
Abstract
A 15-y-old castrated male Maine Coon cat was evaluated for an ulcerated soft tissue mass on the right hindlimb that had been observed for 4 mo and had grown rapidly. A 3 × 3 cm soft, raised, amorphous, and ulcerated subcutaneous mass was observed on the lateral right metatarsus. In-house cytology via fine-needle aspiration was nondiagnostic. Incisional biopsy of the mass and further staging was declined, and amputation was elected. The amputated limb was submitted for histopathology, which revealed severe chronic nodular granulomatous dermatitis and multifocal granulomatous popliteal lymphadenitis with large numbers of intralesional fungal hyphae. Fungal PCR and sequencing on formalin-fixed, paraffin-embedded tissue identified Chalastospora gossypii. No adjunctive therapy was elected at the time. The patient has done well clinically 1 y post-operatively. C. gossypii is a rare microfungus found worldwide and is considered a minor pathogen of several plants. To our knowledge, infection by this fungus has not been reported previously in veterinary species. Features in our case are comparable to other mycotic infections. Nodular granulomatous mycotic dermatitis and cellulitis, although uncommon, should be a differential for soft tissue masses in veterinary species; C. gossypii is a novel isolate.
A 15-y-old, 5.95-kg (13.1 lb) castrated male, previously healthy, indoor-only Maine Coon cat was examined at the BluePearl Veterinary Specialty Hospital Emergency Department (Auburn Hills, MI, USA) for evaluation of an ulcerated mass on the right pelvic limb. The mass was first noted by the groomer as a small swelling that grew progressively over a 4-mo period, with acute increase in size during the month prior to evaluation. No medical treatment or diagnostic testing, including cytology, was performed previously or recommended by the primary care veterinarian because the mass was suspected to be a lipoma. Surgical excision of the mass at the time of dental prophylaxis was initially scheduled to be performed by the primary care veterinarian according to the owners; however, the owners presented the cat to the BluePearl Emergency Department prior to the scheduled surgery because the mass became ulcerated. On examination, the cat was bright, alert, and ambulatory on all 4 limbs. A 3 × 3 cm soft, raised, irregularly round, amorphous subcutaneous mass was observed and palpated on the lateral right metatarsus. The mass was deeply ulcerated and adherent with palpable subcutaneous tentacle-like projections spanning from the bulk of the mass in proximal and plantar directions. A grade III/VI parasternal heart murmur was auscultated. The remainder of the examination was within normal limits.
The cat was fed a commercial dry cat food diet and was up-to-date on vaccinations. There was no history of travel outside of Michigan. The feline leukemia virus and feline immunodeficiency virus status of the cat was unknown based on medical records available. Three-view thoracic radiographs indicated mild cardiomegaly without pulmonary vessel enlargement or pulmonary edema. A small ovoid, mildly heterogeneous caudoventral soft tissue opacity was observed on the left lateral thoracic radiograph and was suspected to be summation of the pulmonary vessels with normal structures, and less likely a discrete nodule given that it was not identified in the other orthogonal views. There was mild thoracic spondylosis. In-house cytology via fine-needle aspiration (FNA) of the mass identified clusters of well-differentiated epithelial cells and red blood cells, and was considered nondiagnostic. The cat was referred to the Surgery Department for further evaluation and work-up. Gabapentin (Neurontin, Acella; 5 mg/kg, PO q6–8h) was prescribed as needed for pain.
On examination a week later, the cat was bright, alert, and responsive. Vital signs were within acceptable limits. Body condition score based on the World Small Animal Veterinary Association (WSAVA) scale for cats was 6 of 9. Pain score based on the Glasgow Composite Measure Pain Scale (CMPS) was 1 of 24. The grade III/VI parasternal heart murmur was auscultated with no arrhythmias. Clear bronchovesicular lung sounds were auscultated bilaterally. Femoral pulses were strong and synchronous. The mass on the right metatarsus was unchanged and no other masses, lesions, or lymphadenopathy were identified. The cat did not exhibit pain on palpation of the mass. The remainder of the physical examination was within normal limits.
Complete blood count results were unremarkable other than a mild normocytic, normochromic non-regenerative anemia (Hb: 92 g/L; reference interval [RI]: 93–159 g/L) and mild thrombocytopenia (164 × 109/L; RI: 200–500 × 109/L) attributed to platelet clumping identified on a blood smear. The serum chemistry panel was within acceptable limits. Radiographs of the limb were not performed given that bony involvement was not suspected based on cytologic findings and palpation of the mass during physical examination. Abdominal ultrasound and cardiac consultation were declined.
The top differential diagnosis for the ulcerated, adherent mass on the limb was neoplasia based on the history and physical examination findings. An infectious cause was considered far less likely. Given the extent and location of the mass, an incisional biopsy was strongly recommended to confirm a diagnosis. Biopsy was declined, and with the owner’s informed consent, pelvic limb amputation was elected. The cat was anesthetized, and a right pelvic limb amputation via coxofemoral disarticulation was performed routinely. The right pelvic limb including the mass and popliteal lymph node were submitted fresh to the Colorado State University Veterinary Diagnostic Laboratory (Fort Collins, CO, USA) for histologic examination. The cat recovered from general anesthesia uneventfully and was discharged the following day. In addition to liposomal bupivacaine (Nocita, Aratana; 5.3 mg/kg) administered via infiltration injection into the tissue layers at the time of the incisional closure, the cat was prescribed robenacoxib (Onsior, Elanco; 1 mg/kg, PO q24h × 3 d), gabapentin (Neurontin, 5 mg/kg, PO q8–12h), and buprenorphine (Buprenex, Reckitt Benckiser; 0.015 mg/kg, SL q8–12h) for analgesia.
Histologically, the dermis and deeper soft tissues of the metatarsus were markedly expanded by a well-demarcated, unencapsulated mass comprised of epithelioid macrophages, low numbers of multinucleate giant cells, and moderate numbers of lymphocytes and plasma cells with a few scattered neutrophils. Numerous diffusely dispersed fungal hyphae of ~3 µm diameter were identified (Fig. 1). The hyphae were pauci-septate and nonpigmented with occasional branching. Multifocal necrosis was identified with sparse multifocal acute hemorrhage. There were nodular foci of granulomatous inflammation within the right popliteal lymph node, each with numerous intralesional fungal hyphae identical to those in the mass. Severe chronic nodular granulomatous dermatitis and cellulitis and granulomatous lymphadenitis with intralesional fungal hyphae were diagnosed. Formalin-fixed, paraffin-embedded (FFPE) tissue samples submitted to the Washington State University Veterinary Diagnostic Laboratory (Pullman, WA, USA) for fungal PCR and sequencing were 100% homologous with Chalastospora gossypii.
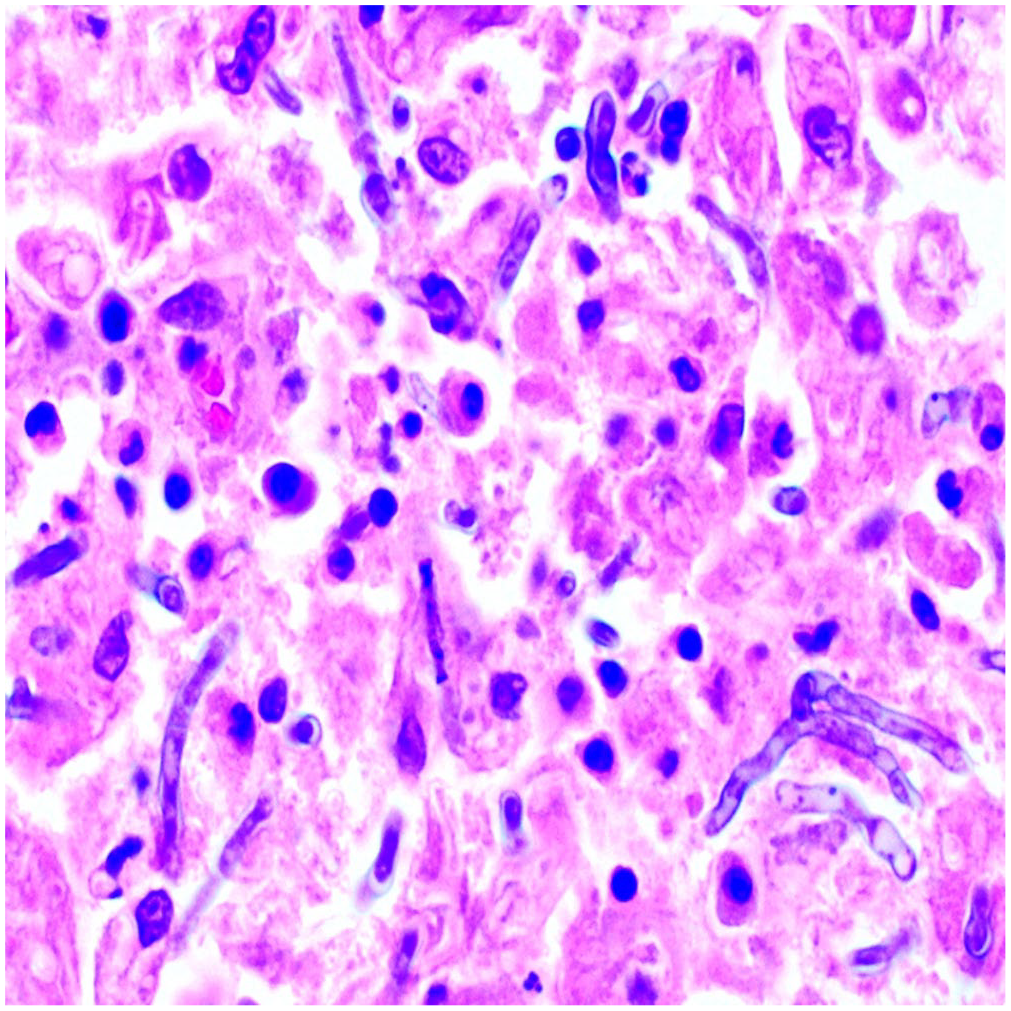
The mass on the lateral right metatarsus of the cat is composed of large numbers of macrophages that surround fungal hyphae. The hyphae are ~3 µm diameter, with occasional branching. H&E.
At recheck examination 2 wk later, the incision site was healing appropriately, and sutures were removed. The cat was ambulating well on 3 limbs and was comfortable. No additional testing or adjunctive antifungal therapy was performed. The cat was pain-free and ambulating well at 4-mo follow-up; no other cutaneous lesions or systemic illness were identified. The cat was continuing to do well at 1-y follow-up.
C. gossypii is a rare microfungus that is categorized in the genus Cladosporium or Cladosporium-like Chalastospora in the order Pleosporales. C. gossypii is found worldwide and is considered a minor pathogen of several plants, including barley6,12,13; it is related phylogenetically to C. malorum and Alternaria malorum.2,4 Alternaria was the most common cause of subcutaneous mycosis in cats in a PCR and sequencing analysis of 52 cases, 3 but other unusual hyphal fungi have been reported in cats including Fusarium proliferatum, Cladophialophora bantiana, and Exophiala attenuata.1,15,19
Mycotic disease may be more serious with the potential to disseminate in patients immunocompromised by an underlying condition or immunosuppressive therapy.6,12,17 For example, strains of Alternaria spp. may cause disseminated cutaneous or subcutaneous, cerebral, and corneal mycosis in humans, 18 cats,12,14,16-18 horses, 8 and less commonly dogs.6,20 Importantly, opportunistic veterinary fungal infections are reportedly increasing in frequency because of the increased availability and usage of novel chemotherapeutic protocols and immunosuppressive agents for the treatment of various medical conditions. 5 In a 2017 retrospective cohort study of 113 client-owned dogs managed for selected immune-mediated diseases including immune-mediated hemolytic anemia, immune-mediated thrombocytopenia, immune-mediated polyarthritis, and Evan syndrome, 15 of 113 (13%) dogs were diagnosed subsequently with opportunistic invasive fungal infections (OIFIs) based on cytology, culture, and histopathology. 11 OIFIs in 10 of these 15 dogs (67%) were the result of phaeohyphomycotic infections, including Cladosporium spp. and Alternaria spp. 11 Phaeohyphomycosis is usually transmitted via inhalation or cutaneous penetration; 14 of these 15 dogs developed cutaneous lesions in that study, and only 1 dog developed disseminated OIFI in the renal capsule. 11 The odds and risk of developing OIFIs were increased in dogs treated with immunosuppressive medications, specifically cyclosporine. 11 Identifying the specific fungal disease, including source and route of transmission, is important in facilitating early clinical diagnosis and selecting appropriate treatment (i.e., antifungals, adjusting immunosuppressive medication dosages, or modifying multi-agent protocols) to allow for a favorable outcome in the face of opportunistic fungal infections.
To our knowledge, infection by C. gossypii has not been reported previously in veterinary species. The clinical and histologic findings of an ulcerative and granulomatous nodular mass with intralesional fungal hyphae are comparable to other opportunistic veterinary cutaneous mycotic infections, including Alternaria spp. infection, aspergillosis, mucormycosis, and other forms of hyalohyphomycosis and phaeohyphomycosis in dogs and cats. 9 We do not know if our case represents opportunistic infection or a virulent strain of C. gossypii, and the source of infection is unknown; the cat did not have a history of previous illness or chronic immunotherapy. Although uncommon, a migrating vegetative foreign body carrying or infected with C. gossypii could be speculated as a potential underlying source of the fungal infection and granulomatous reaction in the cat. Taxonomic studies have reported C. gossypii infections of certain plant species, including lupines, cheatgrass, and mountain fern moss, which have been reported to grow in certain areas of Michigan.2,4 Despite the cat being an indoor-only cat, vegetative foreign body migration via fomite transmission (i.e., clothing, shoes, etc.) through penetration of either intact or unidentified compromised skin (e.g., abrasion) cannot be ruled out.
Diagnosis of opportunistic mycosis can sometimes be achieved by FNA and cytology, which may show fungal elements and granulomatous or pyogranulomatous inflammation. Culture of the fungus or PCR with sequence identification from a sample of fresh tissue can provide definitive species identification in many cases, but can require ≥ 2 wk depending on the sample and the organism, and poses risk to laboratory staff unless zoonotic systemic mycoses such as blastomycosis, histoplasmosis, and coccidiomycosis have been ruled out. 9 When a diagnosis is achieved by biopsy, PCR and sequencing for species identification can be performed on formalin-fixed or FFPE tissues.3,7 If a migrating foreign body harboring the microfungus, such as a plant awn, seed, or remaining necrotic plant material, was of concern in this cat, a CT scan and contrast study would have been recommended, particularly if the results of the incisional biopsy were inconclusive for a neoplastic process and the owners wished to move forward with further testing prior to considering surgical and/or other medical treatment options.
The gold standard of treatment of opportunistic mycoses is complete surgical excision, which may be followed by systemic antifungal therapy if there is known or suspected systemic involvement. 10 The prognosis is guarded-to-poor in cats with multiple lesions or systemic involvement, especially when there is neurologic involvement. 10
Footnotes
Acknowledgements
We thank the Washington State University Veterinary Diagnostic Laboratory, and Michael L. West, PharmD, for editing and providing pharmaceutical knowledge regarding treatment.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.