
Abstract
Protothecosis, an infectious disease caused by the green algae Prototheca zopfii and P. wickerhamii, occurs sporadically in domestic animals and humans. Diagnosis of CNS protothecosis is based on neurologic signs that indicate multifocal nervous system lesions and that follow a period of chronic diarrhea and weight loss, cytologic observation of algae in fecal culture or histopathology, and detection of the agent by PCR assay of infected tissues. Here, we report a case of a paraparetic dog with CNS protothecosis that was diagnosed definitively antemortem using CSF cytology, PCR, and DNA sequencing. A 4-y-old mixed-breed dog developed progressive paraparesis that followed weight loss and diarrhea. CSF analysis revealed marked eosinophilic pleocytosis. Prototheca organisms were detected by microscopic examination of the CSF, and speciated as P. zopfii by CSF PCR and DNA sequencing. Other possible causes of paraparesis were ruled out using computed tomography, serology, and CSF PCR. The dog’s condition deteriorated despite treatment, developing forebrain and central vestibular system clinical signs, and it was euthanized at the owner’s request. Postmortem examination was declined. Our findings indicate that when CNS protothecosis is suspected, antemortem diagnosis can be made using CSF analysis and a PCR assay.
Protothecosis is a sporadic infectious disease that has been reported in domestic animals and humans.10,11,16 It is caused by unicellular, achlorophyllous algae of the genus Prototheca, particularly Prototheca zopfii and P. wickerhamii, which are ubiquitous in the environment.16,17 Infection likely occurs through ingestion, mucosal contact, or traumatic inoculation from contaminated sources. The algae enter the body through the mouth or nose, initially causing intestinal infection, which may then spread to the eye, CNS, and kidneys.16,17 Disseminated protothecosis is the most common form in dogs, most frequently involving P. zopfii. 16
The neurologic signs of canine protothecosis usually include lethargy, behavioral abnormalities, paresis, head tilt, cervical pain, circling, ataxia, and seizures.6,10,12,13 The prognosis for a case of disseminated protothecosis is poor, and the diagnosis often leads to euthanasia. 14 The algae can be detected by rectal scrape, urine sediment examination, fecal flotation, histopathology, or culture of infected tissues.16,17 Definitive diagnosis is often made postmortem using PCR, followed by DNA sequencing for speciation.10,12
A 4-y-old, mixed-breed, castrated male outdoor dog, from a rural area in northern Israel with access to a nearby river, was presented to the referring veterinarian with progressive hindlimb ataxia and weakness of 5-wk duration. Eight weeks before presentation, the dog had had mild diarrhea, which resolved spontaneously. Neurologic examination revealed paraparesis with normal spinal reflexes, localizing the lesion to the T3-L3 spinal cord segments. Computed tomography (CT; 16-slice MX 8000 IDT, Philips) of the entire spine was unremarkable, including after IV administration of contrast medium (iopromide, Ultravist 300; Bayer). The serum indirect immunofluorescent antibody test (indirect IFAT) for Neospora caninum 5 was positive (titer, 1:800; cutoff titer, 1:50); indirect IFATs were negative for Toxoplasma gondii 7 and Brucella canis (Dot-ELISA, ImmunoComb canine Brucella antibody test kit; Biogal-Galed). 14 The dog was tentatively diagnosed with acute myelitis, resulting from either intraspinal Spirocerca lupi migration or neosporosis, and was treated with doramectin (400 µg/kg/d SC q24h for 4 d), 3 prednisone (1 mg/kg/d PO q12h), and clindamycin (12.5 mg/kg/d PO q12h). Clinical signs improved initially; however, the dog relapsed and was admitted to the Hebrew University Veterinary Teaching Hospital with severe paraparesis and proprioceptive ataxia of the hindlimbs.
The dog had a history of inappetence and weight loss; physical examination was unremarkable except for diffuse hyperesthesia upon palpation of the thoracolumbar spinal column. Neurologic examination was unremarkable, except for ambulatory paraparesis, and the lesion was again localized to the T3-L3 spinal cord segments. Differential diagnoses included infectious myelitis, immune-mediated myelitis, and spinal cord neoplasia. Although common in Israel,2,3 aberrant S. lupi migration was considered less likely given the chronic course of the disease and lack of response to doramectin treatment. Hematologic abnormalities included mild leukocytosis (22.6 × 109/L; RI: 5.2–13.9 × 109/L), with neutrophilia (neutrophils, 20 × 109/L; RI: 3.9–8.0 × 109/L) and lymphopenia (lymphocytes, 0.94 × 109/L; RI: 1.3–4.1 × 109/L). Serum chemistry abnormalities included increased activities of alanine transaminase (11.67 µkat/L; RI: 0.32–1.12 µkat/L) and aspartate transaminase (9.37 µkat/L; RI: 0.35–2.84 µkat/L), hyperalbuminemia (albumin, 45 g/L; RI: 30–44 g/L), and borderline hypocalcemia (total calcium, 2.35 mmol/L; RI: 2.42–2.88 mmol/L). Urinalysis, including sediment examination, was normal.
Analysis of CSF collected by cisternal puncture revealed marked mixed pleocytosis (total nucleated cells, 1,200 × 106/L; RI: 0–5 × 106/L) composed of monocytes (54%), some of which were reactive macrophages, eosinophils (24%), lymphocytes (14%), and neutrophils (8%) and increased total protein concentration (1.59 g/L; RI: <0.25 g/L). Additionally, oval morula-like organisms of 6–10 × 3–6 µm, each with a thin halo suggestive of a capsule and granular basophilic cytoplasm, were detected (Fig. 1, black arrows). These were consistent with Prototheca sporangia, and their oval shape with P. zopfii.10,13 In addition, free, thin, rod-like, 1–3-µm organisms, some of slightly curved shape, were detected within the cytoplasm of reactive macrophages (Fig. 1, red arrows) and were interpreted as sporangiospores. 12 Results of repeated serum indirect IFAT for N. caninum, 2 wk after the first test, remained stable at 1:800.
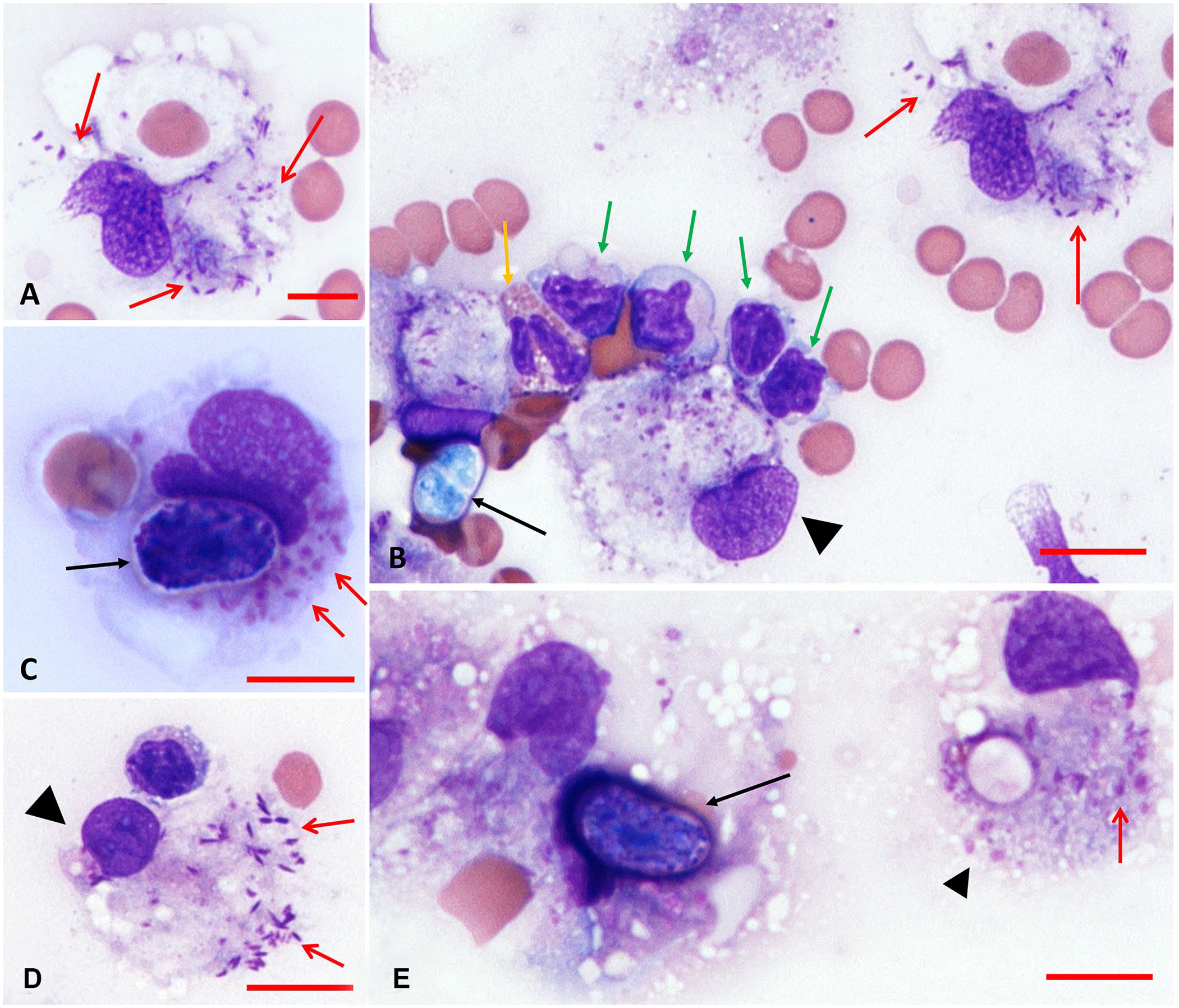
CSF cytologic findings in a dog with CNS protothecosis, with mixed inflammatory cell pleocytosis, consisting of monocytes, reactive macrophages (
DNA was extracted from CSF (DNeasy blood & tissue kit; Qiagen) following the manufacturer’s instructions. Molecular characterization was performed using primers 18PZF1 (3′-ACAATACGTAGCGATGCCGAACT-5′) and 18PZR2 (3′-GCCAGCCAGAGGACGCCGAA-5′), which amplify partial sequences of the Prototheca spp. 18S rRNA gene, 15 and primers Pro-28S-F (3′-TGGGAATGCAGCTC TAAGCC-5′) and Pro-28S-R (3′-GAAGGATCGACGAG TCCACG-5′), which were designed for our study to amplify a segment of the Prototheca spp. 28S rRNA gene. The primers were designed with Primer-BLAST 19 (http://www.ncbi.nlm.nih.gov/tools/primer-blast) using 28S sequences of various Prototheca spp., including P. zopfii (MH374899.1) and P. wickerhamii (KX828712.1).
Real-time PCR was performed in a total volume of 20 μL, containing 4 μL of DNA (19.2 μg, final concentration 4.8 μg/μL), 0.6 μL of each primer (final concentration 0.3 μM), 10 μL of DreamTaq hot start PCR master mix (2×; Thermo Scientific), 0.6 μL of SYTO9 solution (50 μM; Invitrogen), and 4.2 μL of sterile DNase/RNase-free water (Biological Industries, Israel), using the StepOnePlus real-time PCR thermocycler (Applied Biosystems). Initial denaturation, for 5 min at 95°C, was followed by 40 cycles of denaturation at 95°C for 5 s, annealing and extension at 60°C for 20 s, and final extension at 72°C for 10 s. Amplicons were subsequently subjected to a high-resolution melt (HRM) step, with the temperature increased to 95°C for 10 s and then decreased to 60°C for 1 min. The temperature was then increased to 95°C at a rate of 0.3°C/s. Amplification and HRM profiles were analyzed using the StepOnePlus series. PCR results were positive for Prototheca spp. and, following DNA sequencing, the infectious agent was determined to be P. zopfii (99% identity to GenBank MG832931.1). 15
For detection of N. caninum DNA, nested PCR was performed on the CSF sample using 2 sets of primers based on the Nc5 gene of this species (GenBank X84238). The external set of primers included forward primer (5′-CTGCTGAC GTGTCGTTGTTG-3′) representing nucleotide (nt) position 476 of the referred sequence and reverse primer (5′-CATC TACCAGGCCGCTCTTC-3′) of the reverse sequence of nt position 1014. The internal set of primers included forward primer (5′-GCGTCAGGGTGAGGACAGTG-3′) nt position 631 of the referred sequence and reverse primer (5′-CTCTC CGTTCGCCAGCAGTG-3′) of the reverse sequence of nt position 910. 8 The results were negative.
PCR for detection of T. gondii was based on a 529-bp DNA fragment, as described previously, 9 using the primers Tox4 (CGCTGCAGGGAGGAAGACGAAAGTTG) and Tox5 (CGCTGCAGACACAGTGCATCTGGATT). A third pair of primers (COC-1, 5′-AAGTATAAGCTTTTATACG GCT-3′; COC-2, 5′-CACTGCCACGGTAGTCCAATAC-3′), designed to amplify general coccidian parasites (e.g., Neospora spp., T. gondii, Sarcocystis spp., Cryptosporidium parvum, Eimeria spp.) was also used as described previously, 8 with negative results that excluded infection with these parasites.
Based on the CSF analysis and PCR results, our definitive diagnosis was meningomyelitis associated with P. zopfii infection. The positive but stable N. caninum indirect IFAT titer was considered a result of previous exposure. Given the high cost of specific anti-protothecal treatment, consisting of amphotericin B, itraconazole, and fluconazole,6,11,17 and the grave prognosis despite treatment, the owner declined this option. Instead, the dog was treated with clindamycin (12.5 mg/kg/d PO q12h) and ponazuril (5 mg/kg/d PO q12h) against possible N. caninum coinfection, and prednisone (0.5 mg/kg/d PO q12h) as an anti-inflammatory drug. The neurologic signs remained unchanged for 14 d, after which acute deterioration was observed. The dog displayed obtundation, left-sided head tilt, vertical nystagmus, and non-ambulatory quadriparesis, which were suggestive of multifocal CNS lesions and dissemination of the disease. The owner elected euthanasia; postmortem examination was declined.
CNS protothecosis in dogs has usually been reported as part of disseminated disease, starting with gastrointestinal colonization and proliferation and followed by spread of the algae in leukocytes to several organs, with marked ocular and CNS tropism, although it has also been stated that Prototheca spp. do not show predilection for the CNS.10,13,16,17,20 The diagnosis of CNS protothecosis is often confirmed by finding Prototheca organisms in postmortem histologic sections.12,13,17 Antemortem diagnosis of CNS protothecosis in a dog based on CSF cytology has been reported tentatively; however, it was confirmed only postmortem by PCR assay of cultured samples from CSF and subdural olfactory bulb. 10
All Prototheca spp. grow readily on most laboratory culture media. Culture of tissues and other specimens on blood and Sabouraud cycloheximide-free dextrose agars at 25–37°C can be used for definitive identification of Prototheca. Prototheca spp. form white-to-light-tan colonies on these agars. Differences in sugar and alcohol assimilation or antimicrobial susceptibility are required for routine species differentiation, whereas rRNA sequencing is needed to differentiate P. zopfii biotypes.4,6,10,16,17
P. zopfii genotype 2 is the isolate that causes disseminated protothecosis most commonly in dogs. 16 Based on a retrospective study, the natural course of canine protothecosis appears to start with granulomatous colitis, which then slowly progresses.10,13,16,17 Once signs of dissemination become apparent, death follows rapidly. 17 The disease time course from focal colitis to the disseminated form was much shorter in 5 dogs infected with P. zopfii (median survival of 3.2 mo) than in 2 dogs infected with P. wickerhamii (median survival of 20.5 mo). 17 In our case, transient diarrhea had occurred 3 wk before the onset of neurologic signs, followed by 10 wk of hindlimb ataxia and weakness before the development of the disseminated form. This time course agrees with a report of P. zopfii infection in dogs. 17
Signs of CNS infection include lethargy, behavioral abnormalities, paresis, head tilt, cervical pain, circling, ataxia, or seizures.6,10,12,13 Although CNS infection occurs in ~50% of dogs with systemic protothecosis,16,17 the CNS is rarely the first or only body system affected.6,12 In our case, the initial neurologic signs involved the pelvic limbs, as described only once previously, 6 and remained so during the first 10 wk. Eosinophilic pleocytosis (with 65–85% eosinophils) has been reported in dogs with disseminated CNS protothecosis.11,12 Other causes of marked eosinophilic pleocytosis (>20% eosinophils) in dogs include idiopathic eosinophilic meningitis, cryptococcosis, neosporosis, and migrating helminths.1,3,18 In our case, mononuclear cells predominated in CSF cytology, most likely representing maturation of the immune response, which agrees with reports of protothecosis in dogs. 13 The high N. caninum antibody titer may indicate concurrent neosporosis. However, the lack of increase in the N. caninum antibody titer after 2 wk suggests that neosporosis was not active. Moreover, a PCR assay for Neospora in the CSF, which is used for definitive diagnosis of CNS neosporosis, 1 was negative in our dog.
Although endemic in Israel, spirocercosis2,3 is characterized by acute non-symmetrical paresis or paralysis involving either the hindlimbs or both hind- and forelimbs 3 ; the animal’s condition deteriorates quickly if left untreated. Our case displayed mild symmetrical pelvic limb ataxia, which lasted for weeks despite doramectin therapy, as recommended for cases of intraspinal spirocercosis. 2 The visual identification of algae in the CSF sample, followed by PCR and DNA sequencing, allowed definitive diagnosis of spinal protothecosis before the development of the disseminated form of the disease. We therefore suggest that, although uncommon, spinal protothecosis should be considered among the differential diagnoses in dogs with paraparesis, 6 especially when recent diarrhea and weight loss are reported.
The absence of an autopsy and histologic identification of P. zopfii is a shortcoming of our report. Nevertheless, this 4-y-old dog was presented initially with clear hindlimb proprioceptive paresis and pain upon palpating the thoracolumbar spine, while spinal reflexes were normal. The dog had shown paraparesis only for 8 wk, and it is during this period that the CSF was collected, and the PCR assay was performed and found to be positive for P. zopfii. Given that no other CNS signs were recorded, the lesion was localized to the thoracolumbar spine. The lack of extradural spinal cord compression, the presence of an inflammatory CSF cytogram, and the positive PCR for P. zopfii supported spinal protothecosis strongly as the most likely diagnosis. The deterioration, comprised of multifocal brain involvement, took place 2 wk later, and further supported our diagnosis.
In our case, the diagnosis was made 10 wk after the first identification of a neurologic problem. It is possible that early diagnosis using CSF cytology and PCR, followed by specific anti-algal treatment at an early stage of the disease, would have resulted in a better outcome.
Our report reinforces the importance of thorough evaluation of CSF cytology slides and subsequent application of molecular tools to complete the diagnosis of CNS protothecosis whenever it is suspected. Although the prognosis for CNS protothecosis cases is grave, early diagnosis is crucial for decision making by both owner and attending clinicians and may improve the prognosis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.