
Abstract
Pulmonary hyalinosis is an idiopathic, typically incidental lesion of old dogs, characterized by multifocal aggregates of epithelioid and multinucleate macrophages that surround periodic acid–Schiff (PAS)-positive hyaline material in airways. Lung lesions resembling pulmonary hyalinosis were observed in 6 captive adult sugar gliders (Petaurus breviceps; 5 females and 1 male) in a retrospective review of 18 autopsied animals. Clinical signs for 3 of the sugar gliders included lethargy, tachypnea, and dyspnea. At autopsy, 5 of 6 animals had comorbid lesions that were the primary cause of death. Gross pulmonary lesions were characterized by mildly firm, discolored, vaguely nodular areas of parenchyma. Histologic examination of the lung revealed granulomatous inflammation with intracellular and extracellular amphophilic hyaline bodies within alveoli and airways. Hyaline bodies were positive for PAS and oil red O staining, blue via crystal violet staining, and displayed birefringence under polarized light, similar to findings in dogs with pulmonary hyalinosis.
Pulmonary hyalinosis is an uncommon alveolar-filling disorder of dogs.1,4 Alveolar-filling disorders are a group of overlapping conditions defined by the deposition of abnormal material within alveoli and include alveolar histiocytosis, endogenous lipid pneumonia, pulmonary alveolar proteinosis, pulmonary hyalinosis, and alveolar microlithiasis. Pulmonary hyalinosis in the dog is characterized by abnormal multifocal accumulations of basophilic-to-amphophilic, rounded hyaline bodies in alveoli and larger airways. 3 Lesions are often subpleural or peribronchial. Hyaline bodies are both intrahistiocytic, with epithelioid macrophages and multinucleate giant cells predominating, or forming large extracellular aggregates. The hyaline bodies are positive for periodic acid–Schiff (PAS) and oil red O staining, and stain blue via the crystal violet technique. The bodies also display birefringence under polarized light.1,4
The inciting cause and pathogenesis for this accumulation of pulmonary hyaline material is unknown, but disease is seen predominantly in older dogs and typically is considered incidental. 3 Early descriptions suggested a response to inhalation or aspiration of irritants, including uranium ore dust. 4 Similar to other alveolar-filling disorders, abnormal alveolar hyaline material is thought to accumulate because of some combination of reduced bronchociliary clearance, excessive production, or impaired breakdown, typically by alveolar macrophages.
Sugar gliders (Petaurus breviceps) are nocturnal marsupials native to Australia and New Guinea and are increasingly seen in exotic animal practice. Common ailments encountered in pet sugar gliders include malnutrition, obesity, metabolic bone disease, dental disease, lymphoid neoplasia, stress-related skin disease, and trauma. 9 Respiratory diseases of wild or captive sugar gliders are not well represented in the literature, but cases of bacterial and fungal pneumonia, toxoplasmosis, and pulmonary pentastomiasis have been reported. 6 Herein, we report 6 cases of pulmonary hyalinosis in captive sugar gliders.
A retrospective database search of sugar glider autopsies performed at the New York State Animal Health Diagnostic Center, Cornell University, College of Veterinary Medicine (Ithaca, NY), was undertaken from 1996 to 2015. This search identified 21 cases; however, in 4 cases, no lung tissue was available for review. Pulmonary hyalinosis was identified in 5 of the remaining 17 autopsies. Of the 17 animals, 6 were male (5 intact, 1 neutered), 10 were female (9 of 9 intact), and 1 had no sex recorded. The average age for 12 of the animals was 3.9 y with no age data recorded in 5 animals. An additional case (case 6) was included by one of the coauthors (AD Lewis).
All 6 affected sugar gliders were privately owned pets and reproductively intact. They ranged in age from 3 to 14 y (Table 1). Clinical signs for 3 of the animals included tachypnea and/or dyspnea, and 1 was dead-on-arrival with no clinical history. At autopsy, 5 had significant comorbid lesions including neoplasia (n = 3; hepatocellular carcinoma, urinary bladder sarcoma, and undifferentiated round cell tumor), chronic renal disease (n = 2), endometritis (n = 2), and large bowel impaction (n = 1), which were the primary causes of clinical demise in these animals. The 2 sugar gliders with significant renal disease had no evidence of metastatic mineralization. Cause of death in 1 glider (case 6) was directly attributed to pulmonary disease, as comorbidities were not present.
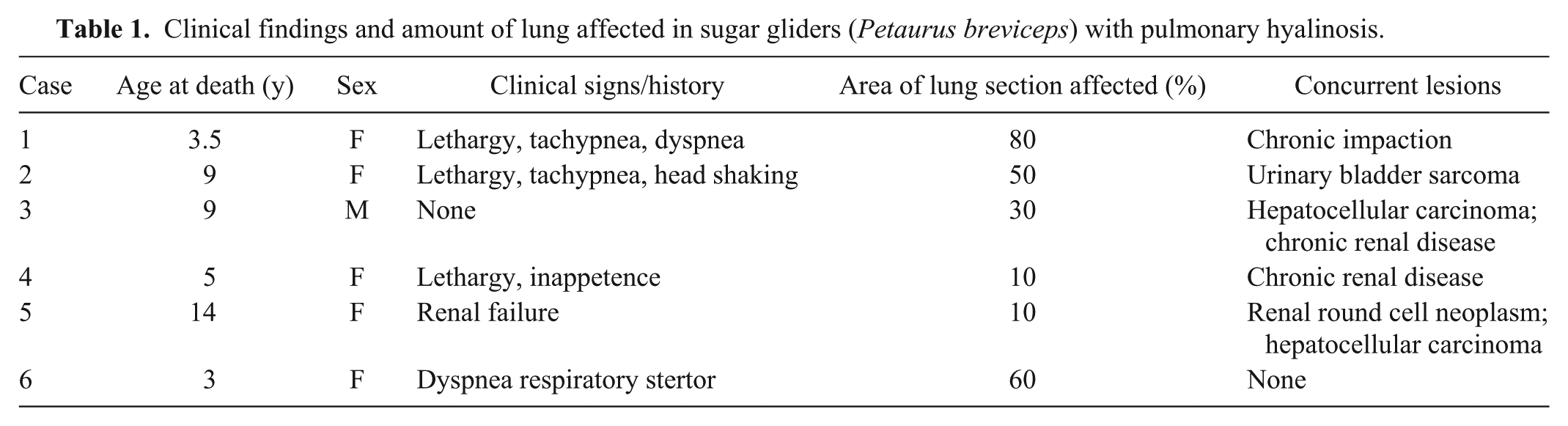
Clinical findings and amount of lung affected in sugar gliders (Petaurus breviceps) with pulmonary hyalinosis.
Gross pulmonary lesions were recognized in 3 of 6 animals and were characterized by mildly firm, discolored, vaguely nodular areas of pulmonary parenchyma. Tissue samples were collected in 10% neutral-buffered formalin, routinely processed for paraffin embedding, sectioned, and stained with hematoxylin and eosin (H&E). Between 1 and 5 sections of lung were examined in each case. Additional stains included PAS, crystal violet, von Kossa, and modified Steiner silver. For cases with available formalin-fixed tissues, lung was snap-frozen for cryosectioning and stained with oil red O. Processing for transmission electron microscopy (TEM) was carried out on 1 case (case 2) and followed routine procedures. Using an H&E slide, an appropriate sample was cut from the paraffin block and deparaffinized with xylene for 24 h, followed by dehydration in absolute ethanol to 70%. Samples were washed in cacodylate buffer, fixed in a mixture of 2.5% glutaraldehyde and 2.5% paraformaldehyde in 0.1 M cacodylate buffer at 4°C for 24 h, post-fixed in 1% osmium tetroxide, and dehydrated in a graded acetone series. Samples were then infiltrated and embedded in resin (Polysciences, Warrington, PA), and 70-µm sections were obtained with an ultramicrotome (RMC Boeckler Instruments, Tucson, AZ) on 200-mesh copper grids stained with uranyl acetate and lead citrate. Sections were imaged with a transmission electron microscope (JEOL, Tokyo, Japan) at a 100-kV accelerating voltage.
Histologic examination of the lung revealed similar lesions in all cases, but affected portions of lung varied ~10–80% in examined sections (Table 1). Alveoli and, to lesser extent, large airways were multifocally filled and often distorted by granulomatous inflammation with intermixed intra- and extracellular, rounded, acellular, amphophilic hyaline bodies, ≤1 mm diameter, with occasional radial striations and concentric laminations (Fig. 1). Hyaline deposits were most prominent around the periphery of the lung lobes and adjacent to large airways and were often surrounded by collapsed alveoli and variable numbers of mixed inflammatory cells, including epithelioid macrophages, multinucleate giant cells, lymphocytes, plasma cells, and a few neutrophils. In one case, prominent numbers of hyaline bodies were present in bronchi and bronchioles (Fig. 2). Adjacent alveolar septa were mildly widened by similar inflammatory cells and small amounts of fibrous connective tissue. Hyaline bodies were positive for PAS and oil red O, blue via crystal violet, and displayed peripheral birefringence under polarized light (Figs. 3–4), similar to findings in dogs with pulmonary hyalinosis, but did not contain identifiable plant or other foreign material on modified Steiner and von Kossa stains.
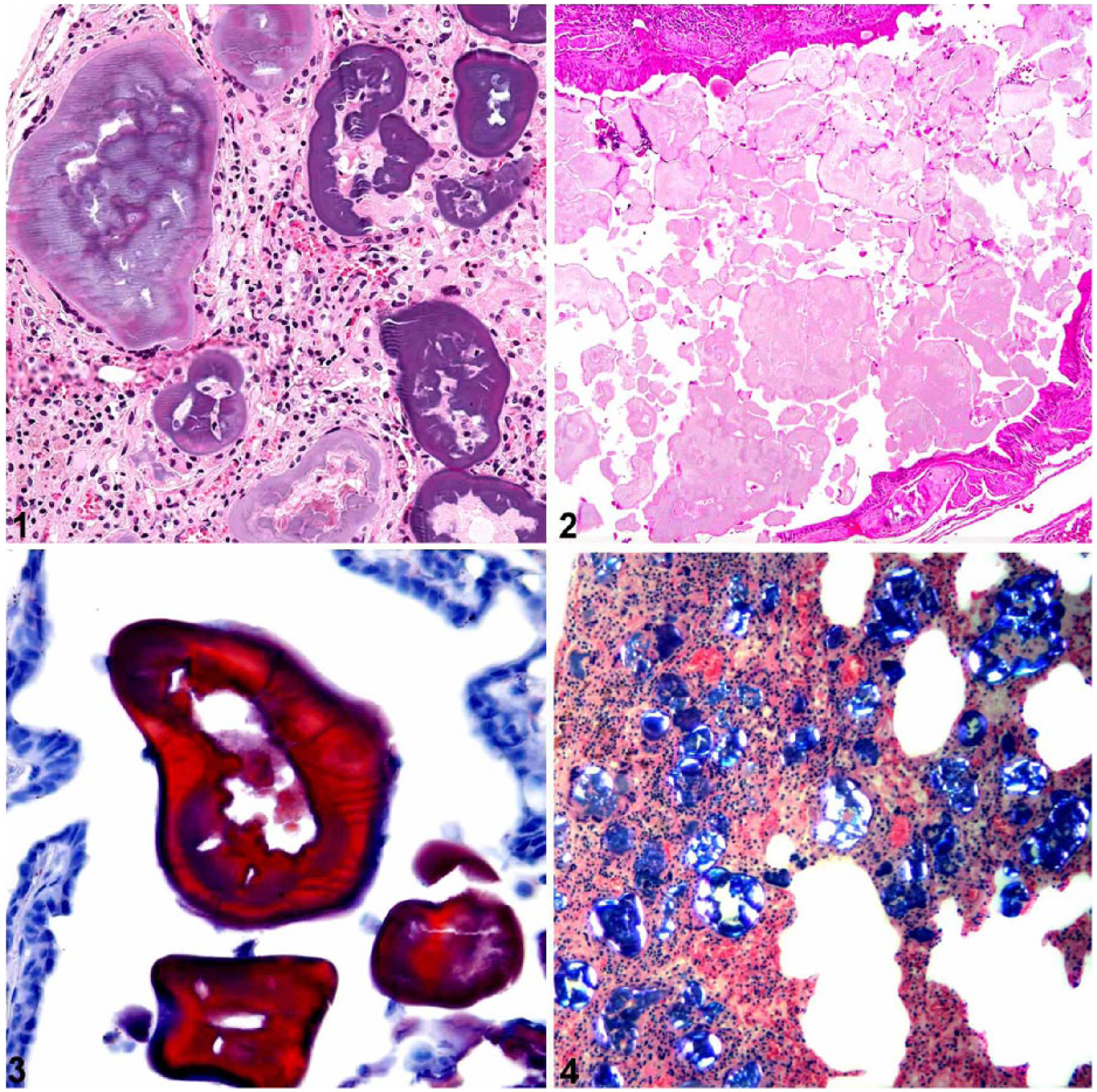
Pulmonary hyalinosis in sugar gliders (Petaurus breviceps).
TEM of the intra-alveolar hyaline material revealed a heterogeneous variably osmiophilic, dense stellate-to-crystalline material that filled alveolar lumina, often compressing and flattening the adjacent epithelium (Fig. 5). In one area, the material closely apposed and interdigitated with remnant cilia (Fig. 6). Lamellar bodies were not appreciated amid this material or within macrophages. Scattered inflammatory cells, including granulocytes, were present adjacent to affected airways. Imaged blood vessels were within normal limits.
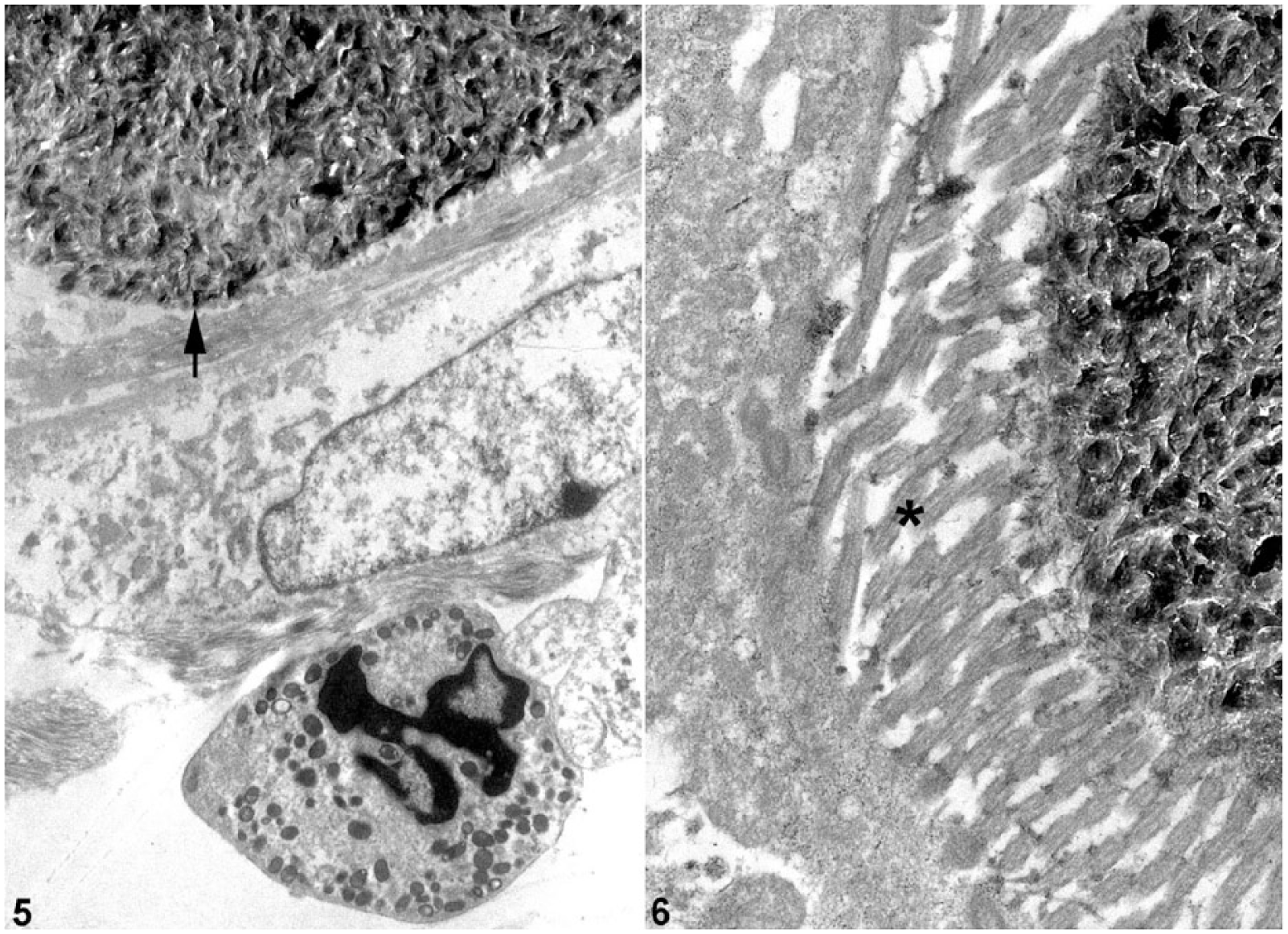
Transmission electron micrographs of pulmonary hyalinosis in sugar gliders (Petaurus breviceps); case 2.
The histologic, histochemical, and TEM findings in these sugar gliders parallel those described in dogs with pulmonary hyalinosis. Possible causes for the lung lesions in these sugar gliders include aspiration pneumonias or other alveolar-filling disorders. Examples of aspiration pneumonia include exogenous lipid pneumonia and silica dust inhalation. We found no evidence of foreign material (e.g., plant, silica, extracellular lipid droplets) on histologic examination (including silver stains) or TEM.
There is considerable overlap in the alveolar-filling disorders, but pulmonary hyalinosis, as seen in these sugar gliders and previously described in dogs, appears distinct. The alveolar-filling disorders are distinguished by the appearance and nature of the accumulated material, but are not necessarily differentiated by an underlying etiology or pathogenesis. Alveolar histiocytosis and endogenous lipid pneumonia encapsulate a spectrum of lesions characterized by focal aggregates of foamy macrophages with or without demonstrable intracellular lipid and cholesterol crystals, but no hyaline material. 3 Most cases are considered idiopathic, but some follow bronchial obstruction; reported cases in wild opossums often coincide with pulmonary nematodiasis. 2
Alveolar microlithiasis is characterized by the presence of predominantly extracellular, alveolar and septal, hard, concentrically laminated concretions of calcium phosphate, calcium hydroxyapatite, or carboxyapatite that require demineralization. Cases have been reported in humans with a mutation in the type IIb sodium-phosphate cotransporter (SLC34A2) gene, involved in phosphate homeostasis, and associated with heart disease in both humans and dogs.3,5,7
Pulmonary alveolar proteinosis (PAP), lipoproteinosis, and phospholipidosis are related alveolar-filling disorders most often encountered in humans and laboratory rodents. In these, acellular eosinophilic-to-amphophilic material, composed largely of surfactant proteins and phospholipids defined ultrastructurally by lamellar and tubular myelin-like arrangements, accumulates extracellularly in alveoli with no significant inflammatory reaction.3,8,10,11 Cases of PAP have been described in humans, lab rodents, dogs, cats, and tamarins.3,8,10,11 PAP has been attributed to excess surfactant production (as a result of silica dust inhalation or surfactant protein deficiencies) and impaired degradation of surfactant proteins by alveolar macrophages (resulting from granulocyte–macrophage colony stimulating factor autoantibodies, knockout, or interleukin 10 inhibition).3,11 In the sugar gliders in our study, a specific identity of the abundant intra-alveolar material was not evident from the ultrastructure, but it did not have the appearance of mucus or protein. The material may be compatible with collapsed and compressed surfactant similar to PAP, but unlike PAP, intra-alveolar material in these sugar gliders was predominantly intracellular, contained no identifiable lamellar bodies, and was accompanied by significant attendant inflammation.
Although pulmonary hyalinosis in dogs is typically considered an incidental lesion in older animals, clinical disease may be more likely in sugar gliders with pulmonary hyalinosis, and it is not a disease of the aged alone. In the 3 sugar gliders with a clinical history of tachypnea and/or dyspnea (cases 1, 2, and 6), the percentage of lung affected in histologically examined sections was ≥50%. In one of these, death was attributed to pulmonary hyalinosis. Two of the gliders were young, suggesting the possibility that this disease starts early in these animals. Interestingly, most affected animals were female, suggesting a possible increased risk. Sugar glider lung anatomy is similar to other small mammals, and significant differences in lung anatomy that may account for predisposition for hyalinosis is not known. Possible causes of pulmonary hyalinosis in these sugar gliders include exposure to chemicals or mineral dusts, dysregulation of surfactant protein homeostasis, and defects in pulmonary macrophage function. Additional analysis, including mass spectrometry or immunohistochemistry for surfactant proteins, may help determine the makeup of the intra-alveolar material in these sugar gliders and illuminate the pathogenesis. Spontaneous pulmonary hyalinosis in sugar gliders or in any non-canine species is a novel cause of respiratory disease in this species.
Footnotes
Acknowledgements
We thank the histopathology technicians at Cornell University, College of Veterinary Medicine for assistance with case processing, and Jen Patterson for assistance with images. We also thank Dr. Alicia Withrow at Michigan State University Center for Advanced Microscopy for TEM preparation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared that they received no financial support for their research and/or authorship of this article.