
Abstract
A Cavalier King Charles Spaniel dog was presented because of a 10-d history of progressive vomiting, inappetence, and lethargy, with mild neurologic signs. Fine-needle aspirates of splenic nodules seen on ultrasound were suggestive of a carcinoma. On autopsy, a disseminated neoplasm was present in the lung, spleen, and adrenal glands. Additionally, there was a Chiari-like malformation of the skull with corresponding syringomyelia of the cranial spinal cord. Histologically, the neoplasm was comprised of a pleomorphic population of round cells with a high mitotic rate. Cells stained positive for vimentin and CD18 and negative for cytokeratin, chromogranin A, CD3, CD20, MHC II, and CD11d, and hence the tumor was diagnosed as a histiocytic sarcoma. The cytologic presentation in this case is uncommon for this type of tumor, as was the clinical presentation.
An 8-y-old male neutered Cavalier King Charles Spaniel dog was presented to the University of Georgia Emergency Service (Athens, GA) because of a 10-d history of progressive vomiting, inappetence, and lethargy. On examination, the patient had dull mentation, cervical pain, and kyphosis. The patient became progressively ataxic and more mentally depressed during hospitalization. Thoracic radiographs revealed a mild-to-moderate interstitial pulmonary pattern that was most severe in the right caudal quadrants. Abdominal ultrasound revealed a mottled splenic parenchyma.
Fine-needle aspirates of the spleen revealed many small, cohesive-like aggregates of round to bluntly rectangular cells with moderately basophilic cytoplasm containing numerous punctate vacuoles (Fig. 1 and inset). Nuclei were centrally located with open chromatin and multiple nucleoli. There were frequent bi- and multi-nucleation and variable micronuclei. Cells had numerous criteria of malignancy including a high nuclear-to-cytoplasmic ratio, multinucleation, nuclear molding, moderate anisocytosis and anisokaryosis, and rare mitotic figures.
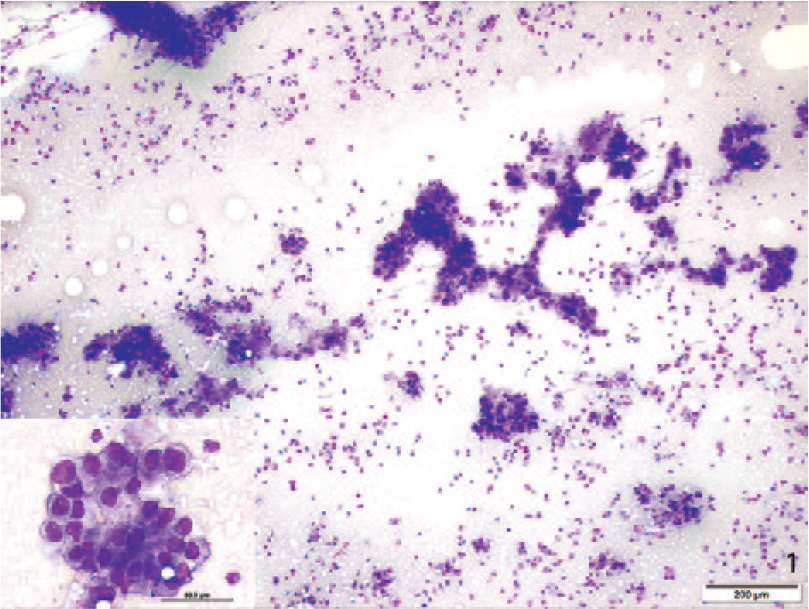
Histiocytic sarcoma in a Cavalier King Charles Spaniel dog. Cytology of fine-needle aspirate from splenic nodule identified on ultrasound. Giemsa. 100×. At low magnification, cells are present in cohesive clusters. Inset: Cells are round to bluntly rectangular with abundant cytoplasm and cytoplasmic vacuoles. 1,000×.
Overall, the cohesiveness of the aggregates and the cell shape were suggestive of a carcinoma. A preliminary differential list included a metastatic pulmonary carcinoma or other metastatic carcinoma, or a primary splenic tumor with epithelioid differentiation.
Because of a poor prognosis and the declining neurologic status of the patient, euthanasia was elected. On autopsy, the spleen contained multifocal 1–2-cm diameter firm nodules with dark discoloration and central tan crumbly debris (Fig. 2a and 2b). Similar 0.5–1-cm nodules were present throughout the lungs. There was a malformation of the caudal fossa of the occipital bone, consistent with Chiari-like malformation, with visualization of the vermis and expansion of the brainstem as a result of edema (Fig. 3).
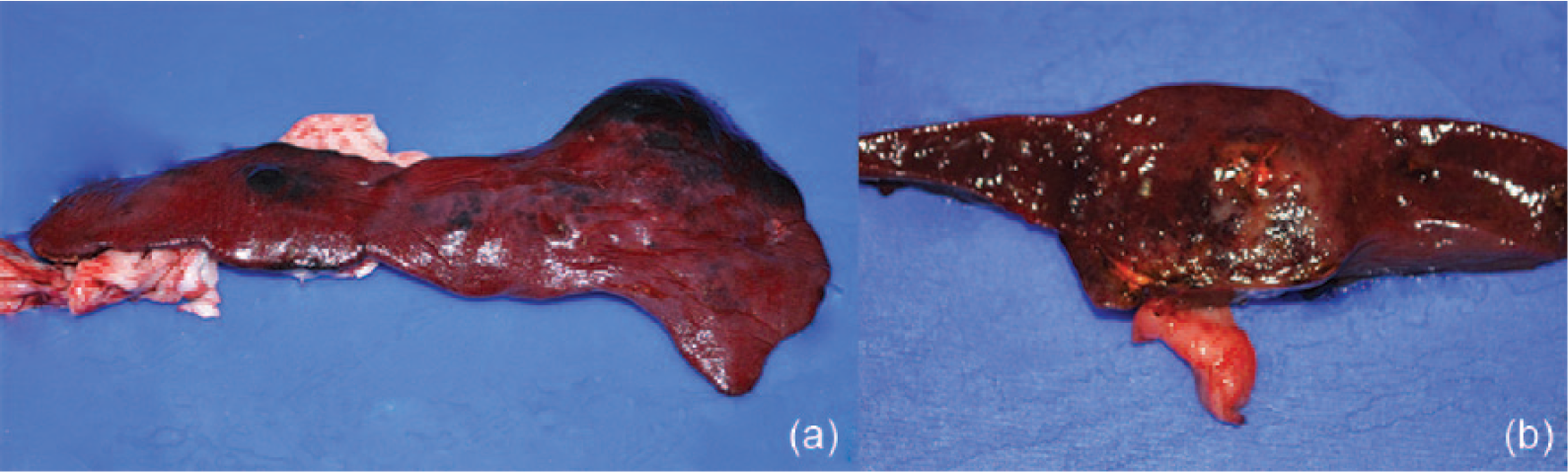
Spleen with multifocal 1–2-cm diameter firm nodules with surrounding hemorrhage and central necrosis (a). Cross-section of a nodule (b).
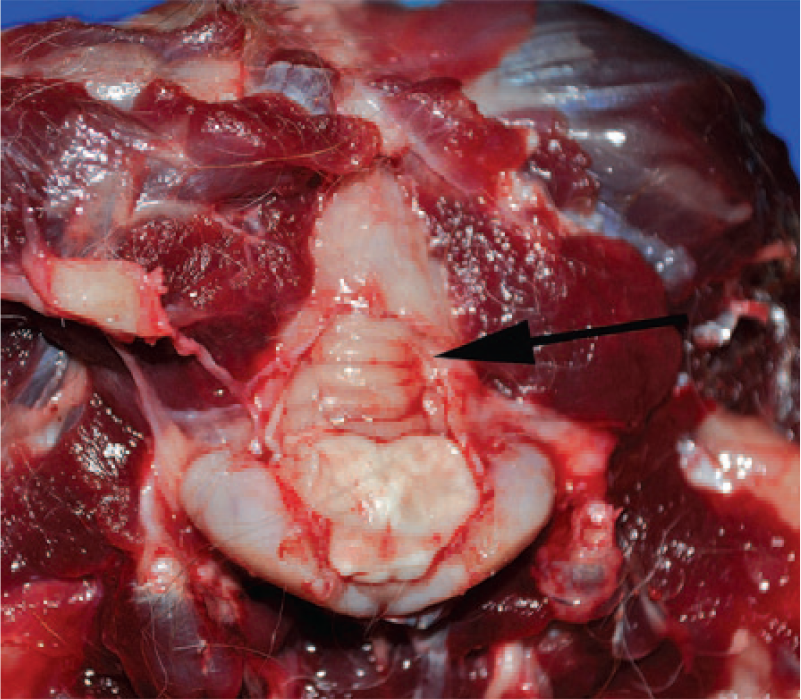
Malformation of the caudal fossa of the occipital bone with visualization of the vermis (arrow). Note expansion of the brainstem by edema.
Histologically, the splenic parenchyma was effaced by a poorly demarcated, unencapsulated, and infiltrative neoplasm. Cells were pleomorphic-to-round and arranged in sheets with fine fibrovascular-to-dense-collagenous stroma, occasionally forming tubular-like structures (Fig. 4). Cells had abundant, granular, eosinophilic cytoplasm. Nuclei were ovoid-to-pleomorphic with open, vesiculated chromatin, and a single prominent nucleolus. Multinucleate cells containing 2–5 nuclei were common (Fig. 4 inset). A high mitotic rate (2 per 400× field) was present along with occasional bizarre mitotic figures. There was compression and loss of red pulp, and lymphoid nodules were hyperplastic.
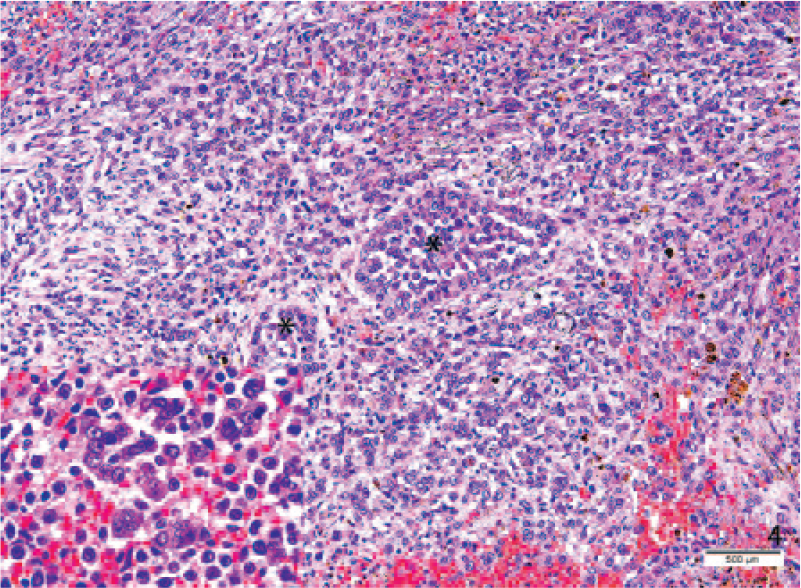
The splenic mass is highly cellular with formation of occasional tubular-like structures (asterisks). Inset: Multinucleated cells with 2–5 nuclei were present throughout the mass. H&E. 400×.
The pulmonary interstitium was multifocally expanded by similar neoplastic cells collapsing and compressing alveoli (Fig. 5). There were increased numbers of fibroblasts and collagen, and the remaining alveoli contained edema fluid and sloughed cells with occasional torn, club-ended septa consistent with emphysema. Collections of plasma cells were present in peribronchiolar areas.
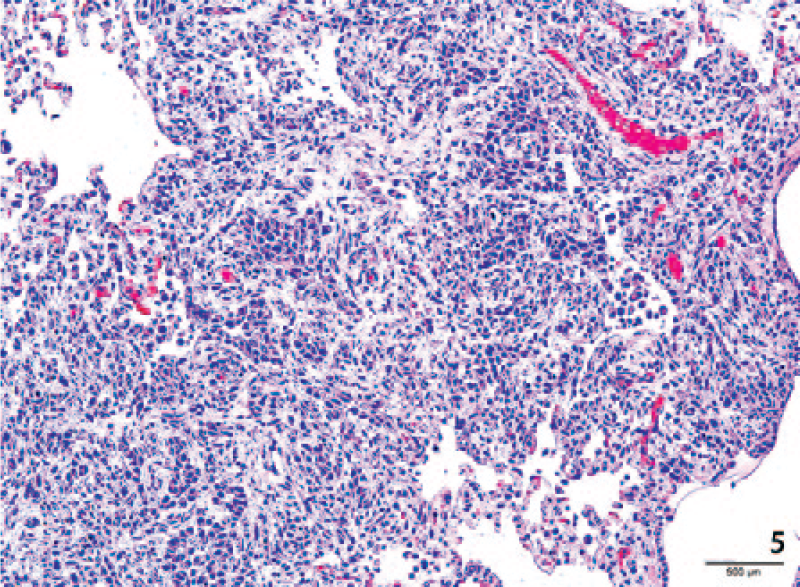
Neoplastic cells expand alveolar septa with compression of pulmonary alveoli. H&E. 200×.
In the adrenal glands, there was bilateral effacement and replacement of 80% of the cortical parenchyma by the neoplastic population, accompanied by infiltrates of plasma cells and fibrosis. Islands of remaining cortical cells were hyperplastic (Fig. 6). There were multifocal areas of hemorrhage and expansion of the capsule with lymphoplasmacytic inflammation and edema.
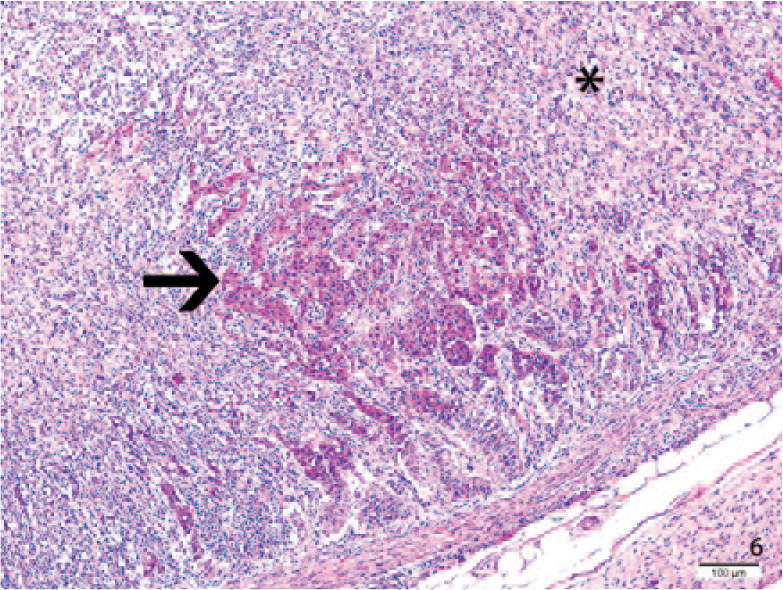
Neoplastic cells (asterisk) efface much of the adrenal gland and surround a focus of cortical hyperplasia (arrow). H&E. 100×.
In the cervical spinal cord, there was mild-to-moderate dilation of the central canal with diffuse axonal swelling and formation of digestion chambers. The gray matter was mildly to moderately compressed with areas of malacia.
Neoplastic cells stained positive for vimentin and cluster of differentiation (CD)18 and negative for cytokeratin A1/E3 and chromogranin A, consistent with histiocytic origin. Further staining for CD3, CD20, and CD11d were also negative, which would be specific for T-cells, B-cells, and splenic macrophages, respectively. Staining for major histocompatibility complex class II (MHC II) was patchy within tumor cells, but ultimately determined to be negative. Heat-mediated antigen retrieval was utilized for all immunohistochemical stains except CD20. Based on the staining pattern, this neoplasm was diagnosed as a disseminated histiocytic sarcoma. Other diagnoses included a Chiari-like malformation of the occipital bone, and corresponding syringomyelia of the cervical spinal cord.
Numerous histiocytic diseases have been described in dogs, including histiocytic sarcomas (arising from either interstitial dendritic cells or macrophages), systemic and cutaneous histiocytosis, and dendritic cell leukemia.1,3 Several breeds, including Bernese Mountain Dogs, Rottweilers, Golden Retrievers, and Flat-Coated Retrievers are predisposed to histiocytic disease because of genetic anomalies. No such anomaly has been described in Cavalier King Charles Spaniels, but tumors can occur sporadically in any breed.1,3 Clinical signs are frequently vague and nonspecific, often depending on the organs involved and the amount of parenchymal destruction.
Histiocytic sarcomas can occur as either localized lesions, such as in the spleen, skin, and subcutis, in the articular tissue of appendicular joints, or can be disseminated with multi-organ involvement. 3 Determining the cell of origin can be difficult using histochemical markers, but most cells express phenotypic profiles consistent with interstitial dendritic cell origin. These cells are positive for CD18, CD1a, CD11c, CD11b, and MHC II.1,3,4 Hemophagocytic splenic histiocytic sarcomas, which arise from splenic macrophages, are positive for CD11d and negative for CD11b. Many of these markers are not assessable on the formalin-fixed tissue that was available in our case, as specific antibodies have only been derived for use on fresh frozen tissue. The patchy MHC II staining exhibited by tumor cells in this dog may be the result of tumor dedifferentiation or alteration of epitopes in the formalin-fixed tissue sections. Given that interstitial dendritic cells are present in almost all tissues, it is difficult to define the origin of the primary mass in this case.
The organs most commonly reported to be affected in dogs with disseminated histiocytic sarcoma are the lung, hilar and mesenteric lymph nodes, liver, spleen, and bone marrow. 1 In a retrospective study, the adrenal glands were involved in 21% of metastatic cancers in dogs, and ~20% of these metastatic adrenal tumors were histiocytic sarcomas. 2 These figures may not be entirely reflective of tumor behavior given that adrenal glands are not always sampled for histologic evaluation. Adrenal metastasis does appear to occur primarily in the late stages of disease when there is multi-organ involvement. Given that many animals with neoplastic disease are euthanized on account of a poor prognosis, adrenal involvement may not have time to develop or adrenal effacement by tumor may not be extensive enough to cause adrenal functional abnormalities. Mild adrenomegaly is difficult to detect on radiographs or ultrasound, possibly leading to further undetected cases. Hypoadrenocorticism resulting from tumor spread has been reported sporadically in animals with metastatic adrenal involvement.2,4
The typical cytologic presentation of a splenic histiocytic sarcoma aspirate is of individually arranged cells with marked anisocytosis and anisokaryosis that are round-to-oval with moderate basophilic cytoplasm and few punctate vacuoles. 5 The cohesiveness, rectangular shape, nuclear blebbing, and relatively mild anisocytosis seen on cytology in our case were atypical for a splenic histiocytic sarcoma. Tumor cells often have a high degree of cellular atypia on cytology, but, in this case, cytologic findings were misleading and led to diagnostic difficulties in determining the tumor type.
Chiari-like malformations, also known as occipital hypoplasia or caudal occipital malformation syndrome, have a 95% prevalence in Cavalier King Charles Spaniels, with syringomyelia occurring in 50% of affected dogs. 6 The proposed pathogenesis for the spinal cord lesion is compression of the subarachnoid space by the defect, resulting in increased cerebrospinal fluid pulse volume, which causes dilation of the spinal cord central canal (hydromyelia). Over time, this leads to cavitation of spinal cord parenchyma. The resulting clinical neurologic condition is progressive, with signs often not being evident prior to 6 mo of age. 6 Affected dogs are often presented with scratching at the back of the neck, ataxia, and fly biting. In the absence of any other lesions in the brain or spinal cord, the neurologic signs in our patient may be attributed in part to syringomyelia. The condition may have been exacerbated by cerebral edema resulting from circulatory disturbances caused by the multicentric neoplasia.
The cytologic presentation of this tumor and nonspecific clinical signs exemplify some of the potential diagnostic difficulties inherent in a case of disseminated histiocytic sarcoma in a dog. Although there is prior evidence of bilateral adrenal metastasis with extensive gland effacement, this feature is often not included in pathology reports given lack of sampling, and we encourage histologic examination of adrenal glands in cases of metastatic neoplasm.
Footnotes
Acknowledgements
Thanks to the University of Georgia Histology and Clinical Pathology Laboratories for processing all tissues and fluid samples.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.