
Abstract
The most prevalent causes of death in racehorses are musculoskeletal injuries, causing ~83% of deaths within the racing industry in California and elsewhere. The vast majority of these injuries have preexisting lesions that predispose to fatal injury. A 4-y-old Thoroughbred colt suffered an acute suspensory apparatus failure, including biaxial proximal sesamoid bone fractures of the right front fetlock, causing loss of support of the fetlock joint and consequent fall with fractures of the cervical and sacral spine. Cervical fracture caused spinal cord damage that resulted in sudden death. A preexisting lesion in the medial proximal sesamoid bone likely predisposed to complete fracture of this bone and fetlock breakdown. Interestingly, a comparable osteopenic lesion was present in the intact medial proximal sesamoid bone of the left forelimb, which is consistent with bilateral repetitive overuse injury in racehorses. The morphologic features of the cervical and sacral spine fractures were compatible with acute injury; no evidence of preexisting lesions was seen. Most likely, these acute vertebral fractures occurred as a result of the horse falling. This case emphasizes the importance of performing a detailed autopsy in horses that suffer an appendicular musculoskeletal injury, particularly in fatal cases when the horse dies following a leg injury.
The most prevalent causes of death in racehorses are musculoskeletal injuries, causing ~83% of deaths in Thoroughbreds within the racing industry in California and elsewhere.7,12 Although the great majority of musculoskeletal injuries with poor prognosis lead to euthanasia, it is rare that a musculoskeletal injury is the direct cause of death. In those unusual cases, the cause of death is frequently not found despite extensive diagnostic workup. We present here a case of fetlock breakdown during training, which led to the falling of the horse, resulting in cervical and sacral fractures. Cervical fracture caused spinal cord damage, which resulted in the death of the horse.
A 4-y-old Thoroughbred colt with a history of completing 9 races during a 23-mo long racing career at high-level competition had a catastrophic injury to the right fore fetlock during his final furlong of a high-speed 5-furlong workout on a dirt surface. It was his third official timed high-speed workout 44 d after completing the last race (Suppl. Fig. 1). The horse fell and collided with the ground with a hyperflexed neck (“head dived”), displaced his jockey, and died on the track within minutes. The jockey was seriously injured in the fall. However, he was able to return to racing several months after the incident.
A detailed autopsy was performed, including examination of visceral organs, forelimbs, spinal canal, and head. 4 Postmortem radiographs of cervical vertebrae, sacrum, and proximal sesamoid bones were taken. Additionally, microCT scans of both medial proximal sesamoid bones were obtained. The autopsy revealed that the third cervical vertebra (C3) and the sacrum had comminuted, complete fractures. The body of C3 was separated into cranial and caudal parts by a comminuted transverse fracture at the level of the cranial aspect of the ventral crest (Figs. 1, 2). Incomplete, minimally displaced transverse fractures extended from the body into the lamina of the vertebra. Additionally, the ventral crest was separated from the vertebral body by a longitudinal fracture at the base of the crest. There was also massive hemorrhage within the spinal canal that, together with protruding bone fragments, produced spinal cord compression. Histology of the cervical spinal cord revealed congestion and increased neutrophils within blood vessels at the level of injury. Otherwise, the spinal cord was unremarkable. The sacrum had a complete, displaced, mildly comminuted, oblique fracture extending in a craniodorsal-to-caudoventral direction from the ventral third of the dorsal spinous process of the second sacral vertebra (S2) through the body of the third sacral vertebra (S3; Figs. 3, 4) with extensive hemorrhage affecting the cauda equina and soft tissues of the dorsal aspect of the pelvic canal.
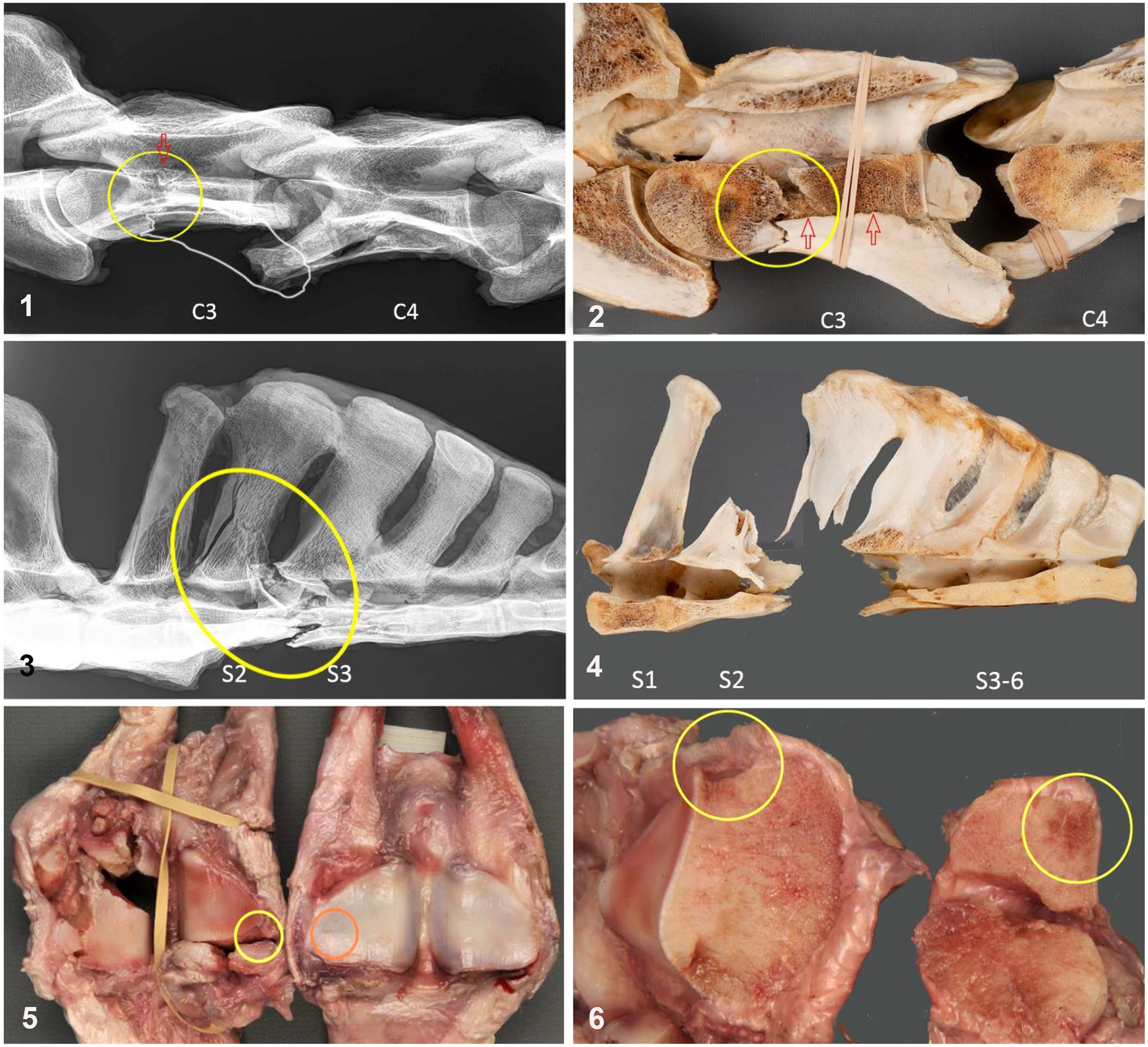
Skeletal lesions in a Thoroughbred horse with fetlock failure and vertebral fractures followed by sudden death.
The right forelimb fetlock had biaxial fracture of the proximal sesamoid bones (PSBs). The lateral PSB had a complete, displaced, articular oblique fracture that separated the bone into a proximal third and distal two-thirds, and an axial avulsion fracture associated with the intersesamoidean ligament. The proximal portion was divided into 2 fragments in a sagittal plane. The distal component was also comminuted, with 2 smaller, abaxial fracture fragments.
The medial PSB had a complete, displaced, articular, transverse, basilar fracture. The basilar component was split into 2 fragments by a sagittal fracture (Fig. 5). The opposing, transverse fracture surfaces revealed a focus of red discoloration surrounded by highly compacted trabecular bone in an abaxial subchondral location with grossly intact articular cartilage (Fig. 6). Microcomputed tomography examination revealed a focal region of osteopenia on the fractured medial PSB that was associated with the opposing fracture surfaces, and in the same subchondral location as the focal discoloration (Fig. 7). Furthermore, the medial PSB from the intact (left) forelimb, also had a focal region of osteopenia in the analogous location described in the right forelimb (Fig. 7). No other significant gross abnormalities were observed in the rest of the carcass.
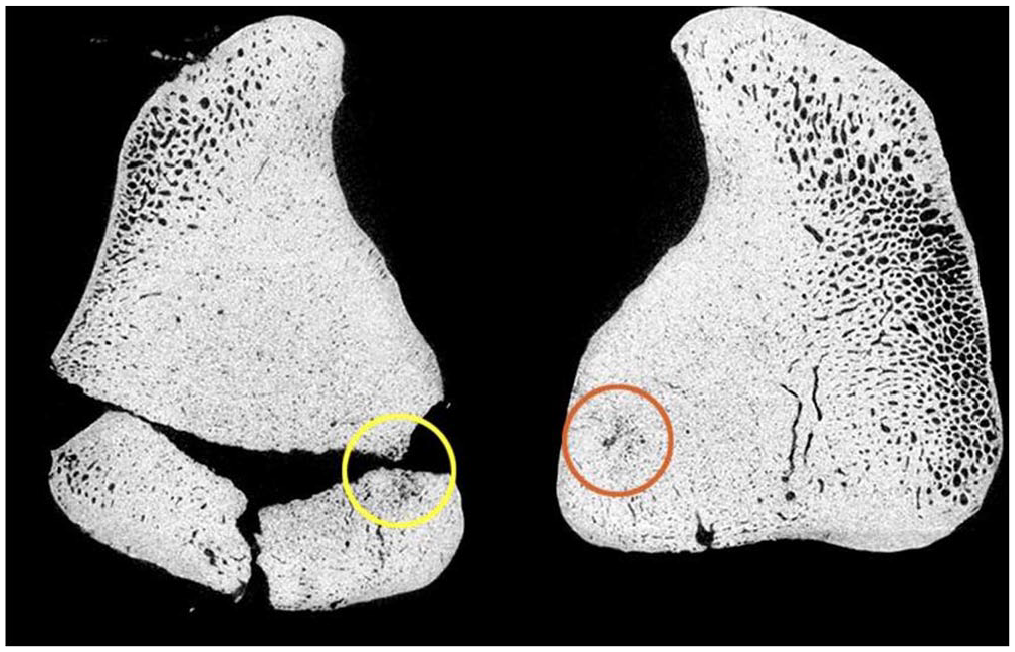
Postmortem microCT images of dorsal sections of bilateral medial proximal sesamoid bones (PSBs) illustrate a subchondral osteopenic focus surrounded by highly compacted (sclerotic) trabecular bone (yellow circle) associated with the fracture plane. This lesion is located at the same site of focal discoloration in the fractured medial PSB. A similar osteopenic focus is present in the intact contralateral medial PSB (orange circle).
The morphologic features, including lack of any evidence of preexisting lesions in the cervical and sacral spine fracture sites, and the characteristics of the fall (horse “head dived,” hit the ground with its hyperflexed neck), are highly indicative of their acute nature. Most likely, both vertebral fractures occurred as a result of the horse falling to the ground. The fall was probably a consequence of the fetlock catastrophic injury and inability to support weight on the right forelimb. The mechanism for the sacral fracture is unclear. However, we speculate, based on the fracture configuration, that hyperextension of the hind end in the second phase of the fall could have contributed to this fracture. Alternatively, this fracture could have been a consequence of the horse flipping over and landing on his sacrum.
The fracture of the 3rd cervical vertebra and resultant hemorrhage in the spinal canal with compression of the spinal cord was the most likely cause of death. Acute spinal cord injuries (SCIs), particularly severe lesions located cranial to C5 in horses, disrupt the transmission of the respiratory signal from the respiratory center located in the brainstem to the phrenic motor neurons located from C5 through C7, resulting in paralysis of the diaphragm.9,18 Also, although not apparent in this horse, any injury to the cervical spinal cord at the origin of the phrenic nerve roots (C5–C7), may also affect the transmission of respiratory impulses to the diaphragm and intercostal muscles that can significantly affect breathing, and potentially lead to diaphragmatic paralysis and respiratory arrest. 18 Histologic examination of the cervical spinal cord revealed only congestion and mild increase of neutrophils within blood vessels. This finding is consistent with acute SCI. 9
A preexisting lesion in the medial PSB (Figs. 6, 7) likely predisposed to complete fracture and catastrophic injury of the fetlock. 13 A comparable osteopenic lesion was present in the intact medial PSB of the left forelimb (Figs. 5, 7), which is consistent with bilateral repetitive overuse injury in racehorses. 13
The metacarpophalangeal joint is a high motion joint with small cross-sectional area, and little soft tissue covering. When ground reaction and muscle forces are taken into consideration, this joint undergoes 5–7 times its body weight in stress. 8 Therefore, the metacarpophalangeal joint remains the most common site of musculoskeletal issues that result in reduced performance, premature retirement, and euthanasia of Thoroughbred racehorses throughout the world10,16; ~45–50% of Thoroughbred racehorse deaths in the United States have been associated with PSB injuries.1,5,6
The great majority of catastrophic PSB injuries in the United States are characterized by biaxial fractures. 1 With fetlock extension, the PSBs are exposed to both tension from ligamentous parts of the suspensory apparatus and compression from the third metacarpal bone. Compressive forces are suspected to cause the microdamage on the subchondral surface; tensile forces may result in focal microdamage accumulation on the palmar surface.3,13 The sclerosis associated with the osteopenic lesion may be an adaptation to increasing intensity of training and racing and/or serve to buttress weakness associated with the osteopenic lesion. Clinically, affected horses are difficult to detect. Clinical manifestation of associated lameness may be vague given the subchondral location and bilateral nature of repetitive overuse injuries. Clinical signs of the subchondral bone disease may not be apparent until the intra-articular environment is involved, 8 which is rare in catastrophic PSB fracture. 13 Further, the osteopenic lesion is difficult to detect in affected horses. Lesions are located most frequently in the subchondral bone of the abaxial portion of the articular surface of the medial PSB. 13 Lesion detection by 2-dimensional planar imaging modalities (radiography and scintigraphy) is difficult given the superimposition of dense bone tissues on the small lesions. Volumetric imaging modalities (computed tomography, CT; magnetic resonance imaging, MRI) may improve localization of lesions. Nevertheless, the results of a 2019 study 14 showed the potential of positron emission tomography (F-NaF PET) for early detection and localization of subtle bone remodeling in the fetlock region, in particular within PSBs.
Given the clinical challenges in detecting preexisting lesions leading to catastrophic PSB fractures, the recognition of horses at risk based on their exercise is important. In contrast to horses sustaining insufficiency fractures early in their career or after a layup, such as humeral, scapular, and tibial fractures,11,15,17 PSB fractures tend to occur in older horses characterized by long periods of intense exercise without sufficient time for recovery.2,7
In our case, the cause of death was spinal cord compression associated with the cervical fracture. This lesion was found because a detailed autopsy that included examination of the entire spinal canal was performed, despite the fact that the horse had an obvious fetlock injury that could be seen externally. Our case emphasizes the need to perform a detailed autopsy in horses that suffered an appendicular musculoskeletal injury; this is particularly useful when a horse dies after suffering a leg injury.
Supplemental Material
sj-pdf-1-jvd-10.1177_10406387211018289 – Supplemental material for Sudden death caused by spinal cord injury associated with vertebral fractures and fetlock failure in a Thoroughbred racehorse
Supplemental material, sj-pdf-1-jvd-10.1177_10406387211018289 for Sudden death caused by spinal cord injury associated with vertebral fractures and fetlock failure in a Thoroughbred racehorse by Monika A. Samol, Francisco A. Uzal, Patricia C. Blanchard, Rick M. Arthur and Susan M. Stover in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank the California Horse Racing Board for the opportunity to perform the diagnostic workup of this particular case, as well as all autopsy technicians and students involved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The autopsy was funded by the California Horse Racing Board Postmortem Program. Special diagnostic procedures were funded by the California Animal Health and Food Safety Laboratory and by the Dolly Green Endowment of the J.D. Wheat Veterinary Orthopedic Research Laboratory.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.