
Abstract
Racehorses are susceptible to bone fractures when damage from repetitive, high-magnitude loads incurred during training and racing exceed concurrent damage removal and replacement, resulting in transient periods of focal osteoporosis and bone weakening. Clinically, these events correspond to cortical stress fractures and subchondral bone stress remodeling. Evidence of these preexisting lesions include periosteal callus, endosteal callus, and intracortical focal hyperemia for cortical stress fractures; and subchondral focal hyperemia located superficial to sclerotic compacted trabecular bone tissue for subchondral stress remodeling. These findings must be in direct physical association with an acute fracture to infer that the abnormalities precipitated complete bone fracture. Recognition of preexisting lesions must be conveyed in the autopsy report to the racehorse industry audience because this is the mechanism for education of racehorse trainers, veterinarians, and owners. Standardized anatomic nomenclature, fracture classification, and documentation of gross autopsy findings specific to catastrophic bone fractures in racehorses provides information to empower changes in management of racehorses for the detection and management of mild injuries and prevention of catastrophic fractures.
Introduction
The vast majority of catastrophic fractures in racehorses are subsequent to the culmination of injuries that develop over time as the result of repetitive limb loading during training and racing. Consequently, catastrophic fractures are occupational injuries that are predictable in their locations and configuration. Fractures often occur because of continuing to train and race with preexisting injuries that reduce a bone’s normal breaking strength, and thus are “pathologic fractures.” Fractures occur during high-risk periods caused by the events in the 2–3 mo, although sometimes 6 mo to years, preceding acute, catastrophic fracture.
In a 2-y study of bone fractures in California racehorses using an enhanced orthopedic gross autopsy procedure, clear evidence of stress fracture or subchondral stress remodeling (stress-related bone injury) was observed in direct association with the fracture in 74% of bone fractures, with some evidence in an additional 19% of bone fractures (UCDavis CHRB Racing Injury Prevention Program, https://goo.gl/Zr2fFt). These features create focal areas of weakness within the bone structure that make affected bones highly susceptible to complete fracture under otherwise normal training and racing circumstances, consistent with theories of the genesis of lateral condylar third metacarpal and metatarsal bone fractures14,15 and complete fracture secondary to stress fracture.5,18
The diagnostic pathologist plays a critical role in the treatment and prevention of future fractures in racehorses by educating racing industry professionals about findings associated with present fractures, particularly abnormalities that preceded, and likely contributed to, catastrophic bone fracture. Only through the accurate and unambiguous recording of fracture configuration and associated findings is progress made in the understanding of fracture etiopathogenesis, treatment, and prevention.
Thorough observation, standardized documentation, collection of data for prospective studies of risk factors, and targeted description using anatomical nomenclature of racehorse fractures enhance the usefulness of the autopsy findings and report. Thorough observation allows for the recognition of consistent fracture patterns and evidence of preexisting lesions that can provide biomechanical and pathology clues to fracture pathogenesis. A standardized methodology for fracture documentation promotes consistency and thoroughness in the observation of fracture configurations and associated findings. The inclusion of specific observations using explicit terminology and criteria ensures systematic collection of data useful for epidemiologic studies of risk factors for fracture. Accurate characterization using anatomic nomenclature ensures the unambiguous interpretation of findings. Description of the findings in the autopsy report should be targeted to educate racing industry audiences (i.e., regulatory veterinarians, attending veterinarians, trainers, owners, veterinary surgeons interested in fracture treatment, and researchers investigating fracture etiopathogenesis to design preventive strategies).
Anatomic nomenclature
Descriptions of the location of pathologic findings must use anatomic nomenclature, because, regardless of body orientation, the location of the findings cannot then be misconstrued. The system for anatomic nomenclature uses the body as the reference frame, so that whether the body is standing, supine, prone, or in left lateral recumbency, the proximal surface of the radial carpal bone is recognized at the same location on the horse. Whereas, the “top, or upper surface” of the radial carpal bone, using the earth’s coordinate system, would be the proximal surface in the standing horse, but the distal surface in the dorsally recumbent horse. Similarly, use “left or right” leg, rather than “upper or lower” leg, to prevent misinterpretation.
Anatomic terms and rules for terms of direction in domestic animals are found in the Nomina Anatomica Veterinaria 12 and summarized in veterinary textbooks. 6 Veterinary terminology differs from human terminology because the quadruped stance of animals has a different body orientation compared with the biped, upright stance of humans. In veterinary medicine, the terms anterior, posterior, superior, and inferior apply to only a few locations (eye, eyelids, lips, and inner ear) in quadrupeds.
The paired terms cranial and caudal apply to the neck and trunk and the portion of the limbs proximal to the carpus and tarsus (Fig. 1). The terms dorsal and palmar apply to the manus (portion of the forelimb distal to the antebrachium, i.e., antebrachiocarpal joint or radiocarpal joint). The terms dorsal and plantar apply to the pes (portion of the hindlimb distal to the crus, i.e., tarsocrural joint). For the limbs, the terms proximal and distal refer to closer or farther from the trunk.
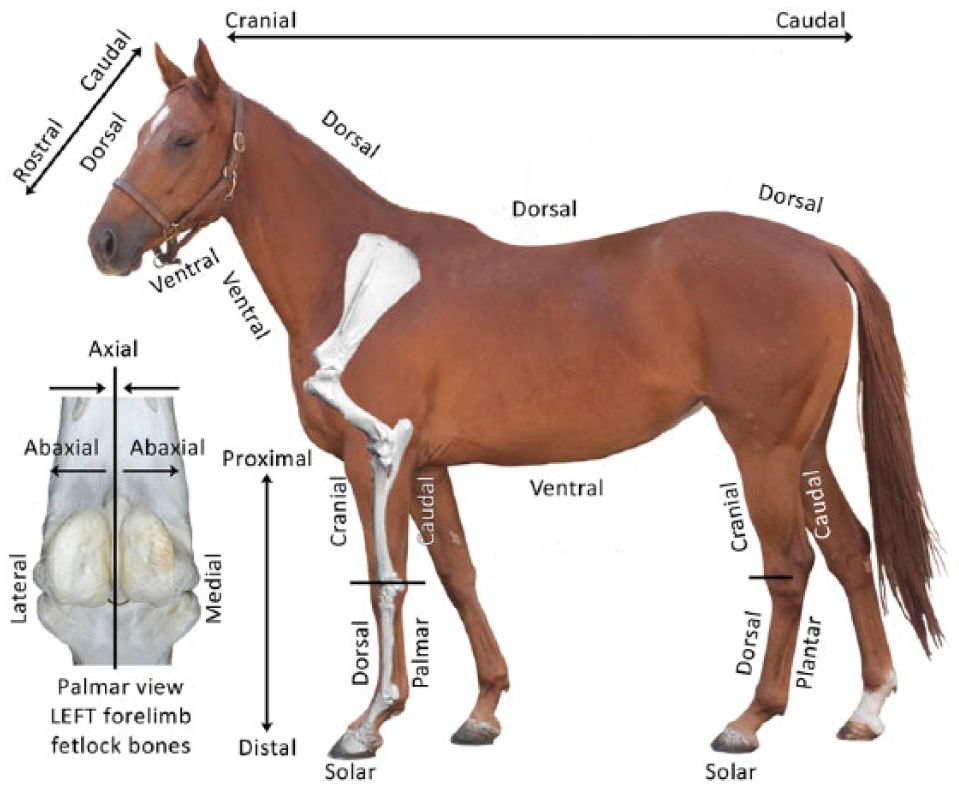
Terms of direction are illustrated on a photograph of a horse, and a palmar view of the bones that articulate in the left metacarpophalangeal (fetlock) joint.
It is often useful to refer to planes of the body when describing fracture orientation. The plane that divides the body into left and right halves is the median plane. Sagittal planes are planes that are parallel to the median plane. Sagittal planes also apply to the limbs. Transverse planes are those planes perpendicular to the long axis of the body or body part. Dorsal planes are parallel to the dorsal surface of the body or body part and perpendicular to the median and transverse planes (the term frontal plane is not applicable to quadrupeds). Additional terms of direction relative to planes include medial and lateral (i.e., toward or away from the median plane) and axial or abaxial (i.e., toward or away from the mid-sagittal plane or axis of a limb; Fig. 1).
Acute fracture classification
Several components of fractures are important to characterize because they inform fracture treatment and prognosis for other horses with similar fractures, and provide clues to biomechanical factors that promoted fracture and could be useful in fracture prevention (Fig. 2). The description should capture affected bone(s) and fracture location and configuration. Key components of fracture location and configuration that should be explicitly captured include those in Table 1.
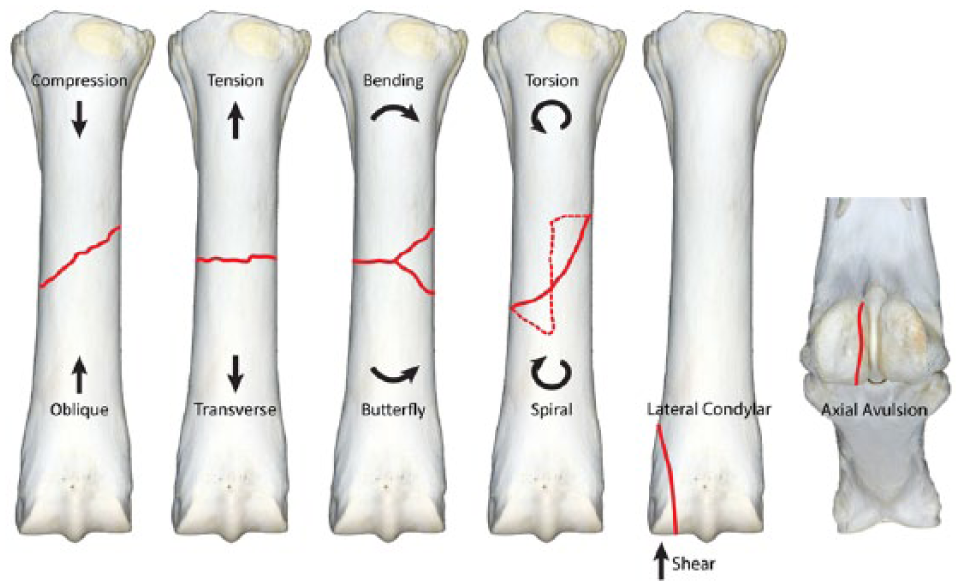
Common fracture configurations and simplified forces that contribute to those fracture configurations are illustrated on diagrams of the dorsal surface of the right forelimb third metacarpal bone and the palmar surfaces of the bones that articulate in the metacarpophalangeal joint. The longitudinal fracture of the proximal sesamoid bone is on the axial side of the bone and associated with tension of the intersesamoidean ligament.
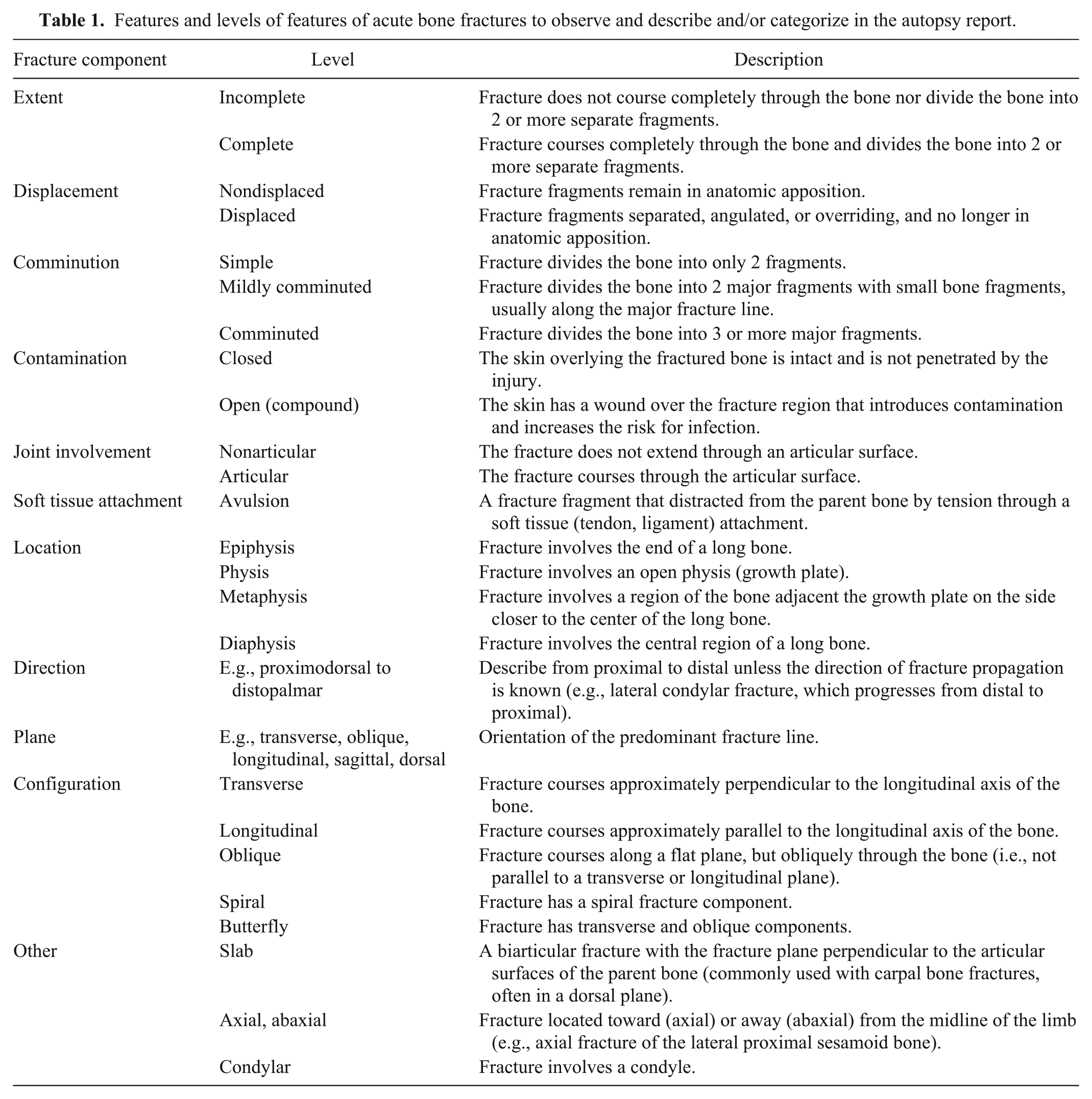
Features and levels of features of acute bone fractures to observe and describe and/or categorize in the autopsy report.
Description of the fracture should facilitate interpretation of the findings by the intended audience. Understanding will be enhanced when the description starts with an orientation of the larger picture or most important fracture component, followed by lesser fracture components. Furthermore, each segment of the description provides the “what,” “where,” and “significance” of the finding. As an example, the description of a typical fracture of the scapula in racehorses (Fig. 3) would be first described as “a complete, displaced, oblique fracture (what) at the level of the distal end of the spine of the scapula (where) that separated the scapula into a large proximal fragment and a smaller distal fragment (significance). The distal fragment had a complete, displaced, longitudinal, articular fracture that divided the distal fragment into cranial and caudal fragments. An incomplete, non-displaced fracture with a missing fragment coursed from the major oblique fracture proximally into the infraspinatus fossa.” The first sentence provides the major finding that resulted in inability to bear weight on the leg and provided the reference frame for the description of other components of the fracture.

The scapula from a racehorse that incurred catastrophic fracture during training or racing. An oblique fracture at the level of the distal end of the spine of the scapula divides the bone into a larger proximal fragment and smaller distal fragment. The distal fragment is divided into cranial and caudal fragments by a complete longitudinal articular fracture that extended to the glenoid cavity. An incomplete fracture courses proximally from the oblique fracture into the infraspinatus fossa. A bone fragment is missing adjacent to the incomplete fracture line.
Fracture diagram
The use of a diagram for recording fracture findings enforces a systematic examination of the fracture from several anatomical perspectives (e.g., dorsal, palmar, medial, lateral, and articular aspects of a long bone) and provides a mechanism for recording important features of the fracture that are difficult to capture in text format (Fig. 4). This technique also leads the pathologist to attempt reconstruction of the fracture fragments and enhances focused observation on fracture fragments for abnormal findings. Diagram templates of each bone typically affected with fracture facilitate the process of recording abnormal findings. Further, the diagram can be used to track the location of samples taken for further processing and examination. Diagram templates can be downloaded from http://www.vetmed.ucdavis.edu/vorl/local_resources/docs/.
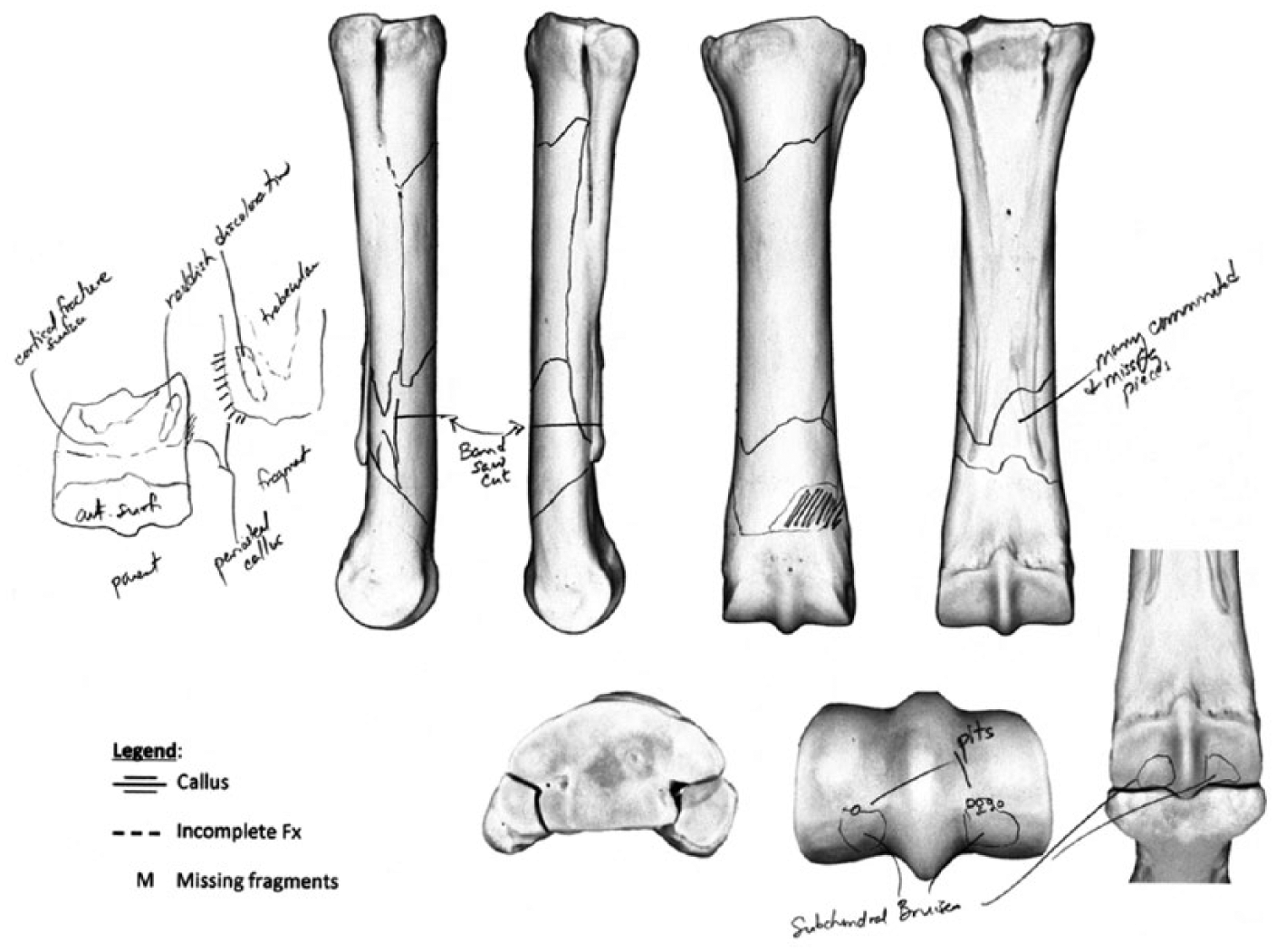
Diagram of a left third metacarpal bone fracture in a racehorse illustrates observations that would be difficult to capture in text alone. Locations for sampling tissues (e.g., for histology) can also be delineated for future reference when interpreting the sample findings.
Bone-specific diagrams can incorporate a list of common features of bone-specific fractures to simplify and standardize categorization of fractures according to features in Table 1 (Fig. 5). Explicitly categorized features facilitate the recording of findings for retrospective and epidemiologic studies. Furthermore, this mechanism can ensure that observations were actually made and features were not present (as opposed to no observation or missing data).

Example of a form that captures key features of the fracture location, configuration, and nature with a bone diagram.
Pathologic findings
The majority of bone fractures in racehorses are secondary to preexisting stress fractures or subchondral bone stress remodeling.1,4,8,17 –20 (Stover SM. Diagnostic workup of upper-limb stress fractures and proximal sesamoid bone stress remodeling. Proc Am Assoc Equine Pract 2013:427-435; Nashville, TN). The detection and documentation of abnormalities that preceded complete fracture and likely predisposed to acute, catastrophic fracture is paramount. Extending this knowledge to industry personnel is the mechanism for invoking change in racehorse management and preventing catastrophic injuries in other racehorses. Preexisting lesions that contributed to a pathologic, catastrophic fracture must be clearly documented in the autopsy report.
Gross dissection technique for detection of preexisting lesions
Most preexisting lesions that likely predispose to catastrophic bone fracture can be observed by a focused gross autopsy alone. Because any preexisting lesion that predisposed to pathologic complete fracture must be in direct physical association with the complete fracture, the examination is focused on the fracture surfaces, and adjacent periosteal surface and endosteal bone tissues. The fracture surfaces can be cleaned under running tap water with a soft brush (e.g., surgical scrub brush) to remove hemorrhage and debris for visualization of fracture interfaces. Periosteal tissues should be removed for a minimum distance of 1–2 cm from all fracture margins. In young racehorses, the periosteum usually strips easily away from the bone with forceps, traction, and blunt dissection. Gentle scraping of periosteal tissues with a scalpel may be needed, but aggressive scraping will remove fresh, newly woven bone callus from periosteal surfaces. Occasionally, a thick layer of unusually adherent fibrous connective tissue will cover a chronic periosteal callus. Endosteal bone tissues adjacent to the fracture edge can be gently washed.
Signs of preexisting lesions
The signs of preexisting lesions are related to the responses of bone tissues to injury. Microdamage causes the first response to injury. Microdamage occurs in racehorses because of repetitive, high-magnitude loads incurred during training and racing.9,13 Microdamage incites bone repair responses. 2 Microdamage that causes osteocyte death or compromises osteocyte health induces bone remodeling,3,21 which causes an initial, rapid resorption of damaged bone tissue, within days or weeks. 11 Bone resorption is followed by the slower replacement of removed bone by healthy bone tissue, which requires months. 11 These temporally related events can cause transient focal osteopenia characterized by fragile bone tissue within an area of hyperemia. Focal regions of osteopenia can frequently be visualized in 2 locations, the fracture surface of cortical bone with a preexisting stress fracture and the subchondral bone of articular fractures (Figs. 6, 7). Biomechanically, the osteopenic focus causes a stress riser and weakens the bone structures 7 so that the bone is susceptible to stress fracture 10 or complete fracture under otherwise normal loading (training and racing) circumstances.
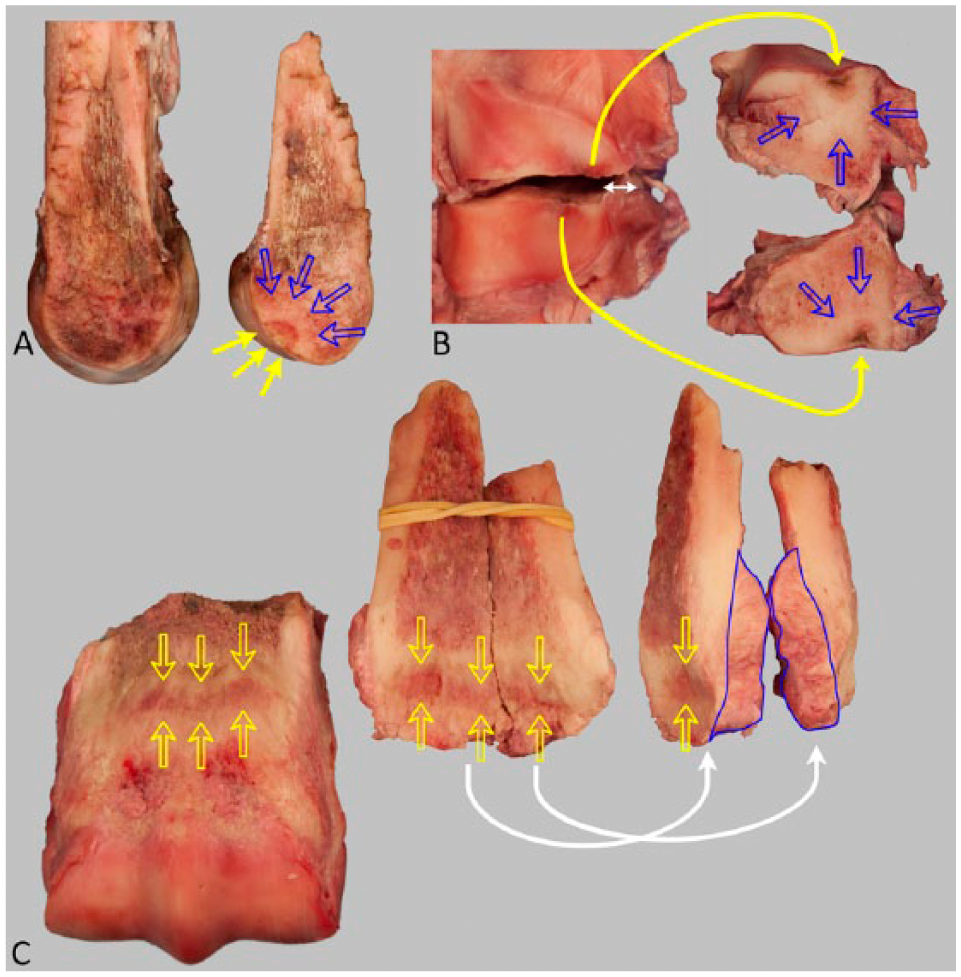
Focal regions of stress remodeling (yellow arrows; i.e., active bone remodeling predominated by bone resorption and characterized grossly by focal regions of red discoloration and roughened surfaces usually within a region of sclerosis [blue arrows]).
The right third metacarpal bone from a 5-y-old Thoroughbred racehorse that had bilateral third metacarpal bone fractures.
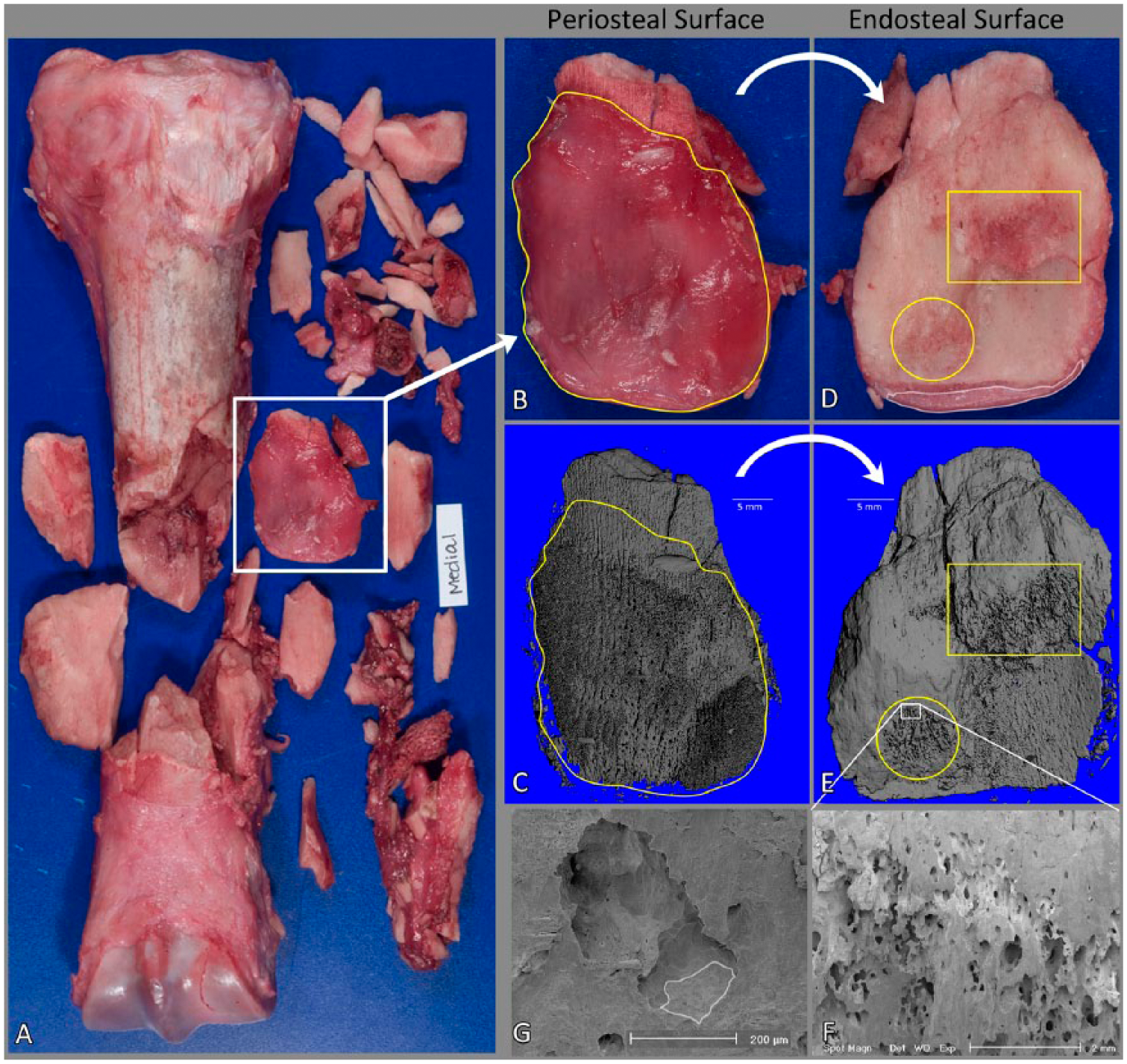
The second response is the attempt of bone to buttress the weakness associated with the accumulation of microdamage and focal osteopenia in the stress fracture or subchondral stress remodeling site. Physiologic loads on compromised bone material cause supraphysiologic bone strains, which induce modeling (i.e., bone apposition) on bone surfaces. 16 This mechanism buttresses the weakened region by apposition of new bone on periosteal and endosteal bone surfaces (Fig. 8). The signs of buttressing of stress fractures in cortical locations are the presence of periosteal callus and endosteal callus. The callus must be present in physical association with the acute, complete bone fracture (i.e., present on adjacent fracture fragments indicating that the callus had bridged the focal lesion that induced fracture). In subchondral regions, buttressing is prevented on articular surfaces because of the overlying hyaline cartilage, but manifests in the form of compaction and sclerosis of trabecular bone tissue (Fig. 6).
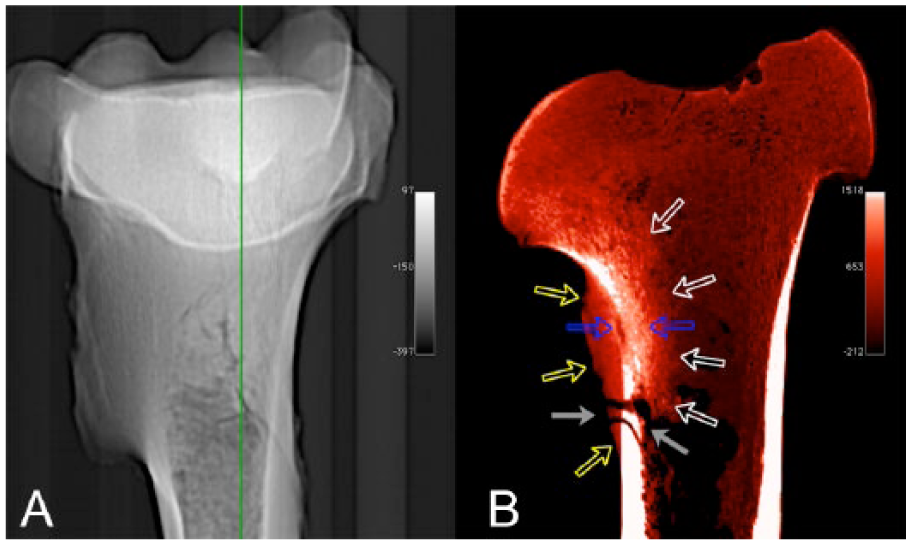
Computed tomography (CT) scan of the proximal portion of the left humerus with a reconstructed fracture.
The nature of the callus depends on the chronicity and course of the response. 16 Recently formed periosteal callus is thin (<1 mm thick), red (highly vascular), rough, woven (soft) bone tissue that often has a subtle pattern with an orientation that parallels the longitudinal axis of a long bone (Fig. 9). Callus that has been present for a longer period and has undergone remodeling and replacement of woven bone tissue by lamellar bone tissue can be large, firm, pale, and smooth-surfaced (Fig. 9). Acute, complete bone fractures with a chronic callus often also have more recently formed callus on the periphery of the chronic callus indicating a recent exacerbation of the stress fracture disease.
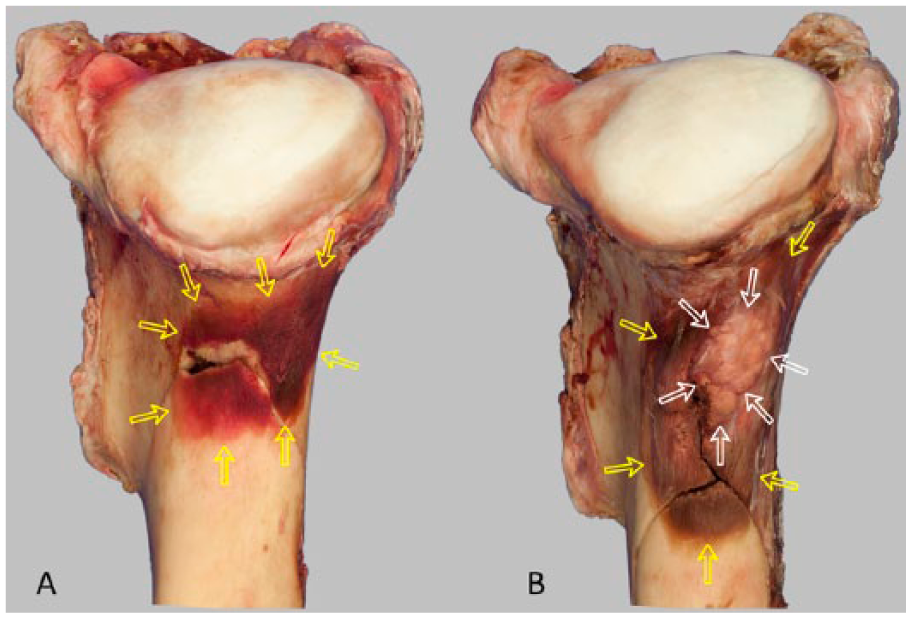
Caudal aspect of the proximal portion of the reconstructed complete fracture of the left humerus in 2 different racehorses.
The contralateral, intact (or occasionally fractures are bilateral) bone should always also be examined. The contralateral, intact bone often reveals signs of the preexisting disease that preceded fracture of the affected bone because of the bilateral nature of repetitive, overuse injuries18,20 (Stover SM. Diagnostic workup of upper-limb stress fractures and proximal sesamoid bone stress remodeling). Bilateral bones are often affected with stress fracture and subchondral stress remodeling responses; although, the weakest bone is subject to catastrophic complete fracture. Examination of contralateral bones is also useful because sentinel fracture fragments can be missing from open, comminuted fractures (e.g., metacarpal bone fractures).
Description of the pathologic findings associated with preexisting lesions must be conveyed to industry personnel because findings may be detectable using clinical diagnostic techniques. Furthermore, racehorse trainers and veterinarians can correlate the presence of preexisting stress fractures and stress remodeling with clinical histories, and thus enhance detection of these disorders in other racehorses before catastrophic fracture.
Radiographs
Radiographs of bone fractures are useful adjuncts to the autopsy examination. Radiographic visualization of large, chronic periosteal calluses can convey to racehorse trainers and veterinarians the usefulness of radiographs for detection of lesions in live racehorses. However, recently formed, thin, woven bone (periosteal callus) does not have sufficient bone mineralization for visualization on clinical radiographs. Radiographs are also useful for detecting some intracortical lesions (incomplete stress fractures), endosteal callus, and subchondral bone sclerosis, particularly on the intact, contralateral bone of horses that had bilateral disease and catastrophic fracture in the other limb (Fig. 10).

Lateromedial radiographs of the bilateral metacarpal bones of a racehorse that had unilateral, comminuted, open third metacarpal diaphyseal bone fracture. The fractured bone had key missing fragments, however. Note the incomplete stress fractures in the contralateral bone (arrows) at a similar location and orientation to the proximopalmar to distodorsal oblique fracture surface in the fractured bone. This horse likely had bilateral metacarpal stress fractures, with the weakest third metacarpal bone sustaining complete fracture.
Ancillary techniques
Occasionally, it is helpful to remove all soft tissues for preparation of a dried bone specimen. Examination of dried specimens is most helpful early in the discovery of bone-specific sites of predisposition for stress fracture and stress remodeling changes. However, debridement of all soft tissues is not routine or necessary in most cases. Furthermore, complete soft tissue debridement is not a replacement for a gross autopsy examination. When desired, there are several techniques for removal or dissolution of soft tissues, ranging from natural debridement (environmental exposure, beetles) to boiling and chemical (lye, bleach) debridement. Digestion of the soft tissues should be done slowly in a controlled environment and bones examined frequently during the process because new woven bone tissue is soft and easily and quickly digested, removing the evidence of callus. Beetles effectively remove only soft tissue, but the bones usually require further cleaning. Boiling is not recommended because bones may demineralize during the process. In our facility, digestion is controlled using 1% potassium hydroxide at 45°C for a variable amount of time (3–14 d), depending on the size of the bone and the remaining soft tissues after manual debridement. Bones are examined and debridement assisted manually as often as daily during the process.
Autopsy report
The autopsy report serves several functions for the racehorse industry and regulatory agencies. The report brings closure to what happened to individual horses. Collectively, the reports are useful for monitoring diseases and disorders in the racehorse population.
Importantly, the report is also an educational tool for horse owners, trainers, and veterinarians. In addition to the characterization of the acute bone fracture, the pathologist must observe and convey the factors that likely contributed to bone fracture to the racehorse industry through the autopsy report. Preexisting stress fractures and stress remodeling are the most common contributing factors to catastrophic fracture (https://goo.gl/Zr2fFt). The factors that contribute to causes of musculoskeletal deaths must be relayed to industry professionals and horse owners. This information is critical for the detection and management of milder injuries that are the precursor to catastrophic injuries, thus enhancing the management of other racehorses for the prevention of catastrophic injuries.
Footnotes
Acknowledgements
The California Horse Racing Board’s Postmortem Program and Racing Injury Prevention Program, and California Animal Health and Food Safety Diagnostic Laboratory System pathologists made much of this work possible.
Author’s contributions
SM Stover contributed to conception and design of the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication of this article was supported by the Center for Equine Health with funds provided by the State of California pari-mutuel fund and contributions by private donors.