
Abstract
Flow cytometry (FC) is widely applied to characterize and stage nodal lymphomas in dogs because it has a short turnaround time, requires minimally invasive sampling, and allows contemporary evaluation of neoplastic cells in the primary lesion and of blood and marrow involvement. We investigated advantages and limitations of FC in suspected extranodal lymphomas in dogs. The likelihood of obtaining a suitable FC sample was significantly lower for aspirates of extranodal lesions than for lymph node aspirates. However, we noted no differences among different extranodal lesion sites. We also describe FC results for 39 samples compatible with extranodal lymphoma. A dominant population of large cells was easily identified on morphologic FC scattergrams in many cases. Phenotypic aberrancies were frequently present, mainly in T-cell lymphomas. Lymphoma cells were distinguishable from normal residual lymphocytes in >85% of cases, facilitating the quantification of putative blood and marrow involvement by FC. Despite the high percentage of non-diagnostic samples (32 of 73, >40%), we support the inclusion of FC in the diagnostic workup of suspected extranodal lymphomas in dogs, in conjunction with histopathology. Histopathology is the gold standard for diagnosing lymphoma, provides relevant information, including tissue invasion and epitheliotropism, but has a longer turnaround time.
Introduction
Diagnostic flow cytometry (FC) was introduced in veterinary medicine at the end of the 20th century 35 ; the primary use of FC is in characterizing canine hematopoietic neoplasms.6,27 FC provides useful information in dogs with lymphoma, including phenotype of neoplastic cells, 12 lymphoma subtype, 36 expression of specific markers,25,26 stage,20,21,28,29 and presence of minimal residual disease. 1
Most FC studies in dogs have focused on nodal lymphoma; only a few reports have characterized primary extranodal lymphomas.9,11,15,31 Conversely, in human medicine, FC is routinely included in the diagnostic workup of extranodal lymphomas.3,19,32,34,37,38 In addition, FC is a safe and minimally invasive technique to confirm the diagnosis of lymphoma in cats, a species with a high prevalence of extranodal forms.14,23
Given these premises, the aim of our retrospective study was to describe FC results in a case series of suspected canine extranodal lymphomas. We initially questioned whether the likelihood of obtaining a diagnostic sample varied between nodal and extranodal forms, and among different extranodal sites. Then, we describe the FC features of a series of cases compatible with extranodal lymphomas, including detailed phenotype and putative tumor burden in blood and bone marrow quantified by FC. For this second aim, we added cases obtained from a second FC database in order to consolidate the dataset.
Materials and methods
Case selection
To assess the likelihood of obtaining diagnostic samples, the FC database of the Department of Veterinary Medicine, University of Milan (Milan, Italy) was examined retrospectively from January 2009 to September 2017, and canine cases were extracted. Cases were included if FC immunophenotyping was requested for a fine-needle aspirate obtained from lesions suspected to be lymphoma at extranodal sites, excluding effusions and lymphoid organs (thymus, spleen, and tonsils). Cases were subsequently excluded if generalized lymphadenopathy was identified or if the nodal status was not reported. For each case, lesion site and FC results were retrieved.
FC results were considered consistent with lymphoma if cases fulfilled the following criteria: 1) cytologic evaluation performed prior to FC was compatible or suggestive of round-cell neoplasia, likely of lymphoid origin; 2) well-preserved FC sample, with minimal debris and disrupted cells and minimal hemocontamination; and 3) presence of a dominant lymphoid population sharing a unique morphologic and phenotypic pattern. 5 Hepatic samples were diagnosed as lymphoma only if infiltrating leukemia was unambiguously ruled out. Acute leukemia was suspected if CD34+ cells were detected, whereas chronic lymphocytic leukemia (CLL) was included in the differential if neoplastic cells had a mature morphologic appearance, were small, CD34–, and CD21+, CD4+, or CD8+ on FC. One dog had a proliferation of small mature CD4+ lymphocytes in the liver and was retained in the study. CLL was excluded in this dog based on the following: slight peripheral blood (PB) lymphocytosis, mild enlargement of hepatic lymph nodes (LNs) with all other LNs within normal limits, and death from progressive disease within 15 d of the diagnosis, despite corticosteroid therapy.
Control canine cases consisted of suspected nodal lymphoma cases extracted from the same FC database, according to the following inclusion criteria: 1) generalized lymphadenopathy; 2) no extranodal lesions; and 3) LN aspirate sent to the laboratory for FC.
In a second step, to consolidate the dataset of samples with FC results compatible with extranodal lymphomas, additional cases were included from the FC database of the Veterinary Teaching Hospital, University of Turin (Grugliasco, Italy). For all cases included in this dataset, the referring veterinarians were contacted to retrieve follow-up data.
All of the dogs were privately owned and sampled for diagnostic purposes with the informed consent of the owners. Thus, specific formal approval by the authors’ Institution Committee for Animal Care was not required (protocol 1965–2017, Ethical Committee, University of Turin).
Flow cytometry
FC was performed on tissue aspirates collected in tubes containing 1 mL of a liquid medium (either RPMI-1640 or saline solution). Prior to labeling, sample cellularity was assessed with an automated hematology analyzer (XT-2000iV, Sysmex, Kobe, Japan; or ADVIA 120, Siemens Healthcare Diagnostics, Milan, Italy). Also, a visual inspection was done by the operator, in order to assess the gross quality of the sample and decide whether to perform FC labeling. 23
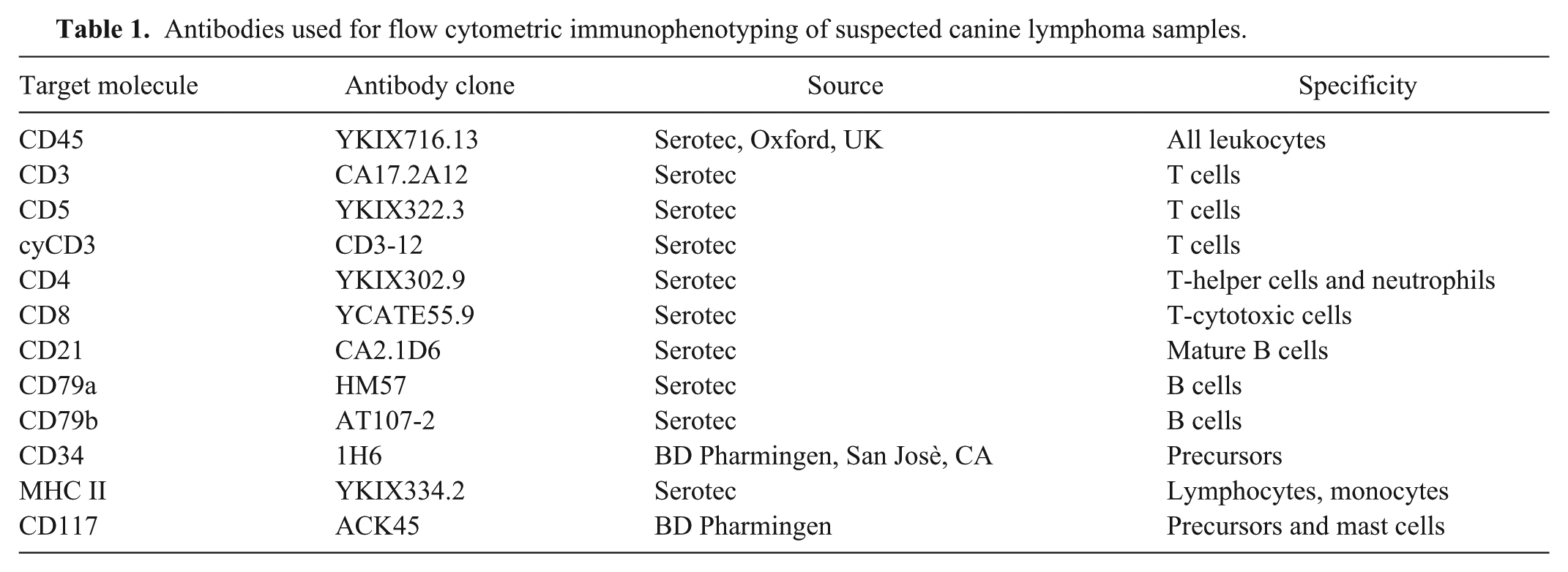
Processing for FC was performed as described previously, 12 using different combinations of antibodies (Table 1), with a multicolor approach. For intracellular staining, a permeabilization procedure was performed using either Leucoperm reagents (Serotec, Oxford, UK) following the manufacturer’s instructions, or FACS permeabilizing solution 2 (Becton Dickinson, San Josè, CA) as described. 12 Samples were acquired with a FACSCalibur or a Accuri C6 flow cytometer (Becton Dickinson) and analyzed with Cell Quest or CFlow Plus software (Becton Dickinson).
Antibodies used for flow cytometric immunophenotyping of suspected canine lymphoma samples.
Cells were classified as “small” when showing the same FC morphologic properties (forward-scatter [FSC] and side-scatter [SSC]) of residual normal lymphocytes, and as “large” when 2 distinct lymphoid populations were identifiable based on FSC and SSC (normal small lymphocytes and large neoplastic cells). Cases compatible with lymphoma were classified as B cell if cells from the dominant population expressed CD21, CD79a, or CD79b, and did not express any T-cell marker. T-cell lymphomas were identified when cells expressed CD3, CD5, CD4, CD8, or cyCD3, and did not express any B-cell marker. Cases were classified as T cell when the dominant population expressed concomitantly any T-cell marker and CD21 but not CD45. 22
When available, PB and/or bone marrow (BM) samples collected into EDTA tubes were also analyzed by FC to quantify the infiltration by putative neoplastic cells. Red blood cells were lysed prior to labeling by means of an erythrocyte lysis buffer containing 8% ammonium chloride. Putative infiltration degree was defined as the percentage of nucleated cells showing the same FC morphologic and phenotypic characteristics of the dominant population identified in the tissue aspirate.
Statistical analysis
For statistical analysis, extranodal lesions were grouped into skin, liver, head and neck, and other sites. Contingency tables were prepared, and the Pearson chi-square test was performed to assess possible different likelihoods of obtaining a sample suitable for FC assessment by comparing nodal and extranodal samples, and extranodal samples among different sites. Analyses were then performed (Statistics v.20.0, SPSS, Chicago, IL). Significance was set at p ⩽ 0.05.
Results
Diagnostic yield of nodal and extranodal samples from different sites
Seventy-three canine extranodal samples were retrieved from the FC database of the Department of Veterinary Medicine (Milan). Poor cellularity, excessive hemodilution, and high content of debris and disrupted cells were the principal limitations affecting the quality of the samples and the suitability for FC assessment. Lesions were located in the skin in 33 cases (45%), liver in 13 (18%), head and neck in 8 (11%), and elsewhere in 19 (26%), including kidney (n = 5), cerebrospinal fluid (n = 4), bowel (n = 2), lung (n = 2), and 1 each of the following: anal sac, joint, pancreas, stomach, peritoneum, and adrenal gland. Forty-one samples (56%) were considered suitable for FC assessment.
Considering only the acceptable samples, FC results were compatible with histiocytic proliferative disease in 3 cases (7%), and 1 case (2%) was suspect for infiltration by CLL because a unique population of small mature CD8+ lymphocytes was identified invading liver and bone marrow. A mixed population of small lymphocytes was present in 9 cases (22%), with large cells accounting for <5% of the population in all instances; because none of the lymphoid population was dominant, these samples were considered negative for hematopoietic neoplasia. In the remaining 28 (68%) cases, a dominant cell population was identifiable; these samples were considered consistent with extranodal lymphoma (Table 2).
Flow cytometric immunophenotype of 771 dogs with nodal or suspected extranodal lymphoma.
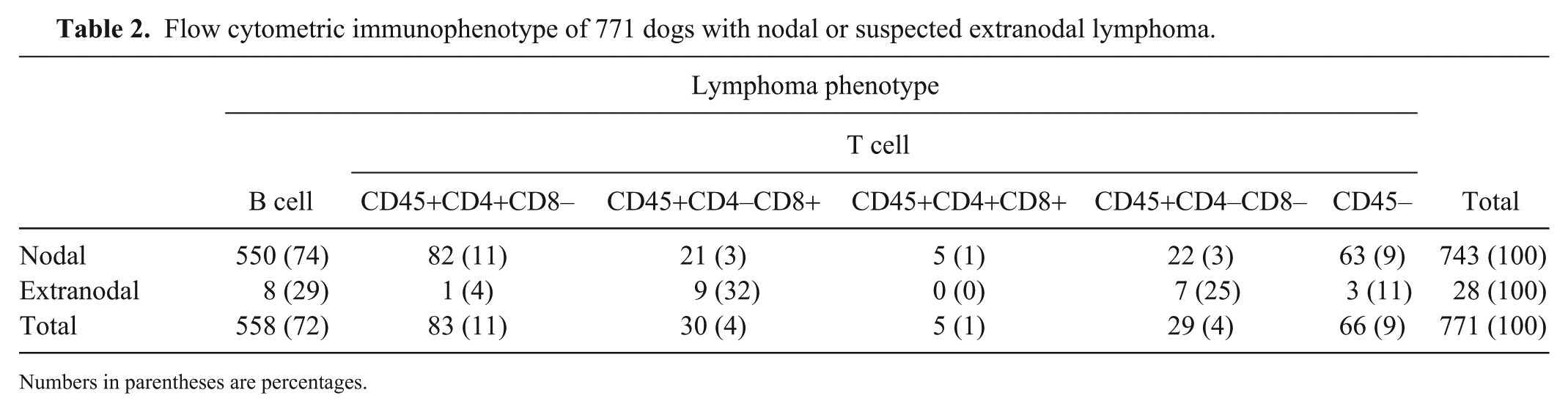
Numbers in parentheses are percentages.
The control population consisted of 894 dogs in which nodal lymphoma was suspected. A total of 820 cases (92%) were suitable for FC assessment, and 743 cases (91%) were consistent with lymphoma (Table 2).
The proportion of samples suitable for FC assessment varied significantly between extranodal and nodal samples (p < 0.001), with the latter being more likely acceptable (odds ratio: 8.64; 95% confidence interval: 5.14–14.5). The difference was not significant among different extranodal sites (p > 0.05).
FC features of extranodal lymphomas
To consolidate the dataset, 11 additional samples consistent with extranodal lymphoma obtained from the Veterinary Teaching Hospital (Turin) were included. Thus, the FC features of 39 cases were described (Table 3). The skin was involved in 16 (41%) dogs, the liver in 9 (23%), and the head and neck in 5 (13%). The remaining 9 (23%) cases involved kidneys (n = 3), bowel (n = 2), and 1 each in urinary bladder, tibia, lung, and peritoneum. A round cell tumor was suspected in all cases based on cytologic examination performed prior to FC; histopathology and immunohistochemistry were performed in 9 cases, with a diagnosis of lymphoma.
Flow cytometric features of the dominant lymphoid population in extranodal lesions compatible with lymphoma from 39 dogs.
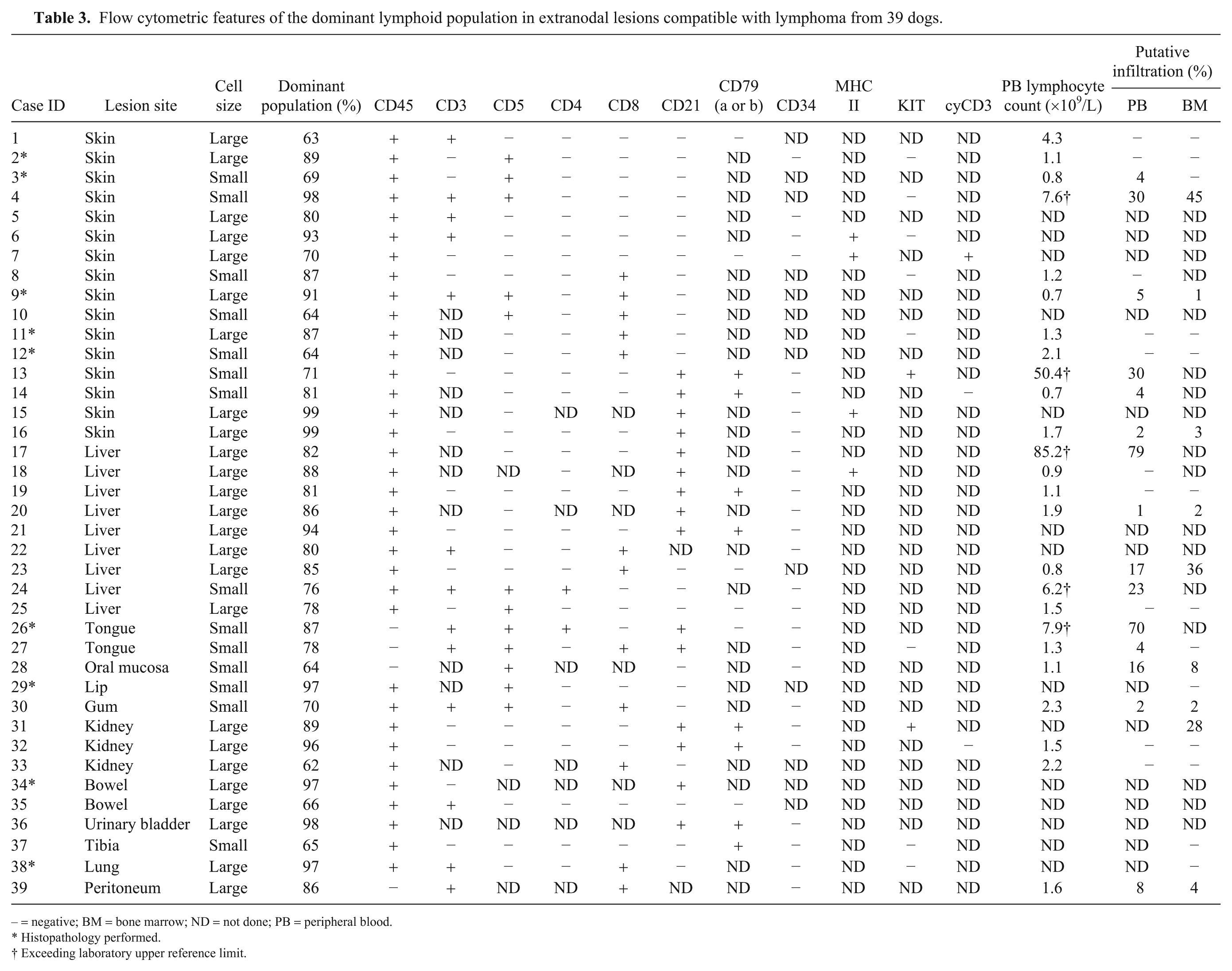
– = negative; BM = bone marrow; ND = not done; PB = peripheral blood.
Histopathology performed.
Exceeding laboratory upper reference limit.
A dominant population of cells was easily identified based on morphologic features (large cells) in 25 (64%) cases. Phenotypic aberrancies were commonly found in T-cell lymphomas (20 cases, 80%), including lack of expression of both CD4 and CD8, discordant expression of pan–T-cell markers, expression of CD8 but not of CD3 or CD5, lack of expression of CD45, and expression of CD21. In particular, 10 (50%) of these cases had more than 1 phenotypic aberrancy. Among suspected B-cell lymphomas, only 1 case (7%) was CD21–CD79+. Interestingly, KIT expression was detected in 2 B-cell lymphomas (14%). In 5 (13%) cases, the dominant population was cells with FC properties overlapping those of normal small lymphocytes; the dominant cells were also small and showed no phenotypic aberrancies, with the exception of KIT expression in 1 dog.
Concerning phenotype distribution, the skin was more commonly affected by proliferation of CD45+CD4–CD8– T cells (n = 7, 44%), the liver by B cells (n = 5, 56%), and the head and neck by CD45– T-cell lymphomas (n = 3, 60%). B-cell proliferation was more common in the miscellaneous group (n = 5, 56%).
PB and BM samples were available for FC analysis in 25 and 22 cases, respectively. Putative neoplastic lymphoid cells were present in 15 (60%) PB samples, with a mean infiltration level of 20 ± 24% (median: 8%, min.–max.: 1–79%) and in 9 (41%) BM samples, with a mean infiltration level of 14 ± 17% (median: 4%, min.–max.: 1–37%).
Follow-up data were retrieved for 14 dogs. Lesions involved the skin in 8 cases; head and neck in 3; liver, bowel, and kidney in 1 each. Ten (71%) dogs were treated with corticosteroids or different chemotherapy protocols and died because of progressive disease, with a median survival of 77 d (range: 15–249 d). Two (14%) dogs with cutaneous lymphoma were treated with multi-agent chemotherapy obtaining partial and complete remission and died as a result of lymphoma-unrelated causes after 113 and 603 d, respectively. Two (14%) dogs with tongue lesions received chemotherapy and obtained complete clinical remission; one was still alive after 579 d, the second one died because of lymphoma-unrelated causes after 427 d.
Discussion
Approximately half of the suspected extranodal lymphomas included in our study had an intra-abdominal location, and most of them involved the liver, which caused the dominant health issue in these dogs. This was unexpected, considering the low frequency reported in the literature for this lymphoma presentation in dogs. 16 Conversely, cutaneous lymphomas are common, with the epitheliotropic subtype alone accounting for 3–8% of all canine lymphomas. 4 This result can be explained by the preferential use of less invasive sampling when intra-abdominal lesions are present, whereas the skin is more likely to be biopsied. Nevertheless, the presence of mild peripheral lymphadenomegaly may have gone unnoticed by the clinicians in some cases, thereby raising the number of dogs with suspected primary hepatic lymphoma.
The phenotypes of the dominant cell population identified by FC in our study showed a different distribution between nodal and extranodal samples. As described previously, B cell is the most common phenotype in nodal lymphomas,2,36 and CD4+ phenotype is the most frequent in multicentric T-cell lymphomas. 9 Cutaneous lymphomas are more frequently composed of CD4– T cells with variable expression of CD8,4,24 whereas cutaneous B-cell lymphomas are less common.7,8
Interestingly, the prevalence of a CD45– T-cell phenotype did not vary between nodal and suspected extranodal lymphomas. This phenotype is considered highly suggestive of T-zone lymphoma (TZL) in dogs.22,30,33 Three of 4 CD45– T-cell extranodal lymphomas in our case series were located within the oral cavity, and 2 of them involved the tongue. This has been described as a novel presentation of canine TZL. 15 The remaining CD45– T-cell lymphoma was a peritoneal mass near the spleen. The neoplastic cells in the mass were large based on the FC morphologic scattergram, and expressed CD3 and CD8. Unfortunately, CD5 and CD21 expression was not tested, and cytologic specimens were not available for review. Because cells were large, it is likely that the final diagnosis in this case was peripheral T-cell lymphoma rather than TZL.
We found that <60% of submitted extranodal samples were suitable for FC assessment, which is considerably lower than the results obtained for nodal samples (>90%). Several possibilities might explain this difference, including discomfort in the sampling procedure given the intra-abdominal location of the lesions, different size and characteristics of the lesion (extranodal tissue thickening vs. gross LN enlargement), different cellular exfoliation from tissues other than nodes, and higher content of debris and parenchymal cells in the extranodal lesions. Further, a greater variety of lesions can affect extranodal sites compared to LN, which is confirmed by the relatively high frequency (>20%) of non-hematopoietic tumors that were encountered among extranodal samples. Finally, other pre-analytical factors may have influenced the diagnostic yield of the samples, as has been demonstrated in canine LNs 5 and nodal and extranodal lesions in cats. 23 Regardless of the underlying causes, the risk of obtaining samples not suitable for FC assessment should be taken into account in the diagnostic workup of extranodal lesions.
Phenotypic aberrancies were commonly found in the cases consistent with extranodal lymphomas. Phenotypic aberrancies are defined as gross antigen deletions, expression of antigens that are not normally present on the cells, and co-expression or loss of both CD4 and CD8. 18 In our case series, phenotypic aberrancies were detected in 20 (80%) samples consistent with T-cell lymphoma and in 1 (7%) consistent with B-cell lymphoma. Phenotypic aberrancies are generally more common in T-cell than B-cell nodal lymphomas, 12 likely because a larger panel of T-cell antigens is tested routinely, allowing more detailed phenotypic definition. Conversely, only a few canine B-cell antigens can be tested by FC in dogs. CD79 labeling requires permeabilization, and is expensive, time-consuming, and is generally omitted if the cells of interest are CD21+. This approach further reduces the number of B-cell antigens tested.
We recorded KIT expression in 2 cases. KIT expression has been investigated in canine nodal lymphomas, 13 and the activity of masitinib, a tyrosine kinase inhibitor, has been documented in 10 dogs with epitheliotropic lymphoma, although none of them expressed KIT by immunohistochemistry. 17 Further studies are needed to assess the possible clinical and therapeutic significance of KIT expression in canine extranodal lymphomas.
We found high percentages of putative neoplastic cells in PB and BM of dogs with suspected extranodal lymphoma, which supports the utility of assessing infiltration of these 2 tissues in extranodal lymphomas. We did not consider clinical and prognostic significance in our study. FC has optimal diagnostic performance in staging canine large B-cell lymphoma, 28 but validation in other lymphoma subtypes is still lacking. However, large cells or phenotypic aberrancies are not present in PB from healthy dogs. 10 Thus, we have confidence in the specificity of the results obtained for FC staging for most of the cases included in our study. A small subset of cases had a dominant population of small cells without phenotypic aberrancies in the primary extranodal lesion; thus, the cells with the same morphologic and phenotypic properties detected in PB and BM may represent either infiltrating neoplastic cells or normal and reactive lymphocytes, or both. PCR for antigen receptor rearrangement would be informative in these cases.
The retrospective nature of our study is a major limitation. Sampling procedures differed among veterinarians, influencing the diagnostic yield of cells. The antibody panel applied also varied in our dataset. In particular, the reduced number of cases tested for MHC II expression prevented us from deriving any information on this marker, which has been associated with a worse prognosis in dogs with nodal B-cell and CD4+ CD8– T-cell lymphomas if not expressed.9,26 Finally, histopathology was performed in only a small number of cases; therefore, we could not assess if FC features differed among different lymphoma histotypes. Further studies are needed to compare FC results and histologic diagnoses in a large case series, in order to assess the diagnostic utility of FC in discriminating lymphomas from non-neoplastic lymphoid lesions.
FC can assist in the diagnostic workup in dogs with suspected extranodal lymphoma, despite the high percentage of non-diagnostic samples. Neoplastic cells may be distinguishable from normal residual lymphocytes by FC, facilitating staging procedures and quantification of infiltrating cells in PB and BM samples. We recommend the concomitant use of histopathology and FC. The advantages of FC are the short turnaround time (results are available the same day of sample delivery to the laboratory), the less invasive nature of sampling, and more comprehensive immunophenotyping; histopathology may provide a definitive diagnosis of lymphoma that includes architectural characterization and epitheliotropism of the neoplastic cells, but has a longer turnaround time.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.