
Abstract
Respiratory diseases have a major impact on racehorses in training and are often cited as the second most common reason of horses failing to perform. Cases were submitted by the California Horse Racing Board to the California Animal Health and Food Safety laboratory for postmortem examination between January 1, 2005 and December 31, 2014. We determined the demographics of racehorses with fatal pneumonia, characterized the pathologic findings in animals with a postmortem diagnosis of respiratory infection, and determined the most significant pathogens associated with lower respiratory tract disease. We analyzed autopsy reports from 83 horses with a diagnosis of pneumonia, bronchopneumonia, and/or pleuropneumonia. The most common presentation was pleuropneumonia (71% of cases), with extensive areas of lytic necrosis and abscesses of the pulmonary parenchyma. Streptococcus equi ssp. zooepidemicus, a normal mucosal commensal of the upper respiratory tract of healthy horses, was the most commonly isolated organism (72% of cases), either in pure culture or accompanied by other aerobic or anaerobic bacteria. Its presence in the pulmonary parenchyma is associated with severe and extensive damage to the lung. Furthermore, this agent has zoonotic potential, which stresses the importance of early detection and proper management of cases of pneumonia in racehorses.
Introduction
Respiratory diseases have a major impact on racehorses and are often cited as the second most common reason for loss of training days and significant veterinary costs.7,10,33 Predisposing factors for infectious pulmonary disease have been reported to include long-distance transportation with inadequate rest periods, complications of esophageal obstruction, inhalation of food or saliva, immunosuppression, and/or strenuous exercise shortly after transport.13,14,17,22,28
Adult horses most commonly develop pneumonia when bacteria aspirated from the environment, nose, or oropharynx reach the lower airways and overwhelm the pulmonary defense mechanisms. Numerous opportunistic pathogens have been isolated in cases of pneumonia in horses, and mixed aerobic and anaerobic bacteria are present in many cases. 26 Pneumonia in racehorses most commonly occurs associated with one or multiple aerobic inhabitants of the upper respiratory mucosa, including, but not limited to, Streptococcus equi ssp. zooepidemicus (S. zooepidemicus), Pasteurella spp., Actinobacillus spp., Klebsiella spp., Escherichia coli, and Actinomyces spp.5,11 Contrary to the situation in other mammalian species, viral infections do not seem to play a major role as a predisposing factor for bacterial pneumonia in horses.4,7,34
A few studies have been published on pneumonia of racehorses. However, most of those studies were either clinical or based on a small number of animals. A postmortem program is run by the California Animal Health and Food Safety Laboratory System (CAHFS) for the California Horse Racing Board (CHRB). This program, created in 1990 by mandate of the California legislature, requires that every horse that dies at any facility under the jurisdiction of the CHRB must undergo a postmortem examination. More than 6,500 horses have been autopsied to date as part of the CHRB postmortem program. Approximately 25–30% of those were medical cases; 70–75% died spontaneously or were euthanized because of catastrophic musculoskeletal injuries (https://goo.gl/pOUCPO). We report herein a brief description and analysis of the cases of pneumonia in racehorses autopsied at CAHFS as part of the CHRB program over a 10-y period, with special emphasis on the epidemiology and pathology findings, as well as review the current literature on equine pneumonia.
Retrospective study
Cases with a diagnosis of lower respiratory disease, including pneumonia, bronchopneumonia, and/or pleuropneumonia as the cause of death in horses submitted to CAHFS San Bernardino and Davis branches by the CHRB between January 1, 2005 and December 31 2014, were collated. The autopsy reports for all of those cases were analyzed.
An autopsy was performed on each case, and samples were collected for histopathology and microbiology testing. A heavy metal screen and/or fecal floatation were performed in a few cases. Tissues for histopathology included, in most cases, trachea, lung, heart, diaphragm, liver, spleen, kidney, urinary bladder, adrenal glands, esophagus, stomach, small intestine, cecum, colon, and brain. These tissues were fixed in 10% neutral-buffered formalin (pH 7.2) and processed by routine histologic methods to obtain 5-µm sections that were stained with hematoxylin and eosin. Selected lung sections were also stained with Gram and/or periodic acid–Schiff stains.
Samples for microbiology, which included lung tissue, swabs from different parts of the respiratory system and/or pleural fluid, were collected aseptically and processed following CAHFS standard operating procedures. Briefly, these specimens were streaked onto chocolate, Columbia blood, and MacConkey agar plates (Hardy Diagnostics, Santa Maria, CA) and incubated at 37°C aerobically and/or under microaerophilic conditions. The plates were examined after 24 and 48 h. For anaerobic cultures, samples were included on pre-reduced anaerobically sterilized Brucella plates (Anaerobe Systems, Morgan Hills, CA) and cultured for up to 5 d at 37°C in an anaerobic environment. For mycoplasma culture, samples were inoculated on mycoplasma N agar plates (Biological Media Services, University of California–Davis, Davis, CA) and incubated for 7 d and/or inoculated in mycoplasma D broth (Biological Media Services) for 48 h and then subcultured on mycoplasma N agar plates for another 7 d.
All cases were tabulated by month of submission, breed, age, sex, morphologic diagnosis, lesion distribution within the lungs, and microbiology results, using commercial software programs (Excel 2013, Microsoft, Redmond, WA; Stata/SE 14.1, StataCorp, College Station, TX). Seasons were defined as winter (January–March), spring (April–June), summer (July–September), or fall (October–December).
The following morphologic diagnoses were defined based on gross and microscopic examination: 1) pleuropneumonia: inflammation of the lung and visceral and/or parietal pleura (Fig. 1); 2) bronchopneumonia: inflammation of the pulmonary parenchyma centered on airways and adjacent alveolar spaces with no involvement of pleura (Fig. 2); 3) pleuritis: inflammation in the visceral and/or parietal pleura without significant inflammation of the pulmonary parenchyma; 4) embolic pneumonia: multifocal inflammation of the pulmonary parenchyma centered on blood vessels; and 5) interstitial pneumonia: diffuse inflammation of alveolar septa and type II pneumocyte hyperplasia. The distribution of the lesions was classified as unilateral or bilateral, cranioventral, caudal, or whole lung. The presence of abscesses (well-demarcated foci of suppuration lined with a fibrous capsule) and areas of lytic necrosis (irregular, dark-brown to black, friable areas of pulmonary parenchyma) were evaluated in each case. An additional category that combined presence of abscesses and areas of lytic necrosis (Fig. 3) and pleuropneumonia or bronchopneumonia was created, with the purpose of evaluating whether the presence of these lesions was associated with side (right or left) or distribution (cranioventral, caudal, or multifocal). The Fisher exact test for data count was used for this purpose, with significance set at p < 0.05.
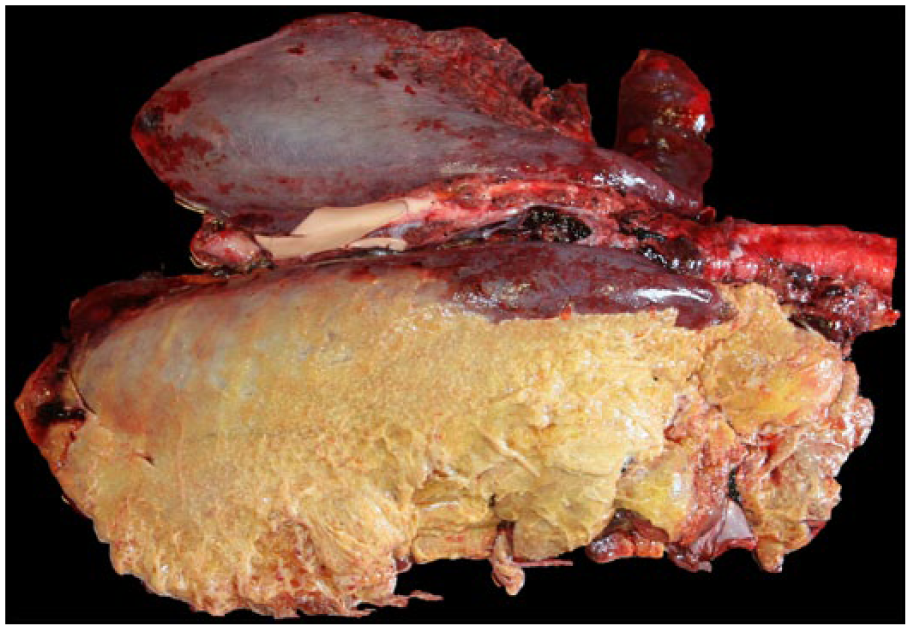
Unilateral fibrinous pleuropneumonia in a horse. The right lung is almost entirely covered by abundant fibrin.
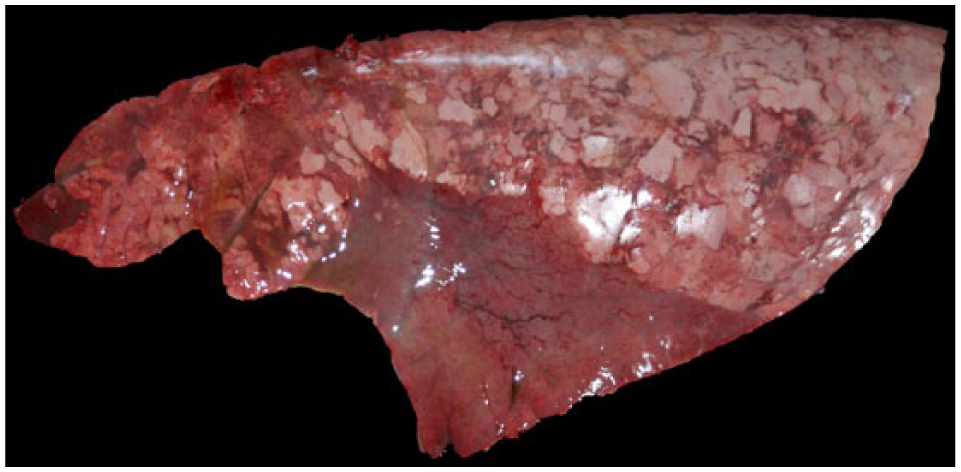
Bronchopneumonia in a horse. There is a well-demarcated area of consolidation and dark red discoloration of the lung.
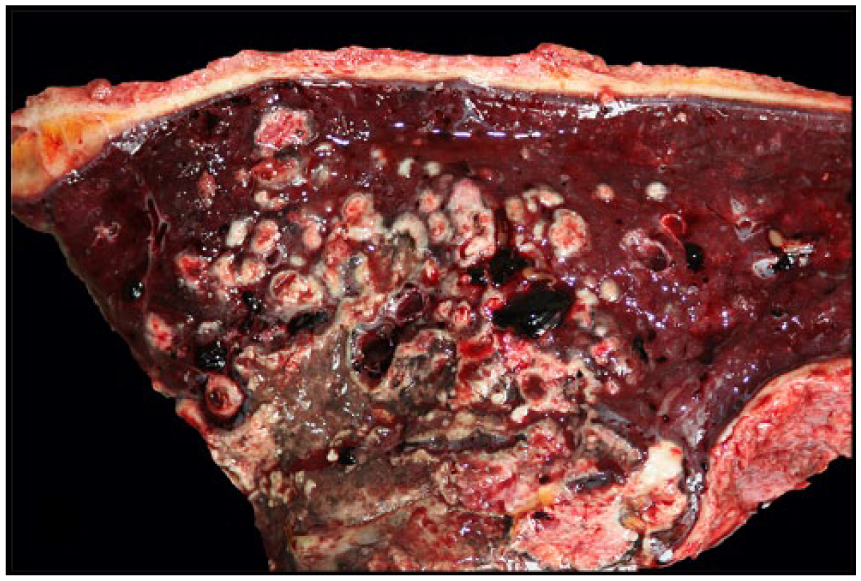
Pleuropneumonia in a horse. Cross-section of the lung showing multifocal-to-coalescing areas of necrosis and abscesses in the pulmonary parenchyma and a pleural surface (top margin) expanded by fibrin.
Between January 2005 and December 2014, 83 autopsies of horses with respiratory disease were performed by CAHFS laboratories, Davis and San Bernardino branches. These cases originated from 4 racetracks in northern California and 4 tracks in southern California. Thirty-eight horses (46%) were female, 33 (40%) were geldings, and 12 (14%) were intact male. Horses were Thoroughbreds (74, 89%) and Quarter Horses (9, 11%). Ages were 2–9 y, although the majority was 2–5 y old (Fig. 4). Horses were received during all 4 seasons, with the following distribution: 16 (19%) in winter, 20 (24%) in spring, 25 (30%) in summer, and 22 (26%) in the fall.
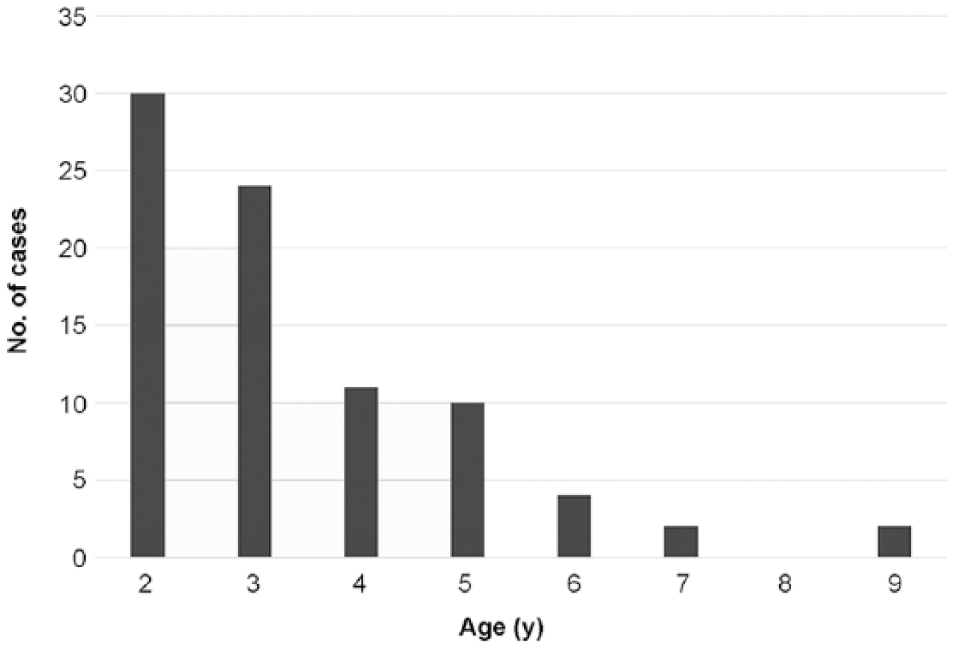
Age of 83 racehorses with respiratory disease.
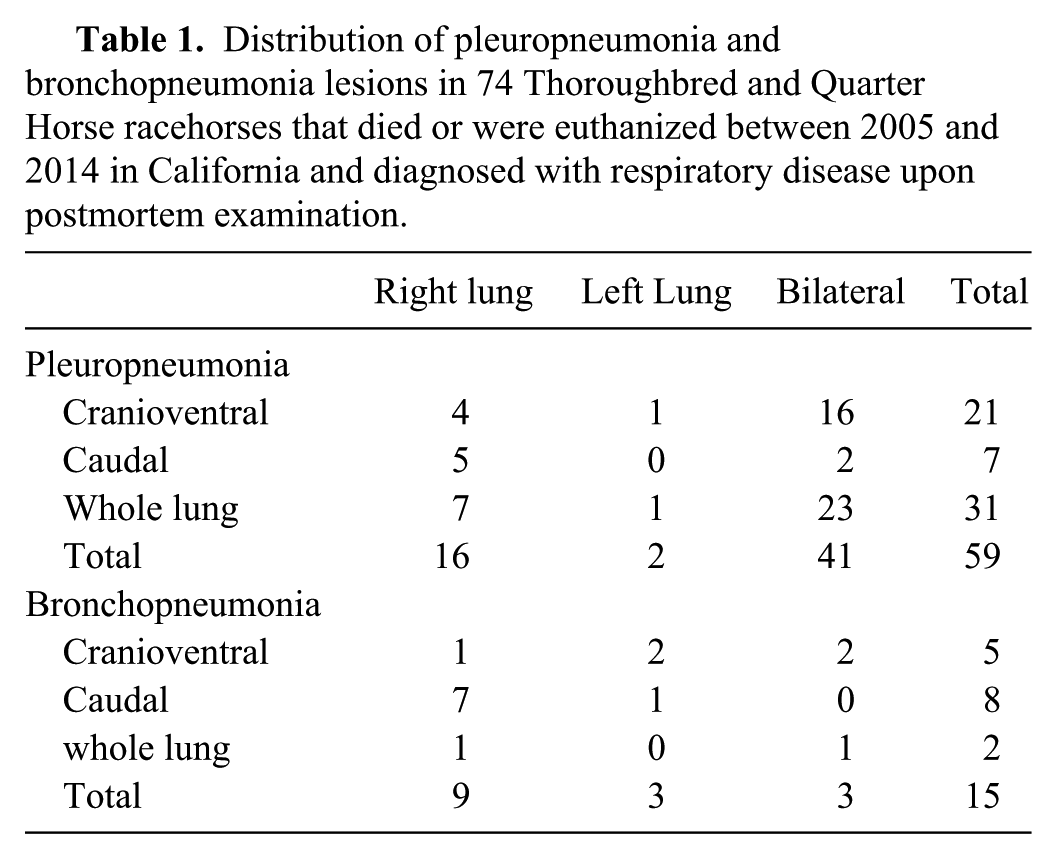
Pleuropneumonia was the most common diagnosis and was detected in 59 cases (71%), followed by bronchopneumonia (15 cases, 18%), pleuritis (4 cases, 5%), embolic pneumonia (3 cases, 4%), and interstitial pneumonia (2 cases, 2%). Pleuropneumonia was most commonly bilateral (41 cases, 70%). In horses with pleuropneumonia, the entire parenchyma of 1 or both lungs was affected in 31 cases (52%); the cranioventral part of 1 or both lungs was affected in 21 cases (36%); and the caudal part was affected in 7 cases. In bronchopneumonia cases (n = 15), the caudal part of the right lung was most commonly affected (7 cases, 44%; Table 1). Four cases (5%) had chronic bilateral pleuritis without significant pneumonia. Three cases (4%) had bacterial embolic pneumonia, all associated with sepsis. Of the cases of embolic pneumonia, one was associated with endocarditis, another with bacteremia in which no particular organ was determined to be the primary site of infection, and a third with colitis. Two horses had interstitial pneumonia, one with findings compatible with equid herpesvirus 5 (EHV-5) infection (although this agent could not be confirmed), and the other with microscopic findings suggestive of a disseminated bacterial infection.
Distribution of pleuropneumonia and bronchopneumonia lesions in 74 Thoroughbred and Quarter Horse racehorses that died or were euthanized between 2005 and 2014 in California and diagnosed with respiratory disease upon postmortem examination.
In 43 cases (73%), one or multiple abscesses and areas of lytic necrosis were noted associated with bronchopneumonia or pleuropneumonia. The most common location for these lesions was the caudal portion of the right lung (p < 0.001; Fig. 5).
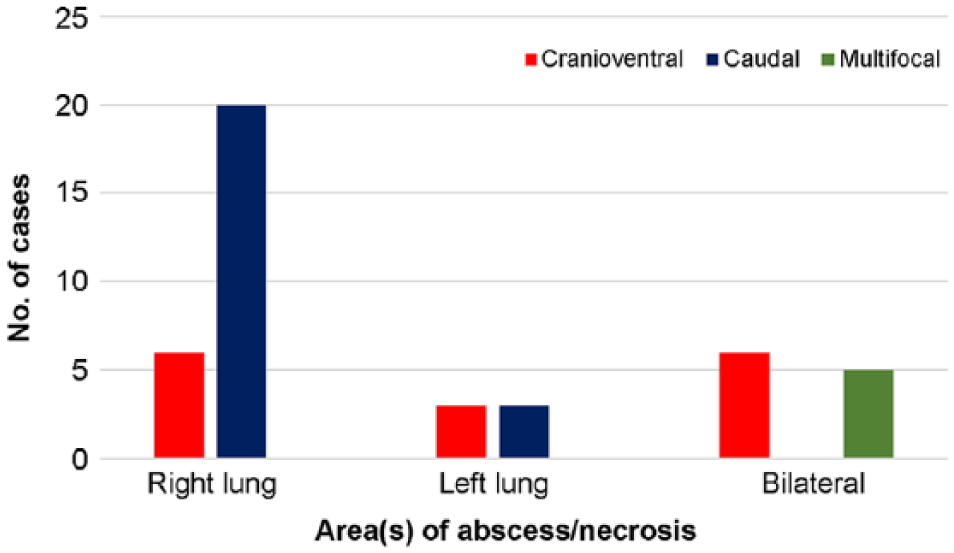
Macroscopic distribution of pulmonary abscess or lytic necrosis in the lungs of horses with pleuropneumonia and bronchopneumonia in which these lesions were present (n = 43).
Aerobic and anaerobic bacterial cultures were performed in all cases of pleuropneumonia, bronchopneumonia, embolic pneumonia, and pleuritis. Bacterial isolates were obtained from 74 cases. In total, 114 bacterial species were isolated, and rare cases had up to 4 different isolates. The most commonly isolated bacterium was S. zooepidemicus, which was isolated from 53 cases (72%), followed by coliforms (16 cases, 22%), mixed bacterial flora (10 cases, 14%), and Actinobacillus spp. (10 cases, 14%), and other bacterial species (Table 2). S. zooepidemicus was the only bacterium isolated in 24 cases (32%).
Bacteria isolated from the lung of 74 Thoroughbred and Quarter Horse racehorses that died or were euthanized between 2005 and 2014 in California and diagnosed with respiratory disease upon postmortem examination.*
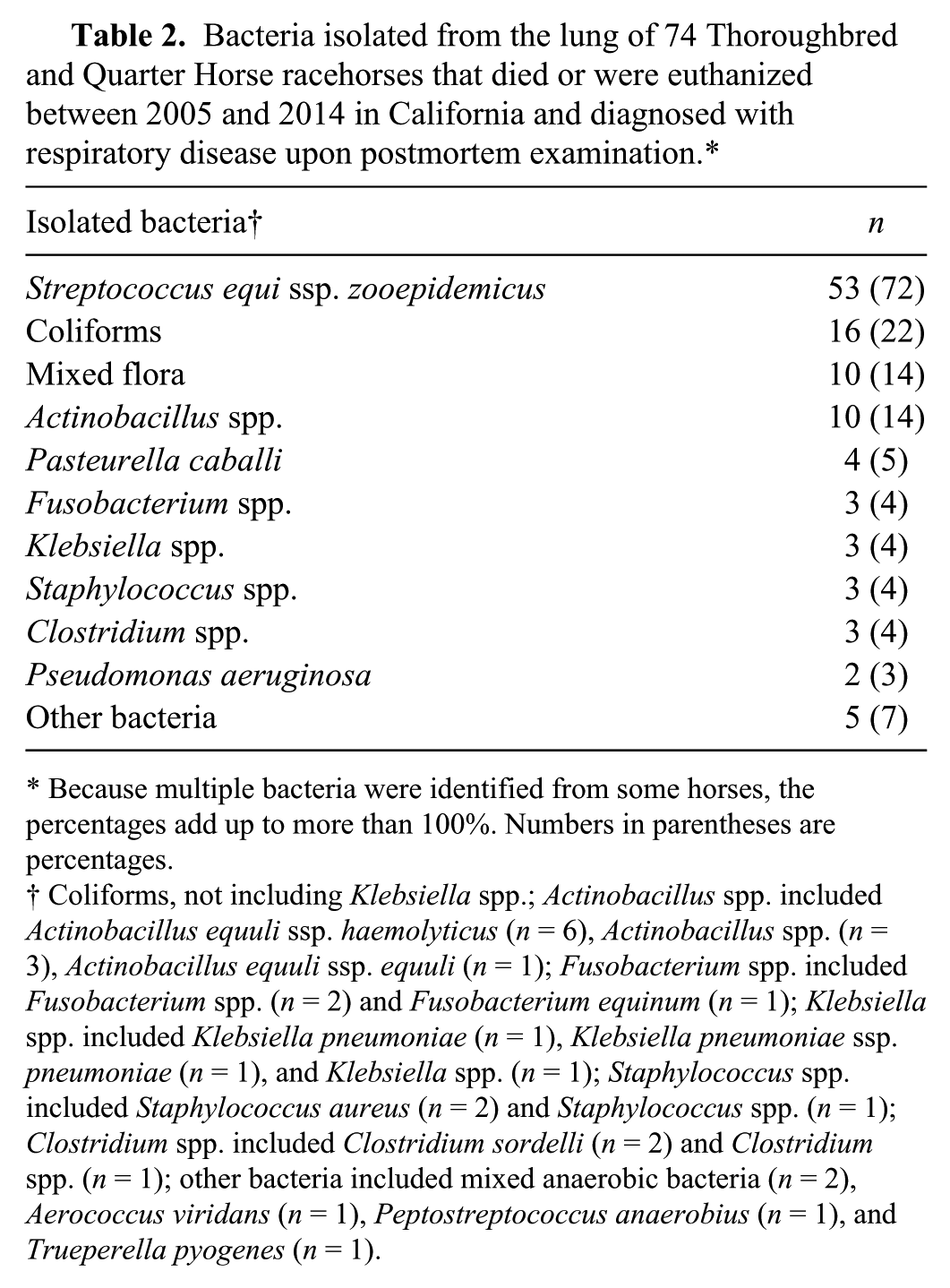
Because multiple bacteria were identified from some horses, the percentages add up to more than 100%. Numbers in parentheses are percentages.
Coliforms, not including Klebsiella spp.; Actinobacillus spp. included Actinobacillus equuli ssp. haemolyticus (n = 6), Actinobacillus spp. (n = 3), Actinobacillus equuli ssp. equuli (n = 1); Fusobacterium spp. included Fusobacterium spp. (n = 2) and Fusobacterium equinum (n = 1); Klebsiella spp. included Klebsiella pneumoniae (n = 1), Klebsiella pneumoniae ssp. pneumoniae (n = 1), and Klebsiella spp. (n = 1); Staphylococcus spp. included Staphylococcus aureus (n = 2) and Staphylococcus spp. (n = 1); Clostridium spp. included Clostridium sordelli (n = 2) and Clostridium spp. (n = 1); other bacteria included mixed anaerobic bacteria (n = 2), Aerococcus viridans (n = 1), Peptostreptococcus anaerobius (n = 1), and Trueperella pyogenes (n = 1).
The results of morphologic diagnosis in relation to the most commonly isolated bacteria are represented in Table 3. S. zooepidemicus was the most commonly isolated bacteria in cases of pleuropneumonia (61%) and bronchopneumonia (73%). Actinobacillus spp. were isolated in all cases of embolic pneumonia (n = 3). S. zooepidemicus was isolated from 31 cases (72%) of pleuropneumonia and bronchopneumonia cases in which intralesional abscesses and areas of lytic necrosis were identified (n = 43; Table 4),
Main isolated bacterial agents from cases of pleuropneumonia, bronchopneumonia, embolic pneumonia, and pleuritis in Thoroughbred and Quarter Horse racehorses that died or were euthanized between 2005 and 2014 in California and diagnosed with respiratory disease upon postmortem examination.*
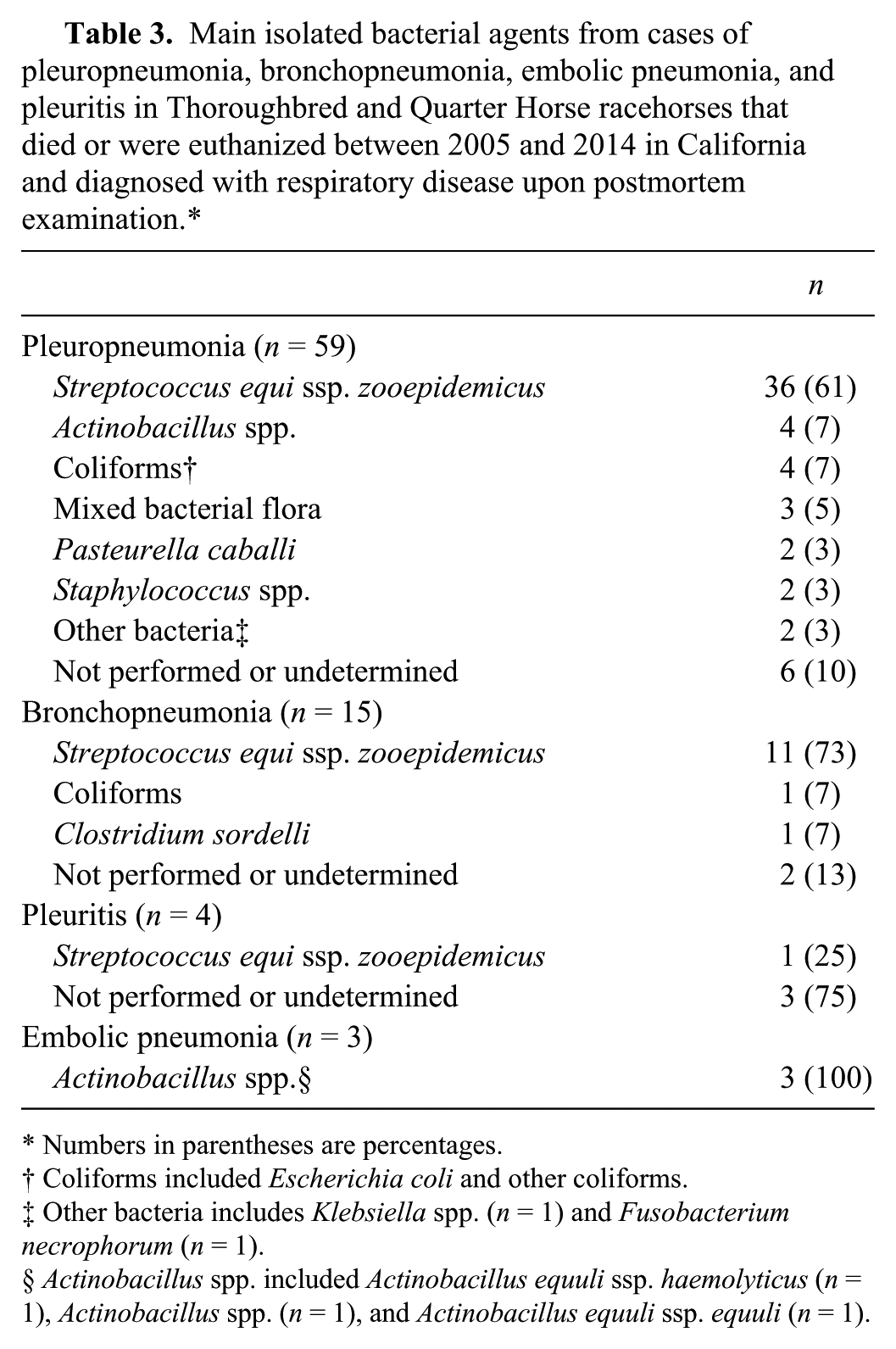
Numbers in parentheses are percentages.
Coliforms included Escherichia coli and other coliforms.
Other bacteria includes Klebsiella spp. (n = 1) and Fusobacterium necrophorum (n = 1).
Actinobacillus spp. included Actinobacillus equuli ssp. haemolyticus (n = 1), Actinobacillus spp. (n = 1), and Actinobacillus equuli ssp. equuli (n = 1).
Main isolated bacterial agent from the areas of abscess and necrosis of 43 Thoroughbred and Quarter Horse racehorses that died or were euthanized between 2005 and 2014 in California and had a diagnosis of pleuropneumonia or bronchopneumonia.*
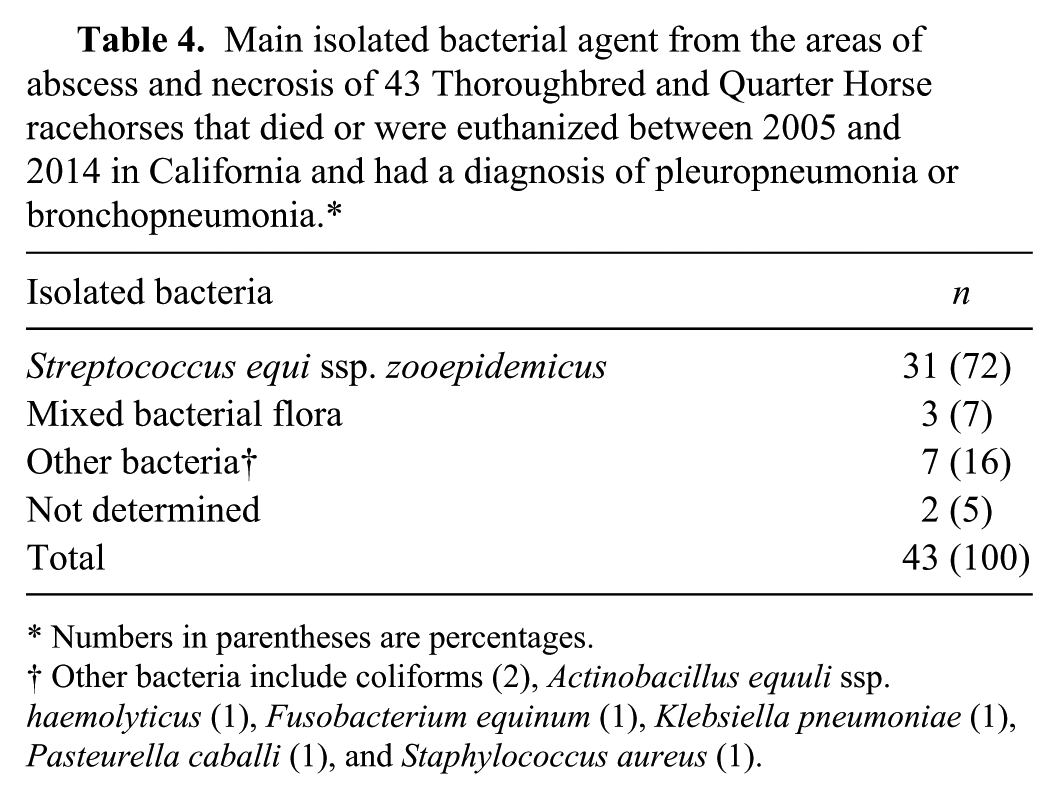
Numbers in parentheses are percentages.
Other bacteria include coliforms (2), Actinobacillus equuli ssp. haemolyticus (1), Fusobacterium equinum (1), Klebsiella pneumoniae (1), Pasteurella caballi (1), and Staphylococcus aureus (1).
Mycoplasma culture was performed in 4 cases. Mycoplasma spp. were only isolated from the lung of a 4-y-old Thoroughbred gelding with pleuropneumonia. Actinobacillus spp. were also isolated from the lung of this horse.
Discussion and review of the literature
The majority of cases of respiratory disease in horses in our study were 2–5 y of age, which is likely because most horses submitted to CAHFS by the CHRB for postmortem examination are within that age range. Therefore, no conclusions can be drawn regarding age predisposition for respiratory disease in racehorses in our study. Previous studies have demonstrated that pneumonia occurs predominantly in young racing horses (2–4-y-old). This is especially true for Thoroughbreds, and is considered to be predisposed by stress, such as that of transportation and strenuous exercise.10,21,25
Pneumonia in racehorses has been strongly associated with restraint during transportation, when animals are unable to lower their heads, which leads to reduced opportunity for clearance of oronasal secretions and consequently increased opportunity for upper respiratory tract normal flora and opportunistic pathogens to reach the lower respiratory tract.18,20,23 In addition, it is postulated that transportation predisposes to desiccating effects of exposure to air currents and low relative humidity, which may reduce the thickness of the respiratory mucus lining and prevent effective ciliary motility. 18 Strenuous exercise, with inhalation of sand, grass, and dirt during racing, can also predispose to lower respiratory tract contamination.2,3,7 In fact, high-intensity exercise can result in a 10-fold increase in aerobic bacterial counts and a 100-fold increase in anaerobic bacterial counts in tracheal aspirates, compared to pre-exercise values. 24 If transportation and exercise both occur within a short period of time, the compound effect of both factors significantly increases the probability of infection of the lower respiratory tract. 22 Housing environment is another important risk factor for respiratory disease in racehorses. Studies of inflammatory airway disease revealed that inflammation of the lower respiratory tract was higher in horses kept in an environment where dust load was high and ventilation was poor. 7 Also, when naive animals are introduced into a new environment, they are exposed to new pathogens and are therefore predisposed to the development of infections. 11
In our study, pleuropneumonia was the most common fatal respiratory infection. The majority of the pleuropneumonia cases were bilateral, and the parenchyma of the caudal portion of the right lung was most commonly affected. A large proportion of animals with pleuropneumonia had abscesses and coalescing areas of lytic necrosis of the pulmonary parenchyma. This is in agreement with previous clinical studies based on both auscultation and radiology, in which the cranial region of the right caudal lobe is an area in which pneumonic lesions are most frequently found associated with transport.2,18 Compared to other domestic species, the location of these lesions is unusual and the pathogenesis remains speculative. The location of pneumonic lesions reported in our review and the identification of multiple bacterial species in some horses supports the hypothesis that many cases of pneumonia in racehorses result from aspiration. This has been associated with the presence of intra-tracheal, bacteria-laden secretions at the thoracic inlet (“tracheal puddle”), which can be aspirated into the deep bronchi. 10
Most horses exhibited extensive fibrinous pleuritis, either unilateral or bilateral, which in many cases was associated with pneumonia (pleuropneumonia), in agreement with previous studies. 21 Pleuritis is a common complication of lung abscess or pneumonia, and is rarely recognized as a primary disease. 3 It can develop from direct spread from infected lung tissue or by blockage of pulmonary lymphatics by inflammatory debris, with subsequent leakage into the pleural cavity of lymphatic fluid contaminated by bacteria. 25 Most horses with pleuritis will survive if properly treated in the acute phase, and many can return to racing. If pleuropneumonia becomes chronic, successful resolution is more difficult. 3 Pleural effusion is usually bilateral because of the incomplete mediastinum present in most horses. 30 This was also the case in our study in which 70% of horses had bilateral pleuritis.
Regardless of the exact mechanism predisposing to bacterial colonization of the lower respiratory tract, a large influx of inflammatory cells leads to consolidation of the pulmonary parenchyma. In many cases, abscesses and areas of lytic necrosis are formed. In response to lung damage, sterile fluid fills the pleural space, but if the infection extends to the pleural surface, pleuropneumonia develops. 26 The presence of necrotizing pneumonia confers a poor prognosis to horses, and most of these animals are euthanized as a result of secondary complications, high cost of medical treatment, or poor prognosis for future performance.9,25
The most commonly isolated bacterium in this series was S. zooepidemicus (72%), followed by coliforms (22%), mixed bacterial flora (14%), and Actinobacillus spp. (14%), which is similar to results of other studies. 21 S. zooepidemicus was the most commonly isolated agent in cases of pleuropneumonia and bronchopneumonia, with or without intralesional abscesses and areas of lytic necrosis. S. zooepidemicus was the most commonly isolated bacteria in cases of pneumonia in racehorses in our series, and its presence was not associated with lesion distribution or the presence of abscesses and lytic necrosis of affected areas.
S. zooepidemicus is considered a mucosal commensal of the upper respiratory tract and is one of the most frequently isolated bacterial pathogens of horses.5,26 Compared to the closely related biovar Streptococcus equi ssp. equi (an obligate pathogen that causes strangles, an important equine specific respiratory disease), S. zooepidemicus has a much broader tissue tropism. 28 S. zooepidemicus is a non–host-adapted agent that is routinely isolated from wounds, arthritis, lymphadenitis, metritis, and from the lower respiratory tract of fetuses, foals, and adults.1,14,28
S. zooepidemicus possesses numerous virulence factors that facilitate infection and its survival in several tissues. Adherence molecules include fibronectin-binding proteins and the presence of a hyaluronic acid capsule.1,15 In addition, this bacterium is able to evade host defenses given the presence of immunoglobulin-binding protein and SzP protein.15,29 The antiphagocytic activity is conferred by the presence of hyaluronic acid, SzP, and M proteins. 28 Microbiologic and molecular analysis of S. zooepidemicus isolated from lungs with pneumonia confirmed that it is not a clonal, homogeneous population, but instead it can include a wide diversity of strains. This leads to potential difficulty for the development of a vaccine, and it is likely that the induction of heterologous, cross-protective immunity will be required.1,6 Studies have demonstrated that certain isolates of S. zooepidemicus are associated with outbreaks of upper respiratory disease in horses, and some strains of this presumed commensal may be more virulent than others. 16 In addition to respiratory diseases in horses, S. zooepidemicus is considered to be an emerging zoonotic agent, with demonstrated infectious potential for persons in contact with horses, causing meningitis, endocarditis, arthritis, abscesses, and sepsis. 19 This stresses the importance of correct etiologic identification and treatment of cases of pneumonia of racehorses.
The severe necrotizing lesions seen in horses with S. zooepidemicus pneumonia in our and previous studies are suggestive of protease release by S. zooepidemicus. 28 In addition, peptidoglycan is a potent activator of the alternative complement pathway, which makes it strongly chemotactic for equine neutrophils and causes fever, the latter because of the release of pyrogenic cytokines such as interleukin 6 and tumor necrosis factor from neutrophils. 28 Horses inoculated experimentally with S. zooepidemicus via an endoscope into the second branch of the principal right and left bronchi developed a heavy influx of neutrophils and macrophages as early as 2 h post-inoculation, formation of caseous necrotic foci 17 h post-inoculation, and the presence of extensive areas of necrosis and abscesses, plus fibrosis and purulent pleuritis 2 wk after the inoculation. 36 Most S. zooepidemicus cases in our study were chronic and likely did not respond to antimicrobial therapy.
In a low proportion of pneumonia cases (5%), anaerobic bacteria such as Peptoststreptococcus anaerobius and Clostridium spp. were isolated. Anaerobic bacterial flora is usually found when the estimated duration of illness is at least 5 d, and its presence is associated with decreased survival rate and poor prognosis.21,27
In our series of cases, Mycoplasma was isolated in only one case. The significance of Mycoplasma spp. (M. felis and M. equirhinis) in the development of pneumonia in racehorses has not been fully determined. 10 A few studies have associated M. felis with pleuritis and/or lower respiratory tract disease. This mycoplasma has been isolated alone or in combination with other bacteria.10,35 More studies are needed to understand the role of Mycoplasma spp. in the development of pneumonia in racehorses.
Numerous reports indicate that bacterial infections are more common than viral infections in racehorse pneumonia cases.8,12,17,33 Nevertheless, horses with a recent viral respiratory tract infection or exposure to other horses with viral infections have increased risk of developing pleuropneumonia.4,33 Alphaherpesvirus 1 and 4 are reported as the most important viral agents associated with respiratory disease in horses. 31 EHV-5, implicated in the pathogenesis of equine multinodular pulmonary fibrosis, can be associated with respiratory disease, but its virulence is low.31,32 In our study, only one case of interstitial pneumonia, suggestive of viral infection, was found. Although the etiology of this lesion could not be determined, changes were suggestive of EHV-5 infection. Viral testing was not performed in any of the cases, and viral involvement therefore cannot be excluded. No fungi or parasites, or lesions suggestive of these organisms, were seen in any of the horses included in our study.
Footnotes
Acknowledgements
We thank Mrs. Sue Ellen Uzal for the correction of this manuscript, and Dr. Mauricio Navarro for comments about statistical procedures.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.