
Abstract
Infectious laryngotracheitis (ILT) can cause severe losses in backyard flocks (BYFs) and commercial poultry. The prevalence of ILT, the circulating strains of ILT virus (ILTV) in BYFs, and the correlation of disease in BYF and commercial operations, is largely unknown. Of 8,656 BYF submissions, 88 cases of ILT were diagnosed at the California Animal Health and Food Safety Laboratory System in 2007–2017. ILT diagnosis by year varied from 0.19% to 1.7% of the total BYF submissions, with the highest number of cases submitted from Amador and Riverside counties. Moderate tracheitis, conjunctivitis, and occluded tracheal lumen were commonly reported gross anatomic lesions. Microscopically, inflammation and edema were observed in the trachea, lung, and conjunctiva; 62 (70%) cases had intranuclear inclusion bodies (INIBs), with 10 cases containing INIBs only in conjunctival sections. To analyze the circulating ILTV strains and to differentiate between field and vaccine strains of ILTV, real-time PCR and sequencing of 996 base pairs of the infected-cell polypeptide 4 (ICP4) gene was performed on 15 ILTV-positive tracheal samples and compared to reference field and vaccine ILTV ICP4 sequences in GenBank. Fourteen strains were identical or closely related to the chicken embryo origin live virus vaccine strains, and one strain was closely related to a Chinese isolate, the USDA reference strain, and a vaccine strain. The presence of ILT in BYFs in counties with high commercial poultry concentrations demonstrates a risk for disease transmission and emphasizes the importance of continued surveillance and improved biosecurity in BYFs.
Infectious laryngotracheitis is caused by infectious laryngotracheitis virus (ILTV; family Herpesviridae, subfamily Alphaherpesvirinae, species Gallid alphaherpesvirus 1). The genome of ILTV contains linear double-stranded DNA and ~152,000 base pairs (bp). 22 ILTV is highly contagious, can cause economically significant respiratory disease in chickens, pheasants, and peafowl, and can result is severe losses of birds.10,19 ILT was first described in the 1920s as a disease of chickens, and was the first avian viral disease to have an effective vaccine developed.10,19
Two distinct clinical presentations are observed: a severe form defined by dyspnea and expectoration of bloody mucus, and a milder form characterized by conjunctivitis, swollen infraorbital sinuses, nasal discharge, poor egg production, and poor weight gain. Transmission occurs through the upper respiratory and ocular systems. ILTV can be isolated from infected birds, dust, litter, fomites, water, and beetles. 10 A carrier state can occur with latently infected birds retaining ILTV for weeks to months in the trachea, and potentially for the life of the bird in the trigeminal ganglion.10,19
Several methods exist for detection of ILTV, including histopathology to detect syncytia and intranuclear inclusion bodies (INIBs), virus isolation, antigen detection with immunofluorescent antibodies (IFA) or immunohistochemistry (IHC), enzyme-linked immunosorbent assay (ELISA), direct electron microscopy (DEM), and DNA detection methods including real-time PCR (rtPCR).2,6,10,19 Real-time PCR is considered the most sensitive method for detection of ILTV given that sample contamination by bacteria or other viruses does not affect amplification of viral DNA. Given the sensitivity of rtPCR, ILTV can be detected in mild forms of disease and cases of low viral load.2,6,19 DEM has reduced sensitivity compared to other detection tests and may not detect ILTV in low numbers. Antigen detection tests such as IFA and IHC are comparable to histopathology results and are limited by ILTV concentration. 6 Histopathology, IHC, and IFA are subject to the reviewers’ skill because ILTV INIBs may be subtle and difficult to detect, and IFA results often have reading variability depending upon the experience of the reader. 21
Differentiation between ILTV field strains and vaccine strains is possible through rtPCR followed by restriction-fragment length polymorphism (RFLP) or DNA sequencing of multiple genome regions, including the infected-cell polypeptide 4 (ICP4) gene, among others.6,19,22 The ICP4 is an ~4,386 nucleotide transcriptional protein that regulates ILTV gene expression in the early and late stages of infection. 13 Sequence analysis of the ICP4 gene is commonly utilized to determine the genotypic origin of ILTV strains in field infections, allowing producers to assess the efficacy of vaccination protocols and methods.13,16
Control of ILT is multifactorial, with biosecurity, management, and vaccination playing key roles. Modified live virus (MLV) vaccines are of tissue culture origin (TCO) or chicken embryo origin (CEO), based on attenuation methods. Several CEO vaccines are available commercially in the United States, including LT-Blen (Merial, Gainesville, GA), Trachivax (Intervet, Omaha, NE), and Laryngo-Vac (Fort Dodge, Exton, PA). LT-Ivax (Intervet) is the only commercially available TCO vaccine. Although the MLV vaccines provide good protection and reduce mortality, the risk exists of MLV vaccine strain reversion to virulence through serial passage in chickens. Given that MLV vaccine strains circulate in a population, mutations and increasing virulence are likely to occur, in part as a result of mass vaccination in commercial flocks creating large numbers of circulating ILTVs and the tendency for ILTV to recombine. 15 These mutated vaccine strains have been referred to as “escaped” vaccine strains. They are frequently involved in ILT outbreaks, and can be maintained in BYFs, which may serve as a reservoir for ILTV infection of nearby commercial flocks.7,10,16 Recombinant viral vector vaccine options are ILTV genes inserted into a fowlpox virus (FPV) or turkey herpesvirus (HVT). Recombinant viral vector vaccines do not have the risk of regaining virulence; however, the level of protection is reduced when compared to MLV vaccines. Shedding of the challenge field ILTV is known to occur even in MLV- or recombinant viral vector–vaccinated birds.9,10,19
A 5-y retrospective study 17 demonstrated the leading role of viral diseases in causing mortality in California BYFs; the prevalence of ILT was 4% of 1,301 examined submissions, and the third most commonly identified disease in BYFs after lymphoproliferative diseases and poxvirus. Our aims for the study reported herein were to provide an overview of the clinical signs, gross anatomic and histologic lesions, and diagnostic methodology, as well as to evaluate the source of ILTV isolated in 15 BYFs as field or vaccinal by rtPCR and the sequence analysis of a 996-bp fragment of the ICP4 gene.
Materials and methods
Case selection
We searched the electronic database of the California Animal Health and Food Safety (CAHFS) laboratory system for postmortem examination cases in which ILT was diagnosed in BYFs from January 1, 2007 to December 31, 2017. Data analyzed for each case included date of submission, clinical signs (when the birds were submitted live or as the submitter specified in the history), flock location, pathologic findings, laboratory tests, and concurrent disease conditions. The concentration of commercial broiler and layer operations in counties in California was also assessed by searching the CAHFS electronic database for premises from which commercial broiler or layer postmortem examination cases were submitted from January 1, 2007 to December 31, 2017.
Postmortem examination, histopathology, and IHC
We included all ILT cases in which a routine postmortem examination was conducted and gross anatomic findings were recorded, but did not include submissions containing only a tracheal or oropharyngeal swab for ILTV rtPCR. Given the various postmortem examination techniques of case coordinators, we analyzed only the records of gross anatomic and histologic lesions associated with the conjunctiva and the respiratory tract to enhance uniformity among case data.
The conjunctiva, lung, trachea, nasal sinuses, and air sacs were collected and fixed in 10% neutral-buffered formalin, processed routinely, and sections stained with hematoxylin and eosin (H&E). IHC (EnVision system HRP-labeled polymer anti-mouse; Dako, Carpinteria, CA) for ILTV was performed on tracheal sections as described previously, 11 and IFA (polyclonal serum reagent; National Veterinary Services Laboratories, Ames, IA) as described previously. 6
Microbiology
Tissues cultured for aerobic bacteria were plated onto 5% sheep blood agar (Remel, Lenexa, KS) and MacConkey agar (Remel), incubated at 37°C and 7% CO2, and examined at 24 h and 48 h post-incubation. Bacterial species were determined based on phenotypic and biochemical characteristics. For detection of Avibacterium paragallinarum, samples were inoculated onto chocolate blood agar (Remel) with a Staphylococcus aureus feeder colony cross-streaked onto the medium. Bacterial colonies compatible with A. paragallinarum were confirmed by biochemical characteristics and PCR. 5 Fungal infections were identified by inoculating suspect tissue samples onto Sabouraud dextrose agar (Remel) with incubation at room temperature (21°C) and periodic examination over 14 d. Fungal species identification was based on phenotypic characteristics and microscopic evaluation of conidia. 14
PCR
Oropharyngeal swabs or oropharyngeal/tracheal swabs were tested for influenza A virus by reverse-transcription (RT)-rtPCR (National Animal Health Laboratory Network protocol) in all birds. Additionally, the swabs were tested for ILTV by rtPCR, for Mycoplasma gallisepticum (MG) and Mycoplasma synoviae (MS) by rtPCR (RealPCR MG/MS multiplex DNA mix; IDEXX, Westbrook, ME), and for infectious bronchitis virus (IBV) by RT-rtPCR in a subset of birds when requested by the case coordinator.1,2
Electron microscopy
Tracheal tissue was collected for DEM (JEM-1400 Plus; JEOL, Peabody, MA) for detection of herpesvirus, and was performed as described previously. 6
ICP4 sequencing
Of the 40 ILTV rtPCR-positive specimens, 15 representative specimens were selected for further analysis based on geographic location, postmortem lesions, case history, and virus concentration. DNA was extracted from ILTV-positive specimens (5x MagMax-96 viral isolation kit, Ambion 1836; Thermo Fisher Scientific, Waltham, MA) following the recommendation of the manufacturer for automatic extraction (Biosprint 96; Qiagen, Hilden, Germany). DNA was subjected to a PCR assay targeting the ICP4 gene. 16 Amplicons were purified following recommendations of the manufacturer (Amicon Ultra centrifugal filters, Ultracel-30K; Merck Millipore, Tullagreen, Carrigtwohill Co, Cork, Ireland) and forwarded to a commercial sequencing facility. A 996-bp fragment of the ICP4 gene (nucleotide positions 216–1212) was compared with reference sequences retrieved from GenBank using the multiple alignment program Geneious (v.10.2.5; Biomatters, Newark, NJ). Phylogenetic analysis using a maximum likelihood method was performed with the program MEGA (v.6, https://www.megasoftware.net/). The Tamura 3-parameter model of nucleotide substitution was used, and bootstrap values were calculated using 1,000 replicates. The following reference sequences (GenBank accessions) were used in our analysis: USDA reference strain (JN542534); LT-Blen (JQ083493); Laryngo-Vac (JQ083494); LT-Ivax (JN580312); Chinese isolate WangGang (DQ995291); and a Russian isolate (MF405079).
Results
Case submissions
BYF submissions to the CAHFS laboratories from January 1, 2007 to December 31, 2017 totaled 8,656; ILT was diagnosed in 88 BYF chicken cases involving 149 birds. The number of submitted birds for each case was 1–11, with most cases having 1 or 2 birds submitted, and included live and dead birds. The percentage of total BYF submissions that were diagnosed with ILT per year followed an undulating pattern every 4–5 y (0.19–1.70%; Fig. 1). The highest percentages of BYF submissions diagnosed with ILT were in northern, central, and southern regions of California (Fig. 2). Commercial meat and layer chicken flock premises are located primarily in the Central Valley of California (Fig. 3).

The percentage of CAHFS backyard flock (BYF) submissions diagnosed with infectious laryngotracheitis (ILT) from 2007 to 2017, by year.
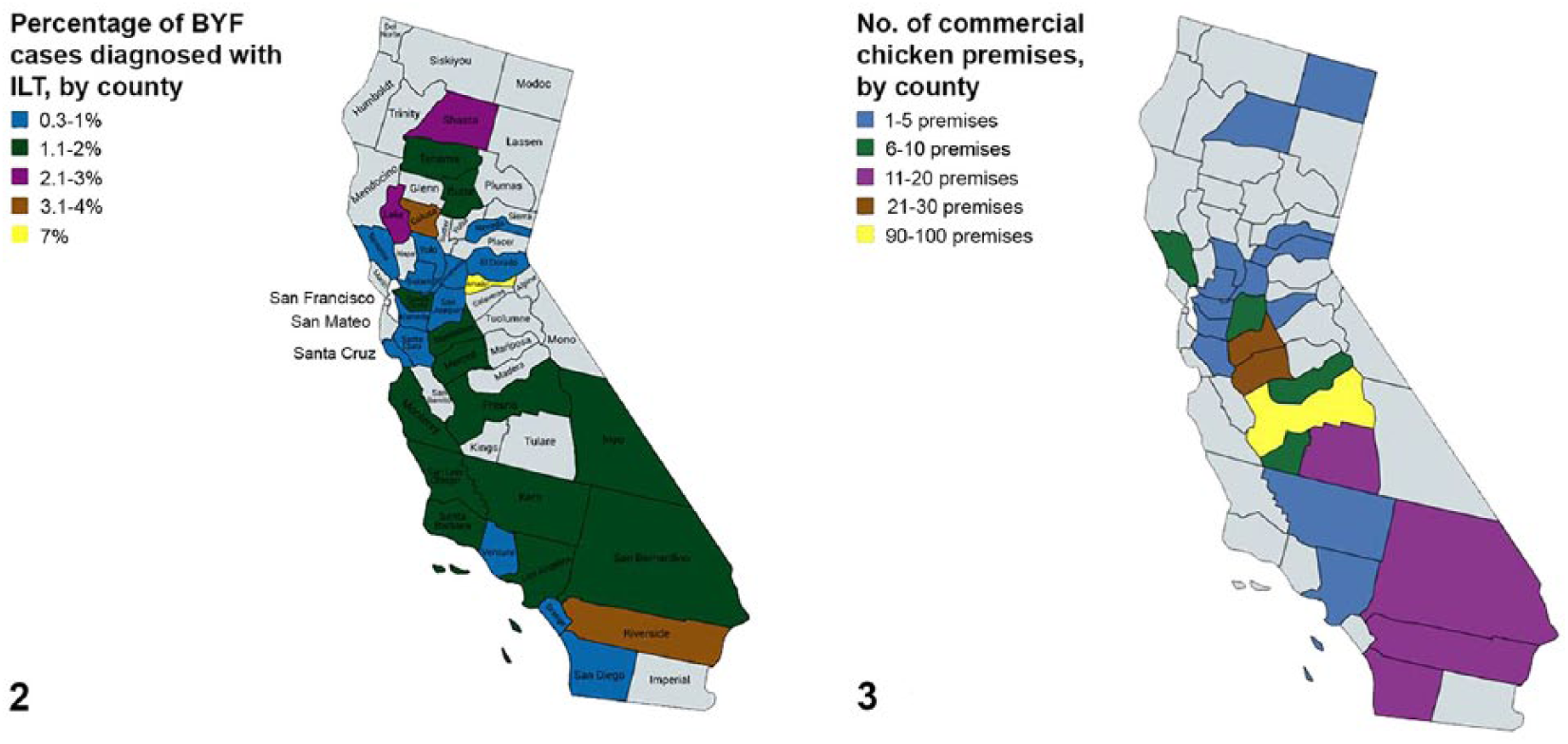
California counties by prevalence of backyard flock (BYF) infectious laryngotracheitis (ILT) and concentration of commercial chicken premises based on submissions to CAHFS from January 1, 2007 to December 31, 2017.
Summary of history and clinical presentation
BYF owners frequently reported respiratory signs, including dyspnea, coughing, sneezing, and rales (51 of 88 cases). Ocular and nasal discharge was frequently observed (26 of 88 cases), with death or sudden death reported in 22 of 88 cases. Signs observed less frequently were conjunctivitis (11 of 88 cases), lethargy (6 of 88), poor health (3 of 88), and ataxia or convulsions (2 of 88). Sinusitis, poor body condition, high mortality, bloody oral discharge, and no signs observed were all reported in one case each.
Postmortem examination, histopathology, and IHC
Given the complicating factor of coinfections, we analyzed only gross anatomic lesions involving the conjunctiva and trachea. Tracheal lesions consisted of mild-to-severe reddened mucosa, excess mucus in the tracheal lumen, fibrinonecrotic exudate, and hemorrhage (Figs. 4–7; Table 1).
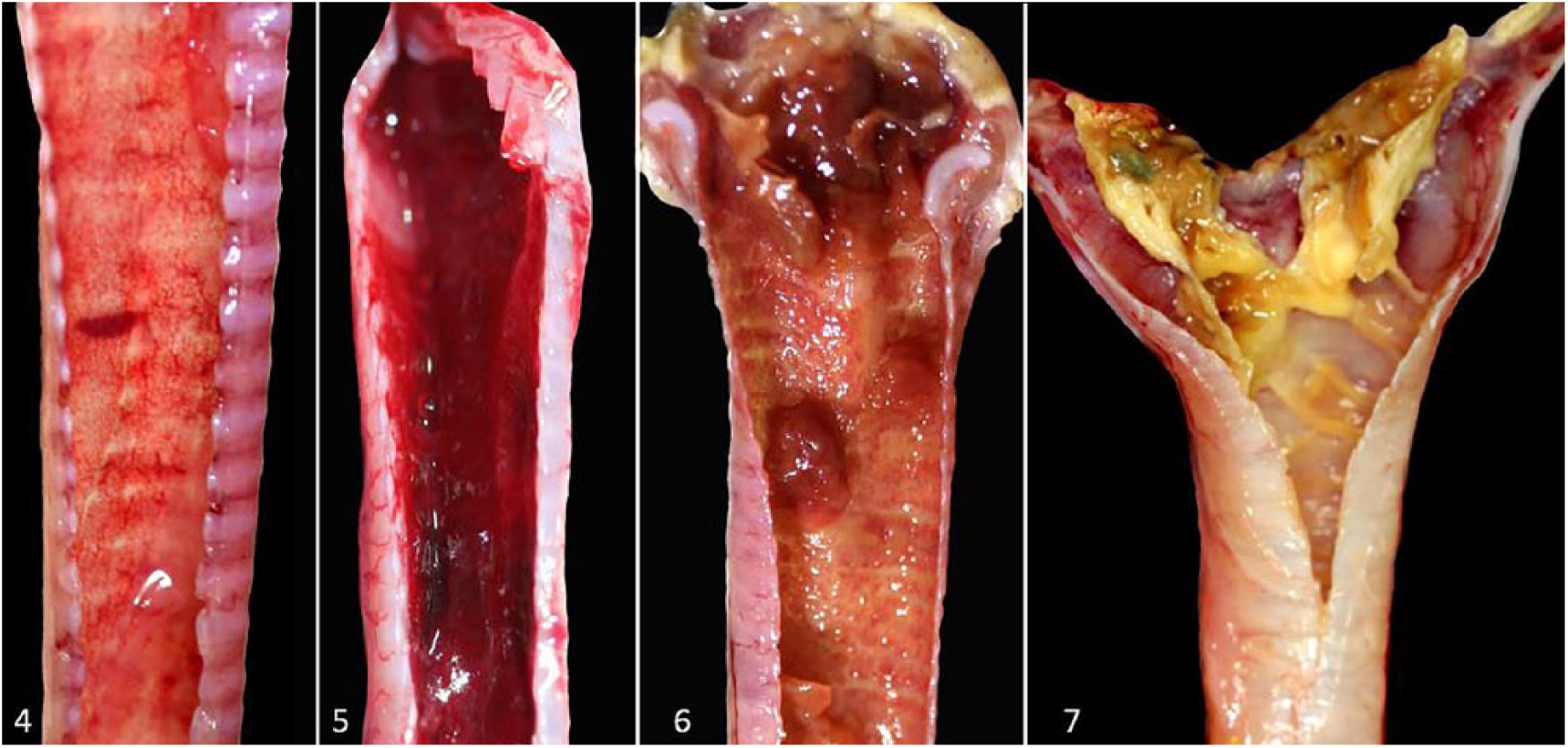
Mild tracheitis with clear mucus in the lumen and reddening of the tracheal mucosa.
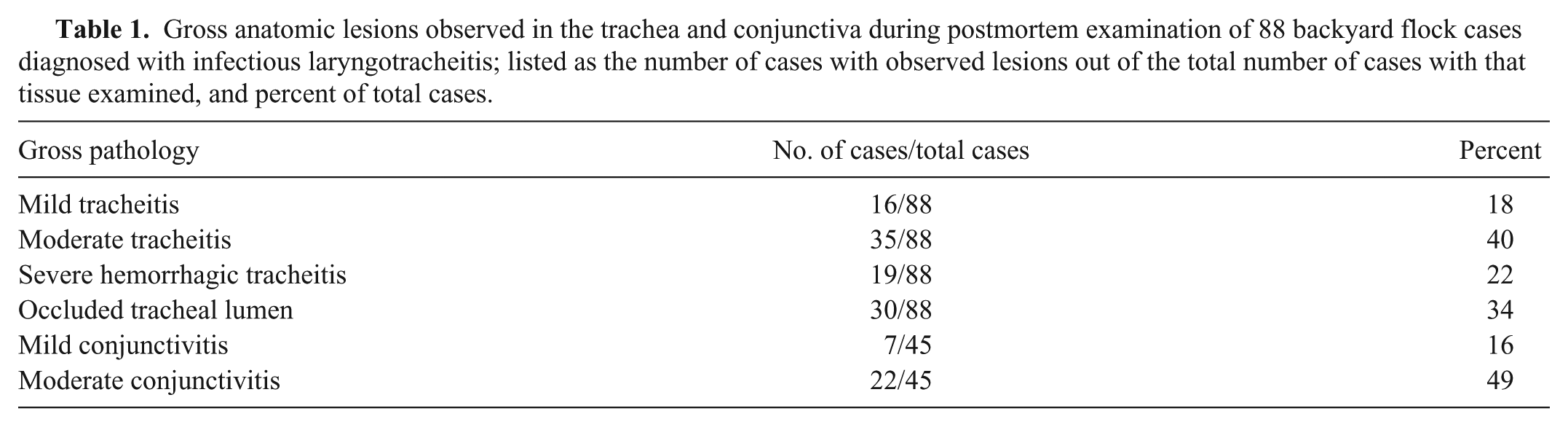
Gross anatomic lesions observed in the trachea and conjunctiva during postmortem examination of 88 backyard flock cases diagnosed with infectious laryngotracheitis; listed as the number of cases with observed lesions out of the total number of cases with that tissue examined, and percent of total cases.
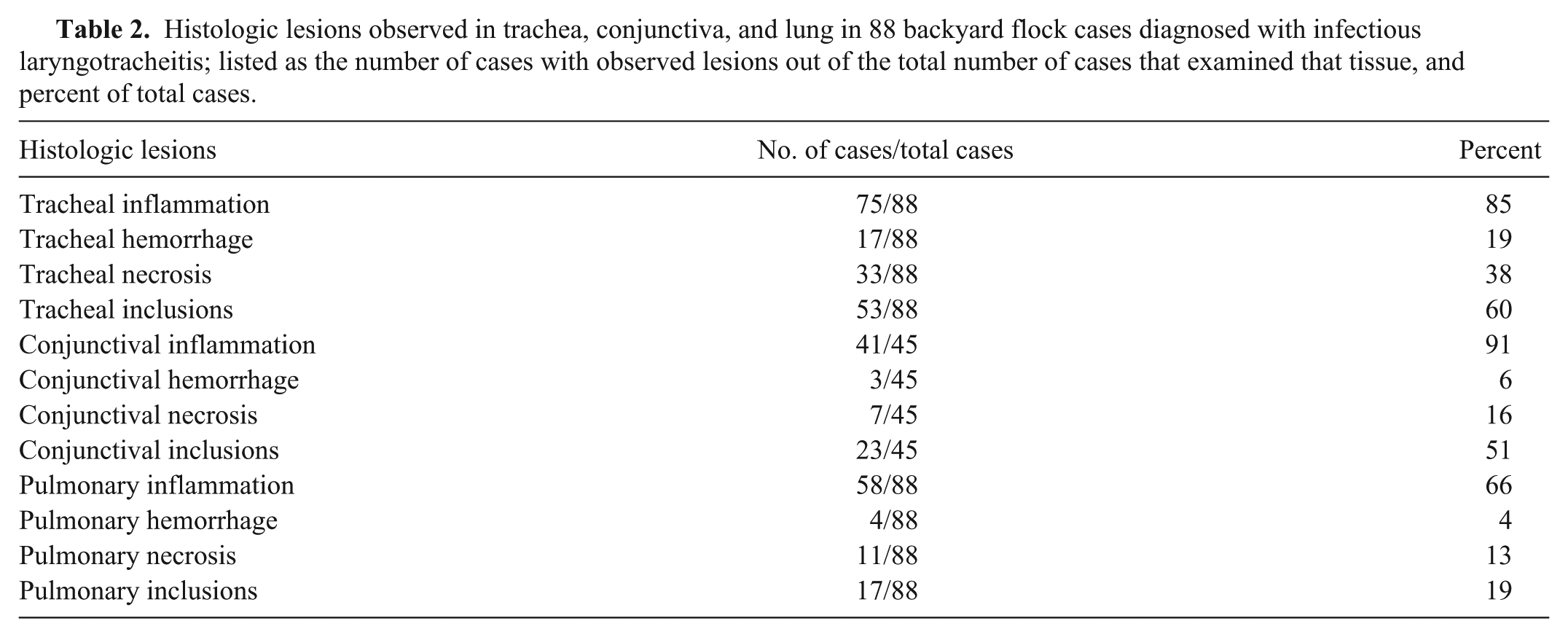
Given the complicating factor of coinfections, we analyzed only histologic lesions involving the conjunctiva, trachea, and lung (Figs. 8, 9). Lymphoplasmacytic inflammation, hemorrhage, epithelial cell necrosis, syncytia, and INIBs were observed (Table 2). INIBs were reported in at least 1 organ in 62 cases. Twenty-eight cases contained INIBs in tracheal sections only, and 10 cases contained INIBs in conjunctival sections only. No cases contained INIBs in lung sections only.
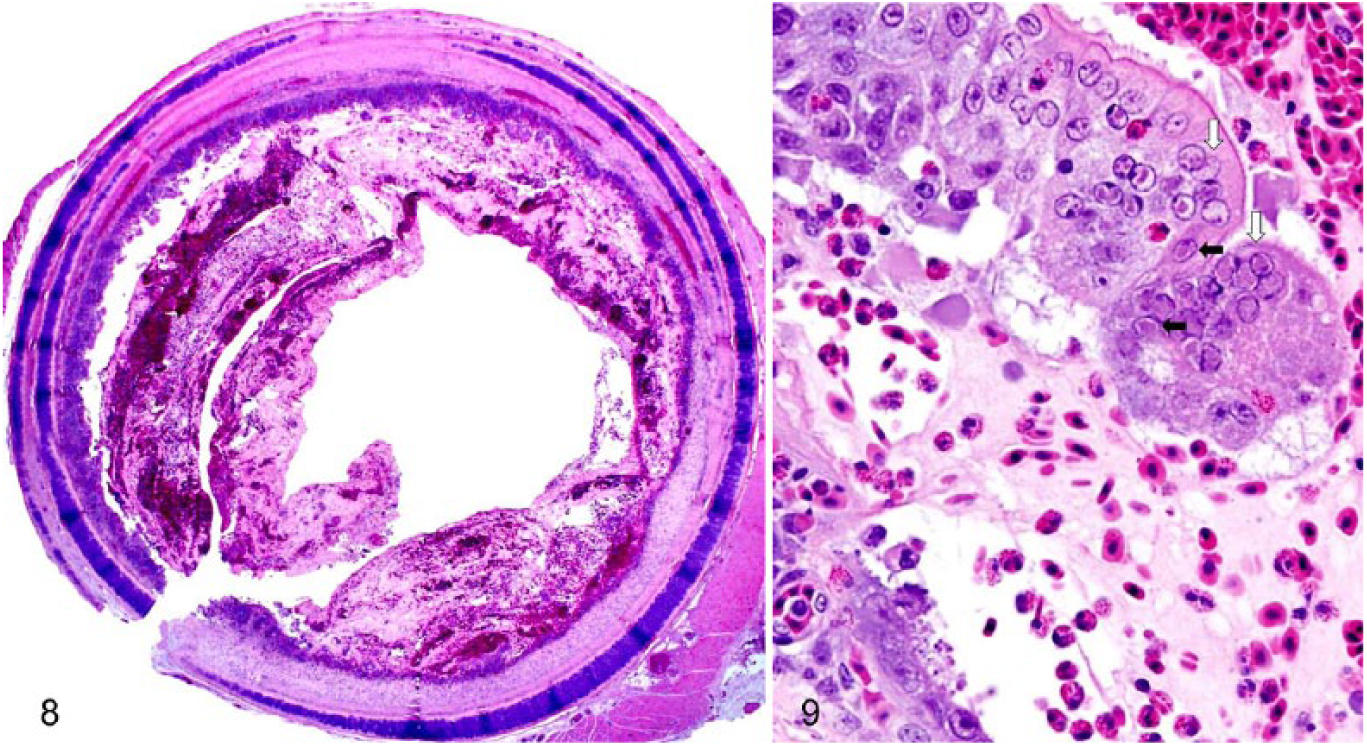
The tracheal lumen is narrowed by mucohemorrhagic exudate with fibrinonecrotic debris. H&E.
Histologic lesions observed in trachea, conjunctiva, and lung in 88 backyard flock cases diagnosed with infectious laryngotracheitis; listed as the number of cases with observed lesions out of the total number of cases that examined that tissue, and percent of total cases.
IHC for ILTV on tracheal sections was performed in 6 cases, with 5 cases resulting in a positive IHC and 1 case declared negative. The one negative IHC case was diagnosed as ILT by a positive ILTV rtPCR from a tracheal swab. IFA testing for ILTV on tracheal sections was performed in 29 cases: 24 cases resulted in a positive IFA, 1 case had a suspicious IFA, and 4 cases had a negative IFA. The 4 negative IFA cases were diagnosed as ILT by identifying INIBs in the trachea, conjunctiva, or lung in all 4 cases, with 2 cases also positive for ILTV by IHC on tracheal sections.
Microbiology
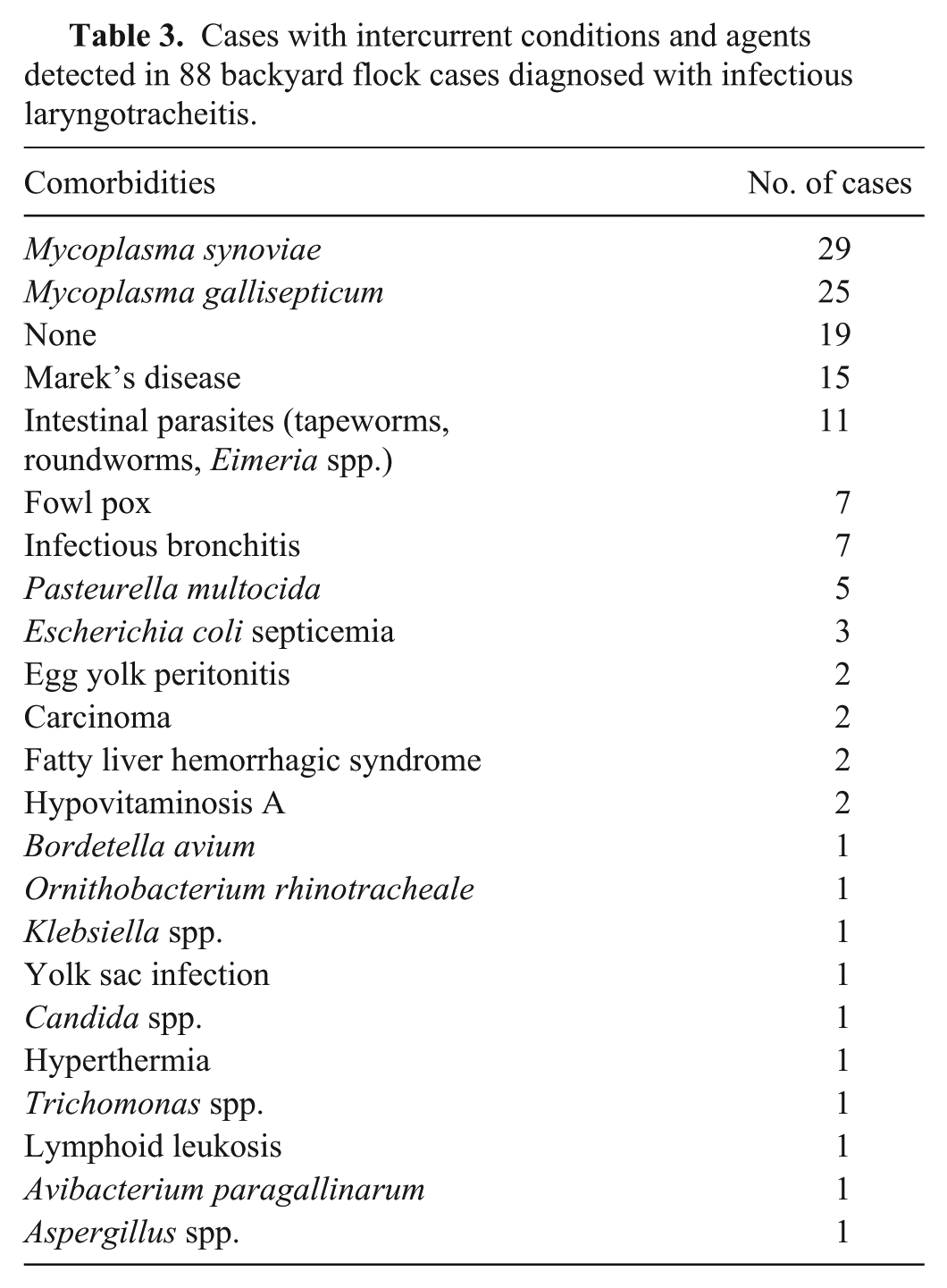
Various comorbidities, including bacterial, metabolic, and other viral agents, were detected in all birds (Table 3), with MS detected most frequently (33% of cases).
Cases with intercurrent conditions and agents detected in 88 backyard flock cases diagnosed with infectious laryngotracheitis.
PCR
Although we analyzed electronic data from 2007, the ILTV rtPCR was implemented at CAHFS for routine use in 2014. ILTV was confirmed by rtPCR from tracheal swabs in 40 of 40 cases in which it was used from 2014 to 2017.
Electron microscopy
DEM was performed on tracheal sections in 6 cases, with 4 cases yielding herpesvirus-like viral particles, and 2 cases reported as negative. The 2 DEM-negative cases were diagnosed as ILT by identifying INIBs in the trachea, conjunctiva, and lung on H&E in the first case, and by a positive IHC from tracheal sections in the second case.
ICP4 sequencing
We compared partial ICP4 sequences from 15 BYF ILTV strains with reference strains, including commonly used vaccine strains and several field strains from other countries (Fig. 10). Nine of the ILTV strains were 100% identical to the LT-Blen vaccine strain in the ICP4 region analyzed. Another 5 were 98.8% identical to the LT-Blen vaccine strain, except for a 12-bp insertion/deletion (indel) near the 3’-end of the ICP4 region analyzed. Strain S1608078 had the same 12-bp indel as well as 6 additional single-nucleotide polymorphisms (SNPs; Fig. 11). Across the ICP4 region analyzed, strain S1608078 was 99.9% identical to the Chinese isolate WangGang, 99.6% identical to the USDA reference strain, and 98%, 98.2%, and 99.6% identical to the vaccine strains Laryngo-Vac, LT-Blen, and LT-Ivax, respectively. Most statistical methods for phylogenetic estimation (including maximum likelihood) treat a gap or indel within the input sequence alignment as missing data, and therefore the 12-bp indel cannot be classified visually.
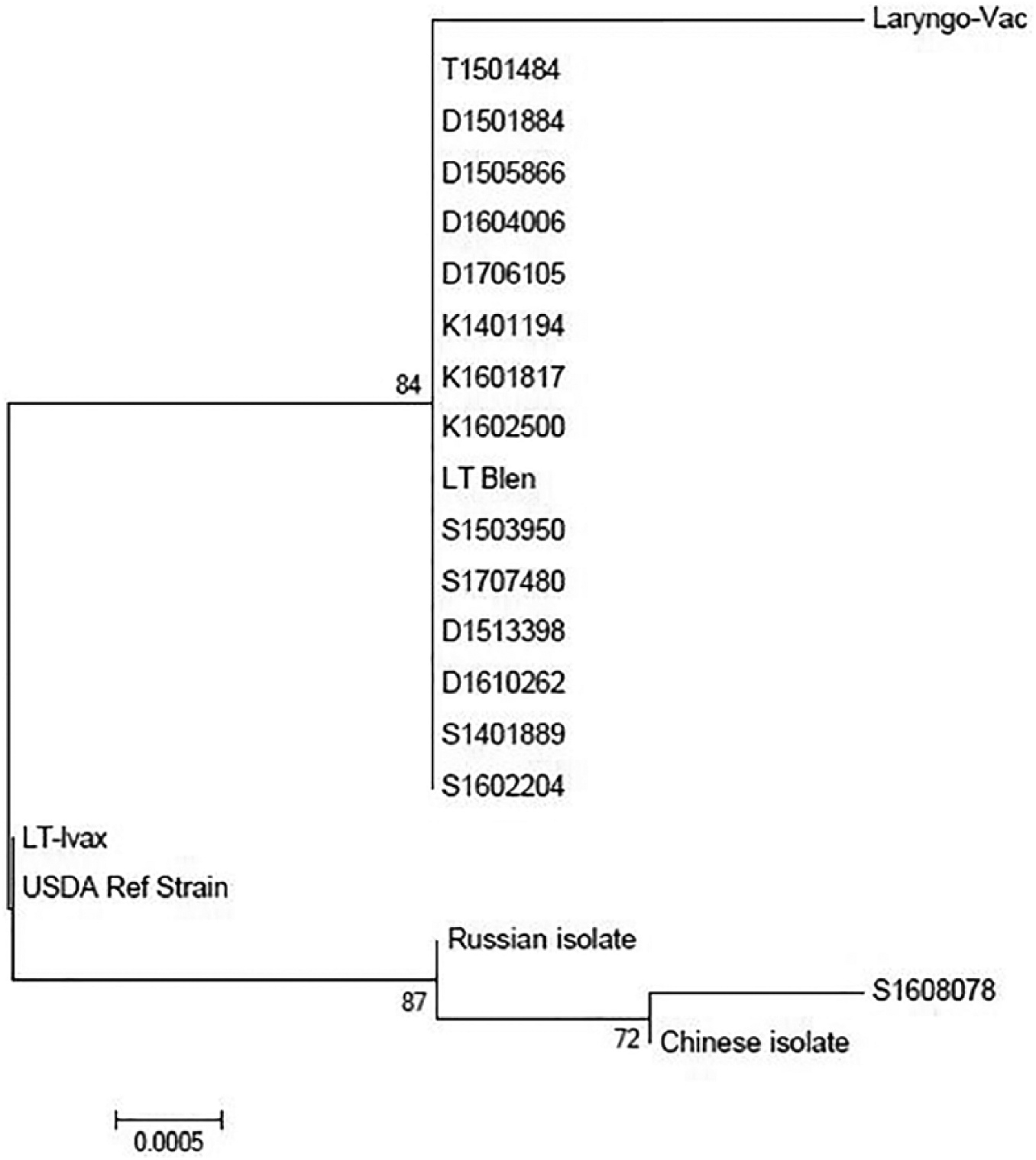
Phylogenetic analysis of the ICP4 sequences from 15 backyard flock infectious laryngotracheitis (ILT) isolates, 2 chicken embryo origin ILT vaccines (Laryngo-Vac and LT-Blen), 1 tissue culture origin ILT vaccine (LT-Ivax), the USDA ILT reference strain, a Russian ILT isolate, and the Chinese ILT isolate WangGang.
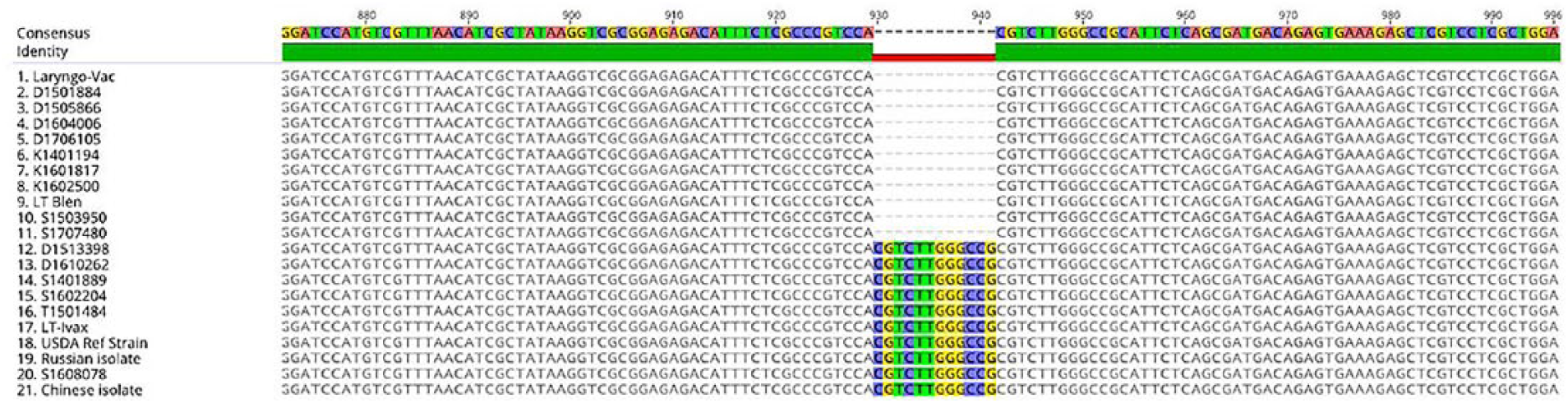
Sequence homology of 996-bp of the ICP4 gene in 15 backyard flock infectious laryngotracheitis (ILT) isolates, 2 chicken embryo origin ILT vaccines (Laryngo-Vac and LT-Blen), 1 tissue culture origin ILT vaccine (LT-Ivax), the USDA ILT reference strain, a Russian ILT isolate, and the Chinese ILT isolate WangGang.
Discussion
All 88 BYF submissions diagnosed with ILT over the studied 10 y were chickens, and the numbers of cases were presented in an oscillating pattern with peaks at 1.7% and valleys from 0.19% to 1%. Every 4–5 y, the incidence peaked to 1.6–1.7%. We did not evaluate the yearly incidence of ILT in surrounding commercial premises; however, earlier observers proposed potential ILT transmission between premises in close proximity. 4 Proximity of BYFs to commercial flocks enhances the potential risk of ILTV vaccine escape from vaccinated commercial birds and reversion to virulence by circulating in naive commercial and BYF birds. 10 In our study, the BYF ILT cases were concentrated throughout northern, central, and southern California with the highest percent of BYF ILT cases identified in Amador County. Commercial chicken premises in California are most concentrated in Fresno County, with high concentrations of premises also in southern and northern California. A previously published analysis 20 of ILT diagnoses in commercial and BYF chickens in California in 2000–2012 also reported a concentration of ILT cases in central California, proposing a risk of potential disease transmission between these flock types. 12
The mild clinical form of ILT is the most common form, and it includes depression, mild respiratory signs, conjunctivitis, and nasal discharge. The severe form of ILT involves dyspnea, expectoration of bloody mucus, and high mortality. 19 In our study, only 22% of cases reported macroscopic lesions of hemorrhagic exudate in tracheas; 40% reported fibrinonecrotic exudate in the larynx and trachea.
Aids for the diagnosis of ILT at CAHFS include histopathology, rtPCR, IFA, IHC, DEM, and virus isolation. Virus isolation is not frequently performed in BYF submissions because of cost concerns. A definitive microscopic diagnosis is possible when INIBs are present; however, these inclusions occur only during the early phase of infection. 6 One to 2 d post-infection, the tracheal lamina propria is infiltrated with mixed inflammatory cells, followed by epithelial syncytial formation 3 d post-infection. INIBs are only present in tracheal and conjunctival epithelial cells at 1–5 d post-infection, and are lost during necrosis and desquamation of infected cells. INIBs may be observed in sloughed epithelial cells in the bronchi as a result of desquamation and migration into the lower respiratory tract.10,19 INIBs were noted in 70% of our BYF cases, with most inclusions observed in the trachea (85% of cases with INIBs present). Although the conjunctiva was not evaluated histologically in every case, 10 cases contained INIBs only in conjunctival sections and not in the trachea and lungs, emphasizing the importance of sampling all 3 tissue types for microscopic examination. Our findings support previously published results confirming the high sensitivity of molecular methods and the subjectivity of microscopic evaluation.2,6,19,21 All submissions in which ILTV rtPCR was performed resulted in a positive diagnosis in our study, whereas H&E, IHC, IFA, and DEM had submissions that relied on a second detection method for a positive diagnosis.
Whole genome sequencing of ILTV provides the most complete genetic analysis and strain differentiation. The ICP4 gene is well conserved among alphaherpesviruses and allows differentiation between vaccine and field strains of ILTV.13,16,18,22 The ICP4 gene is frequently analyzed given its role in encoding a major regulatory protein involved in gene expression during early infection.13,16 The ICP4 gene contains regions that are highly conserved and regions that have fewer similarities, making it a target for analysis and strain differentiation. 13 Partial sequencing and analysis of the ICP4 gene provided comparable results to PCR-RFLP, validating the use of partial ICP4 gene sequencing for ILTV differentiation. 3 In our study, from the 15 ILTV strains that underwent partial ICP4 gene sequencing, 9 strains were 100% identical to the LT-Blen vaccine strain (CEO origin), whereas 5 strains analyzed as 98.8% homologous in the ICP4 region differed by a 12-bp insertion. A previous study analyzed a 592-bp sequence of ICP4 for 10 ILTV isolates, with 9 of 10 isolates 100% identical to CEO and TCO vaccine strains. The remaining isolate was 98.5% identical to LT-Blen, differing by a 9-bp insertion, and was qualified as CEO-related. 16 In our study, given the 100% and 98.8% homology to LT-Blen, these 14 strains were categorized as CEO-related and likely originated from an escaped CEO vaccine that had reverted to virulence. One ILTV strain had 99.9% sequence homology to a Chinese field isolate, as well as 99.6% homology to the USDA reference strain and LT-Ivax vaccine strain in the ICP4 region analyzed. Given the high sequence homology of this strain with multiple strains in GenBank, the exact origin of infection could not be determined. Further gene sequencing or whole genome analysis of this strain would provide further insight into its origin; however, further testing was not performed because of financial constraints.
Coinfections are important to consider when managing ILT because they often have an impact on disease severity and recovery. MS and MG were the most common coinfections at 33% and 28%, respectively, and are commonly reported pathogens in BYFs.7,12 Marek’s disease at an early age can interfere with protection inferred from ILTV vaccination and makes the host more susceptible to coinfections. 8 Marek’s disease is the most common cause of mortality in California BYFs and was a coinfection in 17% of cases in our study. 17 The ability of ILTV to remain in a latent state after recovery and to recrudesce when the host is stressed further emphasizes the importance of limiting coinfections to reduce stress on the host. 10 Control of coinfections is an important factor in ILT management and should not be overlooked.
Footnotes
Acknowledgements
We thank the University of California–Davis Biotechnology department for their support in performing the molecular testing, and Daniel Rejmanek for his expertise in performing the sequencing and phylogenetic analysis of the BYF isolates.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.