
Abstract
Immunohistochemistry (IHC) of tissue samples is considered the gold standard for diagnosing feline infectious peritonitis (FIP), and, in cats without body cavity effusion, IHC is the only method available to establish definitive antemortem diagnosis. However, IHC requires invasive tissue sample collection. We evaluated sensitivity and specificity of an immunocytochemical assay of fine-needle aspirates (FNAs) of mesenteric lymph nodes that can be obtained noninvasively by ultrasound-guided aspiration to diagnose FIP. FNAs of mesenteric lymph nodes were obtained postmortem from 41 cats suspected of having FIP based on clinical and/or laboratory findings. FIP was confirmed immunohistochemically in 30 cats. In the other 11 cats, a disease other than FIP, which explained the clinical signs, was diagnosed histopathologically. Immunocytochemistry (ICC) was performed as an avidin–biotin complex method using a monoclonal anti-FCoV IgG 2A. Sensitivity, specificity, negative and positive predictive values (NPV, PPV, respectively) including 95% confidence intervals (95% CIs) were determined. ICC was positive in 17 of 30 cats with FIP, but also in 1 of 11 control cats that was diagnosed with lymphoma. Sensitivity of ICC was 53% (95% CI: 34–72); specificity 91% (95% CI: 59–100); NPV 42% (95% CI: 22–63); and PPV 94% (95% CI: 71–100). In a lethal disease such as FIP, specificity is most important in order to avoid euthanasia of unaffected cats. Given that a false-positive result occurred and FIP was correctly detected in only approximately half of the cases of FIP, ICC of mesenteric lymph node FNA alone cannot reliably confirm or exclude FIP, but can be a helpful test in conjunction with other diagnostic measures.
Keywords
Introduction
Feline infectious peritonitis (FIP) is a lethal disease that occurs worldwide within the cat population. There is no effective treatment.9,18 Definitive diagnosis therefore is crucial in order to avoid euthanasia of unaffected cats. However, antemortem diagnosis of FIP in clinical cases is still challenging, especially in cats without body cavity effusion. The difficulty in establishing a diagnosis originates from the existence of 2 pathotypes of the causative agent, the feline coronavirus (FCoV), which cannot be distinguished by routine laboratory testing. After infection via the fecal–oral route and replication of feline enteric coronavirus (FECV) in the intestinal epithelium,11,28,34-36 FECV can undergo mutations within an infected cat, by which feline infectious peritonitis virus (FIPV) arises.39,42 Both FECV and FIPV infect macrophages, but only the disease-causing FIPV is able to efficiently replicate within macrophages and to maintain replication at a level sufficient to cause disease.4,40 Additionally, various environmental and host factors have been proposed to play a role in FIP pathogenesis. Age at the time of infection, the proportion of cats shedding FCoV in a cattery or household, stress (e.g. of a surgery), and a complex genetic susceptibility have been shown to be associated with the risk of FIP development.10,11,14,22,38,43
In general, assays performed on effusions, although not specific for FIP, have much better predictive value than assays using blood. 17 Immunofluorescence staining of FCoV antigen in macrophages in effusion samples has previously been shown to have excellent specificity for the diagnosis of FIP.3,17,20,31 However, more recent studies revealed false-positive results of immunostaining of effusion samples in cats with diseases other than FIP.7,29 Moreover, in cats suspected of having FIP without effusion, an appropriate sample type has still to be identified. Positive immunostaining of macrophages in the cerebrospinal fluid (CSF) of cats with FIP has been reported,15,23 but this approach requires tapping of CSF, and positive results in cats not suffering from FIP have been described. 15 Newly developed reverse-transcription PCR (RT-PCR) tests seem capable of distinguishing FIPV and FECV pathotypes by detecting FCoV spike gene mutations. 8 However, RT-PCR methods also are not very useful in cats without effusion, because the sensitivity is very low if blood is used given the very low virus load.5,8,37
The immunohistochemical demonstration of FCoV antigen in macrophages in tissue lesions is considered the gold standard for the diagnosis of FIP.2,13,27,33 If used antemortem, this technique, however, requires invasive tissue collection. Lesions typical for FIP contain FCoV antigen to variable extents.25,32 In one study, fine-needle aspiration (FNA) of liver and kidney was used for staining by immunocytochemistry (ICC), but sensitivity was very low, given that staining of FCoV was only positive in 5 of 16 liver and 2 of 19 kidney samples of cats with FIP. 12 Mesenteric lymph nodes are among the organs known to exhibit a relatively high viral load21,37 and are commonly enlarged in cats with FIP. They can be sampled easily by minimally invasive ultrasound-guided FNA, especially if enlarged. Thus, FNA specimens of mesenteric lymph nodes could provide valuable tissue samples for FCoV antigen staining in cats suspected of having FIP.
We evaluated the sensitivity and specificity of an ICC assay in FNA specimens of mesenteric lymph nodes in cats with confirmed FIP and a defined control group of cats for which FIP was considered an important differential diagnosis by the clinician, but which were diagnosed definitively with another disease. We hypothesized that this minimally invasive technique would allow a definitive antemortem diagnosis of FIP in cats without effusion, thereby finding a relatively noninvasive method for sample collection.
Materials and methods
Cats
Overall, 41 cats that were presented either as patients to the Clinic of Small Animal Medicine (Centre for Clinical Veterinary Medicine, Ludwig-Maximilians-Universitaet, Munich, Germany; n = 28) or directly submitted for autopsy to the Institute of Veterinary Pathology (Centre for Clinical Veterinary Medicine, Ludwig-Maximilians-Universitaet; n = 13) were included in the study between 2012 and 2014. Cats were eligible for inclusion only if they showed one or more clinical and/or laboratory finding consistent with FIP, such as effusion (n = 31), fever with ≤20 × 109/L white blood cells and ≤1 × 109/L band neutrophils (n = 9), icterus (n = 20), neurologic signs (n = 9), uveitis (n = 3), or hyperglobulinemia (n = 10; Table 1). As a result, the study population reflected the cat population that is usually presented to a veterinary practice or clinic in which a clinician would consider FIP as a major differential diagnosis.
Signalment, clinical signs, results of immunocytochemistry and final diagnosis for all 41 included cats.
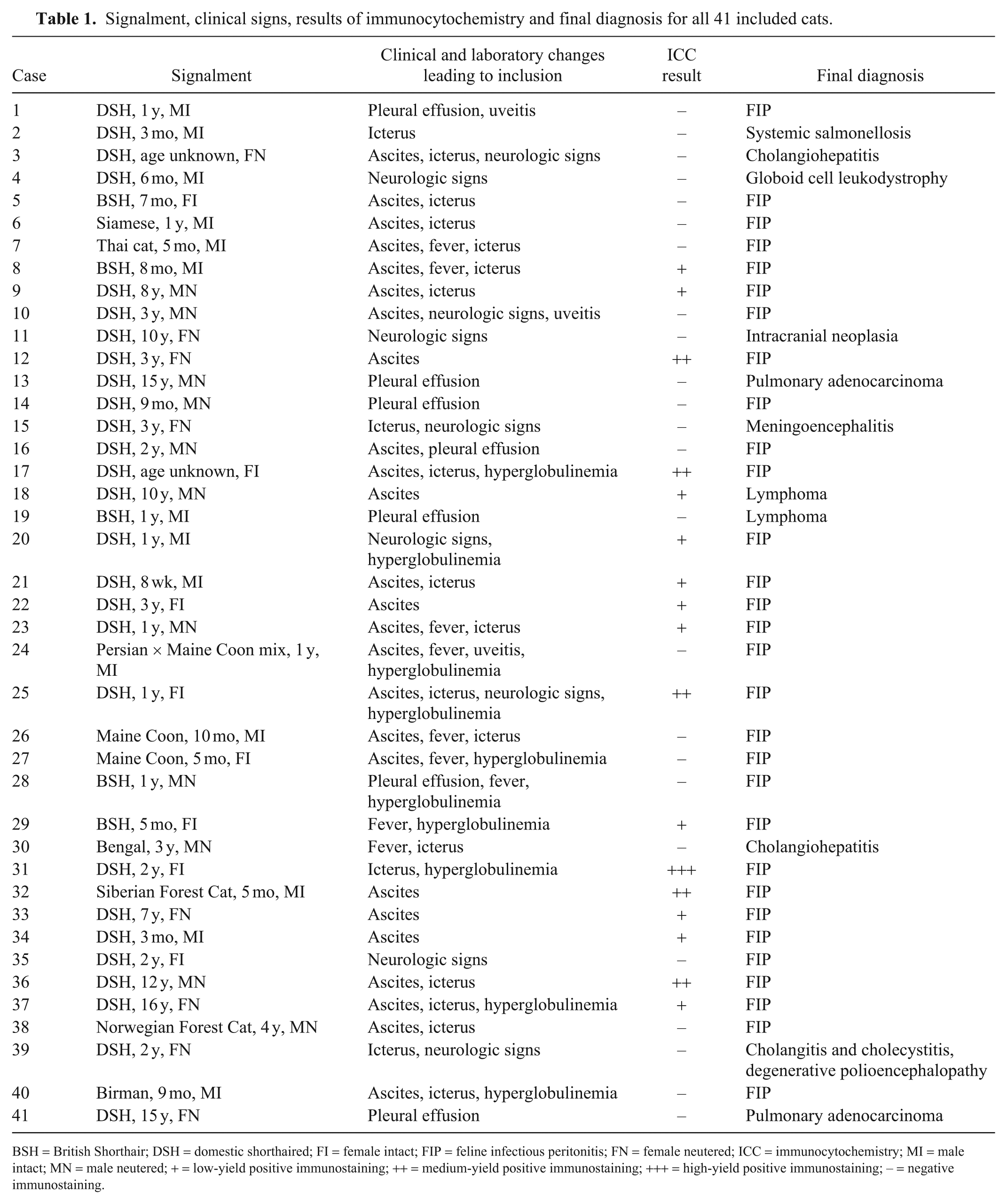
BSH = British Shorthair; DSH = domestic shorthaired; FI = female intact; FIP = feline infectious peritonitis; FN = female neutered; ICC = immunocytochemistry; MI = male intact; MN = male neutered; + = low-yield positive immunostaining; ++ = medium-yield positive immunostaining; +++ = high-yield positive immunostaining; – = negative immunostaining.
In 30 cats, FIP was confirmed by autopsy including histopathology and immunohistochemistry (IHC) of FCoV antigen in macrophages in tissue lesions (Table 1).
The control group included 11 cats for which FIP was initially considered an important differential based on the existence of one or more of the aforementioned clinical and/or laboratory changes. In all of the control cats, a disease other than FIP, which explained the clinical signs, was definitively diagnosed by autopsy including histopathology after the cats had been euthanized or had died as a result of disease progression (Table 1). In order to reduce the likelihood of missing FIP in control cats, immunohistochemical staining of different organs was performed in all cats, and cats had negative IHC results in all samples. The study population in part consisted of cats that had already been included in a previous study evaluating sensitivity and specificity of ICC analysis in effusion. 7
IHC
In all cats, tissue samples of various organs were obtained for immunohistochemical staining. Samples were fixed in 10% buffered formalin and processed routinely. For IHC, 5-µm sections of formalin-fixed, paraffin-embedded tissue samples were cut and dried overnight at 37°C. Sections were deparaffinized in xylene and rehydrated in a graded alcohol series. Microwave pretreatment using a citrate buffer (pH 6.0) was used for heat-induced antigen retrieval in order to reverse antigen-masking effects secondary to fixation. The staining procedure was performed as described for the immunocytochemical staining below.
Samples
FNA samples of mesenteric lymph nodes were obtained using a 21-G needle and a 5-mL syringe by aspirating lymph node material postmortem. One lymph node was used per cat, and each lymph node was sampled at least twice. If enlarged lymph nodes were present, they were preferred to normal-sized ones, given that enlarged lymph nodes would also be sampled in a clinical antemortem setting. After aspiration, cellular material was gently smeared onto a slide. At least 2 slides were prepared for each cat and stored at −20°C until processed.
ICC
To inhibit endogenous peroxidase, FNA samples were incubated with 2.3% hydrogen peroxide in 0.01 M phosphate-buffered saline (PBS; pH 7.0–7.4) for 35 min at room temperature; histologic samples were incubated with 3% hydrogen peroxide in methanol for 30 min at room temperature, thereby reducing background staining. Blocking was carried out using normal goat serum (1:20; MP Biomedicals Germany, Eschwege, Germany) for 30 min at room temperature to avoid nonspecific binding of the antibody. The primary antibody, an anti-FCoV mouse monoclonal IgG 2A (FIPV 3-70; Linaris Biologische Produkte, Dossenheim, Germany) validated for ICC, which was diluted 1:400 in PBS, was applied, and slides were incubated overnight at 4°C in a humidity chamber. The secondary antibody, a biotinylated goat anti-mouse IgG (Dako Deutschland, Hamburg, Germany) was diluted 1:200 in PBS and applied after washing the slides thrice in PBS. Slides were incubated for 1 h at room temperature in the humidity chamber. A complex of avidin and biotinylated horseradish peroxidase (ABC; Vectastain ABC kit, Vector Laboratories, Burlingame, CA) was performed and applied to the slides after 3 washing steps using PBS. Slides were again incubated for 1 h at room temperature in the humidity chamber. After 3 more washes in PBS, 3,3-diaminobenzidine tetrahydrochloride (DAB, pH 7.0; Kem-En-Tec Diagnostics, Taastrup, Denmark), which was used as a chromogen, was applied at an incubation time of 5 min. After washing in PBS, slides were counterstained with Mayer hemalum (PanReac AppliChem, Darmstadt, Germany) and then rinsed in running tap water for 20 min. Slides were dehydrated in an ascending alcohol series and coverslipped using a xylene-based mounting medium (Histokitt, Glaswarenfabrik Karl Hecht, Sondheim v. d. Rhoen, Germany). In order to ensure adequate antibody performance, a positive tissue control (brain tissue from a cat with confirmed FIP affecting the central nervous system) was included in every immunocyto- and immunohistochemical staining protocol.
Immunostained slides were interpreted by 2 independent investigators using light microscopy. All slides were first assessed cytomorphologically and evaluated for cell harvest. Only slides containing >50 nucleated cells in total were further evaluated. The investigators were blinded to all data of the cats, including their final diagnoses. A sample was defined as ICC-positive if it contained macrophages exhibiting dark-brown material with granular appearance within the cytoplasm (Fig. 1). A sample was defined as ICC-negative if it did not contain any immunostained macrophages. ICC-positive samples were further assessed considering their yield of ICC-positive macrophages. Samples were semi-quantitatively categorized as either low-yield positive (a few single macrophages with strong positive signal), medium-yield positive (approximately half of the macrophages with strong positive signal), or high-yield positive (majority of macrophages with strong positive signal).
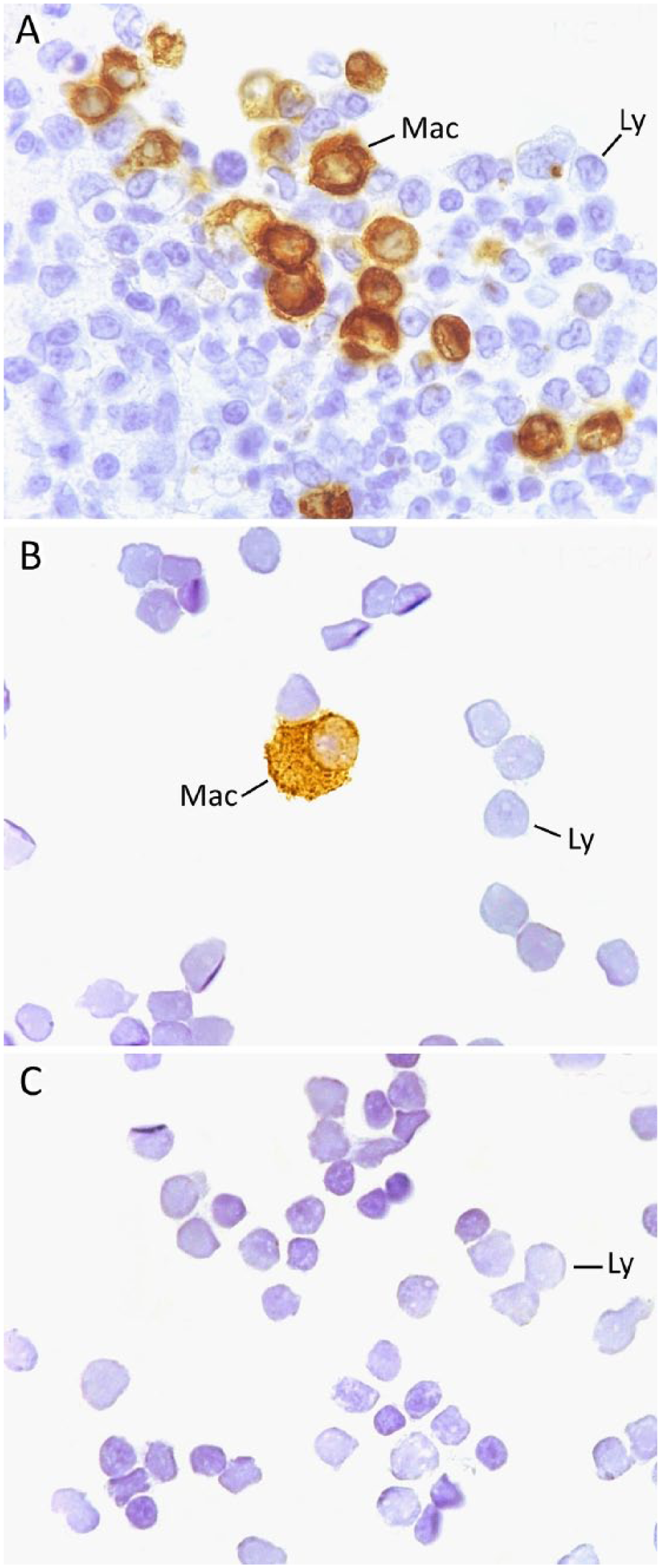
Immunohistochemistry (IHC) and immunocyto-chemistry (ICC) findings of feline mesenteric lymph nodes.
Statistical evaluation
Sensitivity, specificity, NPV (negative predictive value), and PPV (positive predictive value) were determined, and the respective 95% confidence intervals (95% CIs) were calculated.
Results
All slides were of adequate cellularity. Positive ICC results were obtained in 17 mesenteric lymph node FNA samples (Tables 1, 2, Fig. 1). ICC was positive in 16 of 30 cats with confirmed FIP. It was also positive in 1 of 11 control cats. The cat with the false-positive ICC result suffered from lymphoma involving liver, pancreas, and thymus. Diagnosis of lymphoma was established based on the results of postmortem examination and histopathology of various organs. IHC for FCoV of liver, pancreas, and thymus was negative in this cat. Specificity of the ICC assay in mesenteric lymph node FNA samples was 91%, and sensitivity was 53% (Table 3).
Results of immunocytochemistry in 41 mesenteric lymph node fine-needle aspirates.
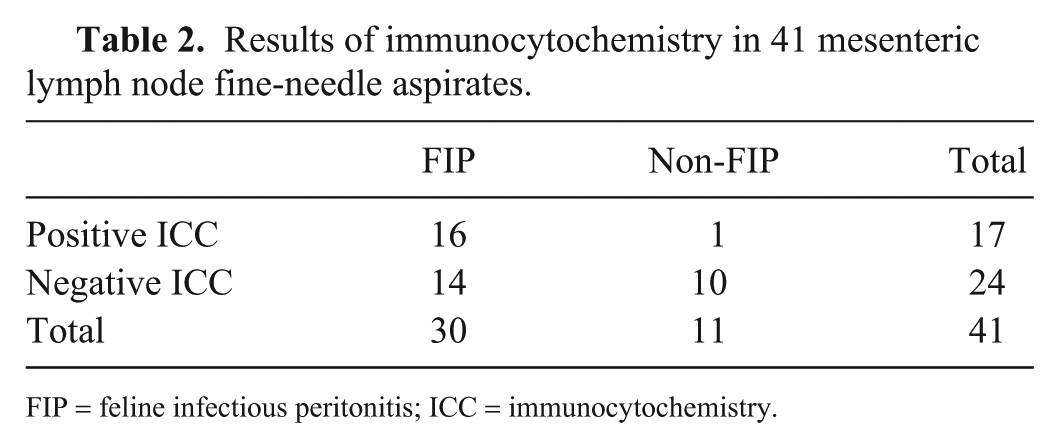
FIP = feline infectious peritonitis; ICC = immunocytochemistry.
Sensitivity, specificity, negative predictive value, and positive predictive value of immunocytochemistry and prevalence of feline infectious peritonitis.

FNA = fine-needle aspiration; ICC = immunocytochemistry; NPV = negative predictive value; PPV = positive predictive value. Numbers in parentheses are 95% confidence intervals.
Discussion
One false-positive ICC result occurred and thus, diagnostic specificity of the ICC in lymph node FNA was only 91%. To date, there are no evaluations of immunostaining of lymph node FNA in the diagnosis of FIP, to our knowledge. Immunostaining, predominantly immunofluorescence, has been used commonly in the past, mainly using effusion material. In these previous studies, specificity and PPV were 100% for effusion.3,17,20,31 However, false-positive results have been demonstrated in 2 studies evaluating immunostaining in effusions, and specificity was only 71% and 72%.7,29 Additionally, specificity of ICC in CSF analysis has been shown to reach only 83%. 15
Still, the detection of a false-positive result of the ICC in lymph node FNA was unexpected, given that the IHC detection of FCoV antigen in macrophages in histologic samples has a specificity of 100% 41 and is considered the gold standard for the diagnosis of FIP.2,13,27,33 One would expect that immunostaining of cellular material collected from a tissue such as the mesenteric lymph node would produce similar specificity. In a fatal disease such as FIP, high specificity of a laboratory test is crucial in order to avoid euthanasia of unaffected cats.
The control cat in which the false-positive result was detected was diagnosed through autopsy and histopathology to have lymphoma involving the liver, pancreas, and thymus. Immunohistochemical staining was performed on various tissues exhibiting macroscopic lesions, and FCoV antigen was not detected.
There are a few explanations for the false-positive result. FIPV replication is restricted to macrophages; thus, immunostaining of FCoV antigen can only be found within the cytoplasm of macrophages.1,25,26,40,44 The primary antibody that we used is known to be specific for the FCoV nucleocapsid. It is conceivable, however, that the antibody is able to bind nonspecifically to other antigens, such as cellular structures of neutrophils or other cells, thereby producing nonspecific immunostaining. Thus, misclassification of other cells as macrophages could lead to false-positive ICC results. Nevertheless, macrophages can easily be differentiated in cytologic specimens such as lymph node FNA and thus, it seems unlikely that a mistake in identifying macrophages could have caused the false-positive result. Nonspecific binding of the antibody to non-FCoV antigens within the cytoplasm of macrophages, however, could explain the false-positive result.
We cannot exclude the possibility that the cat with the false-positive ICC result had comorbidity of lymphoma and early-stage FIP, but without histologic evidence of FIP-typical lesions. FIP develops as a result of mutations of FECV within an infected cat.39,42 Mutations of FECV become more likely if there is more viral replication in the intestinal epithelium, which is the case during any state of immunosuppression. 39 Thus, lymphoma in this cat might have induced immunosuppression, which resulted in enhanced viral replication and ultimately in the mutation of an FECV with which the cat had already been infected. Given that IHC was performed from sections of paraffin-embedded tissue, and FCoV antigen is variably distributed within FIP lesions and often absent in granulomas without extensive necrosis, 25 it is even possible that FCoV antigen was missed by IHC in the examined tissue, but was detected by ICC in the lymph nodes.
Additionally, it would be conceivable that immunostaining of non-mutated FCoV within macrophages can occur. FCoV has been shown to cause monocyte-associated viremia also in healthy FECV-infected cats that never developed FIP.6,16,19,24,30 Episodes of viremia allow for the systemic spread not only of FIPV, but also of FECV. 28 In healthy FECV-infected cats, mesenteric lymph nodes are among the organs that harbor viral antigen with the highest frequency, 28 and FECV could be detected by IHC in monocytic cells in the medullary sinuses of mesenteric lymph nodes of healthy cats without FIP.28,36 Thus, the most likely explanation is that the mesenteric lymph node of the control cat that tested false-positive harbored FECV and that the positive immunostaining resulted from the detection of FECV rather than FIPV.
Sensitivity of the ICC in lymph node FNA was 53.3%. Considerably lower sensitivities of 31% and 11% have been reported previously for ICC of liver and kidney FNA smears, respectively, but, in that study, only 16 and 19 cats were investigated, respectively. 12 The difference in sensitivity can possibly be explained by the different virus loads present in various tissues. Mesenteric lymph nodes have been identified as harboring high levels of FIPV genomic RNA (gRNA) in cats with experimentally induced FIP, whereas low-to-negative levels of FIPV gRNA were found in the kidneys and variable levels in the liver. 37
In any case, sensitivity was lower than expected using mesenteric lymph node FNA in our study. As has been demonstrated, virus load is low if an organ is not grossly or histologically involved in the disease process. 37 We obtained FNAs of the mesenteric lymph nodes of all cats, regardless of whether the nodes were enlarged. It is possible that the mesenteric lymph nodes were not involved in the disease process in some of these cats with FIP and therefore did not contain large amounts of FCoV antigen, which might have lowered sensitivity. Furthermore, at acquisition of the FNA specimens in our study, the needle was inserted into the mesenteric lymph nodes independently of the presence of macroscopic lesions. Viral antigen is known to be variably distributed within FIP lesions. 25 Thus, it is possible that FCoV-containing macrophages were missed. This could explain the low sensitivity of the ICC in FNA samples and also the fact that the majority (10 of 16; 63%) of ICC-positive samples from cats with FIP only showed a low yield of ICC-positive macrophages.
We used a monoclonal anti-FCoV antibody in our staining protocol. Possibly, this influenced sensitivity, and the use of a polyclonal antibody conjugate could lead to better test performance. However, given that a polyclonal antibody conjugate was even less sensitive in immunofluorescence tests of effusions in previous studies,3,17 this seems rather unlikely.
To enable ICC on pooled samples, all FNA samples of mesenteric lymph nodes were obtained postmortem in our study, and slides were stored at −20°C immediately after postmortem sampling until immunostaining. This might have decreased the amount of intact viral antigen present within the samples and therefore could have contributed to the low sensitivity.
Given that cytologic staining in a pilot study proved to impact negatively on immunodetection of the FCoV nucleocapsid, we used unstained specimens for ICC. Likewise, clinicians should be advised to submit duplicate unstained slides for ICC when performing cytologic examinations.
There were 2 limitations to our study. First, FNA samples were obtained postmortem from all cats. Therefore, it is possible that sensitivity was falsely reduced because of degradation of cells and virus. Further studies evaluating ICC of mesenteric lymph node FNA samples obtained antemortem should be performed. Second, internal true-negative controls, such as normal feline liver or kidney from a cat that was not an included case, were not included in the staining protocol. A negative control could have helped in establishing the cutoff for positive immunostaining when defining the staining threshold. We defined samples as ICC-positive if at least 1 macrophage fulfilled the aforementioned criteria for true-positive staining. Potentially, low-yield positive staining of single macrophages could be a normal finding in non-FIP cats.
Additionally, for statistical and analytical purposes, it would be helpful to include more FIP cases without effusion in future studies.
Footnotes
Acknowledgements
We thank Karin Stingl, Institute of Veterinary Pathology, for her excellent technical support while performing the IHC and ICC.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.