
Abstract
A 12-y-old neutered male Portuguese Water dog was presented because of a 1-y history of persistent hyporexia, diarrhea, and recurrent pyelonephritis. Abdominal ultrasound revealed hepatic nodules and diffuse splenomegaly, and radiographs revealed a mediastinal mass. Fine-needle aspirates of the liver, spleen, and mediastinal mass were suspicious for lymphoma. Flow cytometry identified small T cells that co-expressed CD4 and CD8 at all sites, most suspicious for thymoma, but lymphoma could not be ruled out. PCR for antigen receptor rearrangements analysis identified polyclonal amplification of the T-cell receptor genes, more consistent with thymoma than lymphoma. Histopathology of the liver and thymic mass confirmed thymoma with hepatic metastasis.
Thymomas are neoplasms arising from thymic epithelial cells. Thymomas rarely metastasize in dogs,2,10,12 and generally have good overall survival with excision alone. 18 Malignant thymomas with regional infiltration and/or distant metastasis have been reported infrequently in dogs.1,10–12,15 We detail the clinical history, presentation, flow cytometry, PCR for antigen receptor rearrangements (PARR), and lesions of a metastatic thymoma in a dog.
A 12-y-old neutered male Portuguese Water dog was presented to The Animal Medical Center (AMC; New York, NY) with persistent decreased appetite, weight loss, and intermittent diarrhea, following an 18-mo history of recurrent urinary tract infections and pyelonephritis with an incomplete response to antibiotic treatment. The dog had a mild-to-moderate increase in alkaline phosphatase (10.3 μkat/L; reference interval [RI]: 0.25–2.3 μkat/L [619 IU/L; RI: 15–140 IU/L]) on blood chemistry over a 12-mo period. A low-dose dexamethasone suppression test performed before referral was normal; an adrenocorticotropic hormone stimulation test was weakly positive (pre-stimulation 91 nmol/L, RI: 25–125 nmol/L [3.3 μg/dL, RI: 0.9–4.5 μg/dL]; post-stimulation 670 nmol/L, RI: <520 nmol/L [24.3 μg/dL, RI: <22 μg/dL]). The primary veterinarian diagnosed pancreatitis 3 mo prior to presentation based on increased canine pancreatic lipase immunoreactivity (956 μg/L; RI: 0–200 μg/L) and trypsin-like immunoreactivity (>50 μg/L; RI: 5–35 μg/L). Ultrasound revealed hepatic nodules, bilaterally enlarged adrenal glands, segmental intestinal corrugation consistent with enteritis, and a small volume of peritoneal effusion suggestive of regional peritonitis. Full-thickness gastrointestinal biopsies were recommended to further evaluate the cause of the segmental enteritis. At the AMC, prior to exploratory abdominal surgery, thoracic radiographs revealed a mediastinal mass and hepatomegaly, which postponed surgery. Approximately 1 mo later, follow-up abdominal ultrasound revealed further enlargement of the hepatic nodules and the spleen. Ultrasound-guided, fine-needle aspirates of the hepatic nodules, body of the spleen, and cranial mediastinal mass were submitted for cytology at the AMC and for flow cytometry at the Colorado State University Clinical Immunology Laboratory (CSU-CIL; Fort Collins, CO).
Cytology of the mediastinal mass, liver, and spleen identified an expanded population at each site of predominantly intermediate-sized lymphocytes with finely stippled chromatin, often with a concurrent population of small mature lymphocytes. These findings were suspicious for lymphoma.
Aspirates of the spleen–liver sample (combined prior to submission) and mediastinal mass were sent to the CSU-CIL. Flow cytometry was performed on the spleen–liver and mediastinal mass samples as described previously. 17 Flow cytometry analysis (Kaluza software, Beckman Coulter, Fullerton, CA) revealed an almost identical expansion of small lymphocytes in both samples, with co-expression of T-cell subset antigens, CD4 and CD8. Although rare cases of lymphoma can co-express CD4 and CD8, 9 several aspects of the flow cytometry results raised suspicion that these lymphoid cells were a thymocyte population, despite their aberrant location. Displaying features typical of normal canine thymocytes (Fig. 1C), these cells were very small based on forward scatter, and the majority of the cells did not express CD3 (Fig. 1A, 1B) or major histocompatibility complex class II (MHC II; not shown). Although some aggressive T-cell lymphomas can have these properties, the cells involved are usually much larger, 9 and typically express high levels of CD3 (KL Hughes, AC Avery, unpublished observations). Based on the flow cytometry results, a metastatic thymoma was considered most likely; however, we could not rule out an unusual lymphoma.

Flow cytometry of
To further investigate the possibility of an unusual lymphoma, clonality of the splenic–hepatic aspirate was assessed using the PARR assay as described previously. 16 The results showed polyclonal amplification of T-cell receptor genes (Fig. 2) and no amplification of immunoglobulin heavy chain genes. Such findings did not support a diagnosis of lymphoma and further suggested an extensive polyclonal T-cell population, more supportive of a thymocyte population.
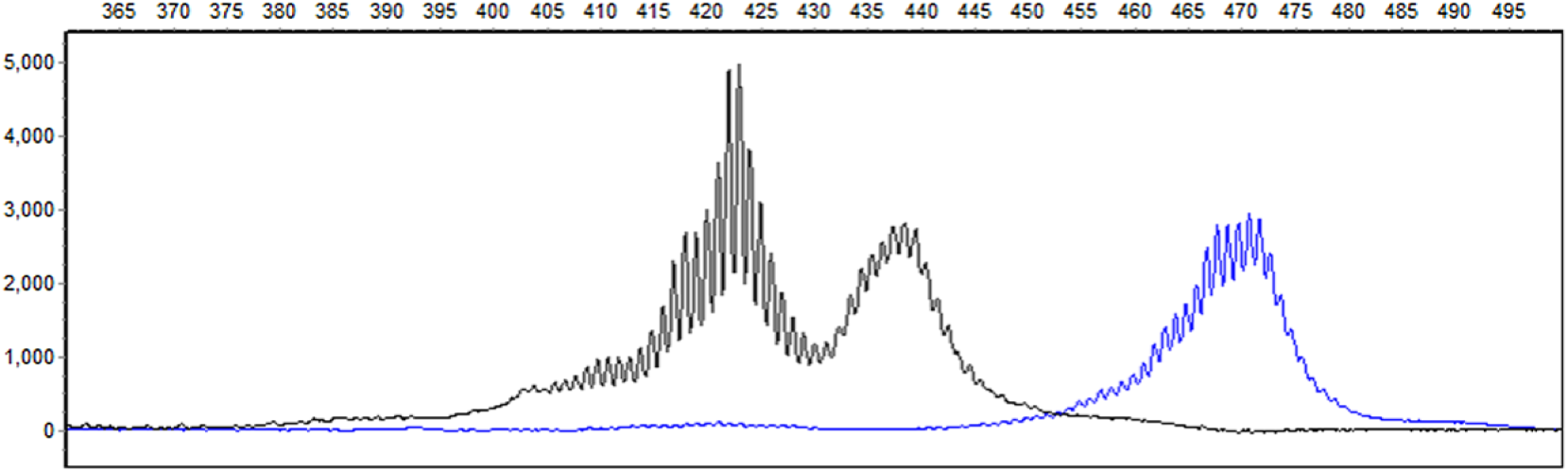
PCR for antigen receptor rearrangements of the spleen of a dog with metastatic thymoma. Molecular clonality assessment of genomic DNA was conducted using capillary electrophoresis and BioCalculator (Qiagen, Hilden, Germany) and GeneMarker (Soft Genetics, State College, PA) analysis. There is a broad polyclonal result when assessed with T-cell receptor gamma primers. The higher molecular weight PCR products (blue) in the 470 nucleotide range were amplified with V gamma 2 primer. The PCR products in the 420 range (black) were amplified with V gamma 3 primer. 8
Approximately 10 d after aspirates were acquired, biopsies of the cranial mediastinal mass, liver, gastrointestinal tract, mesenteric and prescapular lymph nodes, and spleen were obtained for evaluation and fixed in 10% neutral-buffered formalin. Tissues were routinely processed and paraffin-embedded, and tissue sections of 5-μm thickness were cut and stained with hematoxylin and eosin. Immunohistochemistry for sections of the mediastinal mass and liver was performed for CD3 (monoclonal mouse anti-human CD3, LN10 clone, Leica Biosystems, Newcastle Upon Tyne, UK), PAX5 (monoclonal mouse anti-human Pax5, DAK-Pax5 clone, Dako North America, Carpinteria, CA), and the epithelial cell origin in the thymic mass was confirmed with cytokeratin AE1/AE3 (polyclonal mouse anti-human AE1 and AE3, Leica Biosystems). The mediastinal mass was consistent with a thymoma with 2 distinct cell populations (Fig. 3A, 3C, 3D), including a heterogeneous proliferation of intermixed small lymphocytes with less frequent individualized and aggregated polygonal cells (thymic epithelial cells). The epithelial cells had abundant eosinophilic cytoplasm and a round nucleus with dispersed chromatin and one-to-multiple small prominent nucleoli. There was mild-to-moderate anisocytosis and anisokaryosis with 2 mitotic figures identified in 10 high-power fields (400×). In the liver sample, >90% of the evaluated section was effaced by a similar combination of both the lymphoid and epithelial populations described in the mediastinal mass with only a few remaining hepatocytes (Fig. 3B), consistent with hepatic metastasis of the thymic neoplasm. Immunohistochemistry demonstrated that the background lymphocyte population had immunoreactivity for cytoplasmic CD3, and the thymic epithelial cells showed immunoreactivity for cytoplasmic cytokeratin AE1/AE3 (Fig. 3C, mediastinal mass, cytokeratin AE1/AE3; 3D, mediastinal mass, CD3). Very few lymphocytes showed nuclear immunoreactivity for PAX5 (not shown).
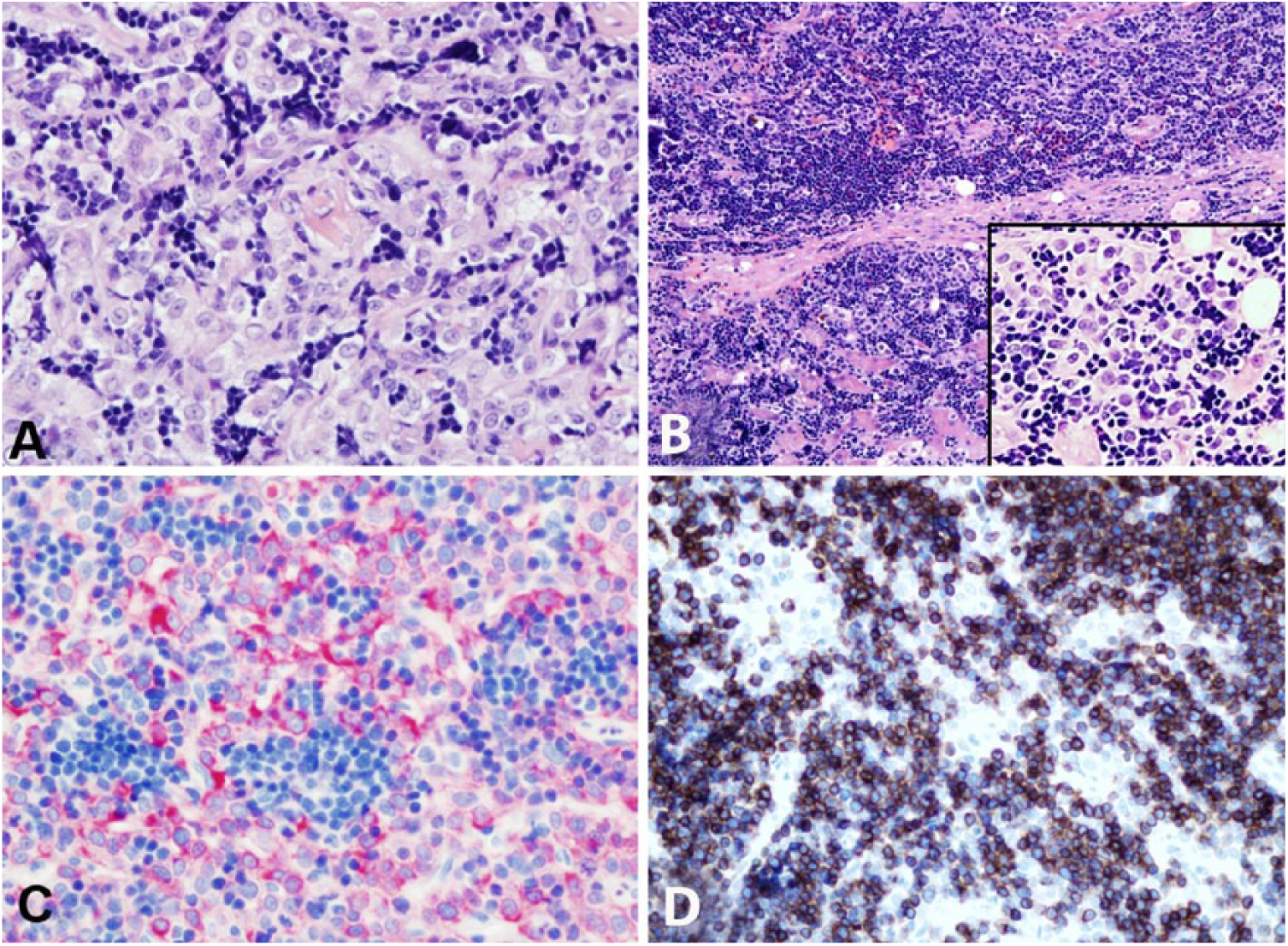
Immunohistochemistry of
The gastrointestinal biopsies revealed neutrophilic gastritis, eosinophilic and lymphoplasmacytic enterocolitis, and lymphoid hyperplasia with eosinophil expansion in the mesenteric lymph node. The prescapular lymph node had evidence of an inflammatory drainage reaction with lymphoid hyperplasia. The splenic sample showed extramedullary hematopoiesis, plasmacytosis, and hemosiderosis, without overt evidence of metastasis of the thymic neoplasia.
Given the metastatic nature of the thymic neoplasia, the owners elected not to pursue further treatment, and the patient was euthanized ~1 mo later. Autopsy was not performed.
In the rare case reports of metastatic thymoma in the dog, which date back to 1974, local and disseminated disease is described.1,10–12,15 There was local metastasis in one dog with dissemination as far as the lung and pharynx; the dog also had generalized myasthenia gravis (MG) and died from either an overdose of pyridostigmine for MG or from an acute cholinergic crisis. 11 In the remaining case reports, one dog was euthanized because of progressive renal failure, with incidental identification of thymoma with widespread metastasis to the liver, spleen, and bone marrow. 10 The clinical signs could not be attributed to the progressive nature of the thymoma, and the consequences of renal failure were the most clinically relevant disease process in that report. 10 A 2017 case report also showed an infiltrative mass in the cranial mediastinum, with dozens of metastases in the abdominal cavity including the pancreas, liver, spleen, and kidney. 12 In our case, we were unable to determine the extent of mediastinal or abdominal infiltration beyond the liver involvement.
Co-expressing CD4+CD8+ T cells are characteristic of thymoma because they represent the most abundant T-cell precursors in the developing thymus. When T-cell precursors enter the thymus, they do not express either CD4 or CD8, but these proteins are upregulated together in the same cell during T-cell receptor rearrangement when thymocytes transition into the double-positive (CD4+CD8+) state.7,13 During T-cell development, successful pre–T-cell antigen receptor (TCR) expression leads to proliferation of the immature double-positive T cells with a diverse TCR repertoire. 13 In the process of positive selection, thymocytes interact with MHC I and MHC II ligands on cortical epithelial cells resulting in down-regulation of either CD4 or CD8, and subsequent single-positive T cells then reside in the medulla. 13 Only mature T cells expressing either CD4 or CD8 will exit the thymus into peripheral circulation. Although peripheral lymphocytosis can be seen in cases of thymoma, it consists only of mature, single-positive CD4 and CD8 T cells, or T cells expressing neither CD4 nor CD8.3,6 These latter cells may be γδ T cells. 6 Therefore, the finding of CD4+CD8+ lymphocytes in the periphery of this dog with thymoma was unexpected.
Differential considerations for the presence of CD4+CD8+ T cells in peripheral non-thymic tissues include: lymphoma derived from a thymic precursor, aberrantly expressed antigens within an activated T-cell population, 4 or as suspected in our case, normal T cells developing on metastatic neoplastic thymic epithelium. In our case, the suspicion for metastatic thymoma in the liver, based on the flow cytometry finding of small lymphocytes co-expressing CD4 and CD8, was further substantiated by the polyclonal PARR results and was confirmed with the biopsy findings and immunohistochemistry results. We estimate the sensitivity of the PARR assay to be 85% in dogs (manuscript in preparation). A false-negative is considered very unlikely given the prominent polyclonal nature, which is typical of a thymocyte population, and the subsequent metastatic lesions identified by histopathology. The splenic biopsy could not confirm metastasis within the spleen, although the splenic sample was very small and may not have been representative.
The dog in our case had a long history of recurrent urinary tract infections and pancreatitis, as well as gastroenterocolitis. Immune-mediated paraneoplastic syndromes described with thymomas in dogs include MG, polyarthritis, masticatory muscle myositis, keratoconjunctivitis sicca, and diabetes mellitus. 14 In humans, MG is the most common autoimmune disease associated with thymic neoplasia, but a variety of autoimmune diseases have been described, including frequent reports of autoantibodies to cytokines. 5 In one study, 30% of human patients with thymic neoplasia had opportunistic infections, and all had multiple anti-cytokine autoantibodies. 5 Similarly, it is possible that the pancreatitis, recurrent urinary tract infections, and/or enteritis in this dog could have been the result of an immune-mediated paraneoplastic syndrome, but this cannot be confirmed because the thymoma remained untreated.
In our case, flow cytometry was the initial laboratory test that supported metastatic thymoma in this dog, based on an expansion of CD4+CD8+ T lymphocytes identified in the liver and spleen. Flow cytometry has previously been employed to distinguish mediastinal lymphoma from thymoma based on the presence of ⩾10% CD4+CD8+ small lymphocytes in cases of thymoma. 9 Our case of a thymoma in a dog with identification of CD4+CD8+ lymphocytosis at sites of distant metastasis highlights the utility of flow cytometry.
Footnotes
Acknowledgements
Preliminary reports of the findings were presented at the 2015 American College of Veterinary Pathology, American Society for Veterinary Clinical Pathology, and Society of Toxicologic Pathology combined annual meeting, 17–21 October 2015, Minneapolis, MN.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.