
Abstract
Catastrophic musculoskeletal injuries are the most common cause of euthanasia or spontaneous death in racehorses, and the most common cause of jockey falls with potential for serious human injury. Horses are predisposed to the vast majority of these injuries by preexisting lesions that can be prevented by early diagnosis and adequate bone injury management. A thorough examination of the musculoskeletal system in racehorses often determines the cause of these injuries and generates data to develop injury prevention strategies. We describe the diagnostic approach to musculoskeletal injury, review the methodology for the examination of racehorse limbs, and provide anatomy and pathology tools to perform an organized and thorough postmortem examination of the musculoskeletal system in equine athletes.
Introduction
Musculoskeletal injuries in racehorses are a common cause of decreased performance, loss of training days, and death.12,25,44 Catastrophic fractures, defined as severe acute bone fractures that carry a poor clinical prognosis, are the most common cause of euthanasia or spontaneous death in racehorses, and the most common cause of jockey falls with potential serious human injury (California Horse Racing Board annual report, https://goo.gl/pOUCPO).19,21,28,38 It is now widely accepted that such life-threatening musculoskeletal injuries are the result of high-intensity, repetitive loading of the skeleton, which leads to weakening of the bone and subsequent failure (Stover S, et al. Diagnostic workup of upper-limb stress fractures and proximal sesamoid bone stress remodeling. Proc Am Assoc Equine Pract Conf; 2013 Dec 7–11; Nashville, Tennessee). 25 Research has proven that horses are predisposed to the vast majority of these catastrophic fractures by preexisting lesions, and fractures can be prevented by early diagnosis and adequate bone injury management (Stover S, et al.).3,24,25,30 In order to determine the reasons for these injuries and to eventually develop injury prevention strategies, a few diagnostic laboratories in the United States and elsewhere have been performing autopsies and diagnostic workup on racehorses for several years. Created in 1990 by the California legislature, the postmortem program that the California Animal Health and Food Safety Laboratory System (CAHFS) runs for the California Horse Racing Board (CHRB) was an early pioneer. 38 To date, more than 6,500 horses have been autopsied through this program, and ~75% of these deaths were to the result of catastrophic musculoskeletal injuries (https://goo.gl/pOUCPO).
The racehorse postmortem program at CAHFS was created, and still operates, with 3 main objectives: 1) to describe musculoskeletal injuries in racehorses, 2) to determine the cause of these injuries, and 3) to generate data for the development of injury prevention strategies. Our report describes the postmortem diagnostic approach to musculoskeletal injury, reviews the methodology for the examination of the racehorse musculoskeletal system, and provides anatomy and pathology nomenclature used for the examination of the musculoskeletal system in racehorses. This approach is based on the combined experience of numerous pathologists that have participated in the CAHFS postmortem program over the past 25 years.
Description of the CAHFS racehorse postmortem procedure
A completed CAHFS submission form (Supplemental Fig. 1, available at http://vdi.sagepub.com/content/by/supplemental-data), signed and dated by the CHRB official veterinarian or attending veterinarian, must be submitted before autopsy is initiated. Whole carcasses are transported to the laboratory in every case, and a detailed identification of the horse is performed before autopsy begins. All the visceral organs are examined during autopsy. Liver, kidney, and urine samples are collected from animals that were injured or died during a race, or when there is a human injury. These samples are typically stored frozen (–20°C) and only processed if required by CHRB or if deemed appropriate by the pathologist, typically for toxicologic examination. Samples for histology and other disciplines, such as bacteriology, virology, parasitology, and immunology are not routinely collected, but are taken at the discretion of the pathologist. Special circumstances may warrant a more in-depth investigation.
Examination of the musculoskeletal system
Examination of the musculoskeletal system focuses on the injured region or limb and, in the case of the legs, the corresponding region of the contralateral limb. All bones and soft tissues distal to the antebrachiocarpal (radiocarpal) or tarsocrural (tibiotarsal) joints are routinely examined when the catastrophic injury occurred at the level of, or distal to, these joints. Lesion descriptions use appropriate anatomic (Nomina Anatomica Veterinaria, https://goo.gl/a9U9wa) and pathology terminology. The use of the appropriate terminology is very important, especially when pathologists with different backgrounds and skills are involved in the examination of musculoskeletal injuries. The basic topographic terms used to document the position of parts of the body, lesion location, and fracture direction relative to the median, dorsal, and transverse planes are shown in Figure 1. In addition to the written description of the musculoskeletal lesions, drawings of the major lesions and checklists typically accompany the autopsy report. See Supplemental Figure 2 (available at http://vdi.sagepub.com/content/by/supplemental-data) for an example of a gross pathology worksheet and checklist for injuries of the third metacarpal bone.
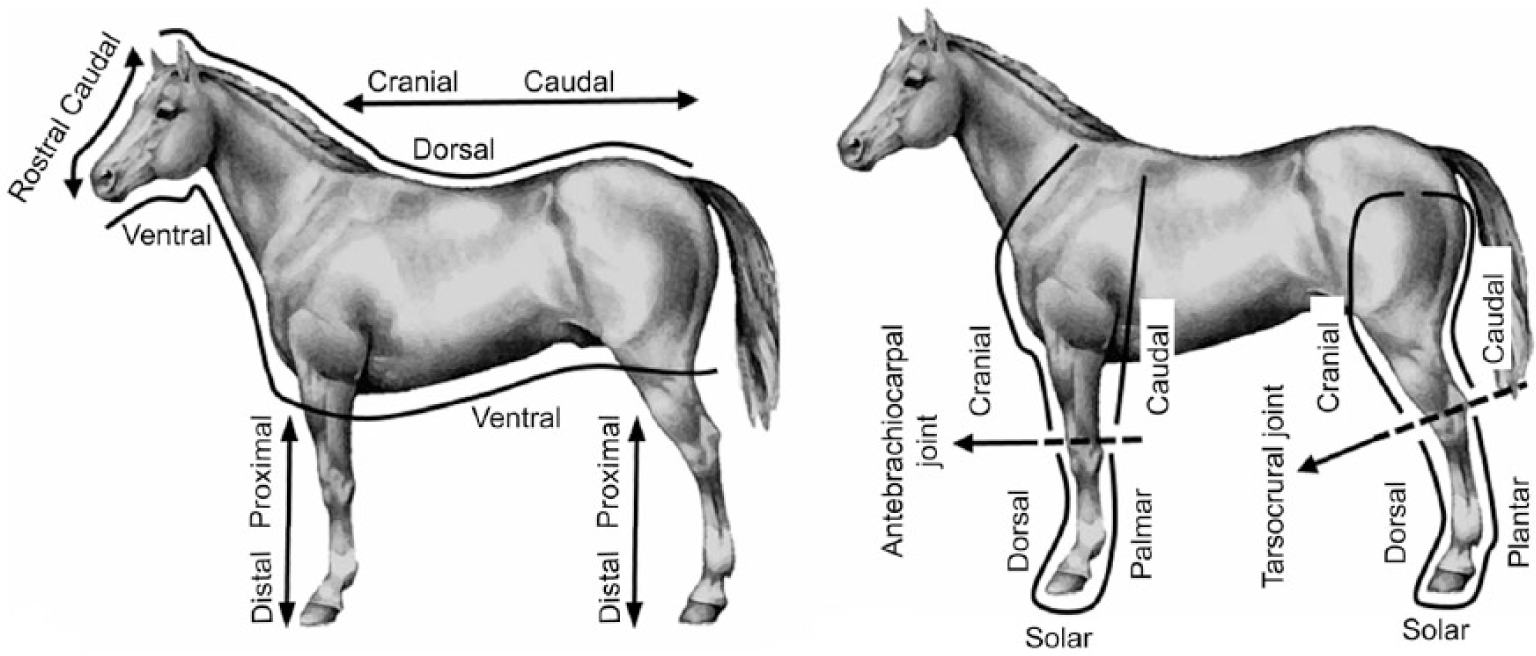
Topographic terms used to document the position of parts of the horse, lesion location, and fracture direction relative to the median, frontal (dorsal), and transverse planes.
Three main categories of lesions are sought and recorded during a routine musculoskeletal gross examination: 1) acute injuries, including fractures, luxations, subluxations, tendon and/or ligament disruption, and associated soft tissue damage; 2) evidence of preexisting lesions associated with the acute injuries (e.g., periosteal calluses/stress fractures); and 3) chronic and/or degenerative conditions of the articular cartilage, bones, ligaments, tendons, or articular capsule that reflect the overall health of a particular limb, joint, or bone and that may or may not be directly associated with the catastrophic fracture.
Examination of the acute injury
Acute fractures should be described thoroughly and consistently. The following features and qualifiers are used for long bones: 1) bone(s) affected; 2) nature of the fracture (open [compound] or closed; simple or comminuted; complete or incomplete; displaced or nondisplaced; articular or nonarticular; avulsion or nonavulsion); 3) location (proximal epiphysis, proximal physis, proximal metaphysis, diaphysis, distal metaphysis, distal physis, distal epiphysis, or other [e.g., apophysis]); 4) direction and/or length (from proximodorsal to distopalmar, from proximolateral to distomedial, etc.); 5) plane (e.g., sagittal, dorsal); and 6) configuration (axial or longitudinal, transverse, segmental, butterfly, spiral, oblique, etc.).
Fracture configuration is related to the biomechanical circumstances that created the fracture (Fig. 2) and can vary when several biomechanical loading modes act simultaneously to create fracture. Configuration is an important consideration for prognostic and treatment considerations of similar fractures in other horses.36,38 Fracture configuration can be simplified by describing key major components, followed by subcomponents. This format is relatively easy to implement and is useful for clinicians to interpret, recognize patterns among horses, and determine prognosis for repair had that been a consideration. For example, with a comminuted, articular scapular fracture: “The major fracture component separated the scapula into a large proximal segment and a smaller distal segment by a complete, transverse fracture at the level of the distal end of the spine of the scapula.” This first sentence provides the framework for the remainder of the description: “the distal segment is separated into cranial and caudal fragments by a longitudinal fracture in a cranial plane that extends into the glenoid cavity. An incomplete fracture in the infraglenoid fossa extends proximally from the transverse fracture” (Fig. 3). Other common examples of fracture configuration in a variety of bones are shown in Figures 4–11.
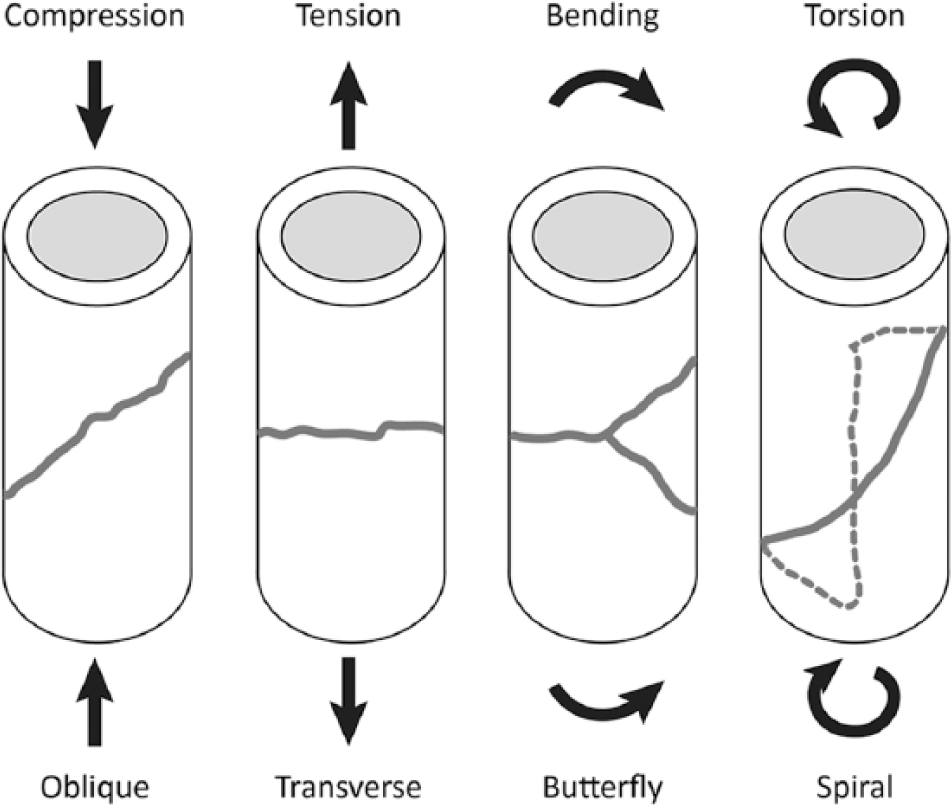
Examples of fracture configuration in relation to the biomechanical circumstances that created the fracture. Configuration can vary when several biomechanical loading modes act simultaneously to create fracture.
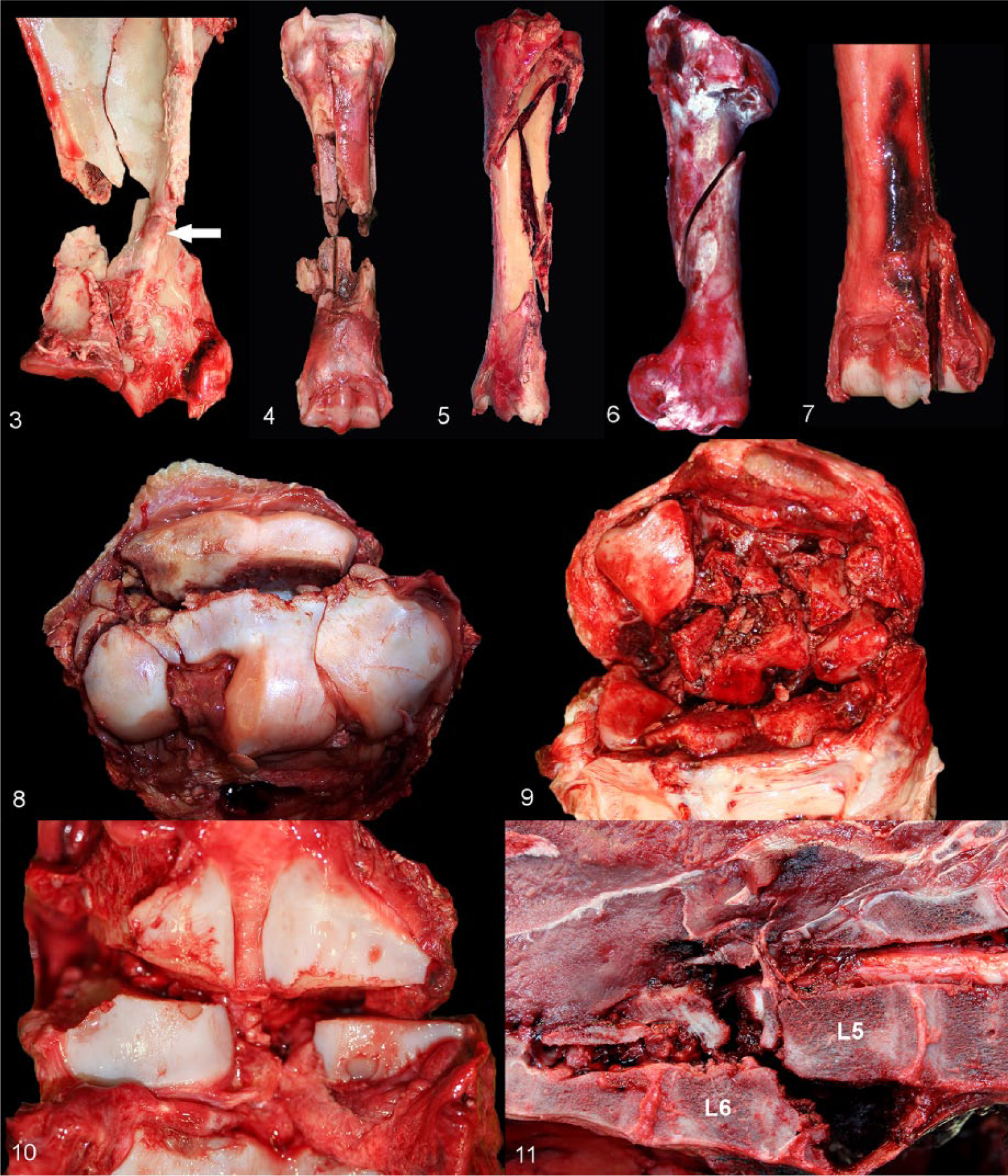
Common examples of fracture types and configurations in a variety of bones.
Description of fractures in some bones requires specific terminology. For instance, fractures of the proximal sesamoid bones are described with specific terminology 3 and differences include 1) bone(s) affected (uniaxial or biaxial) and 2) location (apical, mid-body, basilar; axial, abaxial; Fig. 12). The more common types or combinations of proximal sesamoid bone fractures also include avulsion fractures in the proximal sesamoid bones occur abaxially at the insertion site of the branches of the suspensory ligament, axially at the attachments of the intersesamoidean ligament, or basilarly at the origin of the distal sesamoidean ligaments.
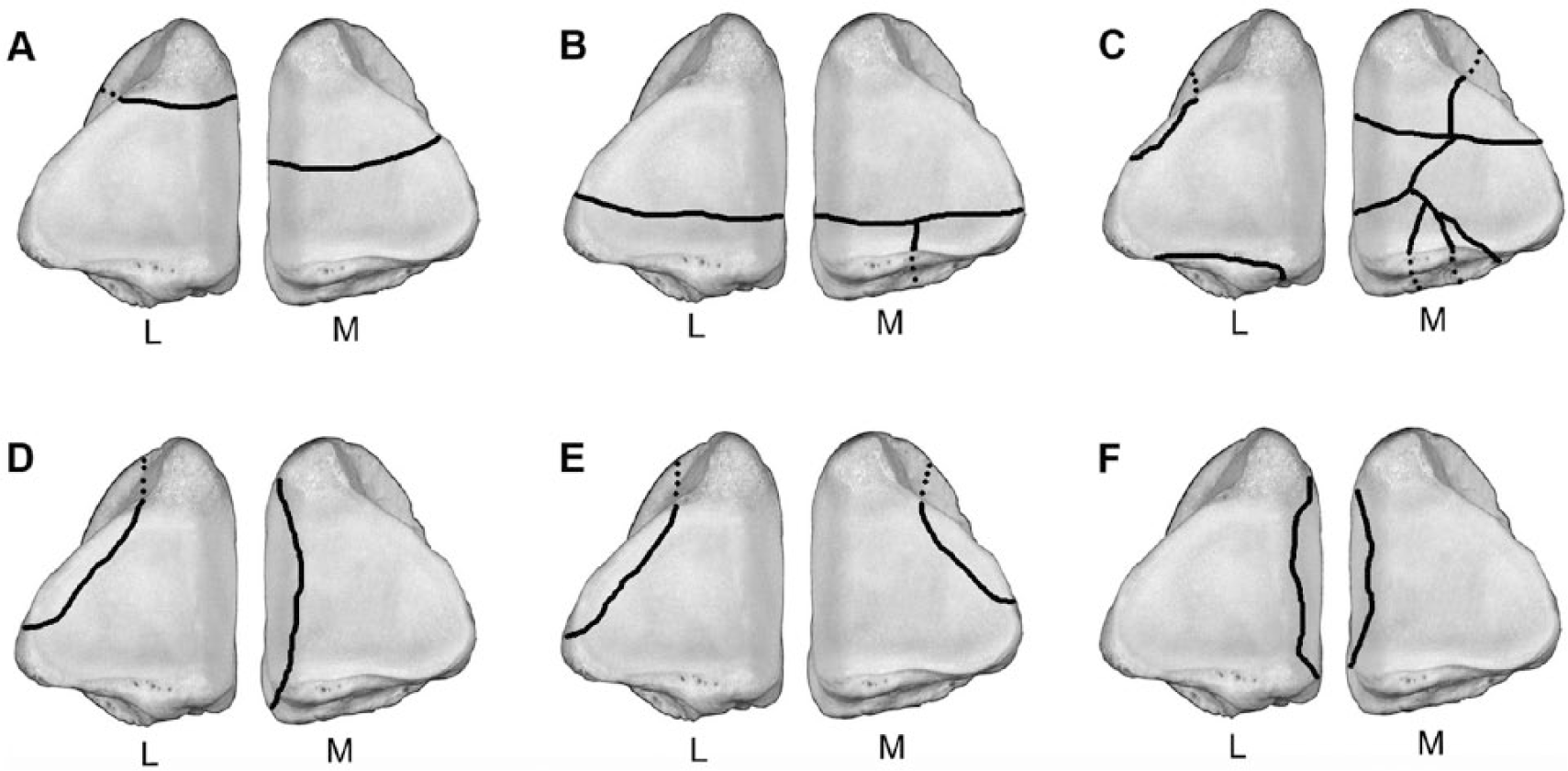
Terminology used to describe articular fracture location and type in the medial (M) and lateral (L) proximal sesamoid bones.
Other short (cuboidal) bones (e.g., the third carpal and central tarsal bones) can sustain a biarticular fracture. When a biarticular fracture occurs in a dorsal plane, it is referred to as a dorsal slab fracture.
Examination of preexisting lesions
Examination of fracture surfaces and soft tissue structures for preexisting lesions is a critical part of the postmortem examination. Knowledge of the presence of preexisting lesions provides veterinarians and trainers with information useful for prevention of similar catastrophic injuries in other horses.
There are 2 types of grossly detectable features that are indicative of preexisting lesions: 1) periosteal and/or endosteal callus formation and 2) intracortical and/or subchondral bone resorption or remodeling. These abnormalities must be in physical association with the acute fracture to be considered relevant to the pathogenesis of the fracture. Accordingly, a careful examination of periosteal, intracortical, and endosteal bone fracture surfaces is paramount. Similar abnormalities are often present on the contralateral bone because of the bilateral nature of repetitive, overuse injuries.
Periosteal and/or endosteal modeling or periosteal and/or endosteal calluses are indicators of preexisting stress fractures and are common in the scapula, 43 humerus (Fig. 13; Stover S, et al. Diagnostic workup of upper-limb stress fractures),10,36–38 tibia,24,36–38 pelvis,16,36,38 and third metacarpal bone (Fig. 14a, 14b). 36 There is also evidence of preexisting lesions leading to acute fractures of the lumbar vertebral column in racehorses. 7 In these bones, fracture margins and other areas in which they are known to occur (Stover S, et al.)36,38 should be carefully evaluated for new bone production on periosteal and endosteal surfaces. Periosteal calluses vary from very subtle (mild) to very obvious (severe). Early calluses may be difficult to detect. Such calluses are formed of typically thin, red, flat, rough-surfaced, highly vascular woven bone with minimal periosteal elevation. With increasing size and maturity, calluses enlarge, and woven bone is gradually replaced by more consolidated lamellar bone, resulting in gradually thicker, soft or firm, white or red, sometimes nodular, smooth or rough-surfaced lesions. Reexacerbation of a chronic lesion is reflected by thin, rough-surfaced, red woven bone tissue surrounding a smooth-surfaced, large, nodular callus. Endosteal callus is grossly evident as focal endosteal sclerosis.
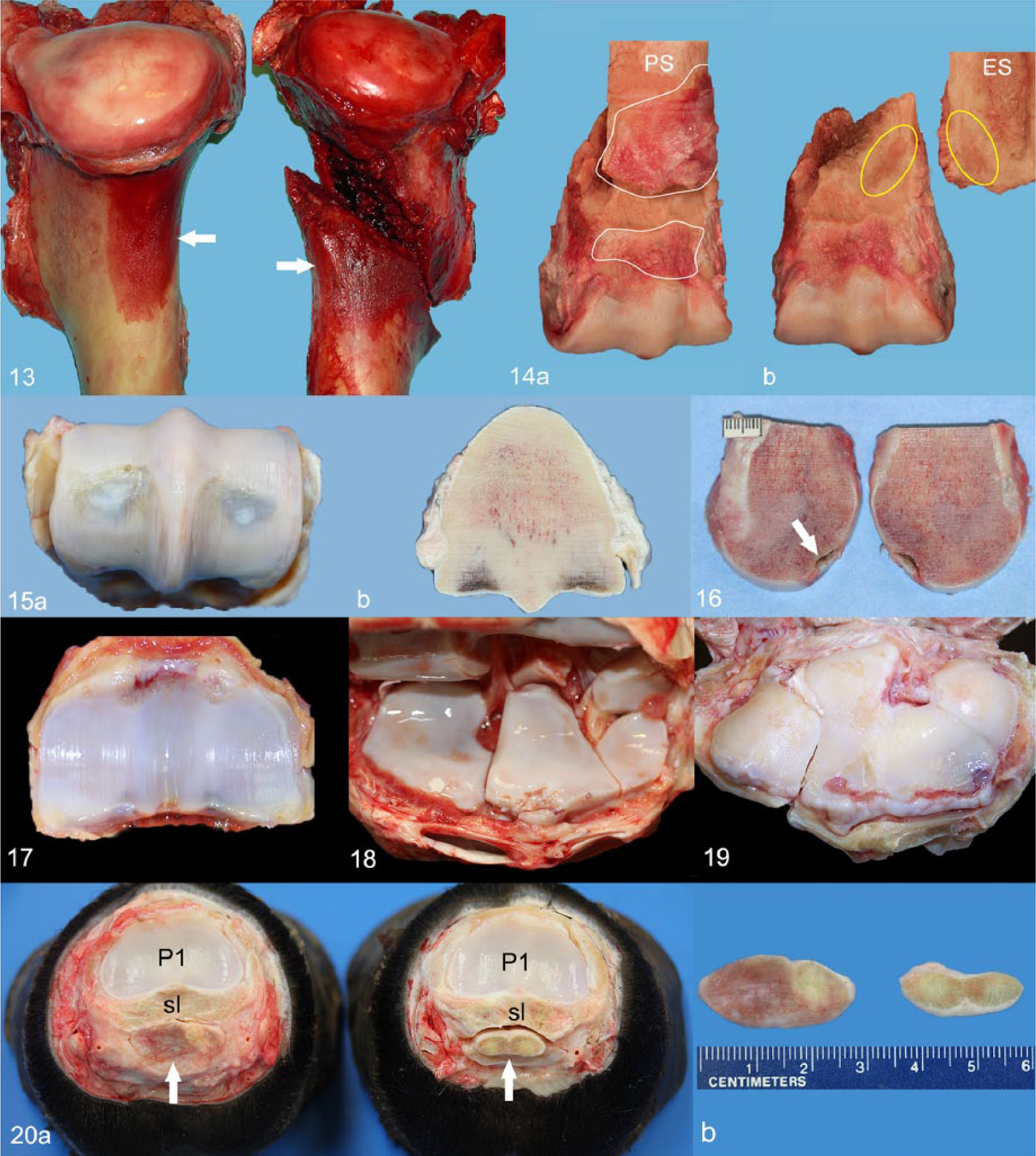
Periosteal remodeling/callus, humeri. Bilaterally symmetrical, moderate (left) and severe (right) periosteal calluses (arrows) at the proximocaudal aspect of the diaphysis of both humeri with associated acute spiral fracture of the right humerus.
Comminuted fractures with multiple small bony fragments may pose a significant challenge for the identification of periosteal callus, especially if these are subtle. Furthermore, key bone fragments may be missing with comminuted open fractures when fracture fragments remained at the site of catastrophic bone failure. Knowledge of the consistent sites for stress fractures (Stover S, et al. Patterns of stress fractures associated with complete bone fractures in racehorses. Proc Am Assoc Equine Pract 39th Ann Conf; 1993, 131–132; Stover S, et al. Diagnostic workup of upper-limb stress fractures)36–38 in individual bones is helpful for focusing initial efforts for callus identification (Stover S, et al. Diagnostic workup of upper-limb stress fractures).16,36,37,41,43
The second feature related to preexisting lesions is intracortical or subchondral remodeling. This feature can be recognized on opposing fracture surfaces by focal red discoloration (Stover S, et al. Diagnostic workup of upper-limb stress fractures). 15 In subchondral locations, the red focus is usually surrounded by a rim of sclerotic bone material. This feature is particularly prominent in the subchondral bone of lateral condylar fractures and the opposing fracture surfaces of supracondylar, nonarticular metacarpal bone fractures (Figs. 15, 16).
In spite of a patient examination of the fracture margins, there are still some instances in which manual cleaning of the bones is not enough to observe periosteal proliferation or remodeling. In these instances, exposing the bones to soft tissue chemical digestion (e.g., lye or chlorine bleach), flesh-eating beetle action, boiling, or autoclaving may allow visualization of preexisting lesions.
Examination of degenerative joint disease and chronic tendon and/or ligament injury
The examiner should document chronic degenerative lesions in structures commonly affected in racehorses (Figs. 17–19). The carpal and fetlock joints support significant biomechanical loading during motion and are therefore very susceptible to developing chronic degenerative lesions. 38
Degenerative joint lesions are often bilaterally symmetrical, may be subtle or severe, focal or multifocal, and may involve the articular cartilage, subchondral bone, periarticular bone, or articular capsule. The articular capsule may present fibrous thickening and chondroid or osseous metaplasia, which creates stiffening of the affected joint. The articular cartilage is particularly susceptible to damage, primarily in areas of weight bearing and/or repetitive trauma.14,22 The cartilage may be fibrillated, thin, eroded, or ulcerated (a term that, strictly speaking, refers to epithelium instead of cartilage, but that has been widely used to describe full-thickness lack of cartilage in joint surfaces), rough, pitted, scored, linearly cracked, or cracked and separated from subchondral bone, and discolored. Score lines (“wear lines”) is a term used to describe straight, parallel, linear grooves oriented in the direction of motion on the articular cartilage of hinge-type joints (i.e., fetlock, hock, and elbow). Articular cartilage “lipping” refers to cartilage proliferation along an articular margin. Chondral or osteochondral fragments (often referred to as “chips”) may partially or totally detach from articular margins. These chips occur with relative frequency along the dorsal margins of the distal end of the humerus and carpal bones and the proximodorsal margin of the proximal phalanx. Blue discoloration of the articular cartilage reflects subchondral bone hyperemia and/or hemorrhage.
Subchondral bone disease in the palmar region of the third metacarpal condyles (palmar osteochondral disease) may lead to collapse of the overlying articular cartilage, and bone weakness may facilitate condylar fracture.4,5,27–29 On cut section, chronic gross lesions in the subchondral bone may be increased porosity or increased density (sclerosis), which is the result of bone remodeling and modeling, the mechanisms used by subchondral bone when adapting to loading stresses. 22
Chronic lesions in ligaments and tendons (Fig. 20) are not as common. When present, such lesions may affect the body or the branches of the suspensory ligament, superficial and/or deep digital flexor tendons, distal ligaments of the proximal sesamoid bones, as well as other structures of the fetlock and foot. These tendons and ligaments may be thickened and/or discolored pink or red.17,35
Fetlock and suspensory apparatus–focused examination
The majority of acute catastrophic injuries occur distal to the antebrachiocarpal or tarsocrural joints, with the highest incidence in the metacarpophalangeal and metatarsophalangeal (fetlock) joints.31,38 A video demonstration of the examination of the distal portion of the front limbs (below the antebrachiocarpal joint) by Dr. Stover from the J.D. Wheat Veterinary Orthopedic Research Laboratory at the University of California, Davis, is available online (https://goo.gl/nF6EyN). Briefly, the limb is examined for abnormal conformation, deformities, and joint laxity. The skin is removed and the subcutaneous tissues and palmar neurovascular bundles examined for hemorrhage and scar tissue. Loose connective tissue and associated neurovascular structures are removed to clearly visualize, separate, and palpate the superficial digital flexor (SDF) and deep digital flexor (DDF) tendons, and the distal check ligament. The SDF and DDF tendons are then transected just below the carpal region and reflected distally away from the limb. At the level of the fetlock, the palmar annular ligament is transected longitudinally medially and laterally between the respective abaxial surfaces of the tendons and palmar border of the proximal sesamoid bones. Further distal reflection of the digital tendon structures in the pastern region is facilitated by transection of the proximal and distal attachments of the proximal digital annular ligament. Subsequently, the suspensory apparatus of the fetlock region (suspensory ligament, proximal sesamoid bones, and distal ligaments of the proximal sesamoid bones) is removed from the limb en bloc. The fetlock joint is then completely disarticulated by transecting the collateral metacarpophalangeal ligaments.
Most training or racing musculoskeletal injuries are accompanied by acute damage to the surrounding musculature and/or associated soft tissues, such as articular capsule, tendons, and ligaments. Skin wounds, hemorrhage, and edema of soft tissues around the fracture site, and tearing, fraying, or rupture of the articular capsule, tendons, and ligaments commonly occur.
The autopsy report
Writing the gross report is the last step of the examination. Findings must be documented in a clear, organized way, utilizing appropriate anatomic and pathology terminology. The report is accompanied by drawings and checklists to complement the text and may also include pictures and radiographs if available. The report has 2 important functions. The first is to carefully document all of the lesions, which is routinely done in a systematic fashion. The second important function is to convey the clinically relevant information related to the cause of death for the regulatory agency and client veterinarian. Because the latter is for client education, it is constructive to provide a short, easy-to-understand summary with the report supplemented by illustrations.
Discussion
The major goals of the CAHFS racehorse autopsy program are to describe catastrophic musculoskeletal injuries, determine their cause, and generate data to develop injury prevention strategies. Investigation of disease and/or death due to nonmusculoskeletal problems is also an integral and significant part of the program that has led to research in other areas.6,8,9,11,40
Valuable information is obtained from the gross examination of the musculoskeletal system by a competent anatomic pathologist familiar with the musculoskeletal anatomy and pathology of racehorses. At CAHFS, the racehorse autopsy program is carried out by anatomic pathologists with a very diverse set of skills.
The opportunity to collaborate with the J.D. Wheat Veterinary Orthopedic Research Laboratory at the University of California–Davis and a diverse group of veterinary specialists in equine orthopedics, bone pathology, biomechanics, and epidemiology for more “in-depth” analysis of these injuries has greatly enhanced our program and led to breakthrough scientific information over the past 25 years.1–3,7,10,13,17–21,23,26,27,31–34,36,37,39,41 –43 This research has improved the understanding of the clinical signs, etiopathogenesis, and risk factors associated with catastrophic musculoskeletal injuries in racehorses. The 2 most important concepts that were identified during the course of our postmortem program were that injuries occur at consistent locations and in characteristic configurations for each specific bone, and that preexisting pathologic conditions commonly precede catastrophic injury.17,30,36,38,43 As a result, there are better tools for the prevention, treatment, and rehabilitation of these injuries before they become life threatening.30,38
A few key concepts that are very important for the examination of musculoskeletal injuries in racehorses must be emphasized. It is of paramount importance to examine the affected and contralateral bone or limb, as the repetitive stresses and forces associated with chronic cartilage and/or bone injury and stress fractures that lead to catastrophic breakdowns are typically bilateral and often symmetrical. 38 Additionally, the severe acute damage to the joint in a fractured limb often obscures preexisting lesions and, therefore, these are often better or even only appreciated in the contralateral limb. It is also good practice to always examine carpal joints and fetlocks for chronic degenerative changes, even when the catastrophic injury occurs above the knee or hock. Largely, the fetlocks are most commonly affected by the early, repetitive, high-impact activities of training and racing.31,38 Periosteal remodeling or periosteal calluses are indicators of preexisting bone inflammation and repair associated with stress fractures and are typically found in specific locations in each bone (Stover S, et al. Diagnostic workup of upper-limb stress fractures).7,10,24,36,38,43
A consistent, systematic approach to the autopsy of equine athletes is critical in generating data that can be used to develop injury-prevention strategies. The use of the appropriate anatomic and pathology terminology is very important. If the presence or absence of lesions at standardized locations, or if the pathologic changes are not described consistently, clearly, and in a standardized form, then the information contained in the report has little or no value.
Footnotes
Authors’ contributions
SS Diab contributed to conception and design of the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; and critically revised the manuscript. SM Stover contributed to conception of the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; and critically revised the manuscript. F Carvallo contributed to conception of the study; contributed to acquisition of data; drafted the manuscript; and critically revised the manuscript. AC Nyaoke contributed to conception of the study and drafted the manuscript. J Moore and A Hill contributed to conception of the study and critically revised the manuscript. R Arthur xxx. FA Uzal contributed to conception and design of the study; contributed to acquisition and interpretation of data; drafted the manuscript; and critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.