
Abstract
The postmortem examination of a 14-y-old Appaloosa gelding with clinically diagnosed pituitary pars intermedia dysfunction showed a unique finding of moderate multifocal lymphocytic hypophysitis (LH). The pituitary glands of 24 horses submitted for postmortem examination were examined grossly and examined histologically for the presence of lymphocytes. Of these 23 horses, 1 additional case suffered from moderate LH. The 2 cases with LH tested negative for Equid herpesvirus 1 and 4 by polymerase chain reaction and immunohistochemistry (IHC), and no viral particles were observed by electron microscopy in 1 case examined. The cause of LH remains unknown, but based on the T-lymphocytic nature of the inflammation and the human literature, an immune-mediated origin is hypothesized. In addition, the review of 24 cases revealed that 10 horses had few and small multifocal lymphocytic infiltrates within the pituitary gland; the remaining 12 horses showed no evident lymphocytes when examined by hematoxylin and eosin. IHC for CD3 showed the presence of a small number of individual T-lymphocytes scattered through the gland in all examined horses, which appears therefore to be a normal feature of the pituitary gland in horses.
The most common pituitary gland abnormality in horses is associated with increased size and activity of the pars intermedia (PI), which is referred to as pituitary pars intermedia dysfunction (PPID; previously known as equine Cushing’s disease). 14 PPID is considered to be a neurodegenerative disease with loss of inhibitory dopaminergic input that eventually leads to increased PI cell proliferation. Horses with PPID have an enlarged pituitary gland as the result of hyperplasia or benign neoplasia of the PI. 14 The primary cause of PPID has not yet been identified, and a multifactorial origin is suspected. The clinical signs of PPID are broad and include hirsutism, weight loss, change in mentation or behavior, secondary infections, endoparasitism, laminitis, polydipsia and polyuria, and sweating abnormalities. 14
In April 2014, a 14-y-old Appaloosa gelding, with clinically diagnosed chronic laminitis, PPID, and recurrent airway obstruction (RAO), was submitted to the Veterinary Pathology Service of the University of Nottingham (Loughborough, UK) for postmortem examination (horse 1). The only gross abnormality was observed in the pituitary gland, which was moderately reduced in size. This finding was unexpected given the clinical suspicion of PPID. On histologic examination, chronic laminitis and RAO were confirmed. The pituitary gland had moderate multifocal, often perivascular, lymphocytic inflammation in the pars nervosa (PN) with mild involvement of the PI, which was diagnosed as lymphocytic hypophysitis (LH). Uncertain of the significance of the observed LH, 23 more equine pituitary glands were collected and examined for gross and microscopic abnormalities.
Pituitary glands were collected from 23 randomly selected horse and pony autopsy cases performed between April 2014 and October 2015 (Table 1). The case collection includes equids of different breeds, sex, and age (1–28 y). Including horse 1, 24 pituitary glands were assessed grossly and histologically by 2 European College of Veterinary Pathologists board-certified veterinary pathologists. Owner’s consent was obtained prior to submission of the horses for postmortem examination. Histologic assessment was done blindly. For those samples for which there was no agreement, a consensus was reached after reexamining and discussing the cases. Of each pituitary gland, 1–3 sagittal sections were cut and routinely processed for histology and stained with hematoxylin and eosin (H&E). The tissue was assessed for the presence of lymphocytes, and the animals were classified into group 1 (moderate lymphocytic infiltrates), group 2 (mild lymphocytic infiltrates), or group 3 (no evident lymphocytes). Additionally, the glands were assessed for other non-inflammatory histologic features (i.e., the presence of colloid-filled dilated follicles in the PI, PI hyperplasia, and intracytoplasmic brown granular pigment in pituicytes). These features were semiquantified, in order to assess a potential association of those lesions with the lymphocytic infiltrates (Table 2). Several sections of brain from all cases were thoroughly examined histologically.
Data and main autopsy findings from horses included in the study. Pituitary pars intermedia dysfunction (PPID) column indicates if clinical evidence of PPID was reported in the clinical history.*
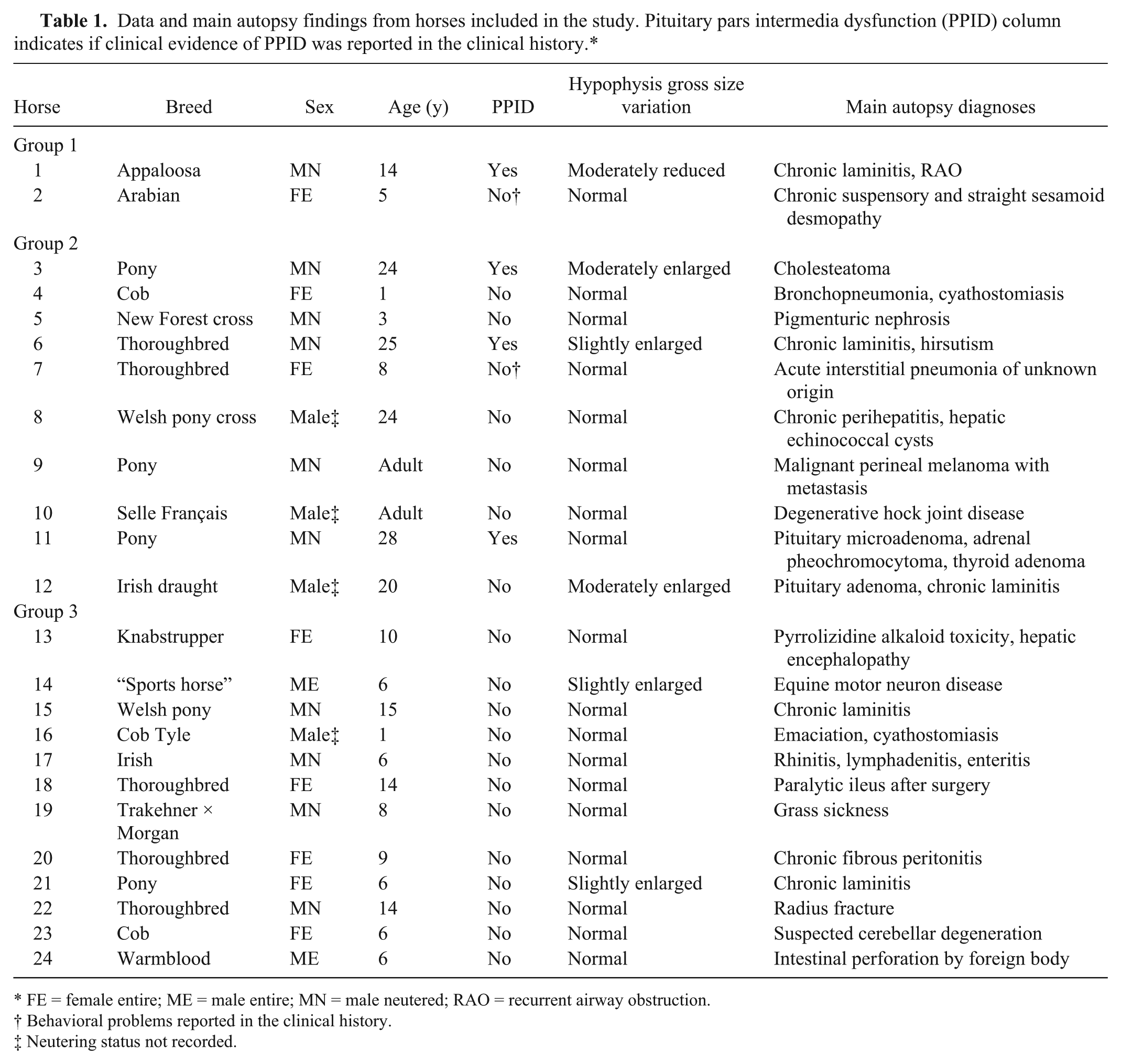
FE = female entire; ME = male entire; MN = male neutered; RAO = recurrent airway obstruction.
Behavioral problems reported in the clinical history.
Neutering status not recorded.
Histologic lesions within pituitary gland, and immunohistochemistry (IHC) for CD3 and CD79a.*
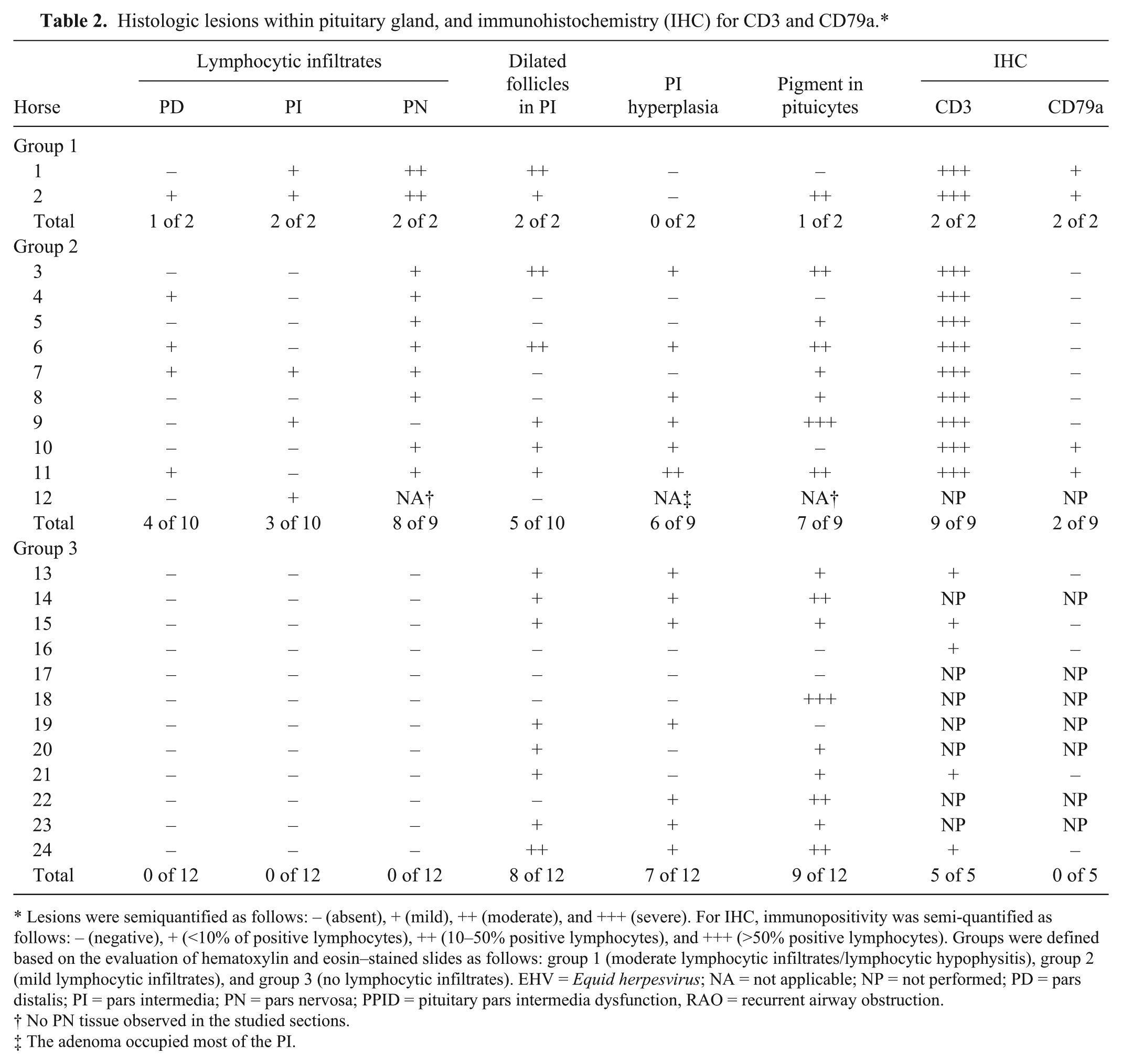
Lesions were semiquantified as follows: – (absent), + (mild), ++ (moderate), and +++ (severe). For IHC, immunopositivity was semi-quantified as follows: – (negative), + (<10% of positive lymphocytes), ++ (10–50% positive lymphocytes), and +++ (>50% positive lymphocytes). Groups were defined based on the evaluation of hematoxylin and eosin–stained slides as follows: group 1 (moderate lymphocytic infiltrates/lymphocytic hypophysitis), group 2 (mild lymphocytic infiltrates), and group 3 (no lymphocytic infiltrates). EHV = Equid herpesvirus; NA = not applicable; NP = not performed; PD = pars distalis; PI = pars intermedia; PN = pars nervosa; PPID = pituitary pars intermedia dysfunction, RAO = recurrent airway obstruction.
No PN tissue observed in the studied sections.
The adenoma occupied most of the PI.
To further characterize the pituitary lymphocytic inflammation, immunohistochemistry (IHC) for CD3 (rabbit polyclonal anti-human, a dilution 1:400) and CD79a (mouse monoclonal anti-human, b dilution 1:400) was performed in 2 of 2 horses from group 1, 9 of 10 horses from group 2 (excluding horse 12 with PI adenoma), and 5 of 10 horses from group 3 (Table 2). The 5 horses from group 3 were selected with the aim of including a broad range of ages (1–15 y old). In order to rule out Equid herpesvirus (EHV) infection, an IHC for EHV-1 (rabbit polyclonal anti-equine, c dilution 1:750) was performed on formalin-fixed, paraffin-embedded (FFPE) pituitary gland tissue from horses 1–3. Following previously reported protocols, a multiplex real-time polymerase chain reaction (PCR) for the detection of EHV-1 5 and -4 6 was performed on FFPE pituitary gland tissue from horses 1–3.
Pituitary gland tissue of horse 1 was examined by transmission electron microscopy (TEM). FFPE tissue was deparaffinized and postfixed in 2.5% glutaraldehyde, osmium tetroxide, and uranyl acetate, and then embedded in resin. Ultrathin (70 nm) sections were then contrasted with lead citrate and scanned thoroughly.
Statistical software d was used for statistical analysis. The distribution of the age variable was assessed by the Shapiro–Wilk test. Kruskal–Wallis and Mann–Whitney tests were used to compare means of age between groups. Fisher exact test was used to compare the proportion of animals from each sex category and the proportion of animals showing presence and absence of dilated follicles in PI, PI hyperplasia, and pigment in pituicytes between the groups in pairs.
Four of 24 (17%) horses were submitted with clinical suspicion of PPID (Table 1), based on clinical signs and/or elevated basal plasma adrenocorticotropic hormone (ACTH) concentrations. ACTH levels were measured in 3 of the 4 suspected PPID cases, which were compared to seasonally adjusted reference values. Horse 1 had a mildly increased plasma ACTH level of 7.17 pmol/L (June 2012; reference: <6.38 pmol/L) 23 m before postmortem examination. In horse 3, a severely increased basal ACTH concentration of 41.36 pmol/L (reference: <6.38 pmol/L) was measured in April 2014, the day before the autopsy was performed. In horse 6, plasma ACTH levels were measured 4 times between September 2012 and March 2014. The initial ACTH concentration was markedly increased (20.32 pmol/L, September 2012; reference: <10.34 pmol/L). The 3 following ACTH measurements were normal (January 2013: 4.22 pmol/mL; June 2013: 4.93 pmol/L) to mildly increased (February 2014: 7.83 pmol/L), which were last measured 3 m before autopsy. Two of the 4 horses with clinically diagnosed PPID (horses 1 and 6) were intermittently treated with the synthetic dopamine-agonist pergolide e (one 1-mg tablet orally, daily) over several months. In addition, horses 2 and 7 had a history of behavioral problems, including increased frequency of urination in the latter.
Grossly, 5 of 24 pituitary glands were mildly to moderately enlarged (Supplemental Figs. 1, 2). The gland of horse 1 was reduced in size with a discoid shape (3 × 2.5 × 1 cm), leaving a partially empty sella turcica (Supplemental Fig. 3). The remaining 18 horses had grossly normal pituitary glands (Supplemental Fig. 4; Table 1). Of 24 horses, 2 horses (1 and 2) had moderate and multifocal lymphocytic infiltrates within the pituitary gland, and were classified as group 1 (lymphocytic hypophysitis). Ten horses (3–12) had mild multifocal lymphocytic infiltrates within the pituitary gland, and were classified as group 2. The remaining 12 horses had no evident lymphocytes when examined by H&E (group 3; Table 2). No other leukocytes (e.g., plasma cells, macrophages, or granulocytes) were observed within the studied pituitary glands. The 3 groups contained horses and/or ponies of different breeds, sex, and age (Table 1). The mean age was 9.5 (± standard deviation [SD] 6.4), 16.6 (± SD 10.8) and 8.4 (± SD 4.2) y in group 1, 2, and 3, respectively. The age variable was shown to be non-normally distributed (p = 0.031), and Kolmogorov–Smirnov test indicated that horses from group 2 were significantly older than group 3 (p < 0.047), although the Mann–Whitney test indicated only a statistical trend (p = 0.135). No other statistically significant differences were found.
In the 2 cases included in group 1, the lesions were considered sufficient to diagnose LH. The lymphocytic aggregates were multifocal, usually around small vessels, and mainly located within the PN, with fewer within the PI in both cases (Fig. 1) but also in the pars distalis (PD) in horse 2. These 2 horses showed no hyperplasia or adenoma within the PI (Table 2). In group 2, lymphocytic aggregates were observed in the PN in 10 of 11, the PI in 5 of 12, and the PD in 5 of 12 horses. Two horses (11 and 12) with mild lymphocytic infiltrates also had PI adenomatous hyperplasia with a microadenoma and a PI adenoma, respectively. The adenoma occupied most of the PI, expanding into adjacent pituitary lobes, with no remaining PN tissue in the studied sections. Dilated follicles in the PI (Fig. 2) and pigment within pituicytes were commonly seen in all 3 groups, showing therefore no association with the presence of lymphocytes. PI hyperplasia was frequent in groups 2 (6 of 9 horses) and 3 (7 of 12 horses). No evidence of inflammation was present in any of the brain sections examined.
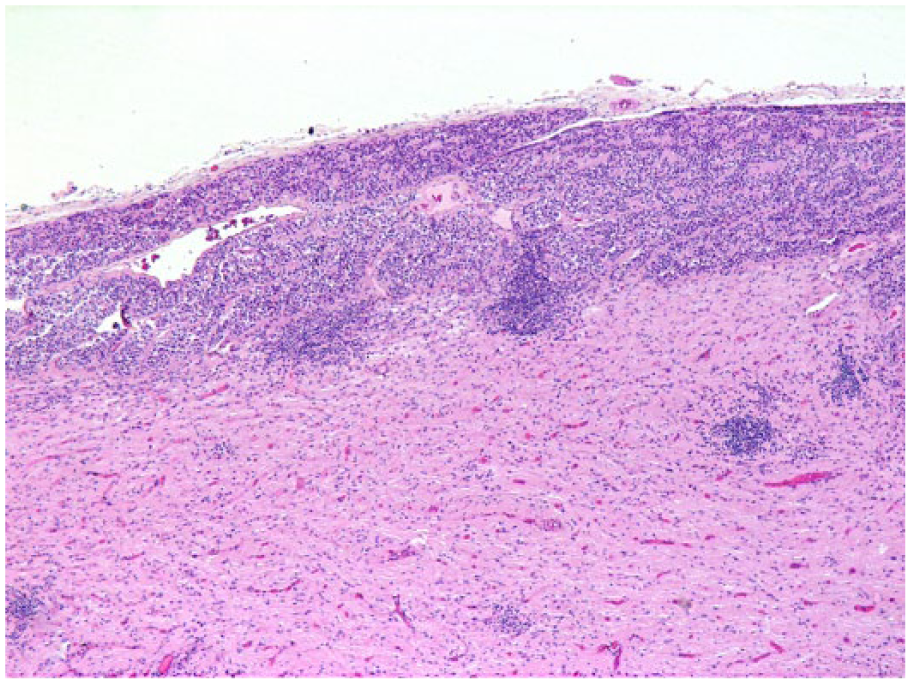
Pituitary gland with lymphocytic hypophysitis (group 1), horse 1. Moderate multifocal lymphocytic aggregates are present within the pars nervosa and pars intermedia. Hematoxylin and eosin.
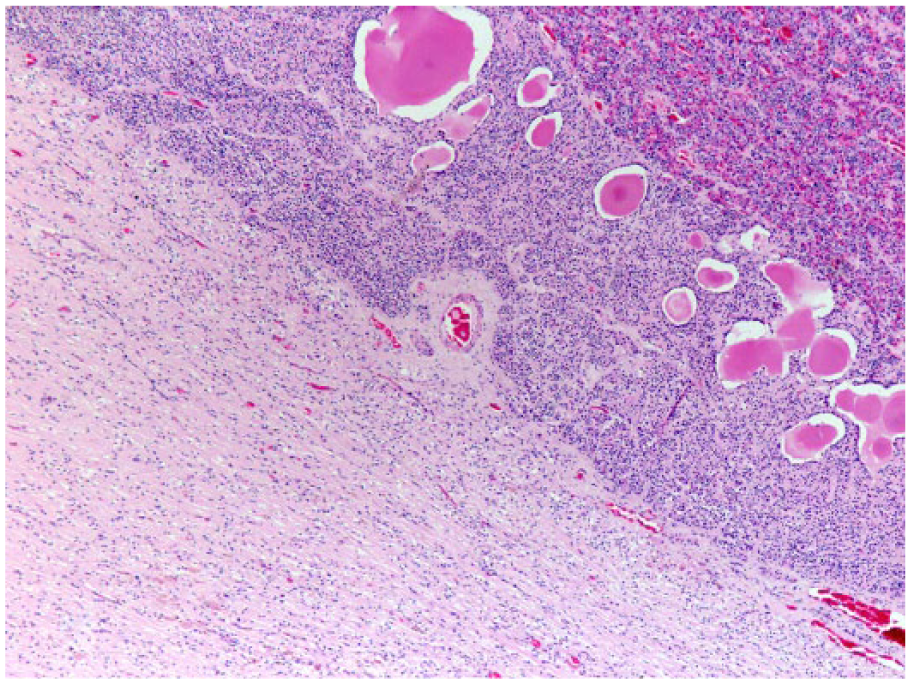
Pituitary gland without lymphocytes visible on H&E (group 3), horse 24. Moderate numbers of dilated colloid-filled follicles are present within the pars intermedia.
In all of the examined horses with lymphocytic infiltrates within the pituitary gland, most lymphocytes (>50% in the studied sections) were CD3+, being therefore compatible with T-lymphocytes (Fig. 3). In 2 of 2 horses of group 1 and 2 of 9 horses of group 2, a very low number of lymphocytes were CD79a+ (Fig. 4).The 5 horses studied from group 3, with no evident lymphocytic infiltrates on H&E, had a low number of individual CD3+ lymphocytes, regularly scattered throughout the PN, PI, and PD (Fig. 5).
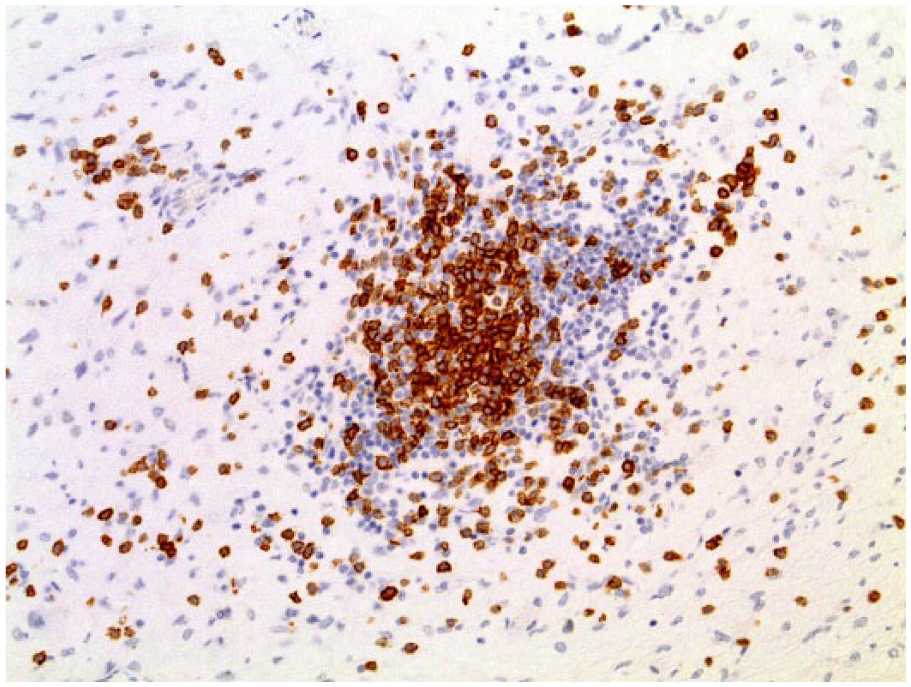
Pituitary gland with lymphocytic hypophysitis (group 1), horse 1. The majority of the lymphocytes show intense cytoplasmic labeling. Immunohistochemistry for CD3.
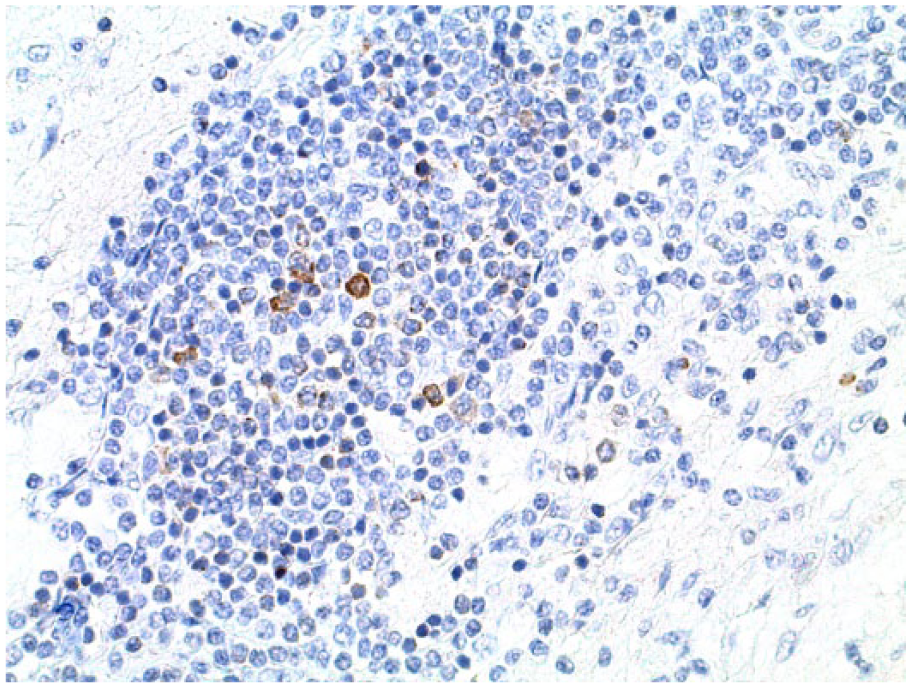
Pituitary gland with lymphocytic hypophysitis (group 1), horse 1. Low numbers of lymphocytes show cytoplasmic labeling. Immunohistochemistry for CD79.
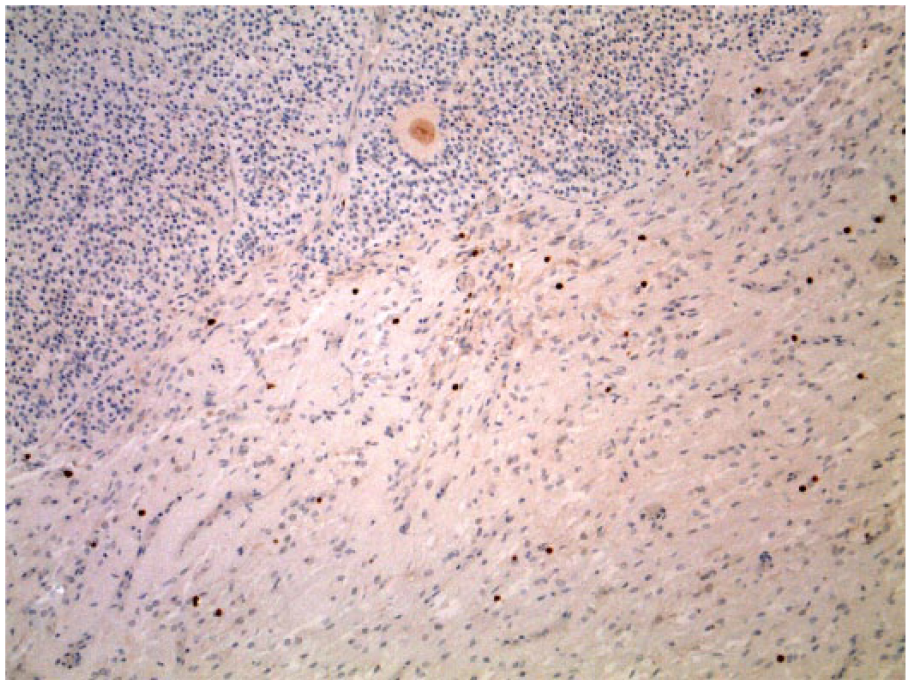
Pituitary gland without lymphocytes visible on H&E (group 3), horse 13. Low numbers of individual, scattered lymphocytes with cytoplasmic labeling are present within pars nervosa and pars intermedia. Immunohistochemistry for CD3.
Horses 1 and 2 with LH and horse 3 from group 2 were tested for infection with EHV-1 and -4 by PCR and IHC, which gave negative results. In addition, horse 1 was also examined by TEM, which confirmed the presence of lymphocytes, but lacked evidence of viral particles (Fig. 6).
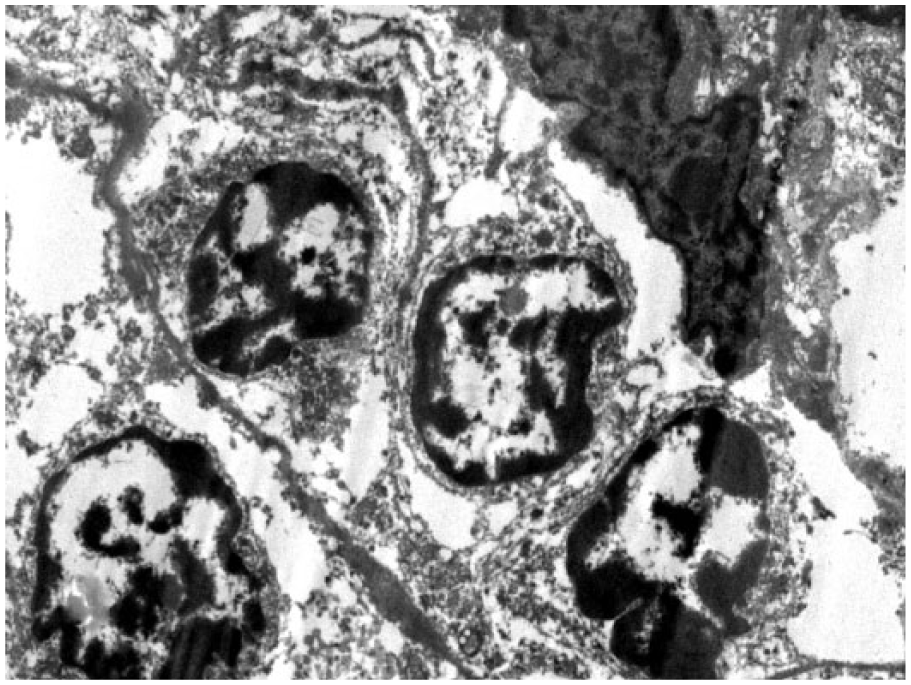
Pituitary gland with lymphocytic hypophysitis, horse 1. Four lymphocytes are seen adjacent to an endothelial cell. Transmission electron micrograph.
As far as we are aware, natural cases of primary hypophysitis in animals have only been reported in dogs,1,4,13,15,20 and in a cat. 18 In humans, hypophysitis is a rare condition with frequencies of <1% of surgical pituitary cases.8,10 Primary hypophysitis in humans comprises 3 distinct histomorphologic entities: lymphocytic (the most common), granulomatous, and xanthomatous.8,10 It can be acute, subacute, or chronic, with symptoms compatible with those of a pituitary mass, and is included in the differential diagnosis in cases of pituitary dysfunction.8,10 LH in people is reported to often lead to enlargement of the pituitary gland but, interestingly, people with chronic LH often have pituitary atrophy. 8 Our horse 1 showed an apparently smaller pituitary gland, which may correspond to a similar situation, although no evidence of fibrosis, as described in humans, was observed histologically. 8 Horse 2 had no obvious gross variation in the size of the pituitary gland. However, slight changes in size of the pituitary glands are difficult to appreciate. The use of previously reported methods measuring height, weight, and PI area,17,19 not performed in our study, would have minimized subjective evaluation. Histologically, the nature of the lesions in both horses with LH was similar to the ones reported in the human literature in cases of primary LH, consisting of multifocal lymphocytic aggregates, predominantly of T-lymphocytes with sparse numbers of B-lymphocytes. 9 However, although in humans the adenohypophysis is reported to be the area most affected, the main lesions in both LH-affected horses was in the PN, with only mild aggregates of lymphocytes present within the PD and/or PI. Moreover, although the presence of plasma cells is usually described in human cases, they were not present in our 2 horses. 9 No evidence of infectious agents was found in the brain or pituitary glands of the studied horses, indicating that the LH was primary. 10 IHC and PCR testing for EHV was negative in both horses, and examination of horse 1 by TEM failed to show any viral particles. Therefore, the cause of LH in both horses remains unclear. In humans, LH etiology is unclear, but is suspected to be autoimmune. 8 Based on the T-lymphocytic nature of the observed inflammation and the information available from humans, an immune-mediated origin is hypothesized for our equine cases.
Because of the novelty of the pituitary lesions, their detection in only 2 cases, and the limited clinical information available, it is difficult to correlate the LH with the clinical signs or other lesions observed in the postmortem examination. Horse 1 was submitted for autopsy with a clinical suspicion of PPID, based on mildly increased plasma levels of ACTH determined ~2 y before. However, the ACTH elevation must be interpreted cautiously because of the long lapse of time between the last ACTH determination and the autopsy, the well-known ACTH seasonal variations, and potential increases of ACTH concentration as the result of other factors such as stress and/or pain.2,3,7 In humans, ACTH concentrations are usually reduced in cases of hypophysitis. 16 As well, ACTH concentrations were not measured in the second horse affected with LH, and it did not have a clinical diagnosis of PPID. However, this horse was reported to suffer from behavioral problems, one of the clinical signs reported with PPID. 14 Regarding other lesions observed during postmortem examination, horse 1 had chronic laminitis, and horse 2 suffered from a chronic desmopathy; both conditions have been associated with PPID.11,14 Interestingly, however, neither of the 2 cases had adenoma or hyperplasia of the PI. In addition, one of the horses was young (5 y), whereas the other was middle aged (14 y), suggesting no relation with the observed lesion and aging.
Given the importance of the pituitary gland in horses, further studies including a large number of horses with well-known clinical diagnosis (including PPID-affected horses and nonaffected horses with known ACTH concentrations) are needed to understand the clinical importance as well as the frequency of occurrence of this condition. Current preliminary results indicate that LH occasionally occurs in horses, and suggest that it may be worth reassessing a large number of paraffin-embedded pituitary tissues for the presence of LH.
The presence of small aggregates of lymphocytes within the pituitary gland was a frequent finding visible by H&E (10 horses [42%], group 2). These infiltrates were demonstrated to consist of mainly T-lymphocytes by IHC. Three of the animals included in this group had a clinical diagnosis of PPID. However, this diagnosis can be well explained because of the presence of 1 pituitary adenoma (horse 11) and hyperplasia of the PI (horse 3 and 6). Remarkably, in the animals with no lymphocytic infiltrates evident on H&E (group 3), a low number of individual T-lymphocytes were observed scattered through the pituitary parenchyma when using IHC. The observation of aggregates of lymphocytes within the pituitary gland (group 2) and of individual scattered T-lymphocytes (group 3) was similar regardless of sex and the presence of other histologic changes in the pituitary gland. However, the animals within group 2 had a higher mean age than the horses within group 3. These results suggest that the presence of a few scattered T-lymphocytes within the equine pituitary gland is a normal finding, and that these may form small aggregates visible on H&E with increasing age. As far as we are aware, the presence of T-lymphocytes within normal pituitary glands has not been reported previously in horses but is described as a normal finding in people. 12
Footnotes
Acknowledgements
We thank Bridge Pathology Ltd. in Bristol, UK (director Dr. Tim Scase) and Animal Health Trust, Pathology, in Newmarket, UK, for performing the IHC. We thank Ms. Natalie Allcock from Leicester University, UK for performing the electron microscopy and Alan Lasslett for his excellent technical assistance.
Authors’ contributions
L Grau-Roma and S de Brot contributed to conception and design of the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; and gave final approval. R Peckham contributed to conception of the study; contributed to acquisition, analysis, and interpretation of data; and critically revised the manuscript. J Paton contributed to acquisition, analysis, and interpretation of data, and critically revised the manuscript. A Stahel contributed to analysis and interpretation of data, and critically revised the manuscript. All authors agreed to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
a.
Dako UK, Cambridgeshire, United Kingdom.
b.
Dako UK, Cambridgeshire, United Kingdom.
c.
Produced in-house by Animal Health Trust, Newmarket, Suffolk, United Kingdom.
d.
SPSS version 22, SPSS, Chicago, IL.
e.
Prascend (pergolide mesylate), Boehringer Ingelheim Vetmedica, St. Joseph, MO.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L Grau-Roma’s research has received funding from the People Programme (Marie Curie Actions) of the European Union’s Seventh Framework Programme (FP7/2007-2013) under REA grant agreement PCOFUND-GA-2012-600181.