
Abstract
A 10-y-old spayed female Cavalier King Charles Spaniel dog was presented to the Veterinary Teaching Hospital because of recurrent chronic abscesses on the distal pelvic limbs, fever, lethargy, lameness of unknown etiology, and chronic pancreatitis. Sterile nodular panniculitis was diagnosed after an extensive workup, and the dog initially responded to immunosuppressive therapy, but relapse and spread of cutaneous lesions and acute lameness occurred after 11 mo, and euthanasia was elected. Postmortem examination confirmed hyalinizing pancreatic adenocarcinoma with pancreatitis, panniculitis, polyarthritis (PPP), and osteomyelitis. Histopathology and bacterial and fungal cultures were supportive of a sterile process, specifically the PPP syndrome, which is a rare, potentially life-threatening, systemic manifestation of pancreatic disease in both people and animals. To our knowledge, a clinicopathologic description of a hyalinizing pancreatic adenocarcinoma associated with this rare syndrome has not been reported previously in a dog.
Keywords
Pancreatitis, panniculitis, and polyarthritis (PPP) syndrome is a recognized, yet rare, clinical manifestation in people affected by chronic pancreatic disease or pancreatic neoplasia.1,4,6,7,9,11,12,15,16 PPP syndrome is primarily reported in humans and describes the typically targeted anatomic sites. Dermatologic lesions of PPP syndrome include erythematous, painful nodules developing predominantly on the distal extremities and trunk concurrently with pancreatic disease (inflammation, neoplasia, pseudocysts) and periarticular and/or intra-osseous involvement. 1 The pathogenesis of this syndrome is poorly understood but is believed to involve the release of pancreatic enzymes (trypsin, lipase, amylase, phospholipase A) into the circulation, resulting in fat necrosis at various sites and secondary inflammation. This condition in people has a mortality rate of ~24%, especially when diagnosis and treatment are delayed. 10
In the veterinary literature, although there are several reports of panniculitis associated with pancreatitis and pancreatic neoplasms (pancreatic exocrine adenocarcinoma, pancreatic adenoma), cases of PPP syndrome are scarce,5,17 and we found no cases of this entity associated with the rare hyalinizing variant of exocrine pancreatic cancer in a comprehensive search of Google, PubMed, CABI Direct, Web of Science, and Scopus, using search terms “hyalinizing”, “pancreatic carcinoma”, “dog”, and “polyarthritis”, suggesting that these entities have not been reported in association in the dog. More commonly, animals are diagnosed with sterile nodular panniculitis (SNP), which is described as noninfectious inflammation of the subcutaneous fat.2,5,10,12,17 In cases of SNP, animals commonly have acute onset of solitary-to-multiple, often non-ulcerated, nodules and are usually systemically healthy, but concurrent diseases such as pancreatitis or polyarthritis may be noted on initial presentation. Nonspecific systemic clinical signs may include lethargy, fever, lameness, weight loss, and gastrointestinal disturbances. Treatment is typically lifelong immunosuppression with glucocorticoids and steroid-sparing immunomodulatory medications.
A 10-y-old spayed female Cavalier King Charles Spaniel dog was presented to the Auburn University Veterinary Teaching Hospital (Auburn, AL, USA) emergency service (day 0) because of a 2-wk history of non-resolving medial patellar luxation with an associated draining tract on her left stifle and a 3-d history of anorexia. Treatment attempted prior to referral included carprofen, prednisolone, and gabapentin without improvement. The dog had previously been diagnosed with chronic pancreatitis of many years’ duration and, 8 mo prior, an abscess on the right forelimb had resolved with an unidentified injectable antibiotic.
Relevant findings during physical examination included bilateral stifle pain with a grade 2 of 5 lameness, a 2 × 2-cm erythematous nodule on the right tarsus, and erythematous nodules with draining tracts on the left stifle and dorsal intrascapular region (Fig. 1A). An infectious etiology with systemic dissemination was suspected. Repeated aerobic, anaerobic, and fungal tissue cultures of the right tarsal and left stifle nodules yielded no growth. Blastomyces sp. urine antigen testing (MiraVista), and culture and PCR testing for Bartonella spp., were negative. Histopathology of the biopsied nodules was consistent with marked, chronic-active, hemorrhagic and suppurative cellulitis, and no organisms were highlighted with Gram, GMS, Fite, or Ziehl–Neelsen stains. However, it was reported that idiopathic sterile panniculitis was an unlikely differential due to the lack of pyogranuloma formation. A CBC revealed moderate leukocytosis with moderate neutrophilia, significant left shift, and moderate monocytosis. Chemistry revealed mild hypoalbuminemia, mild hyperglobulinemia, mildly decreased urea and creatinine, and slightly elevated glucose concentrations. These findings were consistent with systemic inflammation likely related to chronic-active pancreatitis and/or infectious disease. Abdominal ultrasound revealed a heterogeneous, markedly enlarged, and lobular left limb of the pancreas, supportive of chronic pancreatic disease, with several ill-defined hyperechoic nodules, interpreted as nodular hyperplasia, as well as ovoid anechoic cysts, deemed either retention cysts or pseudocysts at the time. The liver was hypoechoic, but of expected size and associated with unremarkable liver enzyme (alanine transaminase, aspartate transaminase) activities and total bilirubin concentrations at the time of ultrasound.
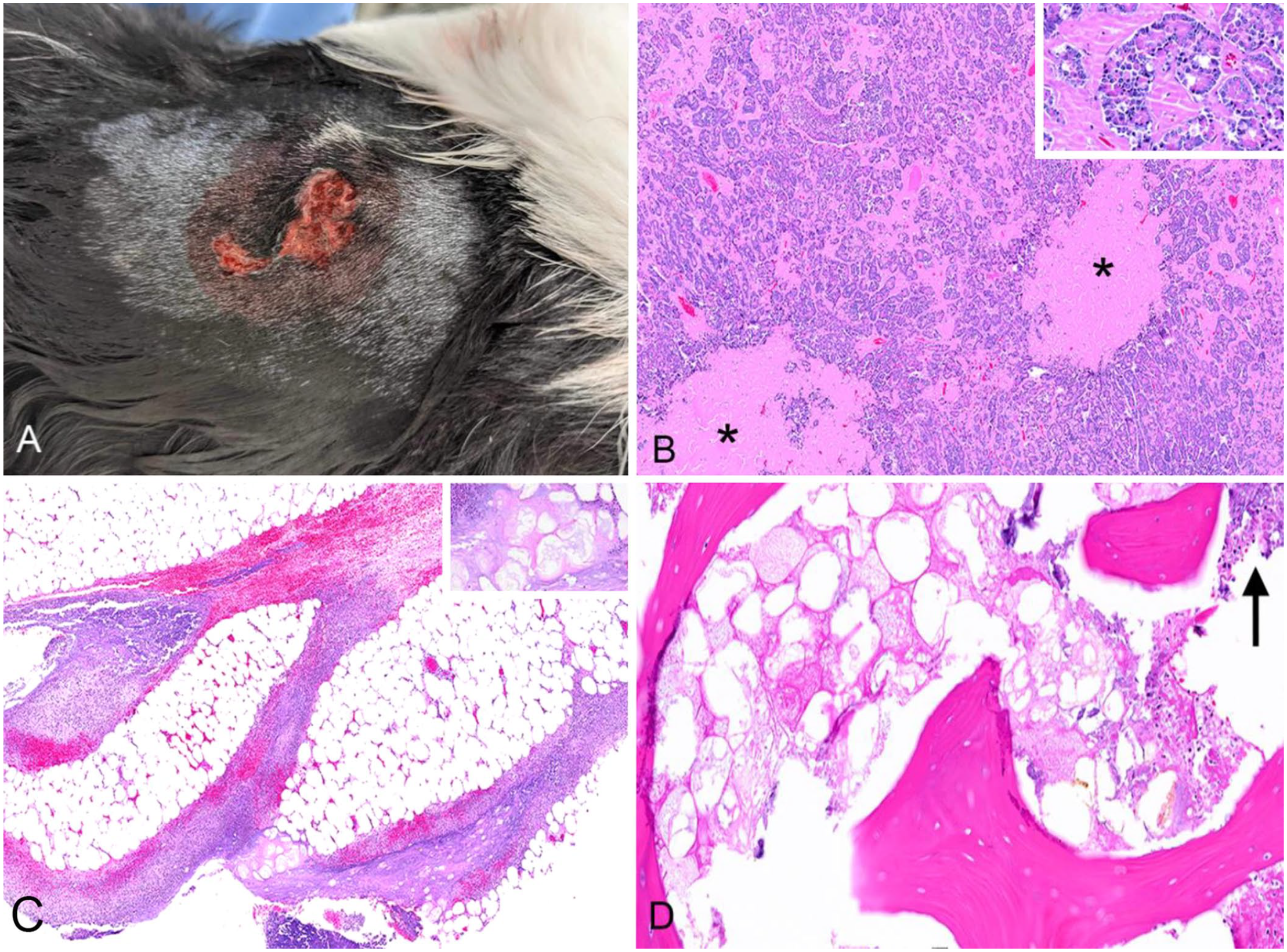
Pancreatitis, panniculitis, and polyarthritis syndrome in a dog.
The dog was hospitalized and initially managed medically with antibiotic therapy for presumptive infectious cellulitis and polyarthritis. The dog was treated with adjunctive fluorescence photobiomodulation (Phovia; Vetoquinol) and K-laser (LiteCure CTX; Companion Animal Health) treatment (10.80 J) to treat tissue inflammation and discomfort. During hospitalization, the patient developed new cutaneous nodules along the right shoulder and dorsum, and bilateral carpal swelling. Cytology of a fine-needle aspirate (FNA) from the new lesions revealed marked neutrophilic inflammation with lesser macrophagic inflammation and no microorganisms. The patient was discharged home (day 11) with ongoing medications including itraconazole, prednisone, enrofloxacin, amoxicillin–clavulanic acid, and codeine to treat for presumptive infectious disease while awaiting additional culture and histopathology results.
Over the next 4 wk, the cutaneous tarsal and stifle nodular lesions remained, abscesses developed on the left hip and left lateral thorax, and the patient was limping. On recheck (day 33), the patient was sedated, the skin was clipped and aseptically prepared, and a syringe and needle were used to collect >30 mL of purulent, sanguineous exudate for repeated aerobic, anaerobic, and fungal cultures, all of which yielded no growth. The original biopsy over the right tarsus was submitted for a second opinion, with a similar morphologic diagnosis and interpretation, including the possibility of sterile polyarthritis and panniculitis associated with pancreatitis. Based on these findings, antimicrobial medications were discontinued, and immunomodulatory therapy was initiated with prednisolone and cyclosporine for the treatment of suspected SNP associated with chronic pancreatitis (day 59). Over the next 30 d, all lesions resolved completely with new hair growth, except for the right dorsal lumbar area, which reduced to a 0.5-cm firm dermal nodule. Limping resolved, and appetite returned to normal. At the recheck examination (day 94), owners were instructed to perform a tapering withdrawal of the prednisone, but cyclosporine was maintained.
Five months later (day 334), a 6 × 4-cm firm nodule developed on the dorsal left shoulder along with intermittent pelvic limb lameness. Cytology revealed pyogranulomatous inflammation with no organisms, consistent with recurrence of SNP. Treatment with prednisolone and cyclosporine was reinstituted, but lameness of the right thoracic limb ensued when prednisolone was reduced. On recheck (day 367), radiographs of this limb revealed periosteal reaction of the ulna with joint involvement, suggestive of bacterial osteomyelitis or neoplasia. Hemorrhagic fluid collected via arthrocentesis yielded no growth on aerobic and anaerobic cultures, and cytology was inconclusive. Three days later (day 370), the patient was admitted for acute lameness in the pelvic limbs and inability to ambulate. Due to quality-of-life concerns, euthanasia was elected followed by postmortem examination.
On gross examination, multiple up to 3.5 × 2.5-cm areas of dark-red, variably edematous subcutis and fascia were over the right tarsus, left dorsal carpus, antebrachium, and lateral tibia, often accompanied by pockets of brown, thick, turbid fluid, which yielded no growth on aerobic and anaerobic bacterial cultures. The synovium of the left tarsal and left stifle joints had numerous light-red, villous projections. The left distal femoral epiphysis had an irregular, rough surface, and amorphous brown-to-tan trabecular bone.
Arising from the pancreas and loosely attached to the colonic mesentery was a 4.5 × 4 × 5-cm amorphous, multilobulated, tan, soft mass with a cavitated center containing brown turbid fluid. Multifocally scattered throughout the peripancreatic mesentery and greater omentum were up to 2-mm, discrete, raised, white-to-tan, firm-to-gritty plaques.
Histopathology of the pancreatic mass revealed pancreatic parenchyma compressed by a multilobular, moderately cellular, partially encapsulated neoplasm composed of polygonal cells arranged in acini and tubules and supported by a moderate amount of fibrovascular stroma that was markedly expanded by lakes of amorphous hyaline material (not highlighted with Congo red staining; Fig. 1B). Extensive areas of necrosis encompassed ~50% of the examined neoplasm and multifocally extended into the surrounding peripancreatic adipose tissue. Histopathology confirmed coalescing-to-extensive necrosuppurative panniculitis and myofasciitis of the left pelvic limb (Fig. 1C), necrosuppurative arthritis of the left carpal and left stifle joints, and necrosuppurative osteomyelitis of the left femur with bone marrow fat necrosis (Fig. 1D). The final diagnosis was a hyalinizing pancreatic adenocarcinoma with attendant inflammation, secondary panniculitis, polyarthritis, and osteomyelitis.
SNP is an idiopathic, immune-mediated condition for which medical management utilizing immunomodulatory agents, such as glucocorticoid therapy (i.e., prednisone) and lymphocyte inhibitors (e.g., cyclosporine, azathioprine), is the mainstay of treatment. Most cases require life-long immunoregulatory therapy. The disease may be primary or associated with other conditions in people and dogs, most notably pancreatic disease. Although the pathogenesis has not been fully elucidated, it is speculated that the release of pancreatic enzymes may lead to fat necrosis and the inflammation seen in panniculitis cases that occur secondary to pancreatic lesions.
In our case, a history of chronic pancreatitis was noted upon initial presentation, along with pancreatic changes on abdominal ultrasound. As the findings on abdominal ultrasound were nonspecific for neoplasia versus inflammation (i.e., pancreatitis), diagnosis of the hyalinizing pancreatic adenocarcinoma was more difficult and affected our treatment outcomes. In fact, the ultrasound appearance of numerous pancreatic diseases overlaps and, in some cases, there may be no gross pancreatic changes despite histologic pancreatic disease. 8 Biopsy for histologic evaluation is the most definitive means to diagnose pancreatic neoplasia; however, assorted diseases affecting the pancreas can have uneven or segmental distribution, and non-representative samples can delay or impede diagnosis. 8 In our case, repeated abdominal ultrasound was discussed with the clients but not pursued due to the initial improvement in standard-of-care immunomodulatory therapy for SNP. It is unknown if the hyalinizing adenocarcinoma was the cause of the initial disease or if it developed independently of ongoing pancreatitis. The veterinary literature reports a median survival time of 1 d (range: 0–51 d) with exocrine pancreatic adenocarcinomas without chemotherapy, mostly due to euthanasia either intraoperatively or shortly after confirming the diagnosis due to the notoriously poor prognosis. 13 In one report of hyalinizing pancreatic adenocarcinoma in 6 dogs, 2 patients survived >15 mo after diagnosis, 1 of which did not receive treatment, suggesting that it may be less biologically aggressive than non-hyalinizing exocrine pancreatic carcinoma. 2 Four dogs had radiographic evidence of a pancreatic mass. 2 Interestingly, 2 dogs had panniculitis as a diagnosis, although a thorough case description and diagnostic workup were not discussed to delineate the inflammatory nature of the disease. 2
Consideration for more advanced imaging including computed tomography or magnetic resonance imaging may be beneficial when determining the extent of pancreatic and extra-pancreatic changes when panniculitis and polyarthritis are present. In people, extra-pancreatic manifestations include osteolysis, osteopenia, periosteal reaction, avascular intramedullary fat necrosis in the bone marrow, and overlying soft tissue edema. 14 For cases lacking evidence of pancreatic disease, a more aggressive clinical approach involving FNA of the pancreas, in addition to biopsy, may allow for a more accurate diagnosis. In people, there is a <1% risk of tumor needle-tract seeding along biopsy and FNA tracts, suggesting that it is a safe diagnostic procedure. 3 In one case of hyalinizing pancreatic adenocarcinoma in a dog, FNA of the pancreatic lesion revealed normal pancreatic tissue; hence, biopsy may be warranted when neoplasia is suspected. 2
Medical management, client expectations, and patient prognosis are significantly variable in cases of nodular panniculitis given the numerous etiologic factors resulting in this condition (e.g., infections, sterile inflammation, neoplasia), the extensive diagnostic workup, and the financial obligation to the client. Veterinarians should be aware of the association of SNP and pancreatic disease, particularly pancreatic neoplasia, and take a more proactive diagnostic and management approach in dogs with a history of pancreatic disease, especially if medical management fails.
Footnotes
Acknowledgements
We thank Dr. Pete Christopherson for his guidance with cytologic diagnosis of pancreatic adenocarcinoma; Dr. Noelle Bergman for her guidance with diagnosis, treatment, and prognosis for pancreatic neoplasms; Drs. B.L. Rasche, K. Beguesse, and K. Linder at North Carolina State Veterinary Hospital Diagnostic Laboratory System for their histopathology consultation service on the original biopsied skin; and the histopathology laboratory at Auburn University for slide preparation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.