
Abstract
We tested the hypothesis that indirect measures of oxidative stress (vitamin E, glutathione peroxidase, and malondialdehyde) differ in dogs in heart failure resulting from either myxomatous mitral valve disease or dilated cardiomyopathy. Dogs were classified according to the International Small Animal Cardiac Health Council (ISACHC) classification. Additionally, the effect of cardiac therapy on oxidative stress parameters and N-terminal pro–B-type natriuretic peptide (NT-proBNP) in advanced stages of congestive heart failure was investigated. There were no significant differences in oxidative stress parameters between healthy dogs and the individual groups of cardiac patients. Significantly lower malondialdehyde (MDA) was observed in the ISACHC II group in comparison to ISACHC groups III and I. A significant positive correlation in treated patients was observed between NT-proBNP and MDA, NT-proBNP and vitamin E, as well as between MDA and vitamin E (and lipid-standardized vitamin E). No significant differences in any of the measured parameters were found between treated and non-treated cardiac patients. Our results suggest an association between MDA (the extent of lipid peroxidation) and NT-proBNP, vitamin E and NT-proBNP, as well as between MDA and vitamin E in treated canine patients. Plasma vitamin E concentration was maintained in all stages of cardiovascular disease in these canine patients.
Introduction
Oxidative stress in a living organism is primarily the result of increased production of reactive oxygen species (ROS) and reactive nitrogen species (RNS) that dominate over endogenous enzymes, such as glutathione peroxidase (GPX) and superoxide dismutase (SOD), and exogenous antioxidant defense mechanisms (vitamins A, E, and C, polyphenols, carotenoids). In heart failure, excess ROS and RNS are produced by the respiratory chain in mitochondria, vascular nicotinamide dinucleotide (phosphate) oxidases, cytochrome P450, xanthine oxidases, auto-oxidation of catecholamines, or nitric oxide synthase activation.14,20,35 ROS-induced cellular injury has been involved in the development of many cardiovascular diseases, including myocardial infarction, coronary artery disease, dilated cardiomyopathy (DCM), congestive heart failure (CHF), and other cardiac diseases in people and animals.2,11,12,14,17,20,24,27,37,49 Besides their cytotoxic effect on myocardial cells, ROS also act as negative inotropes. 14
ROS and RNS are highly reactive, short-lived, and, as such, cannot be practically and directly measured in human and animal in vivo studies. 33 A growing body of evidence suggests that many of the damaging effects of ROS and RNS on the cells of the cardiovascular system are mediated by products of non-enzymatic reactions such as lipid peroxidation, glycation, and amino acid oxidation. 14 Malondialdehyde (MDA), a final product of lipid peroxidation, is the most commonly measured biomarker of oxidative stress 45 and is significantly elevated in the blood in heart failure in humans and dogs.3,7,11,20,23,31,37,49
Vitamin E or α-tocopherol is the main and most potent lipid-soluble antioxidant. It is only synthesized by plants and cyanobacteria and is essential in human and animal nutrition. 36 Vitamin E is one of the most powerful free-radical scavengers, particularly in cell membranes. 25 Vitamin E inhibits lipid peroxidation and hence provides enhanced stability to the cellular membrane. 19 Fat-soluble vitamin E does not have a specific carrier in plasma; it occurs in all plasma lipoproteins. Standardization of vitamin E to lipids enables accurate assessment of serum or plasma vitamin E status.16,41,48 Vitamin E adjustment for the sum of cholesterol and triglycerides reduces the influence of concurrent lipids present in plasma and is highly effective in identifying vitamin E deficiency.16,41 A few studies have shown decreased plasma vitamin E concentrations in human patients with heart failure26,31,32,37 and in dogs with CHF resulting from DCM and myxomatous mitral valve disease (MVD). 12 However, there is also evidence of normal levels of vitamin E in human patients with heart failure5,18 (DCM, post-ischemic cardiomyopathy) and in canine patients with DCM10,11 and MVD (Reimann MJ, et al. Low-density lipoprotein oxidation is breed and gender dependent in dogs with myxomatous mitral valve disease. Proc Am Coll Vet Intern Med Forum 2016; June 2016; Denver, CO).
Glutathione peroxidase (GPX), superoxide dismutase (SOD), and catalase (CAT) represent the primary intracellular enzymatic antioxidant defense against oxidative stress. 22 Clinical trials have shown that human patients who suffer from heart failure have significantly decreased blood levels of GPX.18,23,32 In contrast, clinical studies on dogs with DCM showed significantly increased GPX activity.10,11 Erythrocyte SOD activity was found significantly lower in human chronic heart failure patients than in controls. 24 On the other hand, erythrocyte SOD activity did not differ significantly between dogs with DCM and control dogs.10,11 We found no information about blood catalase activity in human and canine CHF patients.
B-type natriuretic peptide (BNP) is produced primarily within the heart and released into the circulation in response to increased ventricular wall tension. 38 Studies in humans and dogs have shown that heart failure increases the level of N-terminal pro–B-type natriuretic peptide (NT-proBNP) in the blood, which represents a biomarker of the progression of heart failure.3,6,29,38,46
We tested the hypothesis that indirect measures of oxidative stress (vitamin E, GPX, and MDA) differ among different classes of heart failure in dogs with MVD and DCM. Additionally, we investigated the effect of cardiac therapy on oxidative stress parameters and NT-proBNP in advanced stages of heart failure (International Small Animal Cardiac Health Council, ISACHC II and III). We were also interested in determining whether there is an association (correlation) between disease severity (as measured by NT-proBNP levels) and indirect measures of oxidative stress, as well as between MDA and antioxidants (vitamin E, GPX), in different stages of cardiovascular diseases and in groups of cardiac patients with and without therapy.
Materials and methods
Dogs
Client-owned dogs (n = 47) were used in this study: 37 dogs with confirmed cardiovascular disease and 10 healthy dogs. Dogs were judged to be healthy based on their history, a clinical examination including auscultation, the results of hematologic and biochemical analyses, and NT-proBNP levels. A diagnosis of cardiovascular disease and heart failure was confirmed by clinical examination; electrocardiography; 2-D, M-mode, and Doppler echocardiography (Vingmed System Five, General Electric Healthcare, Milwaukee, WI); and thoracic radiography by one experienced examiner (A Domanjko Petrič). Diagnoses of diseases were in accordance with European and American Colleges of Veterinary Internal Medicine guidelines.1,8 Criteria for the diagnosis of CHF were based on clinical signs and radiographic examination. An interstitial or alveolar pulmonary pattern compatible with pulmonary edema with left atrial enlargement and clinical signs of CHF were used to confirm CHF. Hematologic and biochemical analyses were performed (data not shown); dogs with concurrent diseases were excluded from the study. Disease severity was classified with the ISACHC classification for cardiac disease. 9 According to this classification, patients were classified as asymptomatic (ISACHC I), mild-to-moderate heart failure (ISACHC II), or advanced heart failure (ISACHC III) group. The owners of healthy dogs and cardiac patients completed a questionnaire regarding their dogs’ diet, intake of food supplements, treats, and medications. According to owners’ answers, the dogs were fed commercial and/or homemade food (Table 1), and none of the dogs were given food supplements.
Diet of dogs included in the oxidative stress study.*
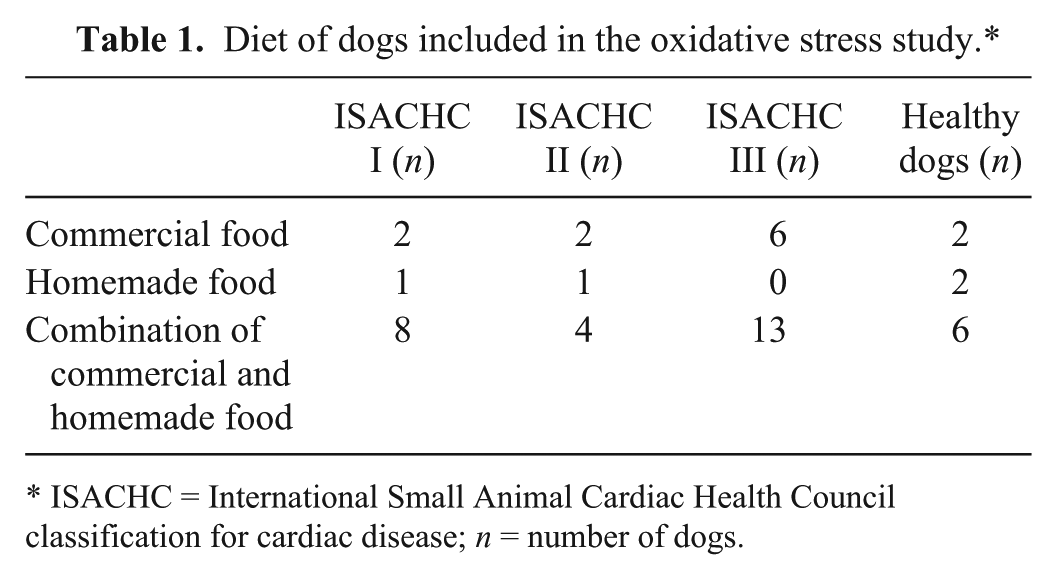
ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; n = number of dogs.
Written consent of the owners was obtained. All procedures were approved by the Ethical Committee of the Ministry of Agriculture, Forestry and Food, Veterinary Administration of the Republic of Slovenia (Animal Protection Act UL RS 43/2007).
Blood sampling and processing
Dogs were fasted at least 12 h, and blood samples were collected from all groups from the jugular or cephalic vein. Blood samples for determining plasma concentrations of NT-proBNP and MDA were collected into tubes containing the anticoagulant EDTA (Vacuette, Greiner Bio-One, Kremsmunster, Austria). Samples were centrifuged immediately after collection (1,500 × g, 15 min, 4°C). Blood samples for determination of plasma vitamin E and whole blood GPX were collected into tubes containing the anticoagulant lithium heparin (Vacuette, Greiner Bio-One). Samples were centrifuged immediately after collection (1,500 × g, 15 min, 4°C). Plasma was separated and immediately frozen at −80°C until analyzed. Aliquots of heparinized whole blood were prepared and immediately frozen at −80°C until analyzed. All measured parameters were analyzed in batch by blinded analysts.
Determination of vitamin E in blood plasma
The procedure was based on analytical methods described elsewhere39,50; 0.5 mL of plasma was placed in glass tubes and mixed with 1 mL of ethanol; 3 mL of n-hexane was added to the mixture and vortexed for 10 s. After the layers separated, 2 mL of the hexane phase was evaporated to dryness under vacuum (Syncore Reactor R-48, Büchi, Flawil, Switzerland) at ~60°C. The dry residue was re-dissolved in 0.5 mL of methanol, and the concentration of vitamin E was determined by high-performance liquid chromatography (HPLC) with fluorescence detection, using an external standard of α-tocopherol (Sigma-Aldrich, St. Louis, MO). The HPLC system (Waters, Milford, MA) was equipped with a C18 column, 10 μm, 3.9 × 300 mm, a fluorescence detector (Waters), and a computer with the Millennium program for system control and data processing. Methanol at a flow rate of 2 mL/min was used as the mobile phase. The injection volume was 20 μL. The column was kept at ambient temperature, and detection was carried out at an excitation wavelength of 295 nm and emission wavelength of 330 nm. Lipid-standardized vitamin E (LS-VE) was calculated as the ratio between concentrations of plasma vitamin E (µmol/L) and the sum of concentrations of serum total cholesterol (mmol/L) and serum triglycerides (mmol/L).41,48
Determination of GPX activity in whole blood
GPX activity was measured spectrophotometrically with an automated biochemistry analyzer (Randox, Crumlin, Great Britain) using a commercial kit (Ransel, Randox), based on a method described elsewhere. 30 GPX activity is determined indirectly by measuring the rate of formation of oxidized glutathione (GSSG). GPX catalyzes the reaction of glutathione with synthetic cumene hydroperoxide to GSSG. In the presence of NADPH and glutathione reductase, GSSG is transformed to glutathione, and NADPH is oxidized to NADP. The rate of oxidation of NADPH was measured spectrophotometrically as reduced absorbance at 340 nm and is proportional to the activity of GPX in the specimen. GPX activity was expressed as units/g of hemoglobin (U/g Hb). Hemoglobin concentration in the whole blood hemolysates was determined spectrophotometrically by the cyano-methemoglobin method using an automated biochemistry analyzer (Randox).
Determination of MDA concentration in plasma samples
The MDA concentration in the plasma samples was analyzed as described elsewhere. 34 MDA was derivatized with thiobarbituric acid (TBA). Two hundred µL of plasma, 20 µL of 0.2% butylated hydroxytoluene (BHT), and 200 µL of 0.44 M H3PO4 were added into a 2-mL plastic microcentrifuge tube, mixed, and left for 15 min. Absolute ethanol (600 µL) was added to each sample, and samples were centrifuged (15,000 × g, 15 min, 4°C). In the glass tubes, 1.5 mL of 0.44 M H3PO4, 700 µL of centrifuged samples, 1.5 mL of 0.6% TBA, and 0.3 mL of ultrapure water were mixed and heated at 90°C for 60 min. The MDA-TBA2 adduct was separated by an HPLC system (Waters) equipped with an ODS chromatographic column (C18, 120 A, 4.6 × 150 mm, 5 μm; Phenomenex HyperClone, Torrance, CA) and a fluorescence detector (Waters). The mobile phase consisted of 50 mmol/L of a 65% KH2PO4 buffer (pH 6.9) and 35% methanol; flow rate of the mobile phase was 1.0 mL/min. The instrument was calibrated using tetraethoxypropane as the external standard.
Determination of NT-proBNP
Plasma samples for determination of NT-proBNP concentrations were sent to IDEXX Laboratories (Westbrook, ME) and analyzed by ELISA. 4
Statistical analysis
The data were analyzed with commercial software (SPSS 22.0, Chicago, IL). Descriptive statistics were used to describe the basic features of the data. The Shapiro–Wilk test was performed to test whether the data were normally distributed. A one-way analysis of variance with Tukey HSD post-hoc test in the case of normal distribution of the data (MDA, GPX, age), or Kruskal–Wallis analysis followed by the Mann–Whitney U test with Bonferroni adjustment in the case of non-normal distributed data (vitamin E, LS-VE, NT-proBNP), were used to test for statistically significant differences in the measured parameters between groups of cardiac patients (ISACHC I–III) and the group of healthy dogs. An independent t-test in the case of normal distribution of the data (vitamin E, LS-VE, GPX, MDA, age), and the Mann–Whitney U test in the case of non-normal distributed data (NT-proBNP, weight), were performed to test for statistically significant differences in the measured parameters (including age) between cardiac patients with and without therapy (ISACHC II+III), between DCM and MVD patients (ISACHC III) as well as between all cardiac patients and control group dogs (age, weight). The data that were normally distributed are presented as means ± standard deviations (SDs); the data not normally distributed are presented as median, minimum, and maximum values. According to the results of the normality tests, a Spearman rank correlation coefficient analysis or a Pearson correlation coefficient analysis was performed to determine the correlation between disease severity (NT-proBNP) and oxidative stress parameters (vitamin E, LS-VE, GPX, and MDA), and between MDA and antioxidants (GPX, vitamin E, LS-VE), respectively, in different stages of cardiovascular diseases and in groups of cardiac patients with and without therapy. A value of p < 0.05 was considered significant.
Results
Dogs
Thirty-seven patients with confirmed cardiovascular disease (Table 2) were included in the study (6 Doberman Pinschers, 5 mixed-breed dogs, 5 Great Danes, 4 Cavalier King Charles Spaniels, 4 German Boxers, 2 Airedale Terriers, 2 Shi-Tzus, 2 Whippets, 1 Dalmatian, 1 Schipperke, 1 Irish Wolfhound, 1 Dachshund, 1 Cirneco dell’Etna, 1 Hovawart, 1 Pekingese). Among all cardiac patients were 6 females and 31 males (mean age 8.8 ± 2.8 y, mean weight 31.1 ± 21.5 kg). Ten healthy dogs were enrolled as controls in the study (2 Border Collies, 2 Labrador Retrievers, 1 Hovawart, 1 Rough Collie, 1 Irish Wolfhound, 1 mixed-breed, 1 White Swiss Shepherd Dog, 1 Afghan Hound; 7 females, 3 males, mean age 4.4 ± 2.5 y, mean weight 28.1 ± 9.1 kg). The ISACHC I group consisted of 11 dogs (2 females, 9 males, mean age 9.3 ± 3.6 y, mean weight 35.4 ± 24.7 kg), the ISACHC II group consisted of 7 dogs (7 males, mean age 10.6 ± 1.5 y, mean weight 17.7 ± 12.0 kg), and the ISACHC III group consisted of 19 dogs (4 females, 15 males, mean age 7.9 ± 2.4 y, mean weight 33.5 ± 21.2 kg).
Cardiovascular diseases of dogs included in the study.*
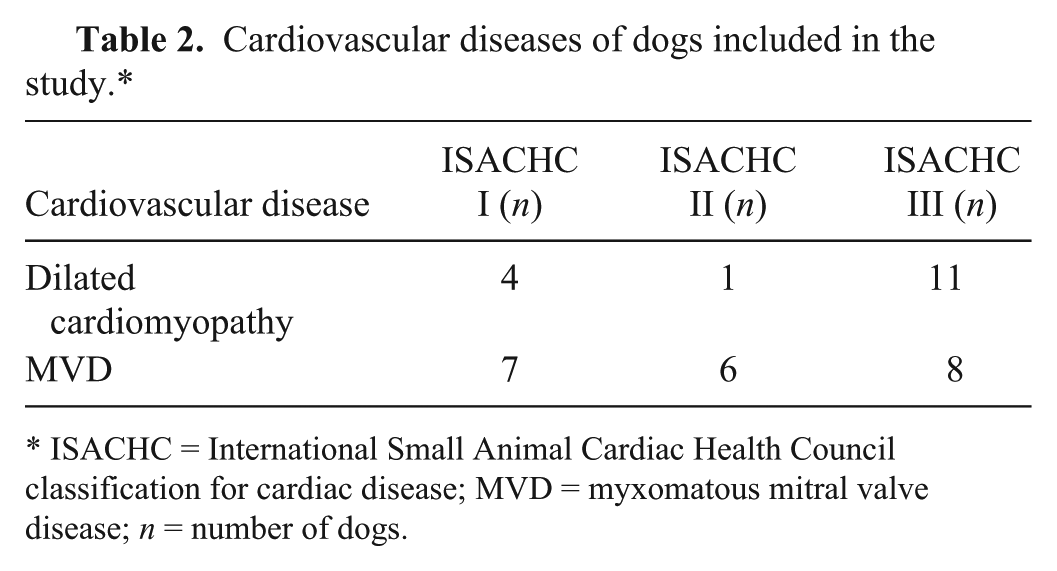
ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; MVD = myxomatous mitral valve disease; n = number of dogs.
The dogs in the ISACHC II and III groups were combined and then subdivided into a group already receiving cardiac therapy at the time of presentation (13 dogs; 2 females, 11 males, mean age 9.4 ± 2.8 y, mean weight 24.6 ± 22.8 kg) and into a group receiving no cardiac therapy (13 dogs; 2 females, 11 males, mean age 7.9 ± 1.9 y, mean weight 33.9 ± 17.0 kg). In the ISACHC II group, 6 of 7 patients were receiving cardiac therapy, and 1 had not been treated at the time of blood sampling. In the ISACHC III group, 7 of 19 dogs were receiving cardiac therapy; the other dogs in this group had not been treated with cardiac medication at the time of blood sampling. Medication regimens included diuretics (furosemide and spironolactone), beta-blockers (atenolol and sotalol), ACE inhibitors, an inodilator (pimobendan), and digoxin (Table 3). The ISACHC III group was further divided into DCM (11 dogs; 1 female, 10 males; mean age 6.8 ± 1.8 y, mean weight 44.0 ± 21.1 kg) and MVD (8 dogs; 3 females, 5 males; mean age 9.5 ± 2.4 y, mean weight 19.0 ± 10.4 kg) patients. There was no significant difference in weight between control group dogs and all cardiac patients; however, control dogs were significantly younger in comparison to all cardiac patients (p = 0.000) and all ISACHC groups (p = 0.001, p = 0.000, p = 0.007, respectively to ISACHC I–III). Dogs in the individual ISACHC groups did not differ significantly in age. Additionally, there was no significant difference in age between dogs with and without therapy (p = 0.109). MVD dogs were significantly older (p = 0.013) and lighter (p = 0.007) than DCM dogs.
Treatment used in dogs included in the International Small Animal Cardiac Health Council (ISACHC) II and III groups.*
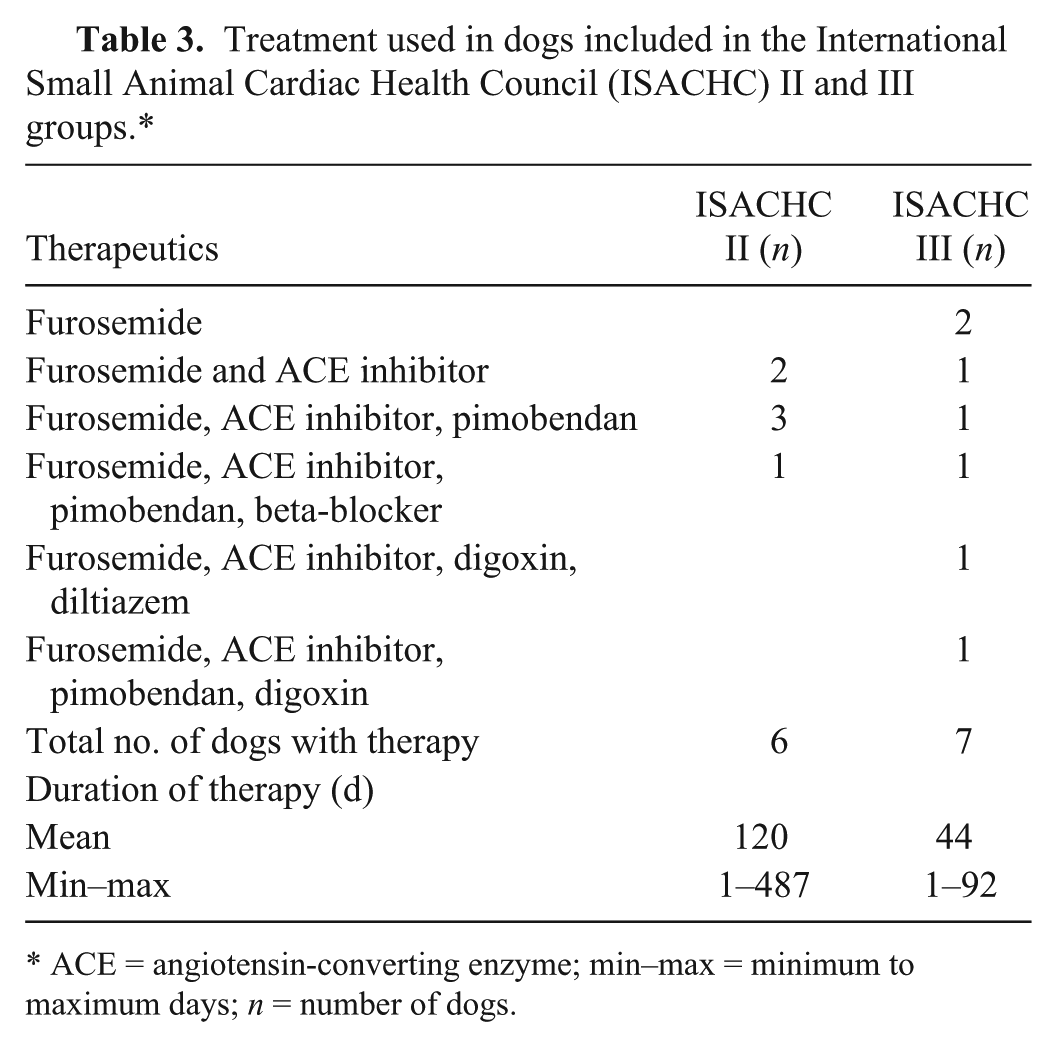
ACE = angiotensin-converting enzyme; min–max = minimum to maximum days; n = number of dogs.
Oxidative stress parameters and NT-proBNP in cardiac patients and healthy dogs
Statistical analysis did not show any significant differences in the activity of GPX (Table 4), vitamin E (Table 4), and LS-VE (Table 4) between controls and individual ISACHC groups or between ISACHC groups. MDA concentration (Table 4) did not differ significantly between controls and individual ISACHC groups. However, MDA concentration (Table 4) in the ISACHC II group was significantly lower in comparison to the ISACHC I (p = 0.004) and ISACHC III (p = 0.017) groups. NT-proBNP concentrations were significantly higher in ISACHC III (median value: 5,173 pmol/L, minimum–maximum values: 2,047–18,631 pmol/L) in comparison to ISACHC II (median value: 2,569 pmol/L, min–max values: 1,340–8,238 pmol/L; p = 0.006) and ISACHC I (median value: 1,207 pmol/L, min–max values: 820–12,056 pmol/L; p = 0.000). NT-proBNP concentrations in control dogs (median value: 822 pmol/L, min–max values: 407–1,331 pmol/L) were significantly lower compared to ISACHC II (p = 0.001) and ISACHC III (p = 0.000), but not to ISACHC I (p = 0.017).
Glutathione peroxidase (GPX), malondialdehyde (MDA), vitamin E, and lipid standardized vitamin E (LS-VE) in cardiac patients and healthy dogs.*
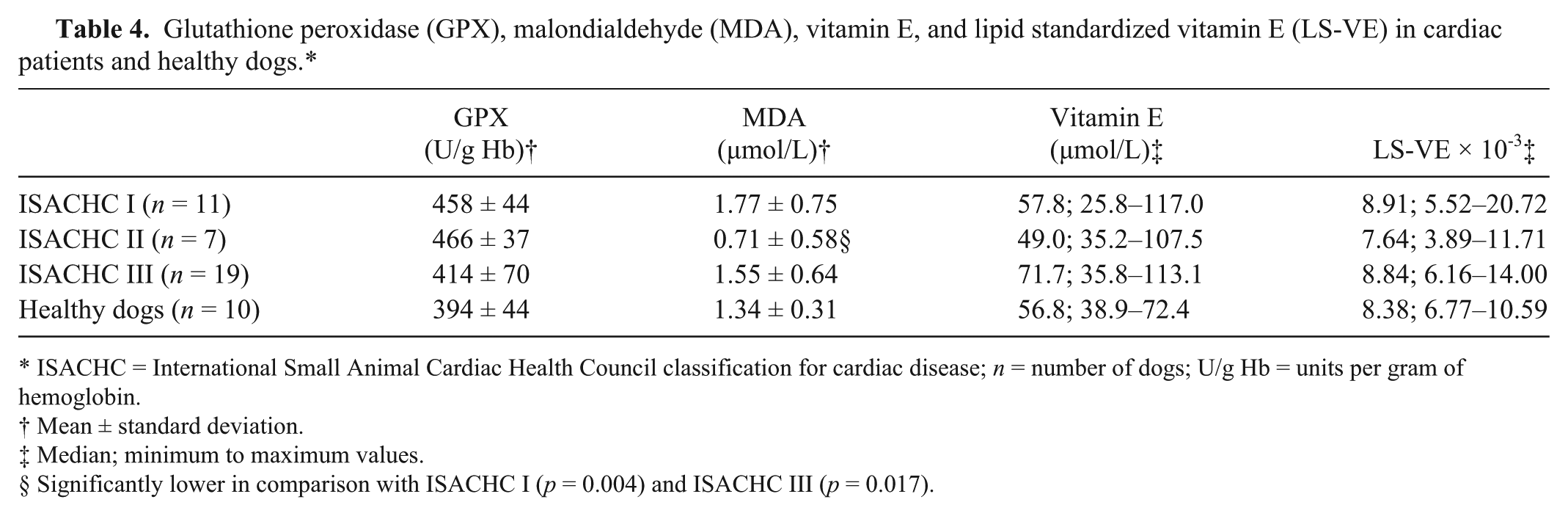
ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; n = number of dogs; U/g Hb = units per gram of hemoglobin.
Mean ± standard deviation.
Median; minimum to maximum values.
Significantly lower in comparison with ISACHC I (p = 0.004) and ISACHC III (p = 0.017).
Statistical comparison between DCM and MVD patients in the ISACHC III group showed no significant differences in MDA, vitamin E, LS-VE, and NT-proBNP; however, GPX activity was significantly higher in MVD dogs than in DCM dogs (p = 0.004; Table 5).
Oxidative stress parameters in canine myxomatous mitral valve disease (MVD) and dilated cardiomyopathy (DCM) patients (ISACHC III).*
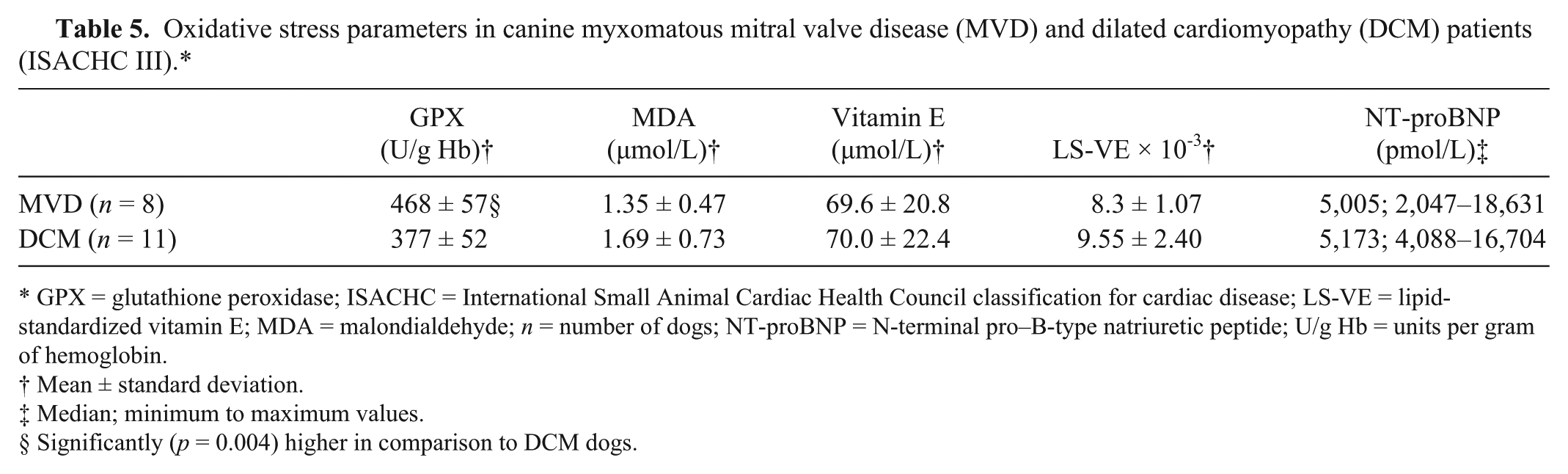
GPX = glutathione peroxidase; ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; LS-VE = lipid-standardized vitamin E; MDA = malondialdehyde; n = number of dogs; NT-proBNP = N-terminal pro–B-type natriuretic peptide; U/g Hb = units per gram of hemoglobin.
Mean ± standard deviation.
Median; minimum to maximum values.
Significantly (p = 0.004) higher in comparison to DCM dogs.
The effect of cardiac therapy
Statistical analysis did not show significant differences in the measured parameters (MDA, GPX, vitamin E, LS-VE) and age between patients receiving cardiac therapy and those without therapy (Table 6). The median value of NT-proBNP in non-treated dogs (4,876 pmol/L, min–max values: 2,047–16,704 pmol/L) was not significantly different from the treated dogs (3,346 pmol/L, min–max values: 1,340–18,631 pmol/L).
Oxidative stress parameters (mean ± standard deviation) in canine cardiac patients with and without therapy (ISACHC II and III).*
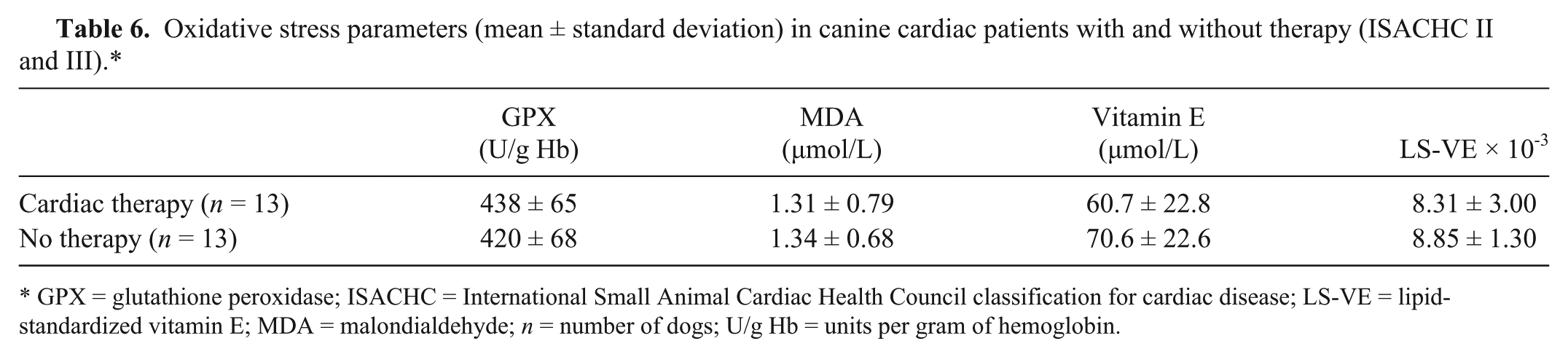
GPX = glutathione peroxidase; ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; LS-VE = lipid-standardized vitamin E; MDA = malondialdehyde; n = number of dogs; U/g Hb = units per gram of hemoglobin.
Correlations
There were no significant correlations between NT-proBNP and oxidative stress parameters in any of the ISACHC groups. In treated cardiac patients, NT-proBNP showed significant correlation with vitamin E (Fig. 1; r = 0.566, p = 0.044) and MDA (Fig. 2; r = 0.637, p = 0.019). In addition, significant positive correlation was observed between MDA and vitamin E (Fig. 3; r = 0.605; p = 0.028) and LS-VE (Fig. 4; r = 0.697; p = 0.008) in treated patients. Correlations between NT-proBNP and GPX (r = −0.573, p = 0.051) and LS-VE (r = 0.549, p = 0.052) were not significant in treated patients. No significant correlations between measured parameters were observed in non-treated patients.
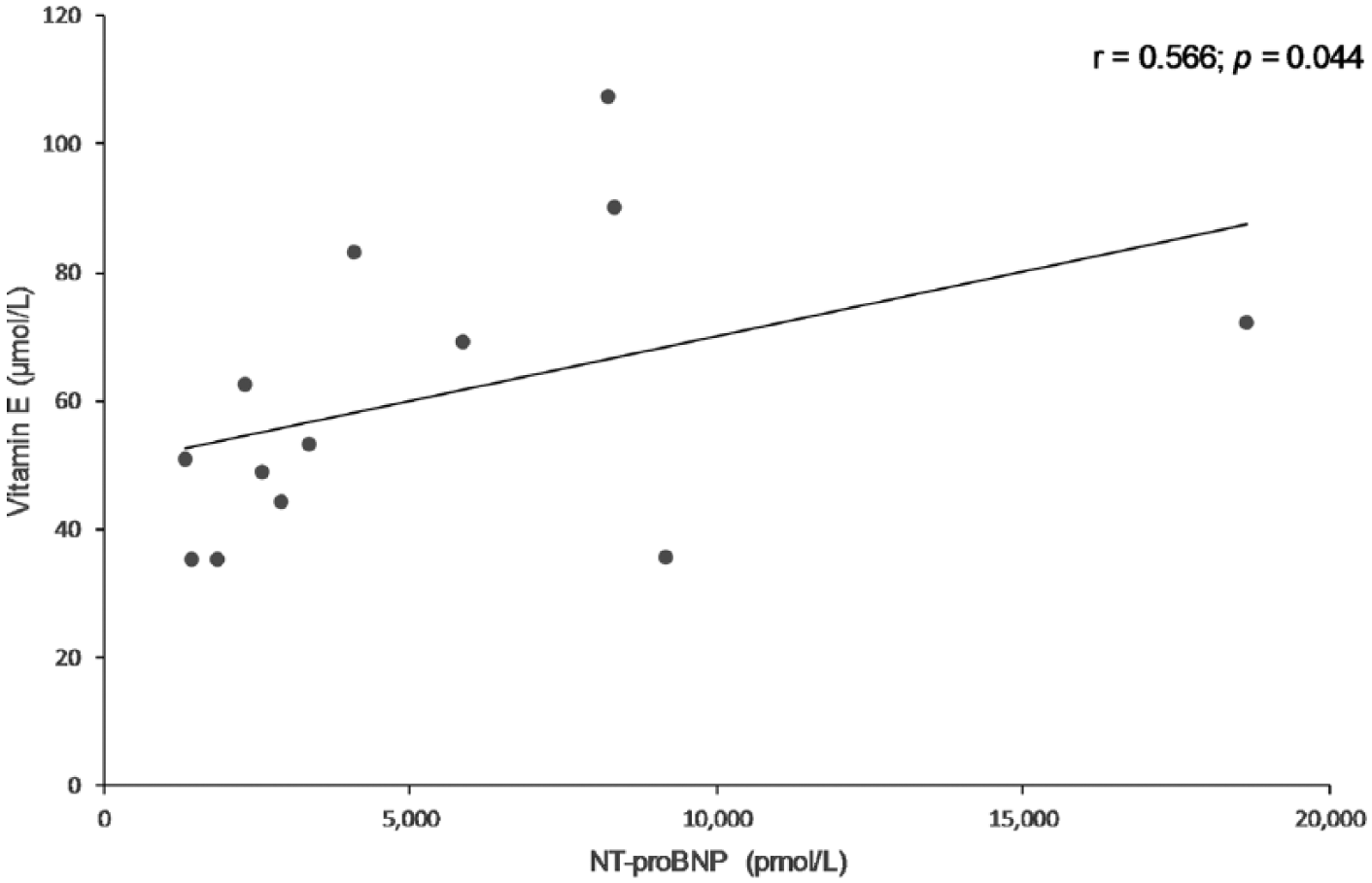
Scatter plot showing a significant positive correlation between plasma vitamin E and N-terminal pro–B-type natriuretic peptide (NT-proBNP) concentrations in cardiac patients with therapy (ISACHC II and III, 13 dogs). ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; r = Spearman correlation coefficient.
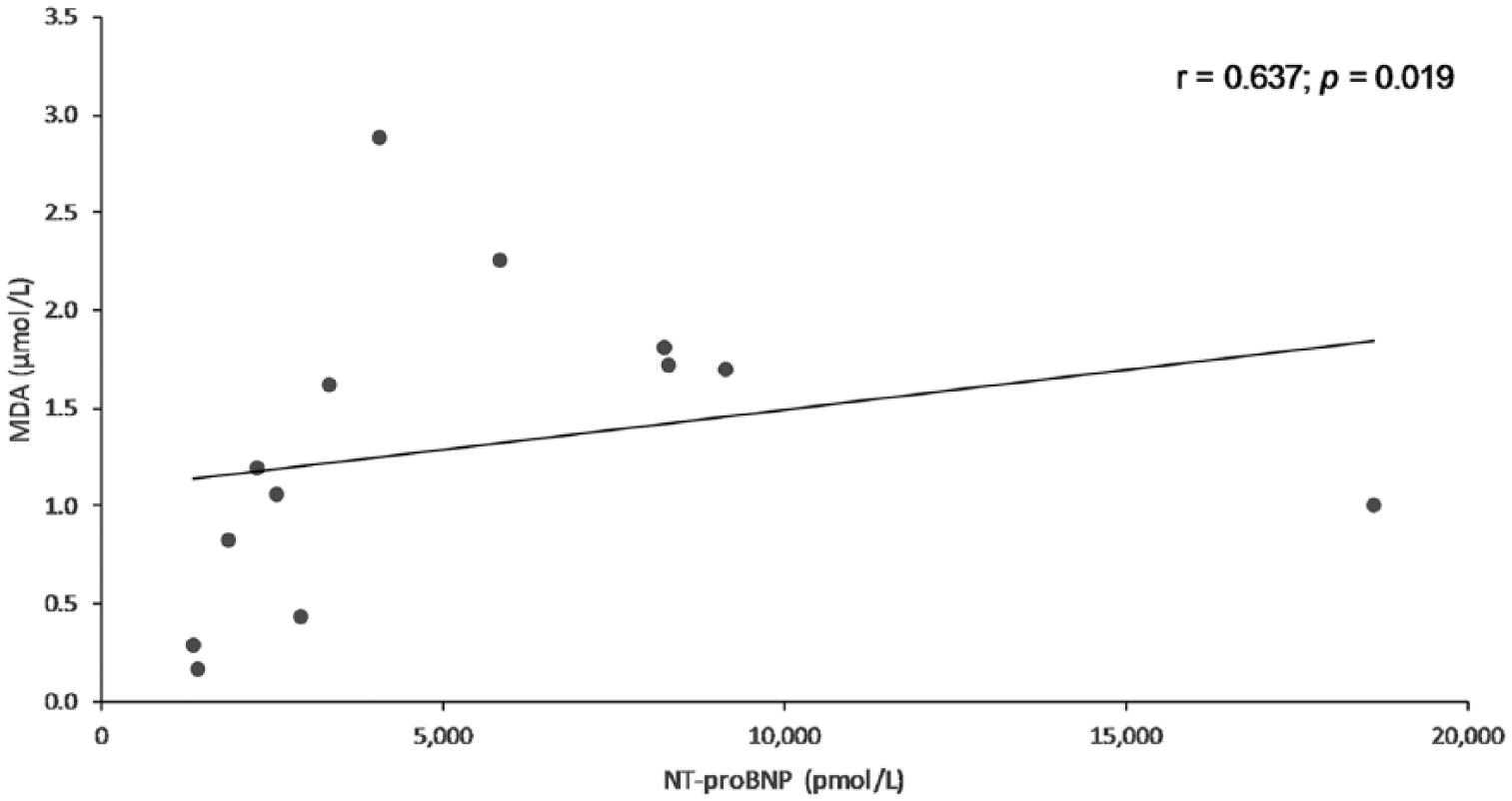
Scatter plot showing a significant positive correlation between plasma malondialdehyde (MDA) and N-terminal pro–B-type natriuretic peptide (NT-proBNP) concentrations in cardiac patients with therapy (ISACHC II and III, 13 dogs). ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; r = Spearman correlation coefficient.
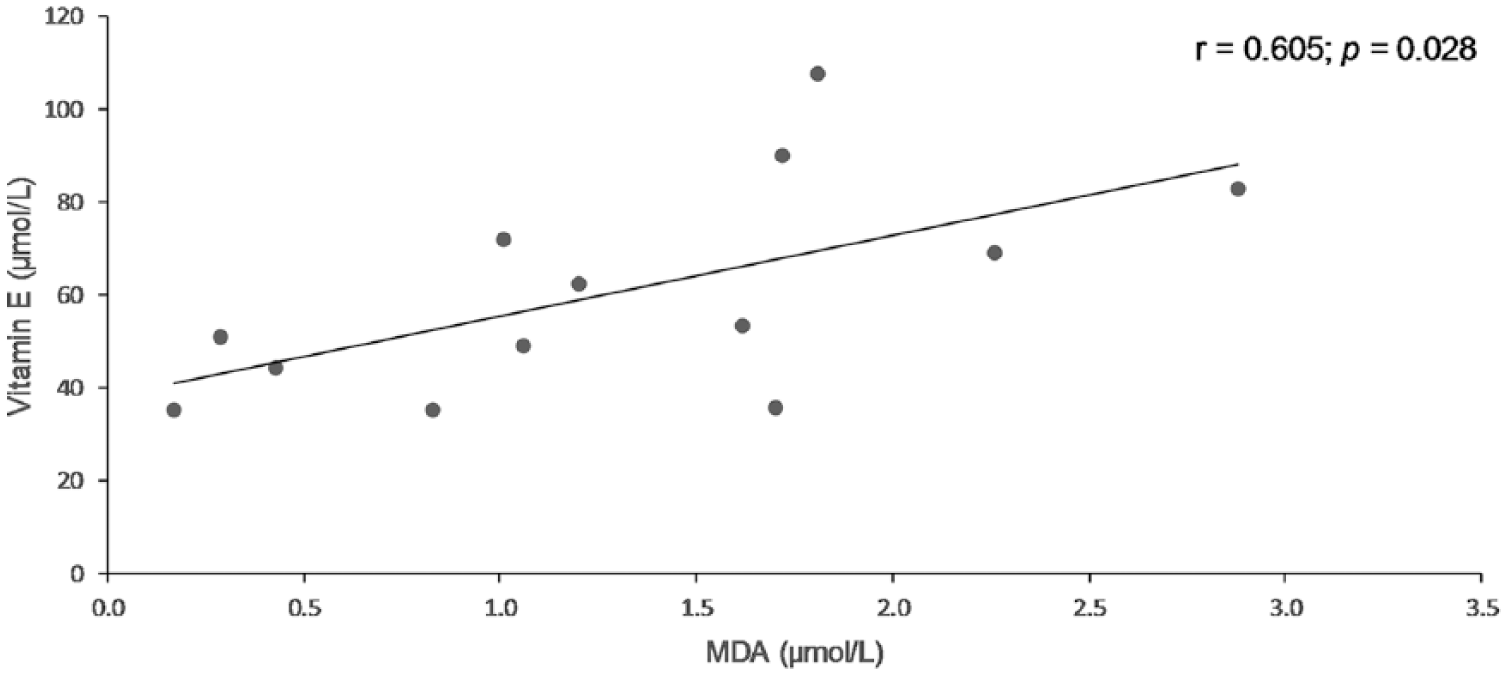
Scatter plot showing a significant positive correlation between plasma vitamin E and malondialdehyde (MDA) concentrations in cardiac patients with therapy (ISACHC II and III, 13 dogs). ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; r = Pearson correlation coefficient.
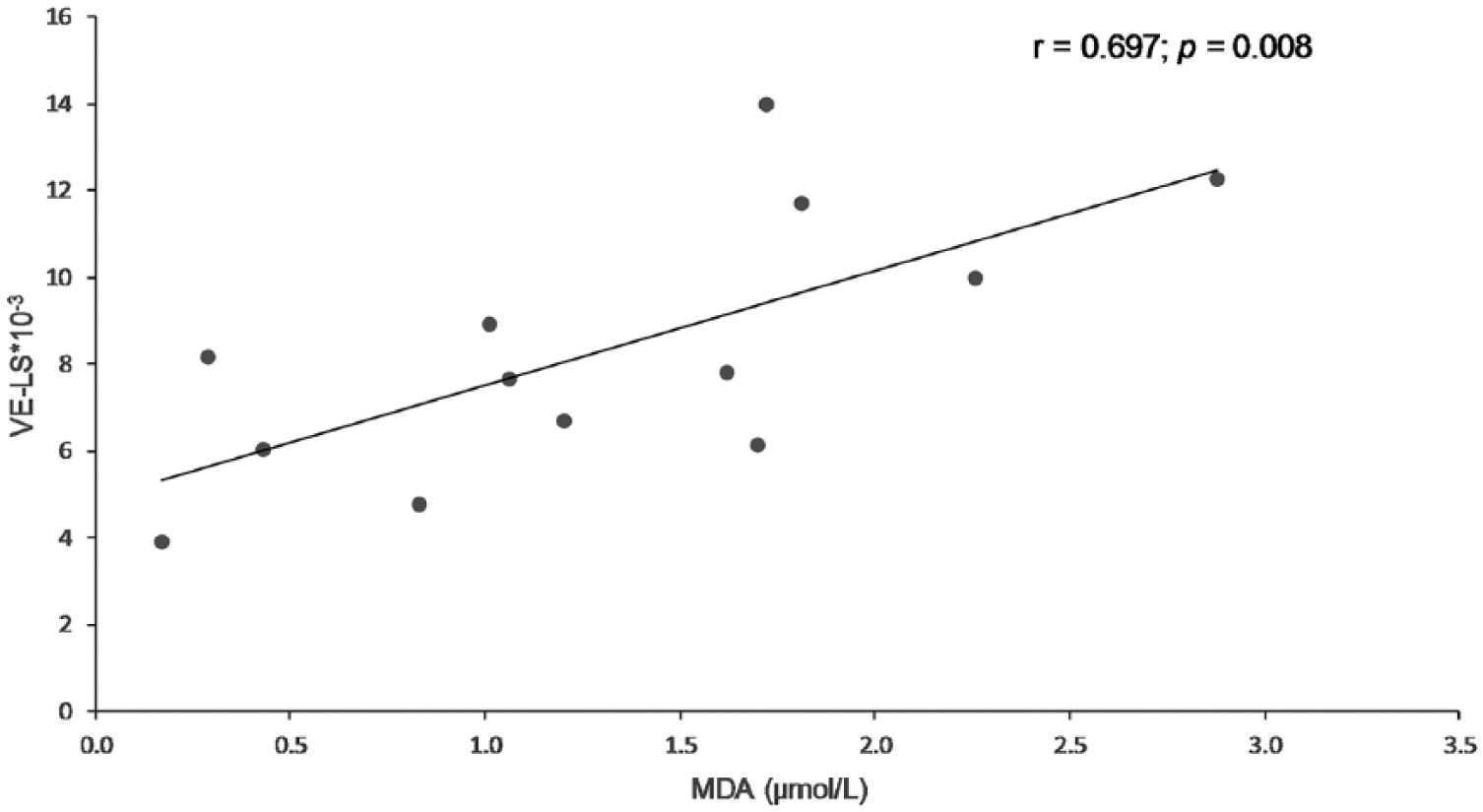
Scatter plot showing a significant positive correlation between plasma lipid-standardized vitamin E (LS-VE) and malondialdehyde (MDA) concentrations in cardiac patients with therapy (ISACHC II and III, 13 dogs). ISACHC = International Small Animal Cardiac Health Council classification for cardiac disease; r = Pearson correlation coefficient.
Discussion
Results of our study showed no significant differences of measured oxidative stress parameters between ISACHC groups or in comparison with the control group. The lack of significant differences in GPX activity between control dogs and individual groups of cardiac patients, or between ISACHC groups, is in contrast to results from human studies that reported significantly decreased GPX activity in CHF patients.18,23,32 However, we found significantly higher GPX activity in MVD patients compared to DCM patients in the ISACHC III group. This might be ascribed to the effect of age, given that the MVD patients were significantly older than the DCM patients, or to disease etiology. A significant increase of whole blood GPX with aging was reported in Labrador Retrievers. 40 A recent study in healthy dogs reports a tendency of higher GPX activity in geriatric dogs. 43
MDA concentrations did not differ significantly between controls and individual ISACHC groups; however, significantly lower MDA concentrations were found in the ISACHC II group compared to the ISACHC I and ISACHC III groups. The latter might be the result of stochastic chance and may not be of biological significance. Several studies have demonstrated elevated plasma concentrations of MDA in human patients with CHF.2,7,20,31,37,49 It has also been shown that MDA increased with the stage of heart failure (New York Heart Association [NYHA] I or II to NYHA III or IV) in human patients.31,37 In contrast, in 2 canine studies, no significant difference in plasma MDA concentration was found between canine DCM patients 11 and controls and between CHF patients (MVD and DCM) 12 and controls. Additionally, plasma MDA concentration did not correlate to disease severity in DCM 11 and MVD patients 12 (Reimann MJ, et al. Low-density lipoprotein oxidation).
Cardiovascular drugs, such as beta-blockers, ACE inhibitors, and calcium channel blockers, have been shown to have antioxidant properties.15,21,27,28,47 Some of these drugs were shown to limit the extent of lipid peroxidation, which resulted in lower MDA concentrations.27,28,47 We expected lower plasma MDA concentrations in treated patients; however, no significant difference in MDA concentrations was found between treated and non-treated patients.
We found no significant differences in vitamin E and LS-VE between control dogs and individual groups of cardiac patients, or between ISACHC groups. Contrary to our results, significantly lower vitamin E concentrations have been found in dogs with CHF (DCM and MVD) in comparison to control dogs. 12 Moreover, in that study, 12 no significant difference was observed in vitamin E concentration between MVD and DCM patients, which is in accordance with the results of our study. An inverse correlation between plasma vitamin E and LS-VE and mortality resulting from ischemic heart disease has been demonstrated in human patients. 13 Although some human studies31,32,37 have shown decreased levels of vitamin E concentration, which decreased with severity of heart failure, other human studies5,18 and studies in canine patients10,11 (Reimann MJ, et al. Low-density lipoprotein oxidation) have shown no changes in vitamin E concentration in CHF.
In our study, significantly higher plasma NT-proBNP concentration was determined in the ISACHC III group in comparison to ISACHC II and ISACHC I. We observed a significant positive correlation in treated patients (ISACHC II and III) between NT-proBNP and MDA, which suggests an association between MDA and NT-proBNP. In human patients, MDA levels correlated significantly positively with heart failure class. 37 The lack of significant correlation between NT-proBNP and MDA in untreated patients might lie in the fact that this group consisted of all but one ISACHC II patient, whereas NT-proBNP concentration was more consistent in comparison with the group of treated patients. In our study, NT-proBNP also significantly positively correlated with vitamin E in treated patients. Moreover, we observed significant positive correlations between MDA and vitamin E and between MDA and LS-VE in treated patients. These results suggest that vitamin E concentration and LS-VE values increase with the extent of lipid peroxidation and with the increase of NT-proBNP in treated canine patients. It is possible that treatment might affect vitamin E homeostasis and MDA levels or that this is the result of wider variation of NT-proBNP in the treated group as mentioned above. Our results are in contrast to those of another study 11 in which a significant negative correlation between disease severity and plasma vitamin E concentration was found in a group of canine cardiac patients (DCM). 11 The difference between our study and the published study 11 might be attributed to differences in dogs included in the study and the use of different classification systems. DCM dogs with and without CHF were included in the published study, 11 and classified according to the modified NYHA classification.
Our study has several limitations. These include no age and sex match between the control group and the 3 groups of cardiac patients; no information regarding reproductive status; as well as the inclusion of 2 different diseases (MVD, DCM). An additional limitation might be that the healthy controls had no echocardiographic examination done. We cannot completely exclude the effect of age and/or sex on the measured parameters. There are only a few reports on the effect of age and/or sex on antioxidant enzyme activity,40,43,44 MDA, 42 and vitamin E 40 in dogs. In addition, the effect of diet on our results cannot be excluded. No detectable differences in several oxidative stress parameters (vitamins E and C, antioxidant capacity, retinol, MDA, 8-F2α-isoprostane, protein carbonyls, reduced and oxidized glutathione) were found between dogs eating antioxidant-enriched diets compared to other diets. 12 According to owners’ answers, the dogs in our study were fed random diets (home-made or commercial food or a combination of both); however, the information in the questionnaire may not have been a true reflection of food intake. Body condition score was not recorded because none of the dogs was extremely under- or overweight. The treatment protocol of dogs in CHF was based on diuretics, ACE inhibitors, an inodilator, and antiarrhythmics; however, the dose regimen and selected drugs were individually adjusted, potentially influencing the results of measured oxidative stress parameters. The ISACHC groups were not completely homogenized regarding the duration of therapy and combination of drugs, which might also have affected our results.
Footnotes
Acknowledgements
We thank Dr. Peter B. Connolly from IDEXX Laboratories (Westbrook, ME) for the analysis of NT-proBNP.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We acknowledge the financial support of the Slovenian Research Agency (research program P4-0053).