
Abstract
Feline infectious peritonitis (FIP) is one of the most important viral diseases of cats worldwide. Our study describes the neuropathology and the diagnostic features of 26 cases of FIP in domestic cats. The average age of affected individuals was 11.8 mo, and there was no sex or breed predisposition. Clinical neurologic signs were noted in 22 cases, and rabies was clinically suspected in 11 cases. Twenty cats had lesions in multiple organs, and 6 cats had lesions only in the brain. Gross neuropathologic changes occurred in 15 cases and consisted of hydrocephalus (10 cases), cerebellar herniation through the foramen magnum (6 cases), cerebral swelling with flattening of gyri (2 cases), and accumulation of fibrin within ventricles (2 cases) or leptomeninges (1 case). Histologically, 3 main distinct distributions of neuropathologic changes were observed, namely periventricular encephalitis (12 cases), rhombencephalitis (8 cases), and diffuse leptomeningitis with superficial encephalitis (6 cases). Fresh tissue samples were submitted for fluorescent antibody testing (FAT) after autopsy in 17 cases, and positive results were found in only 7 cases. Immunohistochemistry (IHC) for feline coronavirus confirmed the diagnosis in all 26 cases. IHC appears to be a more sensitive and reliable test for confirmation of FIP than is FAT.
Introduction
Feline infectious peritonitis (FIP) is one of the most important viral diseases of wild and domestic cats worldwide.10,12,14,22,25 It is caused by the mutant FIP virus (FIPV), which originated from feline enteric coronavirus (FECV), a widespread agent associated with subclinical or transient gastrointestinal disease in young cats.14,32 Given their close genetic relationship, the viral strains are serologically indistinguishable and difficult to differentiate by routine laboratory testing, making an accurate clinical diagnosis of FIP often difficult.9,13,14,32 Despite decades of research since the first description of the disease in the mid-1960s, FIP remains one of the most prevalent and fatal infectious diseases of cats.14,21,24,25 FIPV infection can lead to a wide variety of clinical signs and pathologic changes that can be characterized by localized or disseminated fibrinous and/or pyogranulomatous inflammation in many organs, including the central nervous system (CNS). 14 Lesions in the CNS are typically surface-oriented and mainly target the leptomeninges, ependyma or ventricles, choroid plexus, and to a lesser extent, neuroparenchyma.14,20,28 Although a few reports have briefly described lesions in the CNS of cats with FIP, a comprehensive study systematically evaluating the wide spectrum of these neuropathologic changes is lacking.5,6,11,15,16,20,26,28 We describe 3 distinct types of neuropathologic changes in the brain of 26 cases of FIP diagnosed over a 10-y period. In addition, given the difficulties inherent in the diagnosis of this disease, we also compare 2 laboratory tests used in addition to histopathology for the postmortem diagnosis of FIP.
Material and methods
The University of Georgia Department of Pathology and Athens Veterinary Diagnostic Laboratory (AVDL) record system was searched for cases of FIP between 2005 and 2015. Retrieved cases were reviewed, and those with reported changes in the brain underwent further evaluation. Cases that had tissue sections of telencephalon with basal nuclei, thalamus, brainstem, and cerebellum available were included in the study. Spinal cord was not available in these cases. All information was collected from the submission forms and autopsy reports, and archived histology slides were reexamined. Neuropathologic changes were characterized according to: 1) type (lymphoplasmacytic, neutrophilic, histiocytic, granulomatous, or mixed) and location (leptomeningeal vessels, parenchymal vessels, choroid plexus, ventricles, and gray and white matter) of inflammation; 2) presence or absence of vasculitis; and 3) presence or absence of secondary changes, such as hemorrhage, erythrophagocytosis, status spongiosus, astrocytosis, microgliosis, neuronal necrosis, neuronophagia, and neuroparenchymal necrosis (cavitary areas with foamy macrophages). Cases were grouped into 3 categories according to the overall distribution of neuropathologic changes: 1) diffuse leptomeningitis with superficial encephalitis, characterized by inflammatory infiltrates that were more prominent in the leptomeninges and superficial cerebral or cerebellar cortex; 2) periventricular encephalitis, characterized by inflammatory infiltrates that were more prominent around the ventricular system; and 3) rhombencephalitis, characterized by inflammatory infiltrates that were more prominent in the brainstem and cerebellum. Representative sections of archived paraffin-embedded brain tissue from all cases were submitted to immunohistochemistry (IHC) for feline infectious peritonitis virus (mouse monoclonal antibody, 1:600 dilution at 60 min, Custom Monoclonals International, West Sacramento, CA).
Results
Twenty-six cases met the criteria for inclusion in our study (Table 1). Neurologic clinical signs were reported as the main problem in 22 of 26 cases (85%), and rabies was clinically suspected in 11 cases (42%). The main neurologic signs included ataxia (8 cases, 31%), depression (7 cases, 27%), seizures (5 cases, 19%), head tilt (3 cases, 12%), urinary incontinence, incoordination, opisthotonus, muscle rigidity, recumbency (2 of 26 each, 8%), nystagmus, aggressiveness, anisocoria, and miosis (1 of 26 each, 4%).
Signalment, clinical signs, and gross neuropathologic changes in 26 cases of feline infectious peritonitis with neurologic involvement.
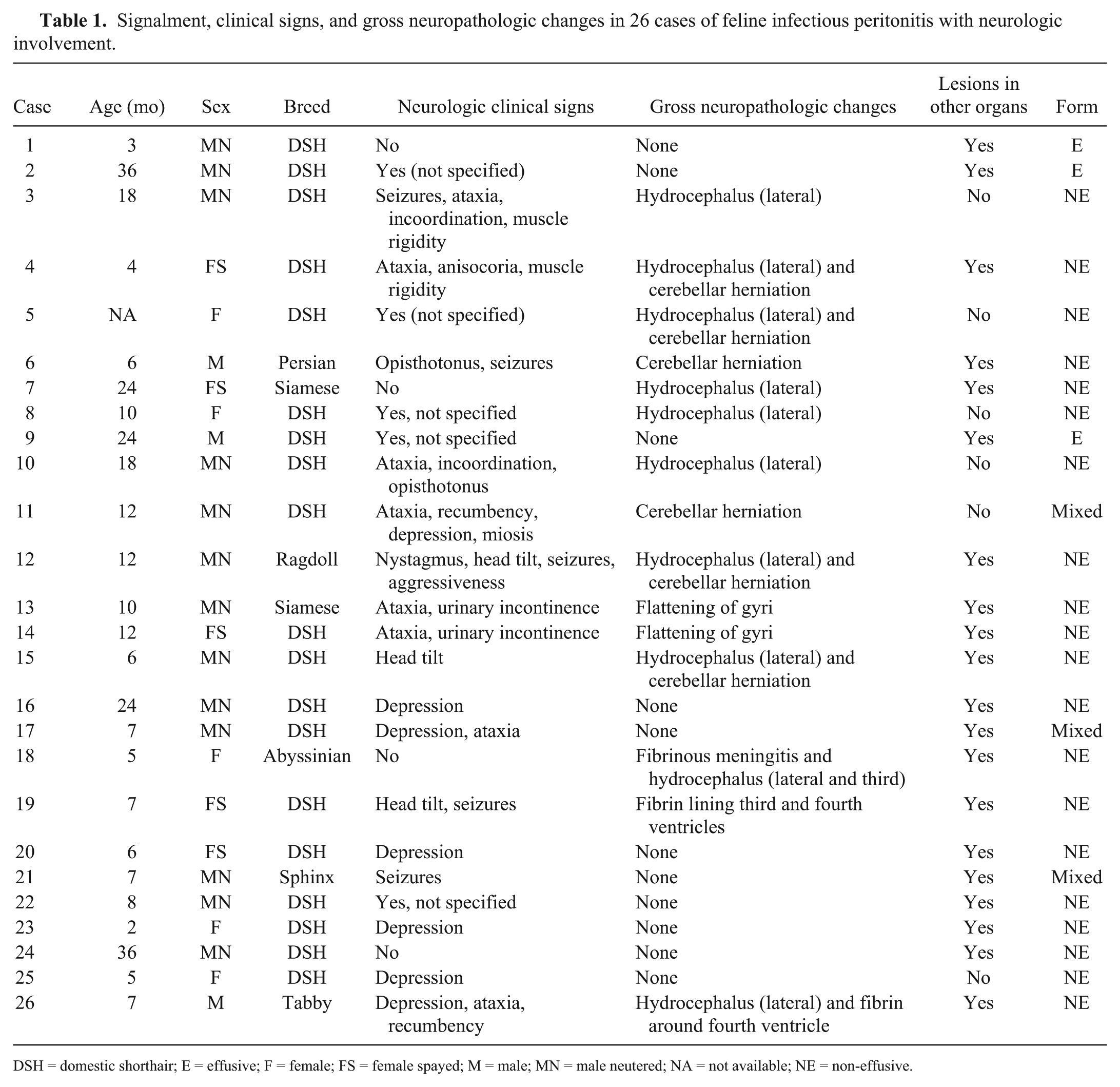
DSH = domestic shorthair; E = effusive; F = female; FS = female spayed; M = male; MN = male neutered; NA = not available; NE = non-effusive.
Gross neuropathologic changes (Fig. 1) in the brain occurred in 15 cases (58%) and consisted of hydrocephalus (10 cases, 38%), cerebellar herniation through the foramen magnum (6 cases, 23%), cerebral swelling with flattening of gyri (2 cases, 8%), and accumulation of fibrin within the ventricles (2 cases, 8%) or leptomeninges (1 case, 4%).
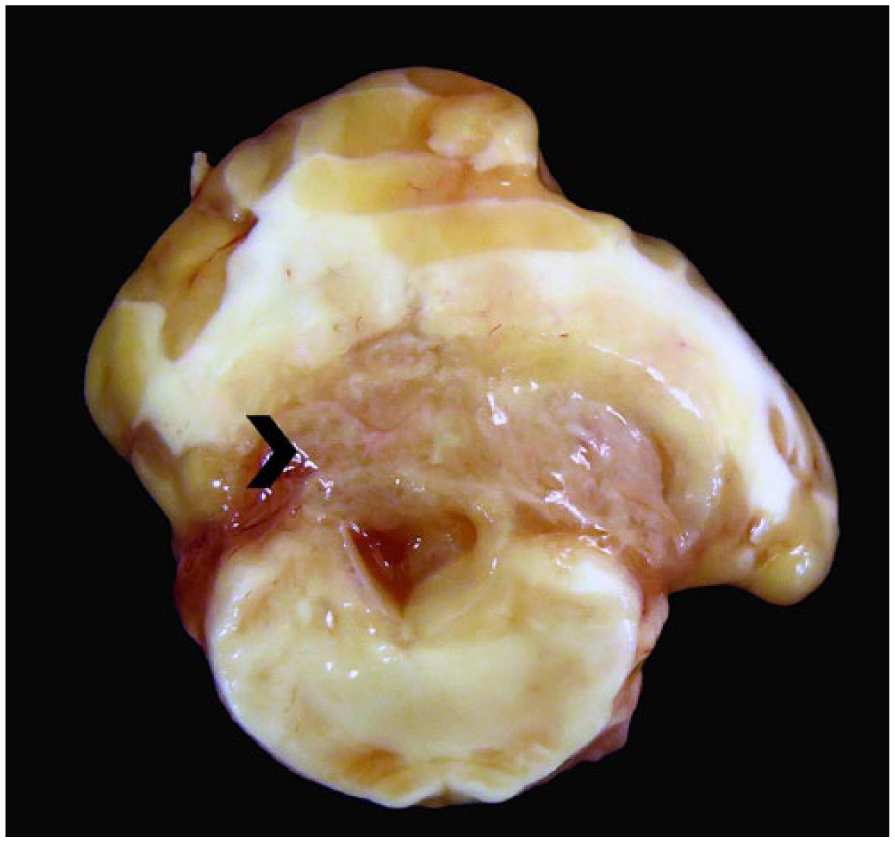
Feline infectious peritonitis in cat 26. Yellow, gelatinous strands of fibrin (arrowhead) expand the periventricular area around the fourth ventricle and compress the overlying cerebellar white matter.
Histologically, the most common distribution of pathologic changes in the brain (Fig. 2) was periventricular encephalitis (12 cases, 46%), followed by rhombencephalitis (8 cases, 31%), and diffuse leptomeningitis with superficial encephalitis (6 cases, 23%). Neurohistopathologic changes were similar regardless of the distribution of the lesions in the brain (Table 2) and were characterized by perivascular accumulations of lymphocytes and plasma cells that were admixed with a variable number of foamy or epithelioid macrophages and neutrophils. The perivascular inflammatory infiltrate was more prominent in the leptomeninges, but also occurred in the superficial cortex, periventricular parenchyma, white matter, and choroid plexus (Figs. 3–8). Vasculitis was observed in 23 cases (88%), and it was more common in leptomeningeal venules and arterioles (Figs. 9–11), but was also present in the affected neuroparenchyma. Affected vessels typically had mural inflammatory infiltration and had often undergone fibrinoid change. Parenchymal changes in the telencephalic gray matter and periventricular areas reflected the perivascular inflammation and consisted of scattered accumulations of inflammatory cells, astrocytosis and microgliosis, and occasional neuronal necrosis and neuronophagia (Fig. 12). Changes in the white matter were less frequent and consisted of status spongiosus and the presence of axonal spheroids. Overall, lesions were more prominent in cases of rhombencephalitis and occurred predominantly over the basal aspect of the brainstem. These cases also tended to have a more severe degree of fibrin exudation and vasculitis when compared to cases with superficial or periventricular inflammation.
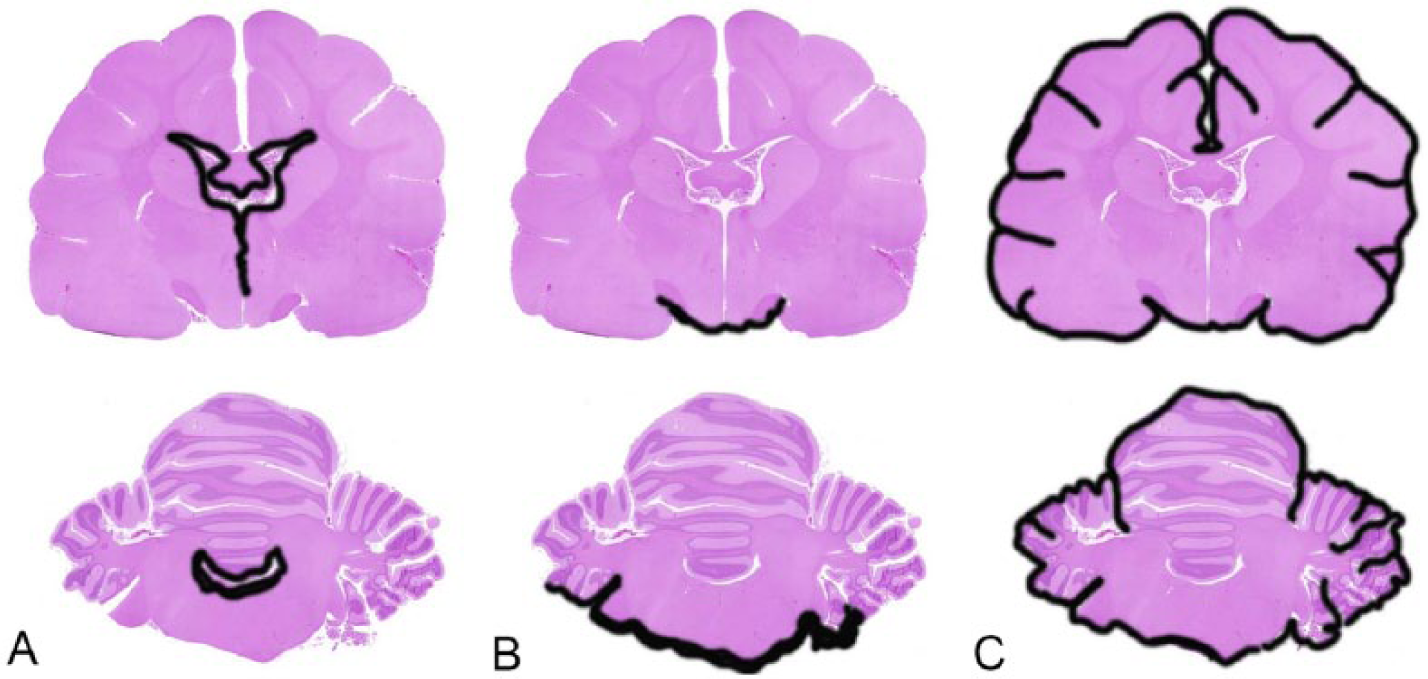
Overall distribution of the neuropathologic changes in 26 cases of feline infectious peritonitis in cats. The most common pattern was
Neurohistopathology, distribution of lesions, and diagnostic confirmation in 26 cases of feline infectious peritonitis with neurologic involvement.
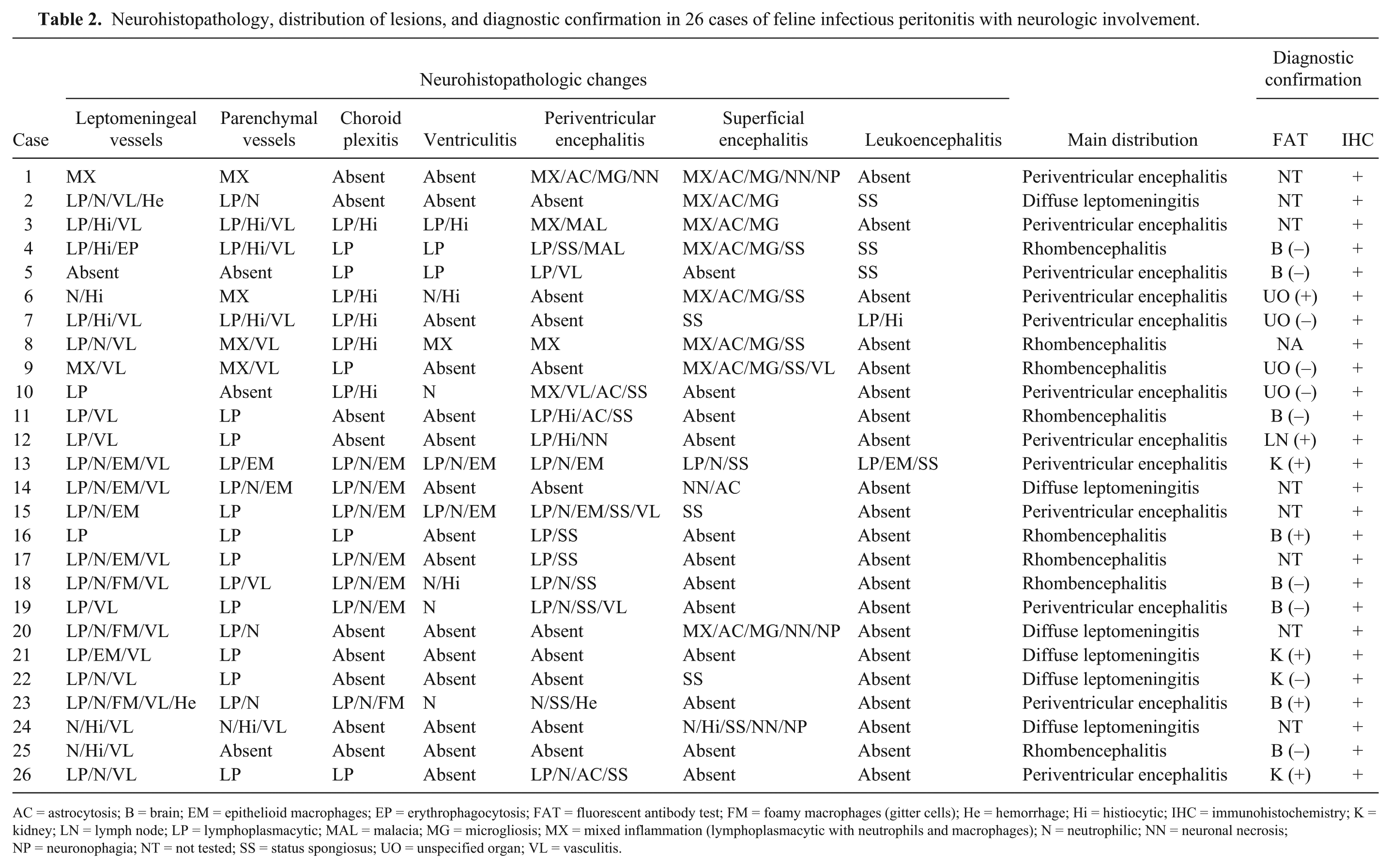
AC = astrocytosis; B = brain; EM = epithelioid macrophages; EP = erythrophagocytosis; FAT = fluorescent antibody test; FM = foamy macrophages (gitter cells); He = hemorrhage; Hi = histiocytic; IHC = immunohistochemistry; K = kidney; LN = lymph node; LP = lymphoplasmacytic; MAL = malacia; MG = microgliosis; MX = mixed inflammation (lymphoplasmacytic with neutrophils and macrophages); N = neutrophilic; NN = neuronal necrosis; NP = neuronophagia; NT = not tested; SS = status spongiosus; UO = unspecified organ; VL = vasculitis.
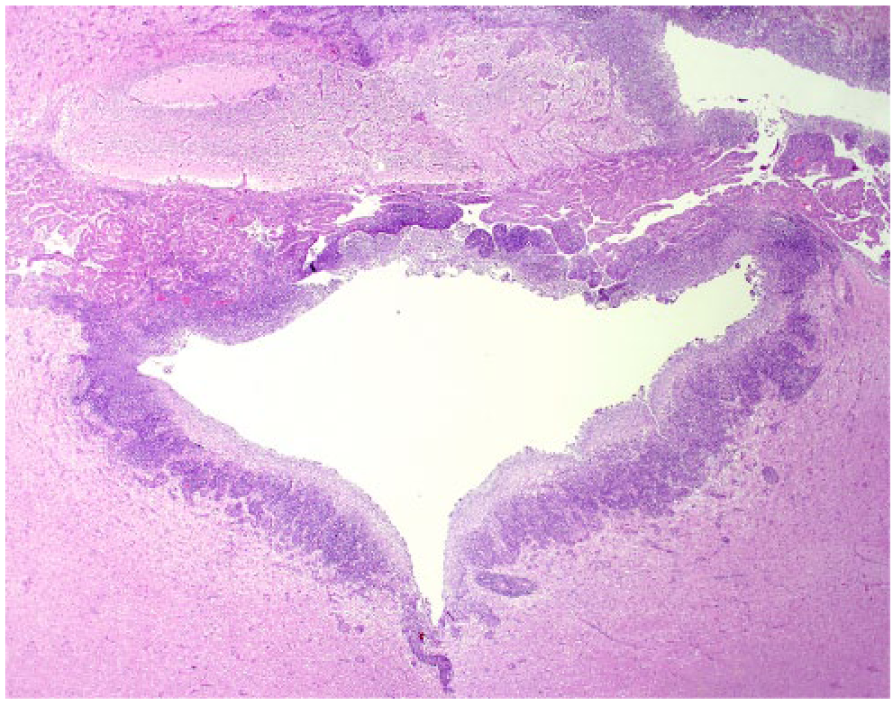
Marked fourth ventricle choroid plexitis and periventricular encephalitis in cat 19. The dense inflammatory infiltrate extends to the perivascular spaces. H&E.
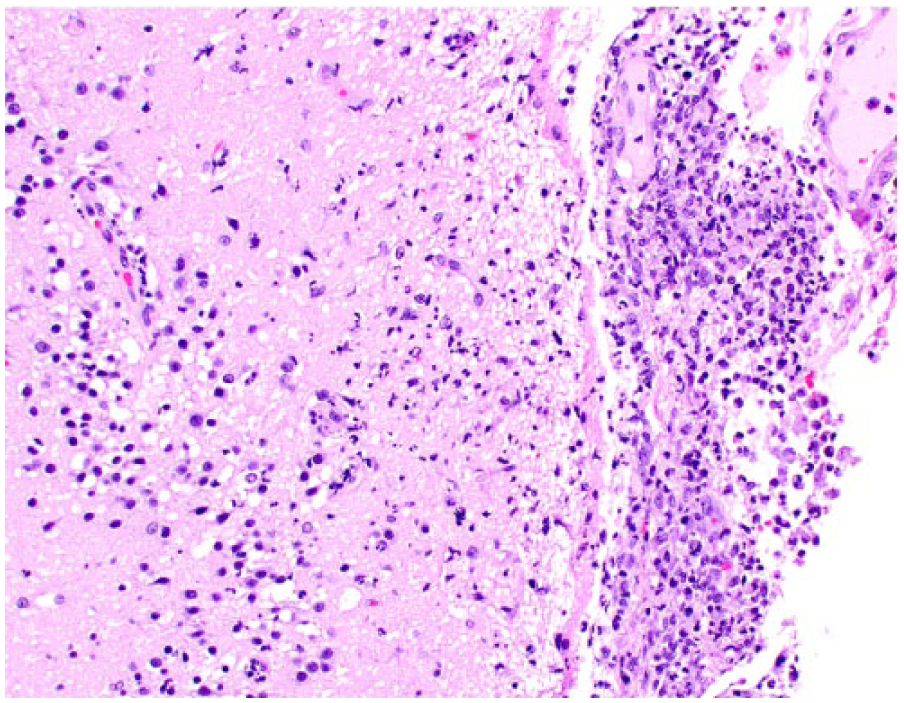
Periventricular encephalitis in a lateral ventricle of cat 18. Layers of neutrophils and macrophages accumulate within the ventricle (right) and extend through the ependyma and into the vacuolated periventricular white matter and perivascular spaces. H&E.
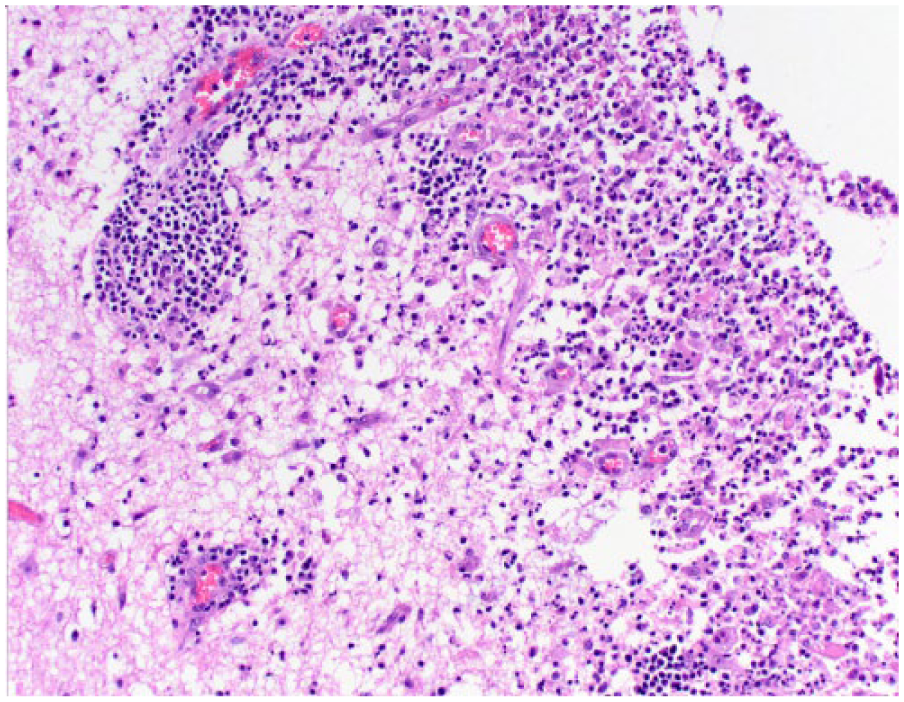
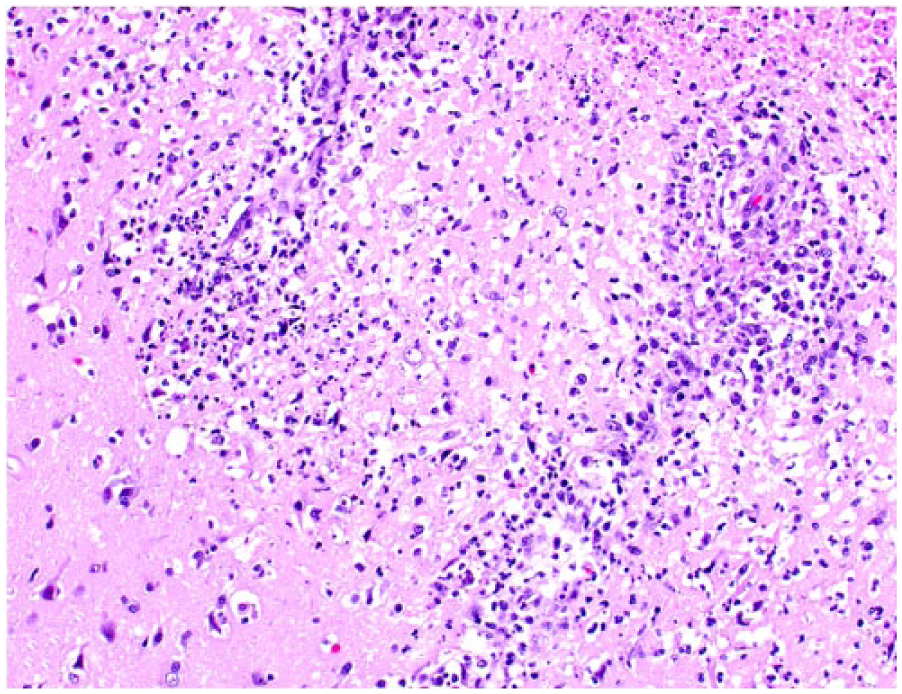
Ventral rhombencephalitis in cat 8. The leptomeninges are markedly expanded by fibrin and inflammatory infiltrate that extends into the overlying neuroparenchyma. H&E.
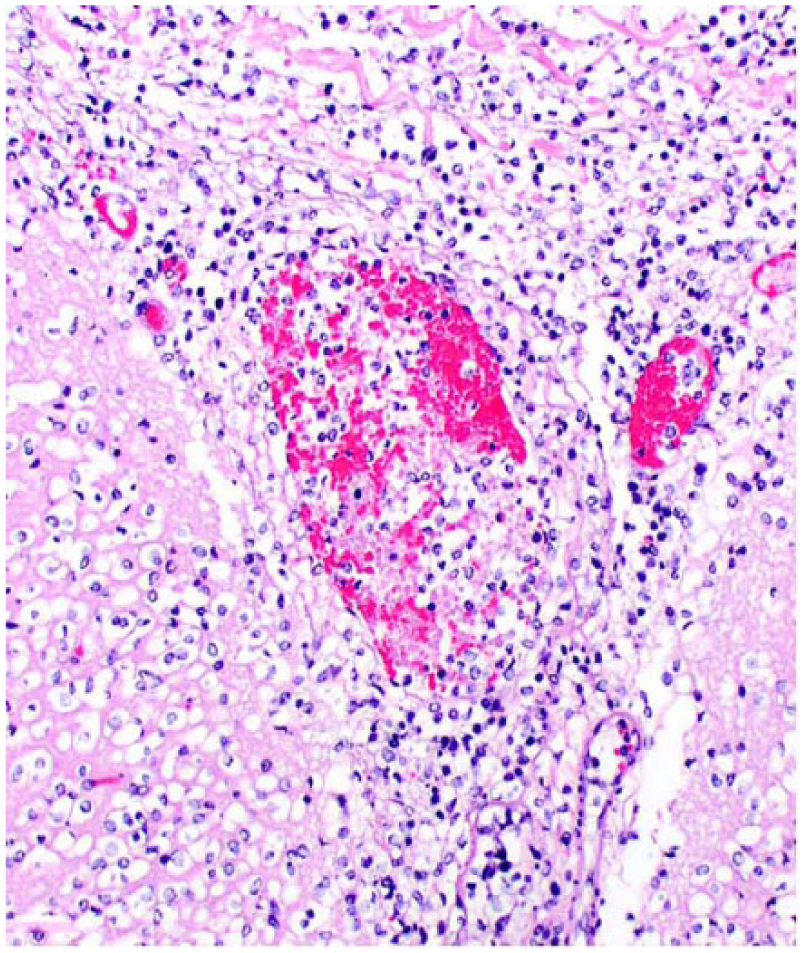
Closer view of the lesion shown in Figure 4 detailing a large amount of fibrin and inflammatory cells, mainly lymphocytes, plasma cells, and neutrophils. H&E.
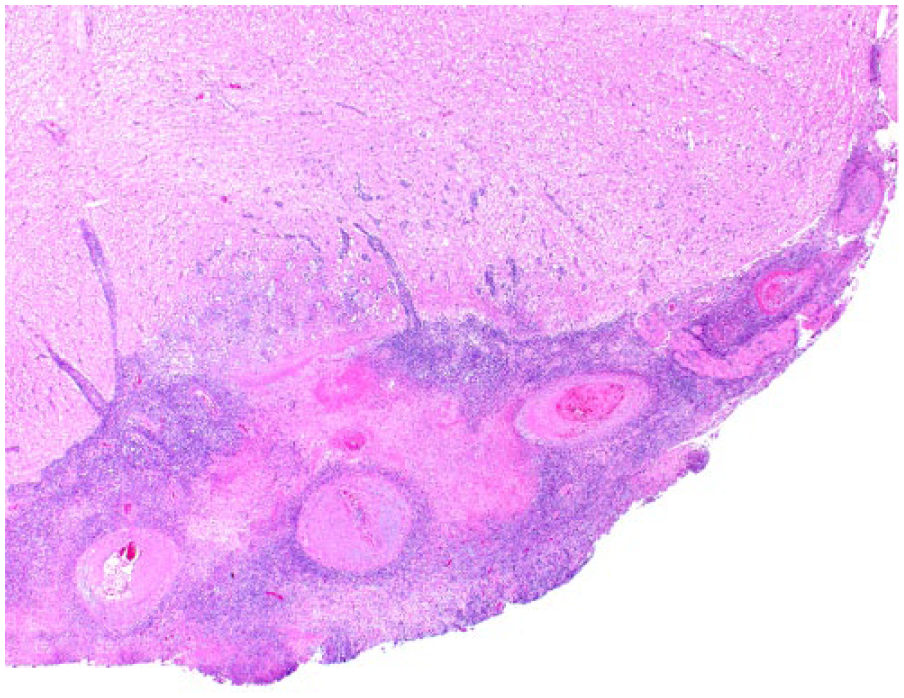
Leptomeningitis over the cerebral cortex in cat 14. The leptomeninges (right) are expanded by neutrophils and macrophages that extend to the superficial layers of the cortex (left).
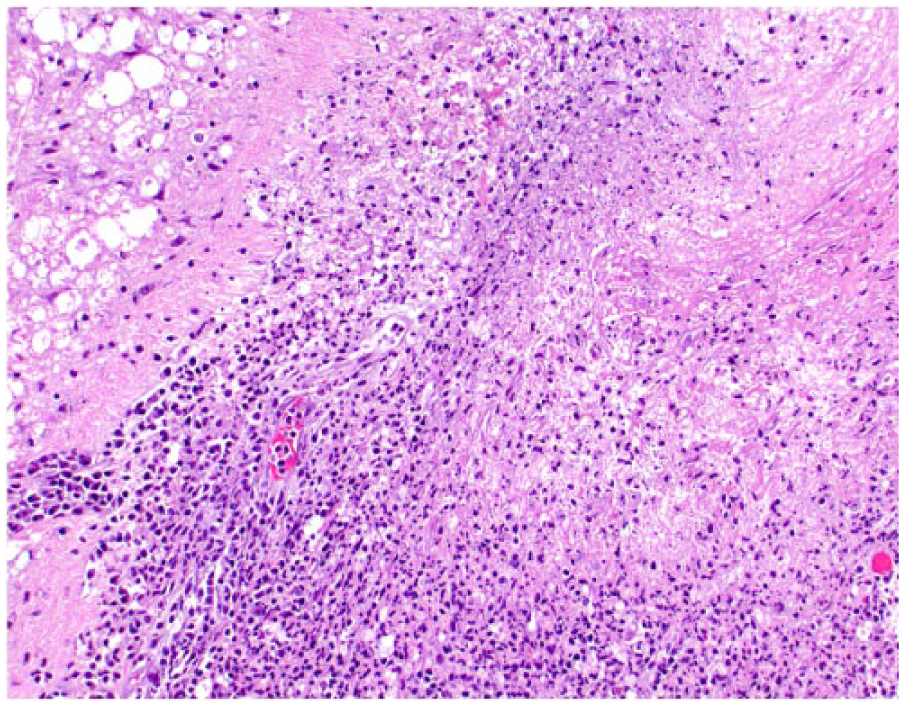
Superficial cerebrocortical encephalitis in cat 24. Vascular-centered areas of inflammation spill over the adjacent spongiotic brain tissue. H&E.
Leptomeningitis and superficial encephalitis in cat 24. The wall of the leptomeningeal venule is expanded and dissected by a mixed inflammatory cell population. H&E.
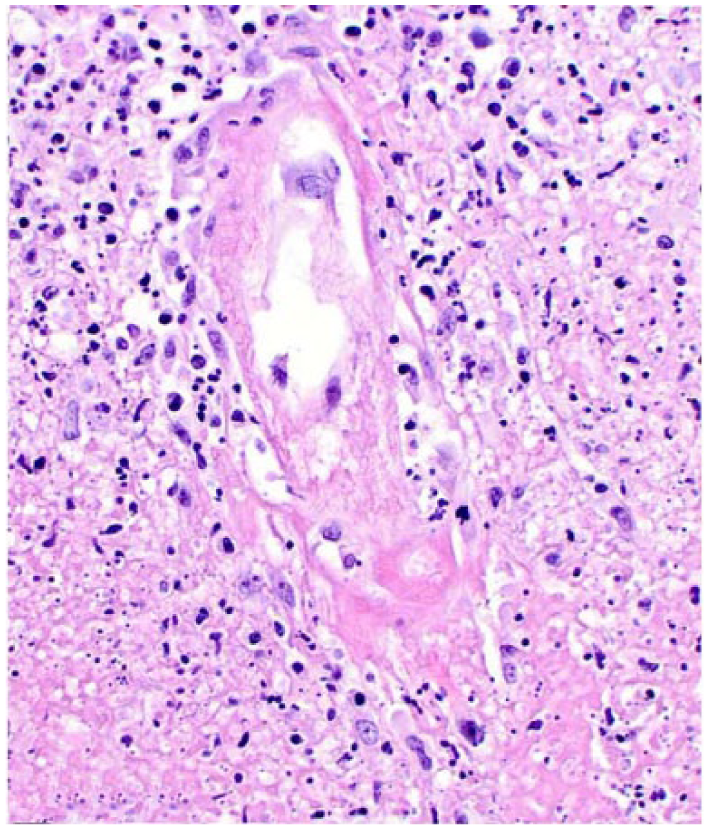
Ventral rhombencephalitis in cat 18. The venular wall is expanded by fibrinoid change and cell debris. H&E.
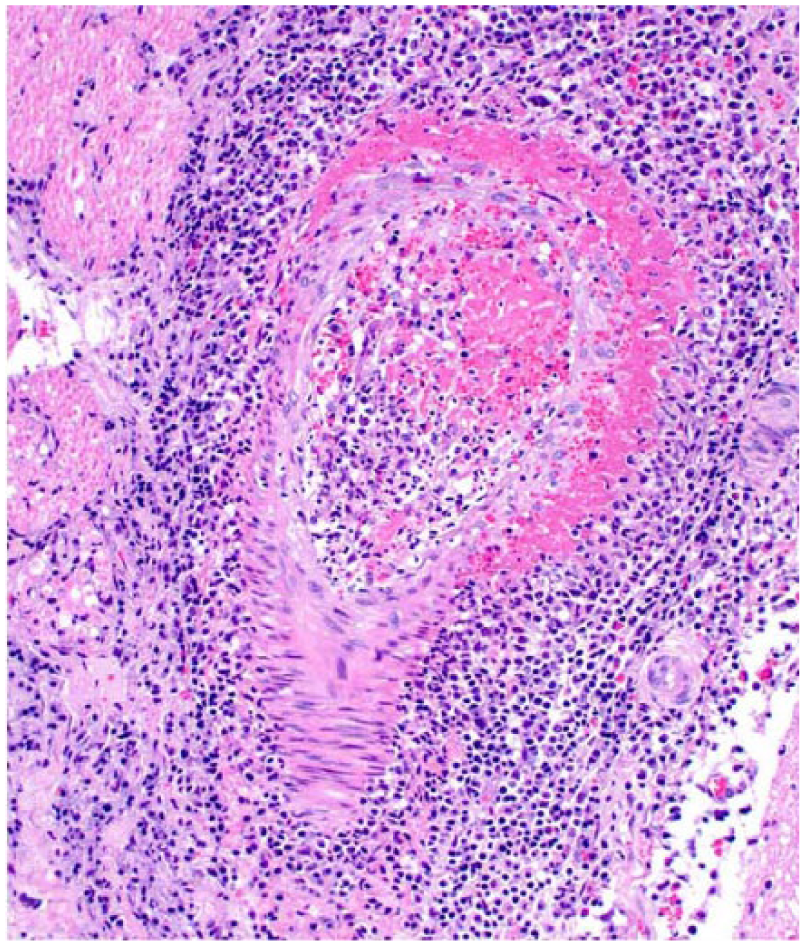
Ventral rhombencephalitis in cat 9. There is fibrinoid change of the arteriolar wall and a mixed perivascular population of inflammatory cells. H&E.
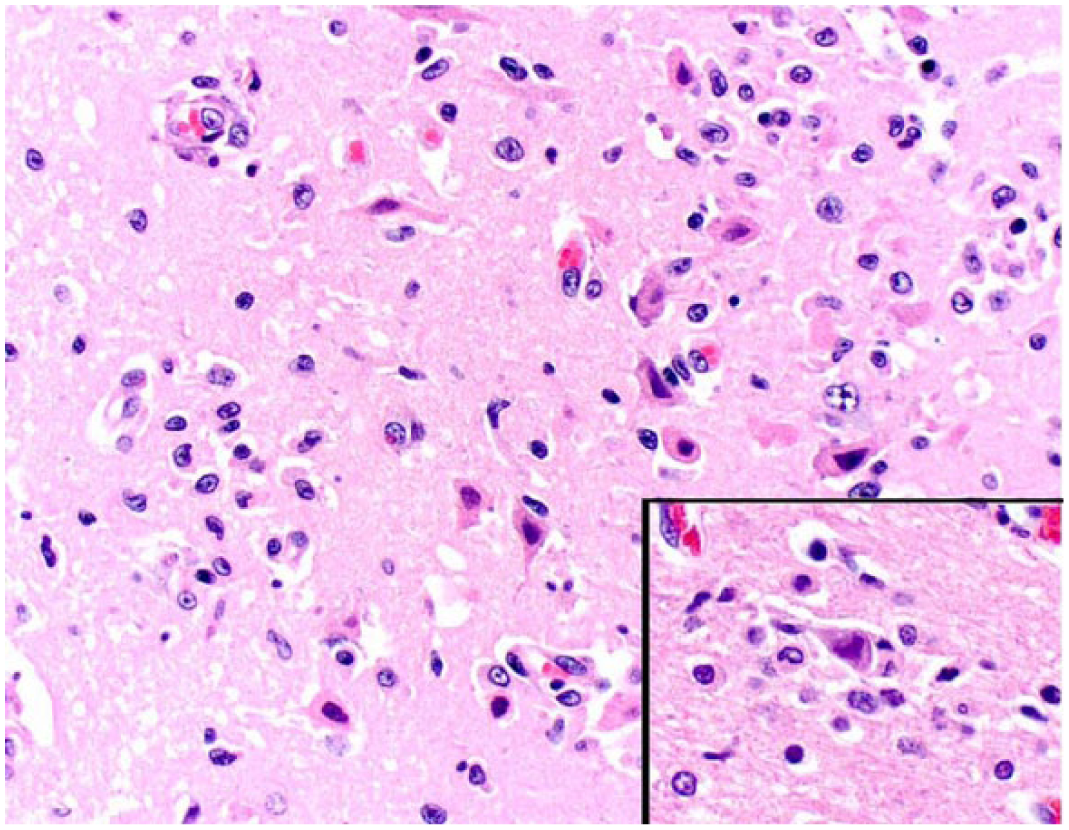
Superficial cerebrocortical encephalitis in cat 1. There is extensive neuronal necrosis with astrocytosis and areas of neuronophagia (inset). H&E.
Fresh samples of brain (8 cases), kidney (4 cases), mesenteric lymph node (1 case), and 4 other organs that were not specified in the records were submitted to fluorescent antibody testing (FAT) for FIPV after autopsy (17 cases total); diagnostic confirmation was achieved in only 7 of 17 cases (41%). The 10 cases negative for FIPV by FAT and 8 cases that were not submitted to FAT were presumptively diagnosed as FIP based on the histologic changes. One case (case 2) was diagnosed as a possible bacterial infection based on histopathology. IHC revealed strong, granular, or less often homogeneous, immunostaining in the cytoplasm of macrophages throughout the affected areas in all cases (Fig. 13).
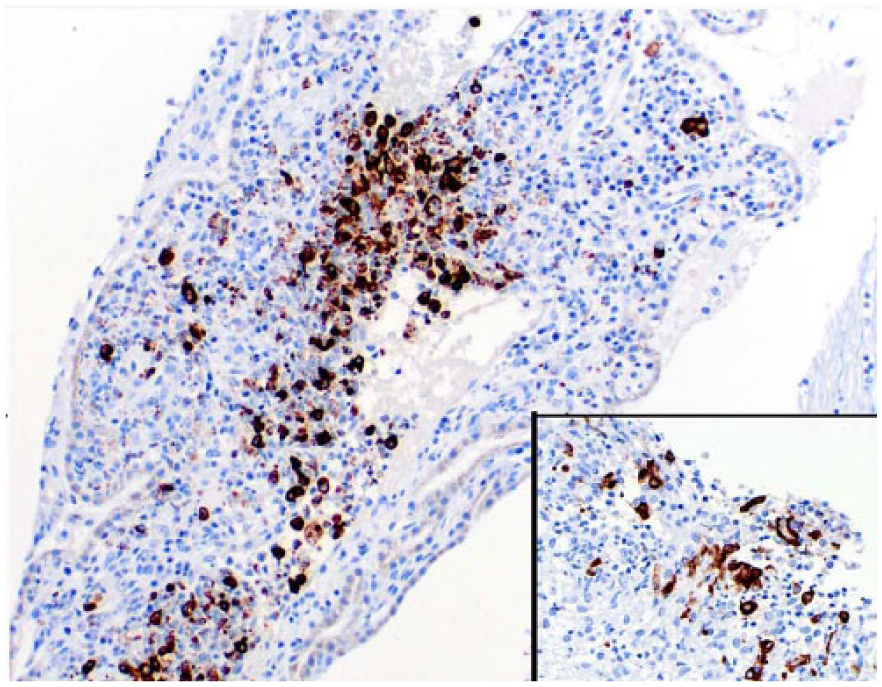
Leptomeningitis in cat 14. Perivascular macrophages exhibit strong immunostaining for feline coronavirus antibody. Inset: Positive immunostaining in periependymal macrophages.
Discussion
The age of FIP-affected cats varied from 2 to 36 mo (mean 12.3 mo), and no sex or breed predisposition was noted. These findings are in accord with previous reports of FIP. 8 Although most individuals in our study were domestic shorthair (DSH) cats, this predominance is noted in most retrospective studies conducted in our laboratory and reflects the wide distribution of this breed in our feline population rather than a true breed predisposition. A search in the AVDL web-based record system revealed that 2,001 cats were submitted for autopsy between 2005 and 2015 and that 1,394 (70%) were DSH cats. Neurologic signs were variable and reported in almost 85% of our cases, similar to previous reports.6,12,27 Although specific clinical signs could have reflected the neurolocalization of lesions in the brain, 27 a full neurologic examination was not conducted in most patients in our study, making it difficult to differentiate truly neurologic signs from other clinical signs that may have been attributed to lesions in other organs or to systemic disease.
Meningoencephalitis and/or meningomyelitis caused by FIPV infection may occur exclusively as a neurologic disease or as part of systemic FIP.6–8,17,18,20,28,30 Neurologic disease has been reported to be more frequent in cases of non-effusive FIP, in which approximately one-third of cats develop neurologic disease either primarily or as part of systemic FIP.6,15,27 Twenty of 26 cats in our study also had lesions of FIP in other organs, and 15 of these 20 cases were diagnosed as non-effusive FIP.
Primary or secondary gross changes in the brain are variable among cases of effusive or non-effusive FIP.6,17,18,28,30 Gross neuropathologic changes were observed in ~58% of our cases and included mainly secondary lesions related to edema. The most common of such changes was hydrocephalus (10 cases). The fact that 7 of these 10 cases were classified in the periventricular encephalitis group suggests that inflammation within or around the ventricular system has a major role in the development of ventricular obstruction and secondary hydrocephalus in cases of FIP. 31 Other changes such as roughened ependyma with reactive syncytial cells have also been described in cases of FIP, 31 but were not detected in our cases. Primary inflammatory changes were reported in only 3 cases (12%) and consisted of accumulation of yellow strands of fibrin on the leptomeninges or in the ventricular system, similar to other reports.6,17,18,28,30 A few reports have briefly characterized the overall neurohistopathologic changes caused by FIPV infection, but no studies have been conducted that fully and thoroughly describe these lesions in the brains of affected cats, to our knowledge.3,5,6,11,15–20,27,28,30 Meningoencephalitis caused by FIPV has been classically described as a surface-oriented reaction centered mainly on the leptomeninges, ependyma, and choroid plexus, and less often neuroparenchyma in the brain and spinal cord.5–8,11,17,18,20,28,30 Although changes may be more prominent in certain areas of the brain, such as the ventral aspect of the brainstem and cerebellum, 6 no detailed characterization of these lesions in other areas of the brain has been reported to date, to our knowledge. In our study, histologic examination of multiple sections of brain revealed that cats with systemic and neurologic (20 cases) or strictly neurologic (6 cases) FIP can develop a wide spectrum of histopathologic changes, including lesions that may resemble bacterial infection. Unfortunately, spinal cord was not available from our cases of FIP.
Although the overall nature of the neuropathologic changes was similar among our cases, the distribution of these changes varied considerably, regardless of the type of inflammation and the presence or absence of lesions in other organs. Three distinct distributions of neurohistopathologic changes were observed, namely periventricular encephalitis, rhombencephalitis, and diffuse leptomeningitis with superficial encephalitis. The reason for these 3 variations remains elusive and may warrant further investigations of the mode of entry, pathogenesis, and cell types involved in the inflammatory infiltrates in the CNS of cats affected by FIP. An interesting finding in our study was the occurrence of different morphologic variations in the macrophage population within the lesions, which were not only composed of epithelioid macrophages, but also non-epithelioid macrophages and foamy macrophages (gitter cells). In addition, lesions in case 2 were mainly neutrophilic, which led to a presumptive diagnosis of a bacterial infection. These features suggest that histologic changes in the brain of cats affected by FIP are variable and do not always reflect the typical pyogranulomatous pattern so commonly attributed to this viral infection.
A definitive clinical diagnosis of FIP is challenging and should rely on the history and clinical pathology data, such as complete blood count, serum biochemistry profile, and effusion or cerebrospinal fluid (CSF) analysis, in combination with direct or indirect viral detection.1,2,9,13,14 Important clinical pathology abnormalities, including anemia, neutrophilic leukocytosis, lymphopenia, and hyperproteinemia with inverted albumin-to-globulin ratio are important changes observed in affected cats and would have been supportive of a presumptive diagnosis during evaluation of these cats, especially in the 11 cases in which rabies was suspected clinically.1,9,14,23,29 In addition, effusion and CSF analysis often reveals high protein content and may provide further evidence for a clinical diagnosis of FIP.1,9 Antibody detection in blood, effusion, and CSF, or direct viral detection by FAT of effusion samples have been widely used to support a clinical diagnosis of FIP, but laboratory tests have been shown to be unreliable given the frequent false-negative results.2,9,14 Reverse-transcription PCR is a sensitive method that can be useful for diagnostic support in cases of FIP, especially in cats that have tested negative using other procedures. However, inconsistent results are frequent when using fecal, blood, effusion, CSF, or tissue samples. In addition, PCR alone cannot differentiate between FIPV and FECV.10,14 Genomic sequencing can discriminate between the viral strains and has offered encouraging results when compared to other tests.4,14
The postmortem diagnosis of FIP is based on the clinical history combined with the pathologic changes, and confirmation is attained via FAT or IHC on fresh and formalin-fixed samples, respectively. 9 However, as observed in our cases, only 7 of 17 (41%) submitted samples were positive when fresh tissues were submitted for FAT following autopsy. In contrast, viral antigen was detected in all cases using IHC, including those cases that were negative by FAT. Therefore, as shown by the results of our study and by other investigations, FAT can be useful as a quick test during or immediately after autopsy, but IHC is a much more reliable test for diagnostic confirmation, especially in cases in which neurologic involvement was confirmed, given that the viral load in brain samples of cats affected by FIP has been shown to be lower compared to other extra-CNS tissues.6,8,9 Therefore, IHC appears to be a highly sensitive and reliable test for confirmation of FIP compared to FAT.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.