reported. 27 Interestingly, in 2 case reports, mature nervous tissue in canine ovaries was diagnosed as monophasic teratoma.32,34 However, the term monophasic teratoma is rarely used in the literature except for those 2 cases and is not found in medical dictionaries. Instead, in human medicine, ovarian monodermal teratoma exists. This term refers to ovarian tumors composed almost exclusively of one embryonic germ cell layer, typically neuroectoderm, with neuroglial or neuroendocrine tumor components.27,29 Given that the cases diagnosed as monophasic teratomas in dogs involved tumors of normal nervous tissue in the ovaries,32,34 a more appropriate diagnosis would be neuroglial choristoma.
Neuroglial choristoma may be observed unexpectedly during clinical or radiologic examination 19 because most neuroglial choristomas grow slowly and are subclinical. 37 Clinical manifestations may vary significantly depending on the location and size of the mass or the age of onset.4,11
Histologically, human neuroglial choristomas typically have a solid appearance, although they can also be cystic. 18 Choroid plexus is commonly observed in the neuroglial choristoma. 7 In some cases, various degrees of fibrosis and mineralization can be found, and special stains such as Masson trichrome are helpful in distinguishing between astrocytic glial scar and fibrosis. 31
IHC can contribute to confirming the diagnosis of neuroglial choristoma. IHC for GFAP, 6 Iba1, 6 neuron-specific enolase (NSE),6,32,34 and S10032,34 have been used on previous ovarian cases in the dog. Although NSE and S100 are useful markers, their nonspecific expression in various cell types requires cautious use and interpretation in diagnostic applications.25,35 We used NeuN antibody; NeuN is a protein found in the nuclei and perinuclear cytoplasm of most mammalian neurons and is a reliable immunohistochemical marker for postmitotic neurons. 15 Olig2 is an oligodendroglial lineage–specific marker that is expressed during cell development.26,38
Neuroglial choristoma is generally recognized as a congenital disorder, and various theories regarding its pathogenesis have been proposed. 5 One theory suggests that, during embryonic development, cerebral tissue of the fetus herniates into a cleft or foramen of the skull, similar to the development of encephalocele, thus becoming separated from the cranial cavity. 5 Another theory proposes that the lesion originates from displaced neuroectodermal cells during early embryogenesis.4–6 There is also a theory that the lesion arises from a neoplasm, such as a teratoma, but this is not widely accepted.4,6
Because wellness examinations have become popular in veterinary medicine, neuroglial choristoma, although rare, can be considered as a differential diagnosis for palpable ovarian enlargement in female dogs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
Our study was supported by BK21 FOUR Future Veterinary Medicine Leading Education and Research Center, College of Veterinary Medicine, Seoul National University, Seoul, Republic of Korea.