
Abstract
Dilated cardiomyopathy (DCM) is a myocardial disease characterized by ventricular chamber dilation associated with systolic myocardial dysfunction in the absence of other cardiac lesions. DCM occasionally develops in conjunction with proliferation of fibroelastic fibers in the endocardium, producing endocardial fibroelastosis (EFE). Although early reports describe EFE as a primary disease, evidence now suggests that EFE may develop as a response to myocardial dysfunction. Echocardiographic evaluation of a 4-wk-old Pallas cat (Otocolobus manul) with respiratory distress revealed enlargement of both atria, enlarged end-systolic left ventricular dimension, and left ventricular dilation. DCM was diagnosed, and the cat was euthanized, given the poor prognosis. Postmortem examination revealed pericardial effusion and biventricular and biatrial enlargement. The interventricular septum and free walls of ventricles were thin. Histologically, the endocardium of the left and right ventricles was diffusely thickened; Verhoeff–Van Gieson staining of the left ventricular endocardium revealed a moderate amount of endocardial accumulation of elastin and collagen. These fibers were more prominent in papillary muscles and around coronary blood vessels. Based on these findings, we diagnosed DCM with EFE. Cardiac diseases are rarely diagnosed in wild felids.
A 1-mo-old female Pallas kitten (Otocolobus manul) owned by a zoo was referred for echocardiographic examination after radiographic identification of cardiomegaly; preliminary echocardiographs were abnormal. The kitten was referred to the Cardiology Service at the Virginia Tech Veterinary Teaching Hospital (Blacksburg, VA). The affected kitten was one of a litter of 4 kittens. One kitten died at 1 wk of age after developing respiratory distress, but an autopsy was not performed. At the time of manuscript submission, the 2 surviving siblings are apparently healthy but were reported to have cardiac murmurs. The queen has not shown signs of illness, but her history includes the presence of a heart murmur.
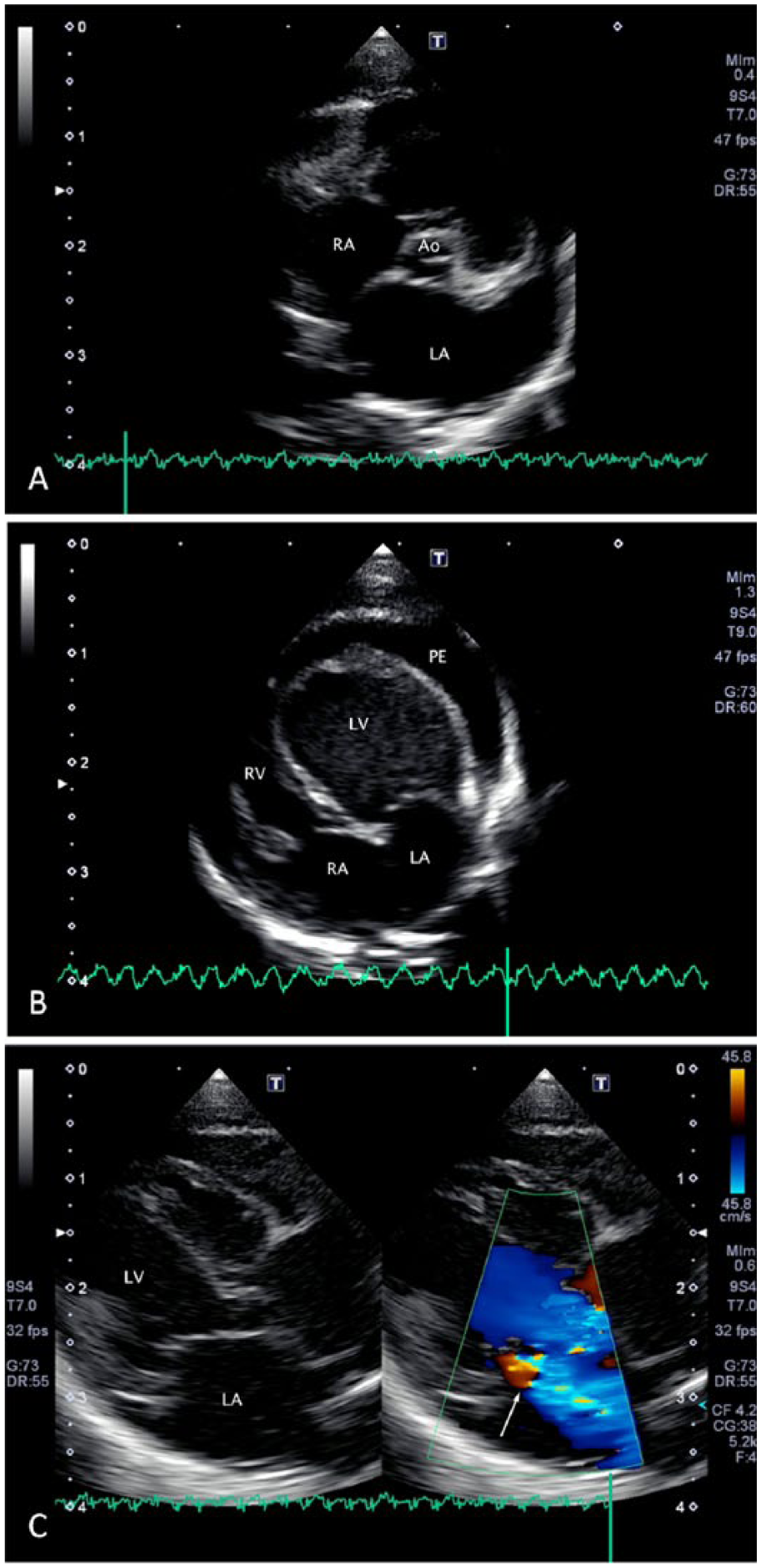
On presentation, the kitten was depressed and weak, body temperature was 38.3ºC, and the kitten was tachypneic (>60 breaths/min) with abnormal respiratory effort. Auscultation was impeded by the patient’s vocalization when restrained. Thoracic radiographs revealed a markedly enlarged cardiac silhouette, vertebral heart score of 11.5 (reference interval [RI] in adult cats is 6–8.1), and diffusely distributed interstitial and alveolar opacities compatible with cardiogenic edema. 6 Echocardiography was performed. Because echocardiographic RIs for patients of this age and species were not available, interpretation was based on evaluation of dimensions indexed to aortic diameter, comparison to RIs for domestic cats, and subjective assessment.1,19 There was moderate left ventricular dilation; the end-diastolic left ventricular internal dimension (LVIDd) was 13.8 mm. At 15%, left ventricular systolic performance evaluated by fractional shortening was reduced relative to healthy domestic cats (RI: 40–67%), and the end-systolic left ventricular internal dimension (LVIDs) of 11.7 mm (RI: 4–11.2 mm) provided evidence of systolic myocardial dysfunction (Fig. 1A). There was marked left atrial enlargement (Fig. 1B); the left atrial to aortic ratio from an M-mode echocardiogram directed by a short-axis, 2-dimensional image (LA:Ao) was 3.0 (RI: 0.96–1.4). Other findings, based on subjective evaluation, included dilated right ventricle and right atrial enlargement. The cardiac valves were structurally normal, but there was mild-to-moderate mitral valve regurgitation and mild tricuspid valve regurgitation (Fig. 1C). There was a small volume of circumferential but non-compressive pericardial effusion. Congenital malformations resulting in volume overload that might explain the echocardiographic appearance were not detected. Based on these findings, idiopathic myocardial disease was identified, and dilated cardiomyopathy (DCM) was diagnosed clinically.
Given the low probability of identifying a specific cause and a presumably poor prognosis, the kitten was euthanized at the owner’s request. Postmortem examination revealed pericardial effusion with 3 mL of serous fluid. The heart had biventricular and biatrial enlargement and weighed 6 g, resulting in a heart weight to body weight (HW:BW) ratio of 1.2% (BW = 500 g; HW:BW[%] = 6/500 × 100%); this higher value was expected based on the dilated condition of the heart and the age of the cat (RI in adult cats = 0.28–0.88%). 13 The walls of both ventricles were thin; the ratio of left ventricular to right ventricular wall thickness was 2:1 (Fig. 2A). Visceral pleural surfaces were glistening, and foamy fluid was present within the airways. Multiple organs and lower extremities were congested.
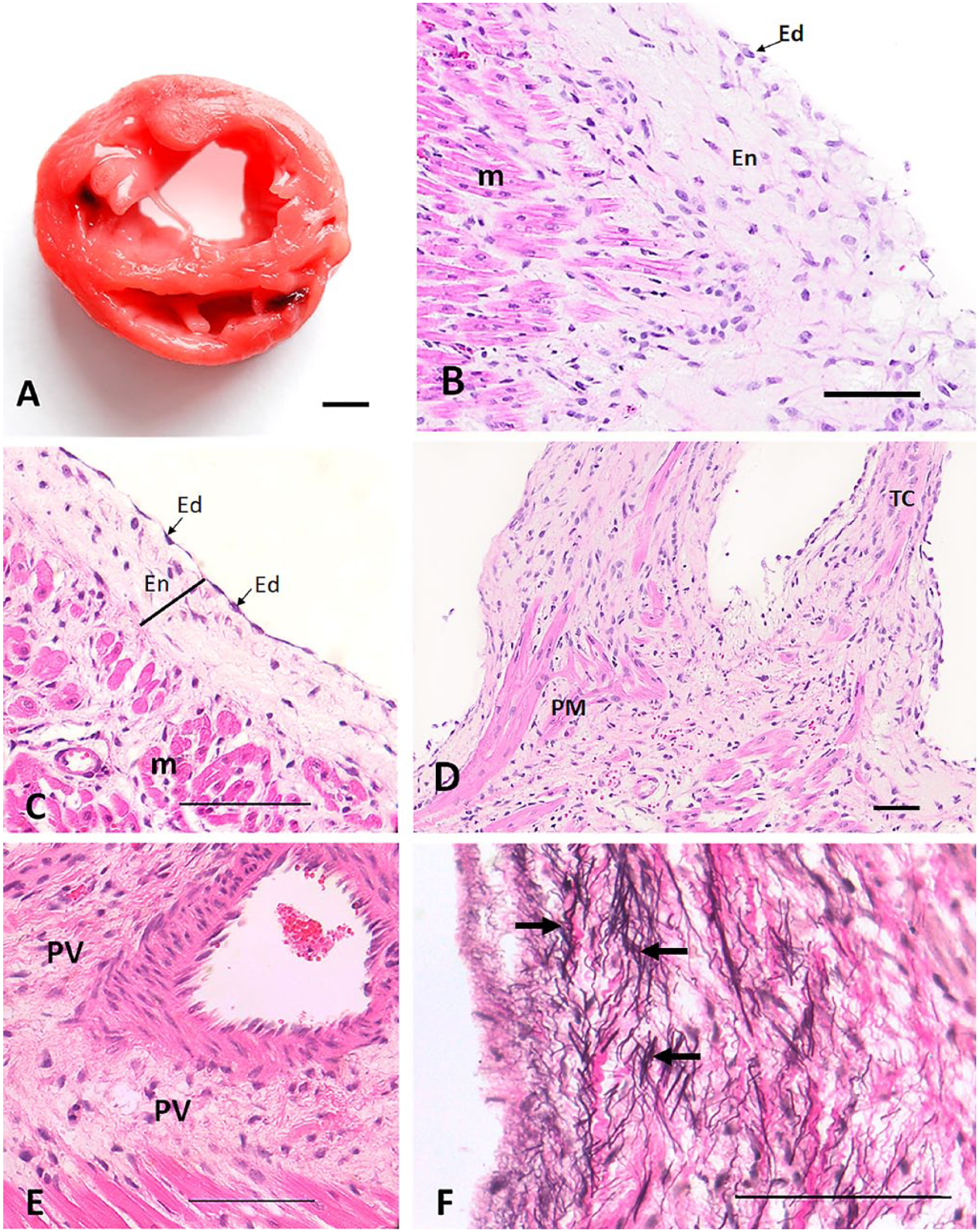
Histologically, the left and right ventricular endocardium was diffusely thickened by a layer of ~70–150 µm of collagen and other fibers, some of which extended into the adjacent myocardium. The papillary muscles of the right and left ventricle were the most severely affected. Verhoeff–Van Gieson staining of the heart showed, in addition to the collagen fibers abovementioned, moderate elastin accumulation in the endocardium, especially in the left ventricle and papillary muscles, compared to that of an age-matched control cat. Many coronary blood vessels were surrounded by small-to-moderate amounts of collagen and elastin (Fig. 2B–D). Some myocardial fibers were attenuated and wavy. In the lungs, alveolar septa were mildly and diffusely thickened and infiltrated by moderate numbers of macrophages. Alveolar spaces contained large amounts of edema fluid and large foamy macrophages.
Postmortem examination confirmed the clinical diagnosis of DCM with an accompanying histologic finding of EFE. DCM is defined as a myocardial disease that is characterized by left or biventricular chamber dilation associated with systolic myocardial dysfunction that develops in the absence of abnormal loading conditions or occlusive coronary artery disease. 8 The identification of genetic causes for many of the cardiomyopathies (CMs) observed in humans and the difficulty in making the distinction between CMs that exclusively affect the heart and those that are secondary to other disorders precludes definitive classification. In general, CMs are classified based on morphopathologic or functional characteristics. 8
DCM is described as a CM of “mixed” etiology. 8 Nutritional taurine deficiency was an important cause of DCM in domestic cats, but cat food is now supplemented appropriately and this form of CM has virtually disappeared. 12 The cause of DCM in the Pallas kitten reported herein can only be conjectured. The clinical presentation was inconsistent with that of nutritional taurine deficiency because DCM associated with taurine deficiency is generally observed in adult cats, but that doesn’t exclude the possibility of another nutritional deficiency, or an inborn metabolic defect causing myocardial dysfunction. In humans, mutations of genes that encode sarcomeric or cytoskeletal proteins are most commonly responsible for familial DCM. 5 DCM is sometimes the consequence of temporally distant myocarditis, although histologic evidence of inflammation might not be present. 20 Because the littermate that died was not subjected to clinical or postmortem examination, we cannot determine if that kitten succumbed to cardiac or other disease. However, the observation of respiratory distress prior to death suggests that cardiac disease might have been responsible and, therefore, genetic or infectious causes of the abnormalities described herein are possible. Given the absence of inflammation and our patient’s age, viral myocarditis does not seem a likely cause.
Histologically, EFE was present, which may be a primary disease process or secondary to another myocardial disease. A number of case reports describe an apparently congenital “primary” EFE, that is, EFE in the absence of other cardiac diseases, in human and dogs.4,17 As well, a familial form of EFE has been described in Burmese cats15,23; these patients generally developed heart failure associated with chamber dilation and systolic myocardial dysfunction at a young age.
The view that primary EFE is a clinical entity that is responsible for heart failure has been questioned, and it has been suggested instead that EFE represents a response to hemodynamic or other stressors associated with cardiac dysfunction. 7 This suggestion is supported by the observation that EFE was identified in a greater proportion of explanted cardiac specimens in a group of adult human patients subject to heart transplant for established causes of heart failure than in a group who received transplants as a result of idiopathic DCM. 3 Furthermore, ventricular dilation and congestive heart failure were observed in 2 of 6 neonatal Burmese cats that did not have grossly evident endocardial thickening, whereas left ventricular dilation was seen in 15 of 16 Burmese cats with grossly evident endocardial thickening. 24 Regardless, it seems unlikely that a disease process largely confined to the endocardium and subendocardium would result in systolic myocardial dysfunction, because endomyocardial fibrosis is an explanation for diastolic dysfunction with preserved systolic function in restrictive CM. 11
A number of causes have been offered for EFE, but none is germane to our case. EFE has been experimentally induced through surgical lymphatic obstruction and has been associated with congenital cardiac malformations.9,18 Perhaps of greater relevance, EFE in human infants has been associated with in utero infection with the mumps virus. Possibly relevant to our case, evidence of mumps virus infection has been documented in hearts of children with DCM and EFE that did not have histologic evidence of myocarditis. 10 Rubuloviruses have not been associated with disease in cats; however, other paramyxoviruses in cats have been reported to cause respiratory disease and may be associated with chronic kidney disease. 22 Additionally, in humans, EFE is observed in association with DCM as a result of genetic disorders, such as Barth syndrome, and in primary carnitine deficiency.2,21
Despite the high prevalence of CM in domestic cats, reports of cardiac disease in captive wild felids are sparse. A 2-y-old male European wildcat (Felis sylvestris) was reported to have DCM, and in 2018, EFE associated with DCM was documented in 2 related tiger cubs.14,16
Footnotes
Acknowledgements
We thank Dr. Paul Stewart for kindly providing the history and laboratory results of the patient prior to referral.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.