
Abstract
A 12-y-old castrated male domestic longhaired cat had progressive paraparesis and neurolocalization of L4–S3. MRI revealed a circumscribed intradural-extraparenchymal mass from L5 to S1 that was T2 and short tau inversion recovery hyperintense and strongly contrast-enhancing. Cytologic interpretation of a blind fine-needle aspirate obtained through the L5–L6 space was a tumor of probable mesenchymal origin. A pair of suspect neoplastic cells was seen on a cytocentrifuged preparation of the atlanto-occipital CSF sample, despite a normal nucleated cell count (0 × 106/L) and total protein (0.11 g/L) with only 3 RBCs × 106/L. Clinical signs progressed despite increasing doses of prednisolone and cytarabine arabinoside. Repeat MRI on day 162 demonstrated tumor progression from L4 to Cd2 vertebral segments with intraparenchymal extension. Surgical tumor debulking was attempted, but an L4–S1 dorsal laminectomy revealed diffusely abnormal neuroparenchyma. Intraoperative cryosection favored lymphoma, and the cat was euthanized intraoperatively 163 d following presentation. Postmortem examination was performed, and the final diagnosis was a high-grade oligodendroglioma. This case illustrates the cytologic, cryosection, and MRI features of a unique clinical presentation of oligodendroglioma.
Oligodendrogliomas are rare in cats, occurring mostly within the brain, with infrequent reports of a spinal cord location.3,4,8,12–14 Feline spinal glial tumors have a low prevalence with a rate of 9.4% of all spinal tumors, of which lymphoma is the most common. 8 Reports on feline spinal cord tumors support a predilection for spinal gliomas to form within the cervical segments; a retrospective study of feline gliomas, with 7 oligodendroglial tumors, indicated only 1 tumor located within the lumbar spinal cord segments, L5–L7.4,8,12
A 12-y-old castrated male domestic longhaired cat was presented to the Cornell University Hospital for Animals (CUHA; Ithaca, NY, USA) emergency service (day 1) for evaluation of a 1-wk history of tail paralysis and paraparesis, and 1-mo history of reduced jumping and climbing. Past pertinent medical history included 2 episodes of urinary obstruction within 2 wk of presentation. Referral radiographs of the lumbar spine taken 4 d prior were reportedly unremarkable.
General physical examination was unremarkable. Neurologic examination revealed ambulatory paraparesis with marked plantigrade stance, reduced hopping in the pelvic limbs, reduced extensor postural thrust, and reduced muscle tone in the pelvic limbs. Segmental reflexes were intact. The tail was paralyzed and flaccid with absent pain sensation. Pain was elicited on caudal lumbar spinal palpation. The patient’s neurolocalization was L4–S3. Differential diagnoses included trauma such as “tail pull” injury, neoplasia, and intervertebral disc herniation.
Diagnostic and therapeutic recommendations were made, and the owners elected conservative management without further testing. Therefore, an injection of meloxicam was administered, and the cat was discharged with meloxicam (0.1 mg/kg PO q24h), gabapentin (20 mg/kg PO q8 12h as needed), and instructions for 4-wk cage rest. Three days later, meloxicam was discontinued, and prednisolone was initiated (0.7 mg/kg PO q12h) because of the progression of paraparesis. Although the cat’s paraparesis improved, the tail remained paralyzed.
The owners later elected to pursue testing and brought the cat to the CUHA neurology service (day 64). Results of a CBC (ADVIA 2120i; Siemens) with blood smear examination revealed eosinopenia attributed to prednisolone administration (1.4 mg/kg daily). Total protein by refractometry was moderately increased at 88 g/L (RI: 59–75 g/L), which may have been the result of the slight lipemia and/or possible hyperfibrinogenemia. Chemistry (Cobas c501 analyzer; Roche) revealed decreased alanine aminotransferase and lactate dehydrogenase activities and mildly increased lipase activity and total iron-binding capacity, considered clinically insignificant. Lumbosacral MRI (1.5T scanner, Vantage Atlas; Canon Medical Systems) revealed a right-sided, intradural-extraparenchymal mass, causing compression and displacement of the spinal cord and cauda equina at L6 and L7. The mass had thin, lobular-to-fimbriated extensions spreading from L5 to S1, partially surrounding the spinal cord and cauda equina. The entire abnormality was circumscribed, homogeneously T2 and short tau inversion recovery (STIR) hyperintense to muscle, T1 isointense to spinal cord, and strongly contrast-enhancing (Fig. 1A). These findings were most consistent with an intradural-extraparenchymal neoplasm, with meningioma or lymphoma prioritized.
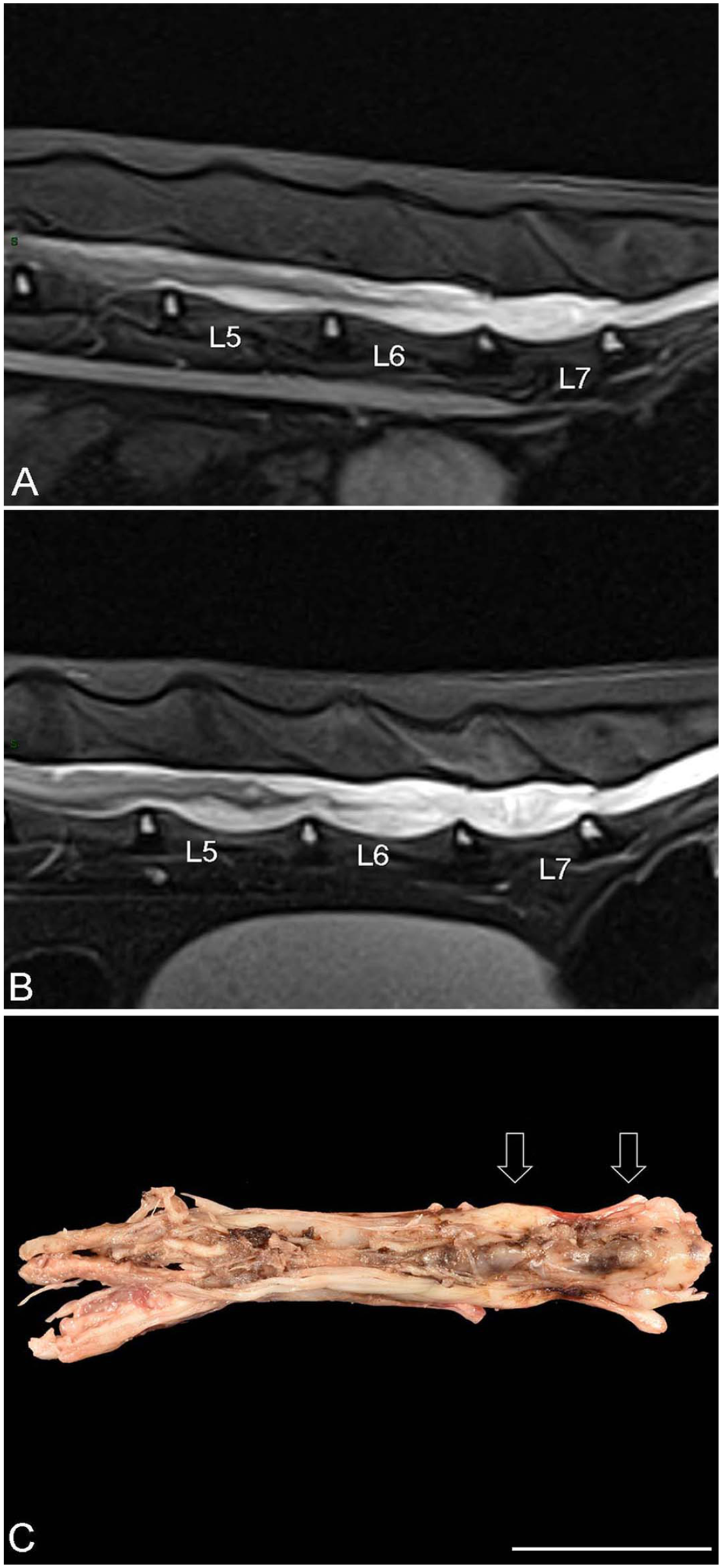
Progression of the lumbosacral neoplasm on MRI (A, B) and at postmortem examination (C).
Given the extensive mass at the L5–L6 space, a blind fine-needle aspirate (FNA) was obtained utilizing the anatomic landmarks for lumbar CSF collection. The spinal needle was redirected, and very light suction was applied. One smear was highly cellular, consisting of a homogeneous neoplastic-cell population present individually and in aggregates on a moderately bloody background with occasional free nuclei. Cellular aggregates were frequently associated with bright pink wispy extracellular matrix (Fig. 2A, 2B). The neoplastic cells were oval to rarely stellate with a moderate-to-high nuclear-to-cytoplasmic (N:C) ratio. The deep-blue grainy cytoplasm often contained small clear discrete vacuoles. Cell borders were variably distinct, often with blebbed margins. The paracentral-to-eccentric nuclei were round-to-oval with coarsely clumped chromatin and an indistinct nucleolus. Anisocytosis and anisokaryosis were moderate, with frequent binucleation and rare mitotic figures. There was subtle windrowing of the background blood, indicating mild viscosity. The cytologic interpretation was a tumor of probable mesenchymal origin. Meningioma was prioritized; however, the cells also had features of a neuroendocrine tumor. Considerations for the pink extracellular matrix included mucopolysaccharide secretory material, as has been described in meningiomas, 2 or possibly osteoid (from an osteosarcoma).

Representative photomicrographs of the fine-needle aspirate (FNA) of the lumbosacral mass (A, B) and cytocentrifuged smear prepared from the CSF (C). Wright stain.
Analysis of an atlanto-occipital CSF sample revealed a normal nucleated cell count (0 × 106/L) and total protein (0.11 g/L) with 3 RBCs × 106/L. A cytocentrifuged smear of the fluid was of low cellularity, consisting of mostly large mononuclear cells and one small lymphocyte with a few erythrocytes. A single pair of small, somewhat cohesive oval cells with a moderate N:C ratio, deep-blue cytoplasm, and a fragmented, eccentric nucleus were noted (Fig. 2C). The chromatin appearance was postulated to represent prophase of mitosis. These cells were suspected to be neoplastic cells given their similar morphologic appearance to those seen in the mass aspirate.
Despite the cytologic findings, a diagnosis of lymphoma was prioritized based on the patient’s signalment and clinical course. Treatment options were discussed, and chemotherapy was elected. The cat was treated with 2 doses of cytarabine arabinoside (Cytosar; Pfizer; 200 mg/m2 each) administered as a single SC dose 4 wk apart. By day 162, the owners elected to pursue surgery given the patient’s progressive paraparesis; therefore, staging and repeat MRI were performed. Neurologic examination revealed paraplegia with intact pain sensation, and a tail with regained pain sensation that remained plegic. Three-view thoracic radiographs and abdominal ultrasound showed no evidence of metastasis. MRI revealed the mass now extended from L4 to Cd2 (Fig. 1B). The mass-like component remained predominantly intradural-extraparenchymal. New findings included intraparenchymal extension causing progressive effacement of the parenchyma and wispy contrast-enhancing projections coalescing with the cord. The cranial extension of the tumor was eccentric and superficial, involving the meninges and peripheral spinal cord. The caudal extension enveloped the cauda equina. Signal characteristics and contrast enhancement were unchanged. The differential diagnoses of lymphoma or meningioma were maintained.
A dorsal L5–S1 laminectomy was performed (day 163). Intraoperatively, focal regions of the lamina were noted to be abnormally thin. The spinal cord was diffusely abnormal with a mottled dark-brown to red, expansive, firm, and fatty-textured appearance. An intraoperative sample was submitted for cryosectioning. The cryosections revealed a mixed round- and spindle-cell population with variable amounts of cytoplasm, round-to-oval nuclei, finely stippled chromatin, and an inapparent nucleolus (Fig. 3A). Atypia was moderate with no mitotic figures noted. The histologic interpretation was a poorly differentiated tumor, with lymphoma favored. Given the cryodiagnosis and the advanced stage of the cat’s disease, intraoperative euthanasia was performed.
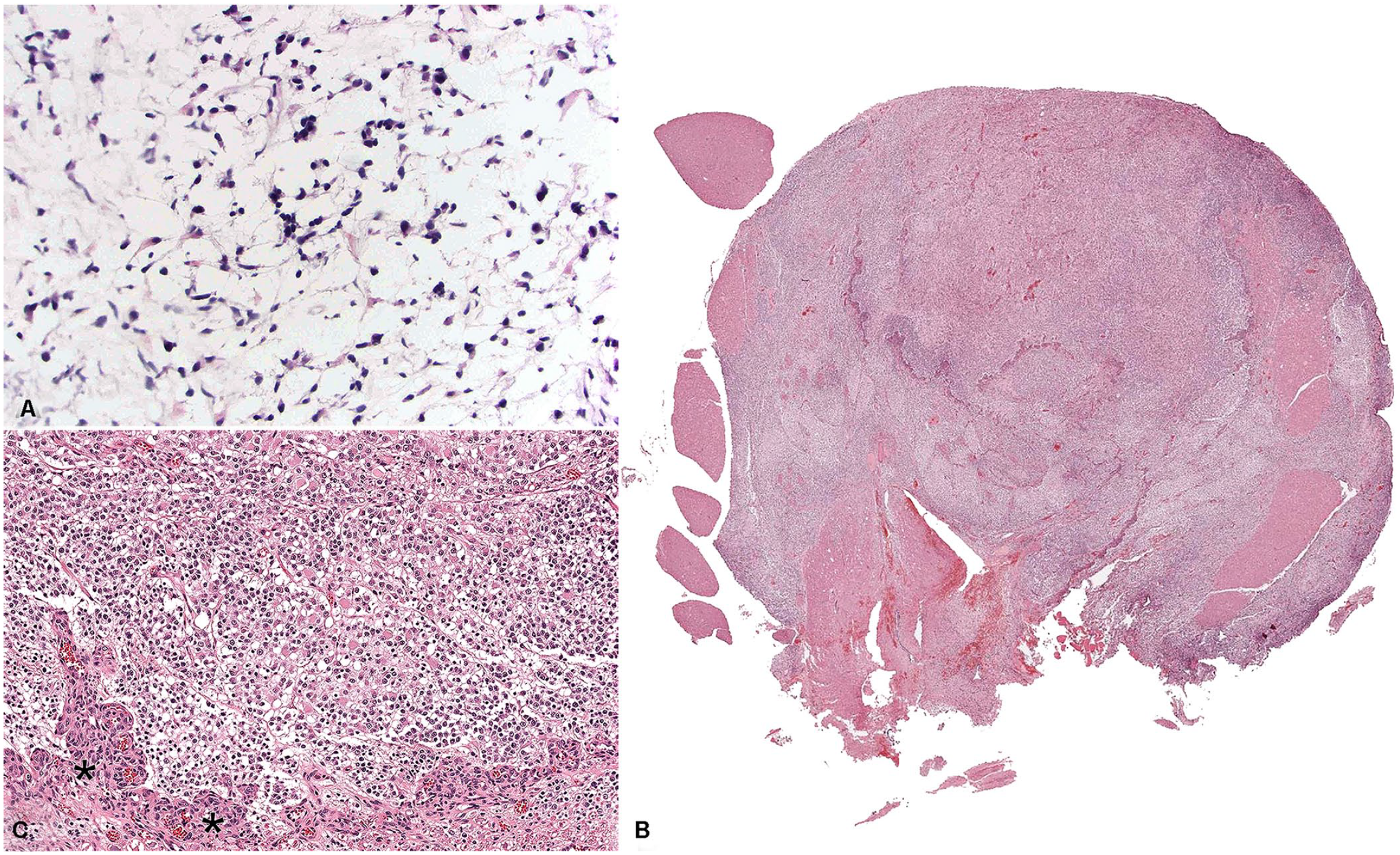
Transverse section of the lumbar spinal mass, cryosection (A) and H&E (B, C).
On postmortem examination, the mass markedly distorted the L5–S1 segment, with no overt evidence of peripheral nerve root involvement (Fig. 1C). Upon serial sectioning, marked, indiscriminate neoplastic infiltration of both the gray and white matter occurred in the affected segments with extension along the nerve roots (Fig. 3B). The neoplasm consisted of tightly packed sheets of neoplastic glial cells with abundant oligodendrocytic and lesser astrocytic morphology, all supported by a faint fibrovascular stroma (Fig. 3C). Approximately 50% of the astrocytes had gemistocytic morphology. Neoplastic cells were often loosely embedded within an abundant mucinous matrix. Several areas of the neoplasm had large arcades of microvascular proliferation. Mitoses were frequent, and rare scattered areas of necrosis were present. The histologic diagnosis was a high-grade oligodendroglioma. This was supported by the immunohistochemistry (IHC) results, in which ~85% of the neoplastic cells had strong nuclear immunolabeling to oligodendrocyte lineage transcription factor 2 (Olig2, for neoplastic glial cells); scattered neoplastic cells had moderate-to-strong cytoplasmic immunolabeling for glial fibrillary acidic protein (GFAP, for astrocytes).
In addition to the atypical lumbosacral location, this oligodendroglioma had an unusual infiltrative progression seen on MRI. Although most gliomas are primarily intraparenchymal tumors, extraparenchymal and intradural tumor extension has been reported. 12 However, extension of these tumors in a reverse manner, as seen in our case, is not typical. The cat had a slowly progressive clinical course, unlike most patients with glial tumors who decline rapidly. Our patient appeared most responsive to high-dose (> 1 mg/kg daily) glucocorticoid administration. Previous reports have most frequently described euthanasia at the time of diagnosis of glial tumors, with a few describing an unsatisfactory response to steroid trials before euthanasia.1,4,9
Surgical subtotal resection was attempted based on favorable imaging characteristics and the patient’s progressive disease. Given the highly invasive process described herein and reported elsewhere for feline glial tumors, spinal gliomas are generally considered poor candidates for surgical excision. 4 The inclusion of an oligodendroglioma in either the MRI or cytologic differentials would have led to the recommendation of radiation therapy over surgical debulking.
Although oligodendrogliomas have a classic description on gross and histologic evaluation, a cytologic description of a Wright-stained FNA of the tumor is lacking in the literature.3,4,6,10–12,14 For predominantly intracranial tumors such as oligodendrogliomas, clinical pathologists are often limited to reports describing a few cells in the CSF. 3 The neoplastic cells in one such report of 2 cats had similar morphologic features to the rare suspected neoplastic cells seen in the CSF sample from our case. These features include cells often in pairs with an eccentrically placed round nucleus and deeply basophilic cytoplasm. 3 Unfortunately, these cells are difficult to distinguish from surface epithelial cells, which can be seen as an incidental finding in CSF. 16 CSF results from other reported canine and feline oligodendrogliomas range from normal to neutrophilic pleocytosis to albuminocytologic dissociation.5,8
The only prior cytologic description of this tumor was in a study that utilized H&E staining, 15 which does not match the tinctorial properties of Wright staining, as evidenced by their description of eosinophilic cytoplasm, versus the deep-blue grainy cytoplasm seen in our case. The prior study described numerous blood vessels and capillary tufts as a consistent and distinctive feature of oligodendrogliomas, which, although seen in the formalin-fixed histopathologic sections in our case, were absent in the cytologic smear, likely given the study’s squash preparations of surgical biopsy samples, compared to our FNA. Grossly, oligodendrogliomas are often soft and gelatinous, and pools of lightly basophilic amorphous mucinous matrix are seen histologically.3–6,11,12,14 This explains the extracellular matrix that we observed cytologically, as well as the subtle windrowing of erythrocytes reflecting sample viscosity. These characteristic cytologic findings can aid clinical pathologists in the diagnosis of oligodendrogliomas given that a mucinous matrix is a common feature of this CNS tumor. 15
Cryosection also proved challenging to recognize and diagnose an oligodendroglioma. Histologically, the neoplastic cells in oligodendrogliomas are described as having a honeycomb or fried-egg appearance given a halo of clear cytoplasm identified by a thin cytoplasmic margin.3–6,11,12,14 This appearance is considered an artifact of sample processing or autolysis because it is absent in fresh samples. 6 This likely explained our discordant initial cryodiagnosis. In the study of H&E-stained squash preparations of fresh tissue, 15 the neoplastic cells were described as small, round, and closely packed, which also differs from the classic histologic description of oligodendrogliomas. 6 The morphologic appearance between fresh and cryosections versus formalin-fixed tissue is important for anatomic pathologists to note, given that densely packed neoplastic cells arranged in sheets mimic lymphoma, the most common feline spinal tumor.
Given that glial tumors can be variable in appearance and share morphologic features with other CNS tumors, adjunctive IHC panels are recommended. 12 Oligodendrogliomas are typically positive for Olig2 and negative for GFAP. 12 Although there was positive labeling for both in our case, the neoplastic oligodendrocytes far outnumbered the neoplastic astrocytes, thereby enabling the diagnosis of oligodendroglioma rather than an undefined glioma. The infiltrative nature, histopathologic features, and microvascular proliferation of our patient’s oligodendroglioma provided the criteria for a high-grade tumor designation, extrapolated from the human and canine glioma classification schemes.6,7
It is important to keep oligodendroglioma on the differential list for a lumbosacral spinal tumor and to recognize the described unique imaging, cytologic, and cryosection features, given that this tumor calls for a different treatment approach than lymphoma and meningioma, which are the more common feline spinal tumors.
Footnotes
Acknowledgements
We thank the senior student on the case, Laura Marti, for her contributions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.