
Abstract
Cryptococcosis, caused by the Cryptococcus gattii and C. neoformans species complexes, is an environmentally acquired mycosis affecting a broad range of host species. Among 9 communally housed ferrets, a 5-y-old castrated male ferret domiciled in an outdoor enclosure in Sydney, Australia was diagnosed with sinonasal cryptococcosis. Clinical signs resolved during 18 mo of itraconazole therapy, but the ferret was eventually euthanized because of splenic hemangiosarcoma. At postmortem, microscopic foci of persistent cryptococcosis were detected. The diagnosis raised concerns that the owners and other ferrets were exposed to a common environmental source of infection, thus prompting an investigation. Soil samples, swabs of a hollow eucalypt log (used for behavioral enrichment), and nasal swabs from 8 asymptomatic ferrets were collected. Nasal exudate (obtained at diagnosis) and tissues (collected at postmortem) were available from the clinical case. Bird seed agar culture resulted in a heavy growth of Cryptococcus spp. from one environmental site (the log), one nasal swab, and nasal exudate and tissues from the clinical case. All other samples were culture-negative. Sub-cultured isolates from the log were a mixture of C. gattii molecular type VGI and C. neoformans molecular type VNI. Ferret isolates were a similar mixture of C. gattii VGI (all disease isolates) and C. neoformans VNI (nasal-colonizing isolate). Multilocus sequence typing further revealed the ferret isolates as identical to environmental isolates collected from the log, confirming the log as the source of clinical disease and nasal colonization. The log was removed to prevent further exposure to a high environmental load of Cryptococcus spp.
Introduction
Cryptococcosis, an uncommon but important fungal disease of a wide variety of human and animal hosts, is caused by yeasts in the Cryptococcus neoformans and Cryptococcus gattii species complexes. 19 Each species complex can be further divided into 4 molecular types, designated as VNI–VNIV (C. neoformans species complex) or VGI–VGIV (C. gattii species complex), through a variety of genotyping techniques.19,25 Infection typically occurs subsequent to the inhalation of either desiccated yeast cells or reproductive basidiospores from the environment, meaning that respiratory tract disease is a common manifestation. 23 There are well-established environmental niches recorded for these organisms, including accumulations of avian excreta (C. neoformans species complex) and hollows in a wide range of tree species (both species complexes).3,23 In Australia, eucalypt trees exhibit a particularly strong association with C. gattii VGI.5,30,34
Ferrets (Mustela putorius furo) are one of many vertebrates in which cryptococcosis has been documented. Their behavioral tendencies (digging, soil sniffing, exploring confined spaces) 1 and high prevalence of intercurrent nasal cavity disease (snuffles) 20 and nonspecific upper respiratory conditions 14 may predispose them to exposure, colonization, and disease caused by yeasts of the C. neoformans and C. gattii species complexes.23,31 This has led to ferrets being considered a sentinel species for human cryptococcosis.22,27,36 A review of the ferret cryptococcosis literature 36 and subsequent case reports 27 indicate that ferrets have been affected by both the C. neoformans and C. gattii species complexes, with no obvious clinical difference between disease caused by either species complex, and no clear link between cryptococcosis (caused by either species complex) and immunosuppression in this host species. Ferrets can develop a range of clinical signs and lesions affecting a variety of body sites, including both the upper and lower respiratory tracts (the usual primary site of infection), central nervous system (CNS), gastrointestinal tract, and skin.22,36 Direct inoculation from penetrating injury may also be a mechanism by which localized subcutaneous disease develops. 22
A domestic ferret residing in western Sydney, Australia, was diagnosed with sinonasal cryptococcosis. The affected animal was communally housed with 8 asymptomatic ferrets. This case prompted concerns from the owner and attending veterinarian regarding whether any of the 8 companion ferrets and the owners exposed to the same environment could be at risk of developing cryptococcosis from a localized, identifiable, heavily contaminated source. The ferrets had access to a confined outdoor area, which included some soil and a large, hollow eucalypt log provided for shelter and environmental enrichment. Our aims were therefore to: 1) determine, via culture of nasal swabs (to assess for colonization) and serologic testing (for subclinical disease) where possible, if exposure of the other ferrets to Cryptococcus spp. had occurred; 2) conduct environmental sampling for mycologic culture in an attempt to determine if a likely source of infection was present in the proximate environment; and 3) use genotyping to explore the molecular epidemiology and characterize any Cryptococcus spp. isolates detected.
Materials and methods
Case background
A 5-y-old, albino, castrated male (or gib) domestic ferret residing in western Sydney, Australia, had a 4-wk history of violent sneezing, with a bilateral bloody purulent nasal discharge. The ferret had access to a confined outdoor area, which included some soil and a large hollow eucalypt log provided for environmental enrichment and as a place of refuge. On physical examination, marked facial asymmetry was noted, with swelling of the nasal bridge on the right side (Fig. 1). Cytology was performed on the nasal discharge, revealing numerous encapsulated yeasts displaying narrow-necked budding and degenerate inflammatory cells (largely macrophages and some neutrophils). In addition, there were some raised circular (0.5-cm diameter) alopecic skin nodules over the neck, face, and body. Cytologic examination of smears from fine-needle aspirates of the skin lesions also revealed encapsulated yeasts with an inflammatory infiltrate dominated by macrophages (Fig. 2). Based on the characteristic cytology, a preliminary diagnosis of cryptococcosis was made. The infection presumably started in the sinonasal cavity, with invasion of the adjacent bone and extension to subcutaneous tissues of the nasal bridge, and hematogenous dissemination giving rise to skin nodules.
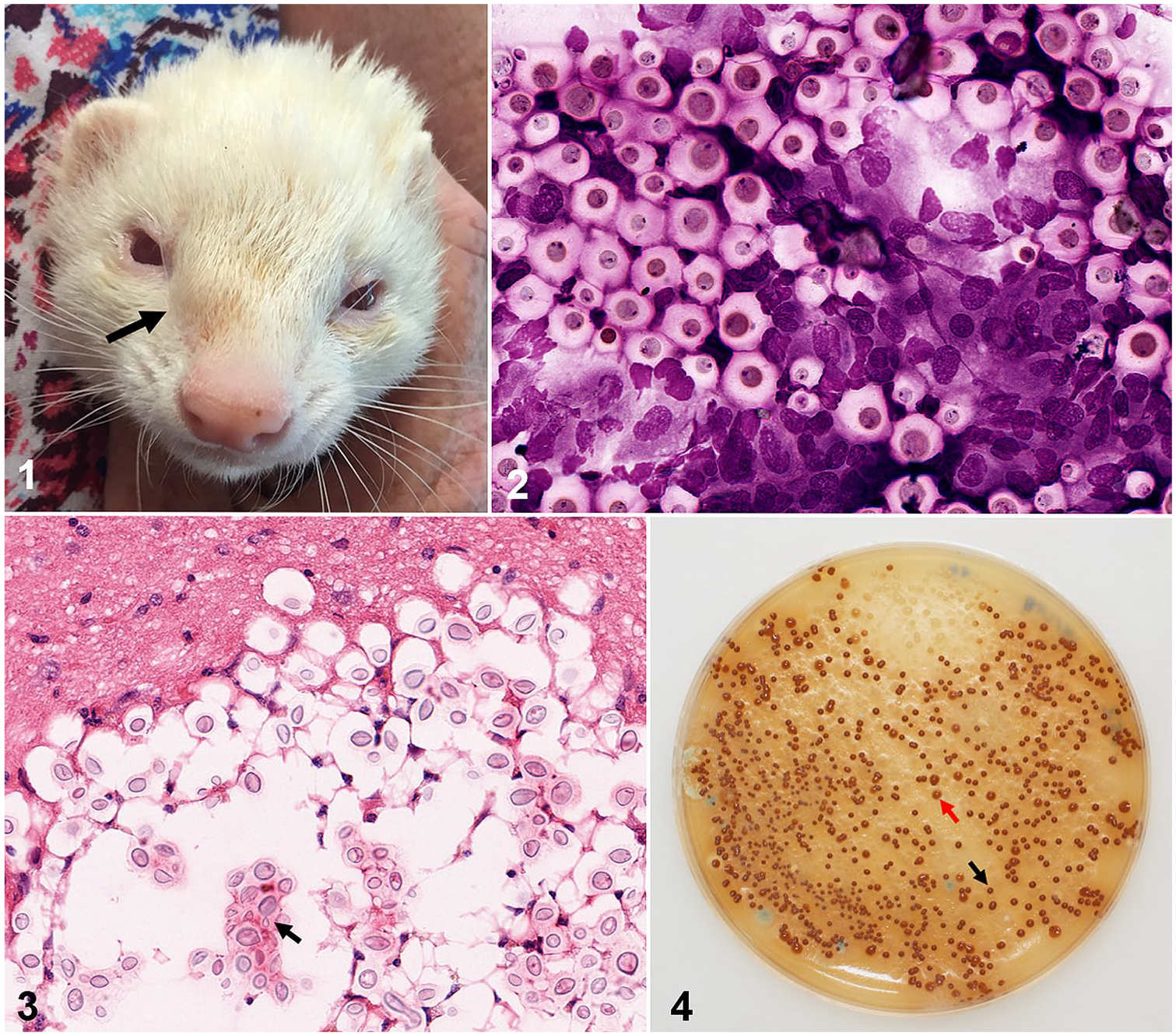
Cryptococcosis in a ferret.
The ferret was anesthetized by the attending veterinarian using isoflurane (IsoFlo Inhalation anesthetic; Abbott Australasia, Sydney, New South Wales, Australia) in 100% oxygen facilitating collection of blood by jugular venipuncture. After centrifugation to harvest serum, cryptococcal antigen testing was performed using both a lateral flow assay (LFA; CrAg LFA; IMMY, Norman, OK) and a latex cryptococcal antigen agglutination test (LCAT; CALAS; Meridian Bioscience, Cincinnati, OH) by Veterinary Pathology Diagnostic Services (VPDS) at The University of Sydney. Serologic testing was positive using both the LFA and LCAT, with the latter recording a reciprocal titer of 1,024, consistent with clinical cryptococcosis in a ferret. 22 Therapy was commenced with itraconazole (Sporanox 100 mg capsules; Janssen, North Ryde, New South Wales, Australia) at a dose of 10 mg/kg once daily orally (mixed in with the ferret’s normal food). No further diagnostic work-up was performed to assess possible underlying causes of immunosuppression. No possible causes of immunosuppression (e.g., lymphoma) 6 were indicated by the history or physical examination, although further investigations were precluded because of financial constraints.
By 4 wk after commencing therapy, nasal discharge and sneezing had resolved, but nasal bridge swelling was still evident. The skin lesions resolved slowly over the next few months. Although the medication was generally well-tolerated, intermittent periods of anorexia resolved when itraconazole therapy was interrupted for 2–3 d. By 12 mo after commencement of therapy, the facial asymmetry had disappeared. The ferret was maintained on itraconazole therapy because complete resolution of the cryptococcal antigenemia was considered unlikely at this stage and further serologic testing was not possible because of financial constraints.
The ferret had been treated with itraconazole for 18 mo when it developed generalized weakness, inappetence, polydipsia, an unkempt coat, and became acutely dyspneic. On physical examination, cutaneous bruising and subcutaneous ecchymoses on the ventrum were evident, accompanied by marked dyspnea and tachypnea. The ferret was in poor body condition, with dull mentation and pale mucous membranes. The owner opted for euthanasia without further investigation. The body was submitted to VPDS for postmortem examination, where hemoabdomen and a ruptured splenic hemangiosarcoma with hepatic metastases were identified. Histologic examination of tissues revealed microscopic cryptococcal lesions in the cerebrum (Fig. 3) and nasal turbinates. Other age-related abnormalities observed incidentally on gross and microscopic examination included chronic renal disease and dilated cardiomyopathy.
Sample collection
Pooled soil samples (3) from pot plants and garden beds to which ferrets had access, and a log within the enclosure, were submitted by the attending veterinarian. Samples from the log were obtained by running moistened sterile cotton swabs thoroughly over its surface.
Nasal swabs from 8 asymptomatic ferrets, co-habiting the same enclosure, were collected by the attending veterinarian at the request of their owner, by inserting a sterile, moistened, thin-tipped cotton urethral swab into the nares and rotating gently while under gentle manual restraint. One nasal swab was obtained from each individual over several weeks after the diagnosis of the clinical case as part of the disease investigation. A convenience blood sample from one asymptomatic ferret was collected through jugular venipuncture while it was under general anesthesia to investigate an intra-abdominal mass (later determined to be intestinal adenocarcinoma), and an aliquot was available for serologic testing. A sample of serosanguineous peritoneal fluid, collected from the clinical case at postmortem, was also available for serologic testing.
A swab of the nasal exudate from the clinical case, also collected by the attending veterinarian at the time of diagnosis using a similar method to that described above, was available for mycologic culture. All samples were submitted to VPDS. The body of the ferret was also submitted after euthanasia, and several tissue samples were collected for mycologic culture during the postmortem examination (nasal turbinate, lung, and brain).
Serology
Serum antigenemia was determined using the LFA (CrAg LFA; IMMY) and LCAT (CALAS; Meridian Bioscience) kits according to the manufacturers’ instructions (both including negative and positive controls) on a sample from one asymptomatic ferret. Serosanguineous abdominal fluid from the clinical case was also obtained at postmortem for LFA and LCAT testing. Samples with a positive LCAT result progressed to a titration procedure (performed using the same LCAT kit and according to the manufacturer’s instructions) to determine the antigen titer.
Culture
All swabs (environmental and nasal) were inoculated onto bird seed agar (containing penicillin G [40 units/L] and gentamicin [80 mg/L]) by gently rolling the swabs across the entire surface of the plate. Soil samples were inoculated by first agitating ~5–10 g of the sample in ~50 mL of sterile saline, allowing the mixture to settle for 10 min and then spreading 1 mL of supernatant across the surface of a bird seed agar plate. 17 Tissue samples were inoculated directly onto the surface of the bird seed agar plates. All plates were incubated at 27°C and checked daily. A positive control plate (inoculated with known Cryptococcus spp.) and negative controls (one inoculated with a Candida spp. and another uninoculated) were cultured concurrently. Plates were considered positive for Cryptococcus spp. if yeast colony-forming units (CFUs) exhibiting the brown-color effect were visually identified and were then classified as either exhibiting a low (1–10 CFUs), moderate (11–100 CFUs), or heavy (>100 CFUs) degree of suspect cryptococcal growth. One or more of these CFUs were randomly subcultured from positive plates onto Sabouraud dextrose agar for isolation and DNA extraction. If more than one colony morphology (exhibiting the brown-color effect) was observed (Fig. 4), then several CFUs of each colony type were randomly selected for subculture. Samples were considered negative if no cryptococcal CFUs were visible after 10 d of observation.
Antifungal susceptibility testing
Two disease isolates, one obtained at the time of diagnosis (from nasal discharge) and the other at postmortem (from brain tissue), were retrospectively submitted to the Clinical Mycology Reference Laboratory at Westmead Hospital in Westmead, New South Wales, Australia for antifungal susceptibility testing using a commercial kit (Sensititre YeastOne; Thermo Scientific, Waltham, MA). Both isolates were tested against amphotericin B, fluconazole, flucytosine, itraconazole, and voriconazole, and results were interpreted using known epidemiologic cutoff values for members of the C. gattii species complex. 3
Molecular and mating type determination
DNA was extracted from all isolates using a previously established protocol for fungi. 8 Restriction-fragment length polymorphism (RFLP) analysis of a PCR product of the URA5 gene was then performed and compared to known standard strains in the C. gattii and C. neoformans species complexes (C. gattii VGI: WM 179; VGII: WM 178; VGIII: WM 175; VGIV: WM 779; C. neoformans VNI: WM 148; VNII: WM 626; VNIII: WM 628; VNIV: WM 629) and a negative control to determine species and molecular type. 25
PCR amplification of the MF
Multilocus sequence typing and phylogenetic analysis
All isolates underwent multilocus sequence typing (MLST) according to the consensus scheme for C. gattii and C. neoformans species complexes. 26 This involved PCR amplification and sequencing of 7 loci (CAP59, GPD1, IGS1, LAC1, PLB1, SOD1, and URA5). Each PCR included a negative control. Assignment of allele and sequence types (STs) was done using the Fungal MLST Database (http://mlst.mycologylab.org). Each unique allele type sequence was submitted to GenBank (accessions MK331932–MK331951).
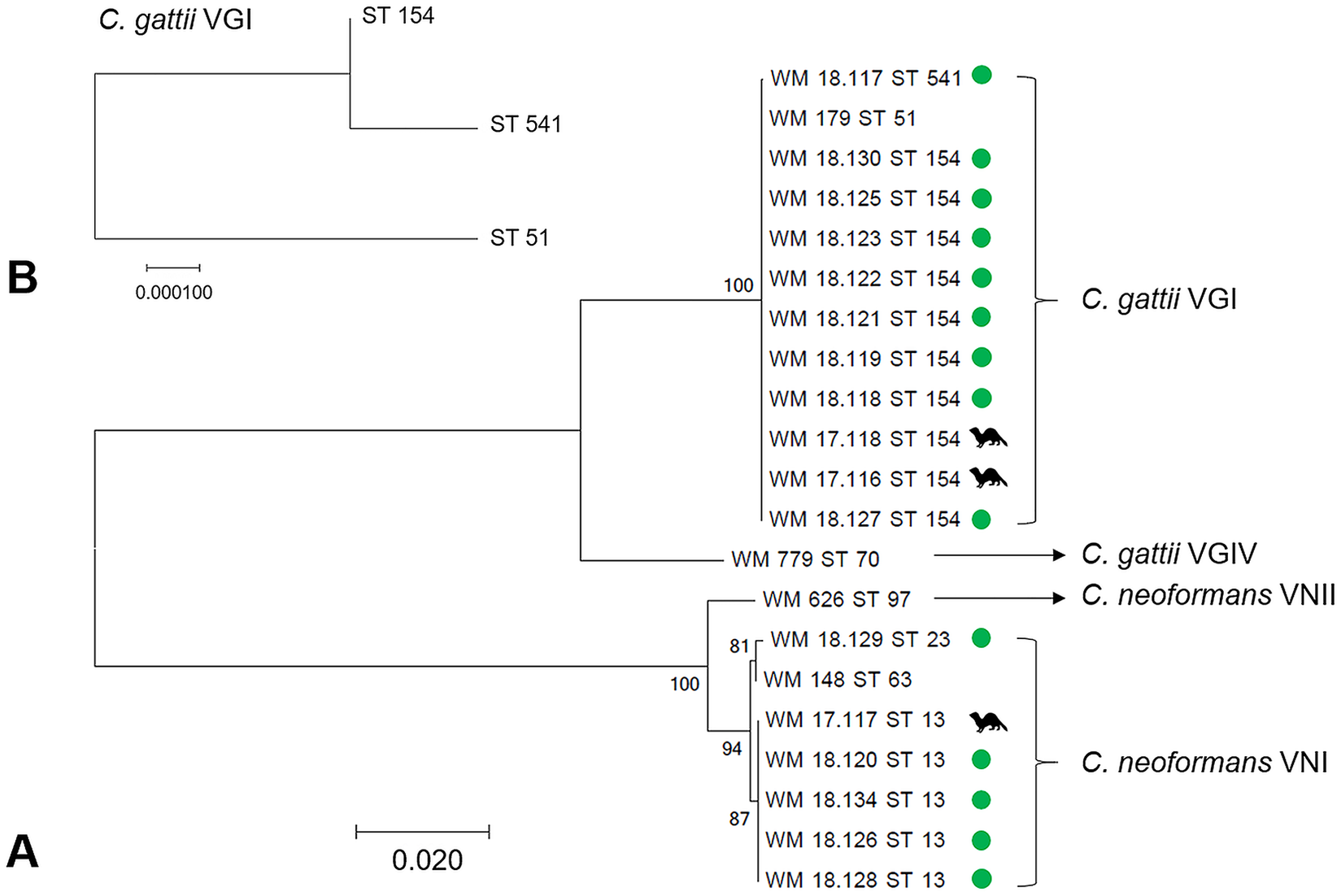
Concatenated MLST sequences were aligned by MUSCLE and underwent maximum-likelihood phylogenetic analysis, using the Kimura 2-parameter model 15 with gamma distribution, to construct a phylogenetic tree. Four standard strains were included for comparison and out-grouping (C. gattii VGI: WM 179; VGIV: WM 779; C. neoformans VNI: WM 148; VNII: WM 626). Bootstrap values were calculated using the maximum-likelihood algorithm and 1,000 replicates. All analyses were performed using the MEGA7 program. 18
Results
Serology
A serum sample from one asymptomatic ferret tested negative for cryptococcal antigen using both the LFA and LCAT. The serosanguineous abdominal fluid, collected postmortem from the clinical case, returned positive LFA and LCAT results (the latter test recording a reciprocal titer of 32, consistent with unresolved cryptococcosis). 22
Culture
All 3 swabs collected from the hollow log were heavily positive (>100 CFUs on the isolation plate) for Cryptococcus spp. on primary culture (Fig. 4). All soil samples were negative. Of the 8 asymptomatic ferrets from which nasal swabs were collected, 1 was heavily culture-positive for Cryptococcus spp. The nasal exudate swab (collected from the clinical case at the time of diagnosis) was also heavily culture-positive for Cryptococcus spp. Of the 3 tissue samples, collected during postmortem examination of the clinical case, the nasal turbinates and brain tissue were moderately culture-positive (11–100 CFUs) for Cryptococcus spp.; the lung was negative.
Antifungal susceptibility testing
Both isolates appeared to be susceptible to all antifungals tested.
Molecular and mating type determination
A total of 17 isolates proceeded to DNA extraction and molecular typing, including 14 environmental isolates collected from the positive log, a colonizing isolate from the nasal swab of an asymptomatic ferret, and 2 disease isolates from the clinical case (1 from the nasal exudate at the time of diagnosis, 1 from the brain at postmortem). URA5 RFLP analysis determined that C. gattii VGI accounted for 11 isolates, comprising 9 environmental and 2 disease isolates. The remaining 6 isolates were C. neoformans VNI, comprising the nasal-colonizing isolate from the asymptomatic ferret and 5 environmental isolates. Thus, isolates from the log were a mixture of C. gattii VGI and C. neoformans VNI.
A total of 15 isolates were mating type α, whereas 2 isolates (both environmental C. gattii VGI from the hollow log) were identified as mating type
MLST and phylogenetic analysis
Among the 11 C. gattii VGI isolates, 2 STs were identified: ST 154 (10 isolates) and ST 541 (1 environmental isolate). Allele type (AT) variation between these 2 STs was seen only at the IGS1 locus, with 2 unique ATs identified, differing by just a single nucleotide polymorphism (SNP; Supplementary Table 1). Of the 6 C. neoformans VNI isolates, 5 were ST 13; the remaining isolate was ST 23. Variation between STs 13 and 23 occurred at the CAP59, GPD1, LAC1, PLB1, and URA5 loci, with 2 unique ATs identified for each (Supplementary Table 2). The phylogenetic tree (Fig. 5) confirmed the URA5 RFLP results by its separation of isolates into clades corresponding with their species and molecular type standards, with high bootstrap support.
Discussion
We identified a hollow eucalypt log, used for shelter and environmental enrichment, as the likely point source of infection for C. gattii VGI in a ferret with cryptococcosis, and the likely source of a nasal-colonizing isolate in another asymptomatic ferret. A mixed mating type C. gattii VGI population (both α and
The 18-mo survival of a ferret with disseminated cryptococcosis is a good clinical outcome, considering the patient had a good quality of life before developing a terminal malignancy, with 2 concurrent age-related comorbidities (dilated cardiomyopathy and chronic renal disease). The prognosis for disseminated cryptococcosis in ferrets is not well-established but could reasonably said to be guarded, based on a review of prior case reports. 36 The decision to use itraconazole was based largely on the ease with which itraconazole capsules can be opened and mixed with palatable food. Ideally, antifungal susceptibility testing should have been undertaken prior to treatment to determine minimum inhibitory concentrations for itraconazole and fluconazole, but financial constraints made this impossible. Retrospective testing of disease isolates suggested that they were susceptible to all antifungals tested (including itraconazole and fluconazole). This is consistent with the expectation that cases of cryptococcosis on the east coast of Australia are usually susceptible to both agents, given that the C. gattii VGII molecular type (more associated with antifungal resistance) 4 is rare in this area. 24
With the benefit of hindsight, it seems likely that this ferret had asymptomatic CNS disease at the time of initial diagnosis, but that long-term itraconazole therapy was enough to prevent this developing further. Indeed, the substantial clinical improvement suggested efficacy of therapy. Microscopic CNS lesions have been detected through postmortem histologic examination of tissues in cases of cryptococcosis (in the absence of CNS-specific clinical signs), including in koalas and ferrets.32,36 Given the full clinical resolution with itraconazole monotherapy, alterations to the treatment regimen were not considered necessary, but other options could have included a higher dose of itraconazole, 22 the substitution of itraconazole by another triazole antifungal with better CNS penetration (such as fluconazole), 7 or the addition of amphotericin B (administered subcutaneously or intravenously).21,31 Our findings of microscopic foci of ongoing infection (despite full resolution of clinical signs) also emphasize the value of sequential antigen titers. Unfortunately, serial LCAT titer determinations were beyond the financial resources of the owner. Therapeutic drug monitoring would have been ideal to ensure that dosing was producing effective itraconazole levels in blood, given that the pharmacokinetics have not been determined for antifungal drugs in ferrets.
Most of the environmental C. gattii VGI strains collected from the enclosure log were of an identical sequence type (ST 154), with 1 C. gattii VGI ST 541 isolate detected also. This ST differed by only 1 SNP in the IGS1 allele. A similar pattern was observed among the C. neoformans VNI isolates obtained from the same log, with a nasal-colonizing isolate from one asymptomatic ferret of an ST identical to most environmental C. neoformans VNI isolates. An additional C. neoformans VNI environmental isolate, ST 23, showed more substantial differences from ST 13, with discrepant results across 5 of the 7 loci. MLST also showed that both disease-associated isolates, collected ~18 mo apart, were identical (C. gattii VGI ST 154). Phylogenetic analysis of the MLST sequences confirmed the molecular typing results, given that all isolates grouped with their appropriate standard strain, and further confirmed a high degree of similarity between C. gattii VGI STs 154 and 541, but a greater difference between C. neoformans VNI STs 13 and 23.
MLST results, along with absence of positive cultures from any other environmental samples, provide high support for the notion that this single eucalypt log was the point source of disease and nasal colonization. The log was therefore removed from the enclosure. Aerosolization of Cryptococcus spp. from a source external to the enclosure cannot be excluded, but in the absence of any large trees nearby and no significant soil disturbances, this appears unlikely. The hollow decaying log, which had been present in the enclosure for 3 y prior to the time of the initial diagnosis, likely provided an ideal substrate for the growth of pathogenic Cryptococcus spp., which may have been enhanced by ongoing scarification by the ferrets and regular soiling of the log with organic matter (urine and feces). This is very similar to a phenomenon observed in captive koalas, in which it is presumed that their use of enclosure “furniture” helps to greatly amplify the amount of Cryptococcus spp. in the proximate environment.17,23 The log, sourced by the ferret’s owner from the locale of Bogan Gate, New South Wales, Australia, is of unknown tree species, but originates from an area within the natural range of Eucalyptus camaldulensis. 2 This tree species has well-established associations with C. gattii VGI. 5 Approximately 2 y after removal, a follow-up swab sample was collected from the log and bird seed agar culture revealed a persistent heavy growth of Cryptococcus spp. The log had been stored in a sealed container in a laboratory. RFLP analysis confirmed that the mixture of C. gattii VGI and C. neoformans VNI isolates remained. A mixed population of the C. neoformans and C. gattii species complexes within the same environmental site appears to be a relatively uncommon finding, but several reports of this exist in the literature, 3 including in koala enclosures and aviaries.17,33
Our findings are similar to a study in which a likely environmental source of infection for C. gattii VGI (a hollow eucalypt) was identified in a large flight aviary. 33 In addition, our study provides comparable findings to another publication, 27 in which an environmental source of infection for C. gattii VGI in a domestic ferret was identified (nearby carob trees), although amplified fragment-length polymorphism (AFLP) typing was used to establish the connection. Another study reported 2 sibling ferrets residing in the same environment developing cryptococcosis, but separated temporally, caused by disease isolates shown to be identical using PCR fingerprinting. 22 The exact source of infection was not identified. MLST is more reproducible between laboratories and typically allows for finer-scale distinctions to be made between strains than either AFLP or PCR fingerprinting. 35
Our findings raise a question similar to prior studies: why did only 1 of 9 ferrets in contact with this source of infection develop clinical cryptococcosis? In our case, the answer remains unclear. Genetic susceptibilities could play a role, as suggested by the report of cryptococcosis in 2 sibling ferrets. 22 In the avian case mentioned previously, a high-stress period was considered the likely cause of increased susceptibility. 33 In one ferret case, concurrent lymphoma was reported as a likely cause of immunosuppression, leading to cryptococcosis. 6 It is also possible that more of the in-contact asymptomatic ferrets were colonized but this remained unidentified because of either transient colonization or the poor performance of the relatively superficial swabs able to be collected safely while under manual restraint. General anesthesia could have allowed for the collection of potentially more representative nasal samples (either deeper swabs or nasal flushes), along with blood samples from all asymptomatic ferrets to test for subclinical cryptococcosis, but this was not possible for logistical reasons. It may also have been of interest to test the human owners for cryptococcal antigenemia and nasal colonization, given that colonized humans were identified in association with another case of ferret cryptococcosis, 28 but this was also not possible.
The mixed mating type population (9 type α and 2 type
Based on our findings, and our knowledge of the environmental niches of pathogenic Cryptococcus spp., we recommend the use of other objects for environmental enrichment in enclosures for ferrets and other species, such as unused porcelain or clay drainage pipes. If hollow logs, particularly from eucalypts, are to be used, the risk of cryptococcal infection might be minimized by regular replacement of the logs, or by manual cleaning and the application of an appropriate disinfectant. Although manual cleaning could theoretically cause increased aerosolization of Cryptococcus spp., the use of appropriate personal protective equipment should effectively mitigate this risk. Systematic studies comparing the utility of various disinfectants for managing environmental Cryptococcus spp. are currently lacking. A quaternary ammonium compound (F10SC Veterinary Disinfectant; Health and Hygiene, Roodepoort, South Africa) used at the manufacturer’s recommended standard concentration (1:500) with contact time for fungi (>30 s) might provide a reasonable option based on a prior study. 16 Accelerated hydrogen peroxide disinfectants have also shown great potential against fungi and infectious agents of animals, including as environmental disinfectants,13,29 but remain untested against Cryptococcus spp.
We successfully identified an environmental point source of infection for C. gattii VGI in captive ferrets, which led to the removal of the enclosure log in question as it posed an ongoing risk of infection to the other ferrets and the owners. Our report emphasizes both the importance of environmental investigations into cases of captive animal cryptococcosis and the utility of ferrets as sentinels for disease in humans and other animals.
Supplemental Material
Supplemental_material – Supplemental material for Identification of the environmental source of infection for a domestic ferret with cryptococcosis
Supplemental material, Supplemental_material for Identification of the environmental source of infection for a domestic ferret with cryptococcosis by Laura J. Schmertmann, Alison Wardman, Laura Setyo, Alex Kan, Wieland Meyer, Richard Malik and Mark B. Krockenberger in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank Suzanne Taylor for her assistance and willingness to allow this case and the subsequent investigation to be published. We also thank Patricia Martin and Christine Black at the Veterinary Pathology Diagnostic Services, The University of Sydney, for their advice and assistance in performing part of the culturing and serologic testing. We thank Veronica Ventura at Sydney School of Veterinary Science, The University of Sydney, for providing the bird seed agar and Krystyna Maszewska at The Westmead Institute for Medical Research, for storing the isolates in the Medical Mycology Culture Collection. We also thank Catriona Halliday of the Clinical Mycology Reference Laboratory at Westmead Hospital for arranging the antifungal susceptibility testing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
R Malik’s position is supported by the Valentine Charlton Bequest. Our research was supported by the Betty Rosalie Richards Bequest at The University of Sydney.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.