
Abstract
A 13-year-old Quarterhorse mare had a 6-month history of diarrhea, progressive weight loss, and lethargy. At presentation the mare was hirsute, had hyperhidrosis, and abnormal fat distribution in addition to severe diarrhea. A presumptive clinical diagnosis of protein-losing enteropathy and pituitary pars intermedia dysfunction was made. T-cell lymphoma was diagnosed in a rectal biopsy specimen. The owner elected to euthanize the mare because of poor prognosis and the severity of the disease. At necropsy, the mare had hypertrichosis and the pituitary gland was diffusely enlarged. Histologically, neoplastic lymphocytes infiltrated the gastrointestinal mucosa, mesenteric lymph nodes, and the pituitary gland. In addition, there was hyperplasia of the pituitary gland pars intermedia. Pituitary adenoma was not present. Hypertrichosis in this case could have been triggered by a combination of adenomatous hyperplasia of pars intermedia and lymphoma resulting in disruption of the hypothalamic dopaminergic tone or disruption of the hypothalamic thermoregulatory center.
Lymphoma accounts for 0.2 to 3.0% of equine neoplasms. 10 The small intestine is more commonly affected than the large intestine in the alimentary form 7,14,15,18 with secondary involvement of the liver 18 and mesenteric lymph nodes. 15 Clinical signs are usually nonspecific and include weight loss, anorexia, malabsorption, and chronic diarrhea. 7,14 Equine alimentary lymphoma is usually of T-cell origin. 7,14 Although equine lymphoma involving central nervous system has been documented sporadically, 11 such tumor in the pituitary gland has not been reported. This report describes the clinicopathologic findings in a horse with alimentary lymphoma and pituitary involvement.
A 13-year-old Quarterhorse mare was presented to the Purdue University Veterinary Teaching Hospital for evaluation of chronic diarrhea and hirsutism. The mare had a 6-month history of watery diarrhea, progressive weight loss, thargy, and weakness in the hind limbs. At presentation the mare had a normal temperature (37.5°C), was tachycardic (60 beats/minute), and was mildly tachypneic (32 breaths/minute). It had a long, thick, wavy hair coat, and moderate muscle wasting. Oral mucous membranes were slightly pale with normal capillary refill time. Rectal examination was within normal limits. Increased breath sounds were ausculted in the dorsal lung fields. The mare's age, physical examination findings, and history of chronic cough suggested recurrent airway obstruction. The mare was mildly ataxic. Complete blood count showed lymphopenia (0.47 × 107μl; reference range, 1.5-5.5 × 10 3 /μI) that was likely glucocorticoid-induced either from stress or in response to pituitary pars intermedia dysfunction (PPID). Serum chemistry showed hypoproteinemia (4.8 g/dl; reference range, 4.7-7.5 g/dl), hypoalbuminemia (1.8 g/dl; reference range, 2.5-3.8 g/dl), hypocalcemia (10.1 mg/dl; reference range, 10.7-13.4 mg/dl), hyponatremia (129 mmol/l; reference range, 132–144 mmol/l), hypomagnesemia (1.3 mg/dl; reference range, 1.6-2.7 mg/dl), and decreased anion gap (4.0 mmol/l; reference range, 12–20 mmol/l). These abnormalities were consistent with a diagnosis of protein-losing enteropathy. The mild hypocalcemia and decreased anion gap were likely caused by hypoalbuminemia. Fecal culture was negative for bacterial pathogens. Because of the chronic diarrhea, weight loss, and hypoalbuminemia, a presumptive diagnosis of protein-losing enteropathy was made. PPID was suspected because of hypertrichosis, hyperhidrosis, and abnormal fat distribution, but further diagnostics for PPID were not performed.
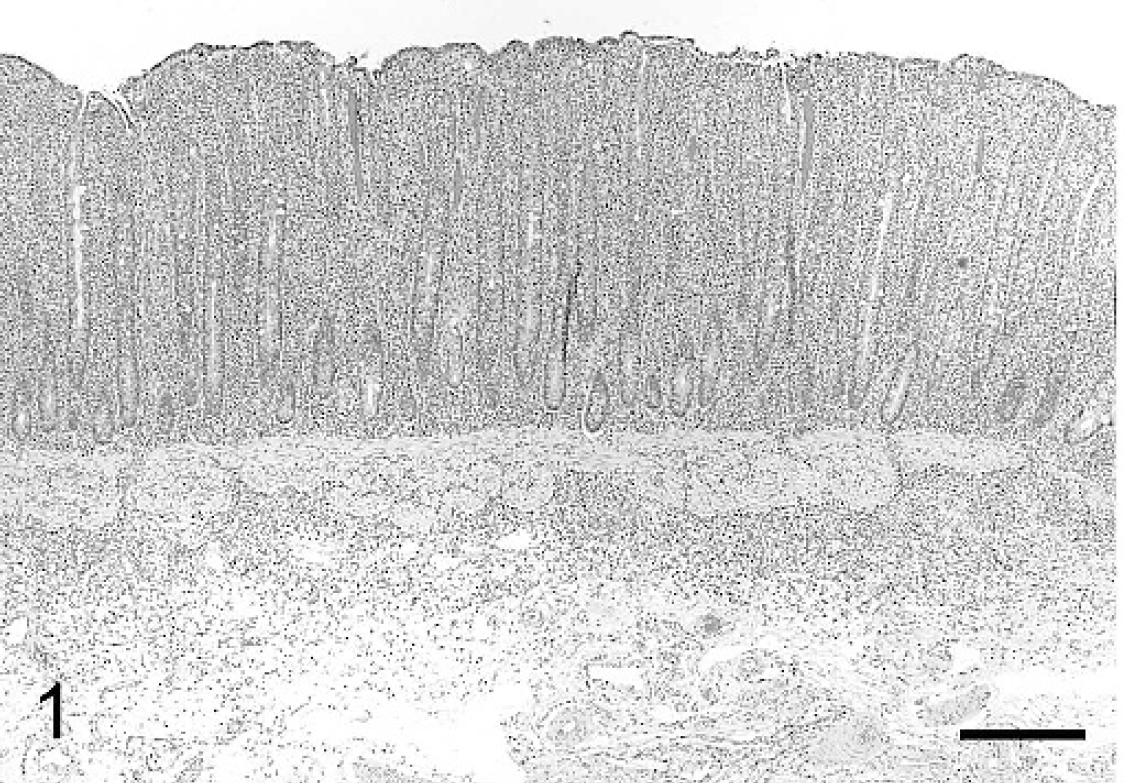
Rectal biopsy sample, horse. The lamina propria is expanded by a proliferation of round cells. The same cells infiltrate the superficial submucosa. Hematoxylin and eosin (HE) stain. Bar = 750 μm.
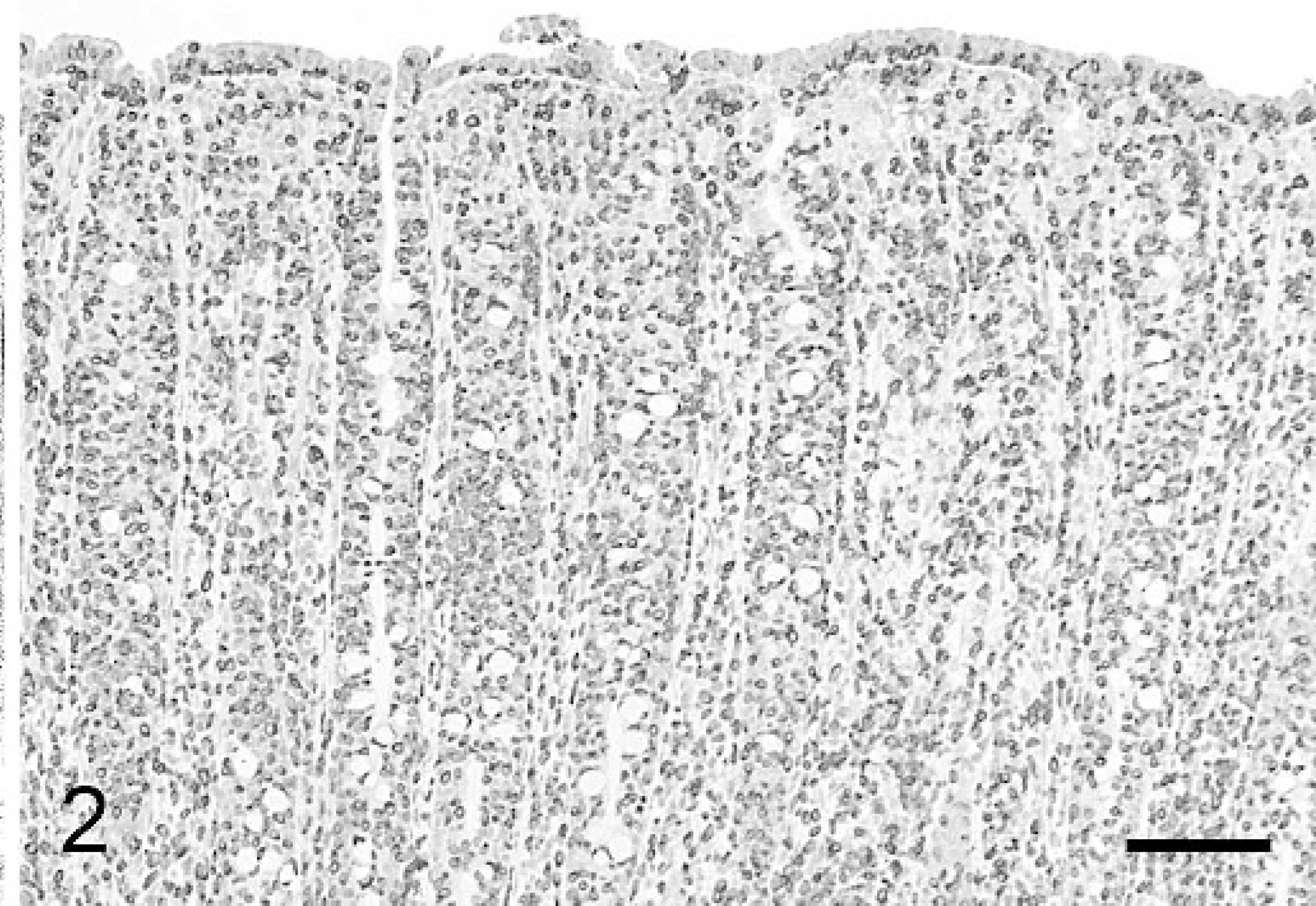
Rectal biopsy sample, horse. Neoplastic lymphocytes are intensely positive for CD3. Immunoperoxidase for CD3, Mayer's hematoxylin counterstain. Bar = 300 μm.
A rectal biopsy using uterine biopsy forceps was taken. Histologically, the lamina propria was mildly expanded by a proliferation of round cells consistent with small and medium-to-large sized lymphocytes with stippled to coarse chromatin, round nuclei, and occasional nuclear membrane indentation (Fig. 1). Nucleoli were usually not apparent. Lymphocytes also infiltrated the epithelium and sometimes obscured the boundaries of glands. Nests of lymphocytes within the epithelium were visible in some glands. Plasma cells or plasmacytoid cells were rarely seen. A similar lymphoid infiltrate was present in the submucosa. Mitotic activity was not observed. Immunohistochemistry was performed for CD3 (A0452, T-cell marker), a CD20 (RB-9013, B-cell marker), b and CD79a (M7051, B-cell marker) a antigens following a published protocol. 16 Antigen retrieval was done for CD3 (decloaker with citrate buffer, pH 6.0) and CD79a (decloaker with EDTA buffer, pH 9.0). Antigen retrieval was not done for CD20. The majority (>95%) of lymphocytes infiltrating the lamina propria and submucosa were CD3-positive and CD20- and CD79a-negative, consistent with T-cell lymphoma (Fig. 2).
The mare was treated with 40 mg of dexamethasone intramuscularly every 3 days. Because alimentary lymphoma has a poor prognosis the owner elected euthanasia of the mare after only 2 treatments with dexamethasone.
Significant findings at necropsy included long and shaggy hair over the entire body. The lungs failed to collapse, were mottled yellowish gray and red, and were edematous. The pituitary gland was enlarged, measuring 2.9 × 2.5 × 2.3 cm, and bulging from the plane of the diaphragma sellae (Fig. 3). On cut section, the pituitary gland was homogeneously tan, without clear demarcation among the pars nervosa, pars intermedia, and pars anterior (Fig. 4).
Selected tissues were fixed for approximately 36 hours in 10% buffered formalin and embedded in paraffin. Five-micrometer sections were stained with hematoxylin and eosin (HE). Histological examination of the large intestine (cecum, colon, and rectum) revealed marked mucosal expansion caused by infiltration by numerous neoplastic lymphocytes and occasional plasma cells and edema. Neoplastic lymphocytes were mostly small to medium sized, but occasionally large, with round to ovoid nuclei, coarsely stippled or sparse chromatin, occasional nuclear indentation, and inconspicuous nucleoli. Mitotic index was 2 to 3 per 400X (magnification) field. Intestinal epithelium was diffusely hyperplastic and multifocally infiltrated by neoplastic cells. Neoplastic lymphocytes extended multifocally into the submucosa. Alterations in the small intestine (duodenum, jejunum, and ileum) and stomach (pylorus) resembled those in large intestine, but infiltrates were less intense and submucosal involvement was minimal. The architecture of the mesenteric lymph nodes was disrupted by infiltration of neoplastic lymphocytes. All segments of the pituitary gland were markedly expanded and effaced by neoplastic lymphocytes (Fig. 5). The pars intermedia had indistinct nodules of hypertrophied cells with mild nuclear pleomorphism (adenomatous hyperplasia) (Fig. 6). There was focal necrosis as well as a few, 1 × 0.5 mm, irregularly shaped cysts filled with eosinophilic or amphophilic colloid and cell debris. The meninges lining the hypothalamus were infiltrated by neoplastic lymphocytes. However, involvement of the hypothalamus by this neoplastic growth was minimal. Immunohistochemically, more than 90% of neoplastic lymphocytes in the pituitary gland were positive for CD3 but negative for CD20 and CD79a (Figs. 7 and 8), confirming the previous diagnosis of T-cell lymphoma.
This mare had alimentary T-cell lymphoma. Most equine alimentary lymphomas are of T-cell origin, 7,14 although a case of B-cell alimentary lymphoma has been reported. 18 In dogs, alimentary lymphoma is usually of T-cell origin. 4 In cats, alimentary lymphomas are predominantly of B-cell type. 3,23
Primary lymphoma of the pituitary gland has rarely been reported in human medicine. 1,17 Immunohistochemically, all human cases were classified as large B-cell lymphoma. Two cases were associated with clinical signs and laboratory data supporting a diagnosis of hypopituitarism. 1,17 One of these cases had concurrent pituitary adenoma. 1 Pituitary lymphoma has not been documented in animal species. The present case had microscopic features compatible with pituitary pars intermedia adenomatous hyperplasia although this assessment was difficult because of the diffuse lymphoid infiltrate. To the authors' knowledge, this case is the first report of primary or secondary pituitary lymphoma in a horse. While pituitary adenomas and adenocarcinomas are not uncommon in domestic animals, metastatic tumors to the pituitary gland are rare, with 1 report of mastocytoma in a dog. 6 A case was reported of epitheliotropic T-cell lymphoma infiltrating the hypothalamus and optic chiasm of a dog, but the pituitary gland was not affected. 5
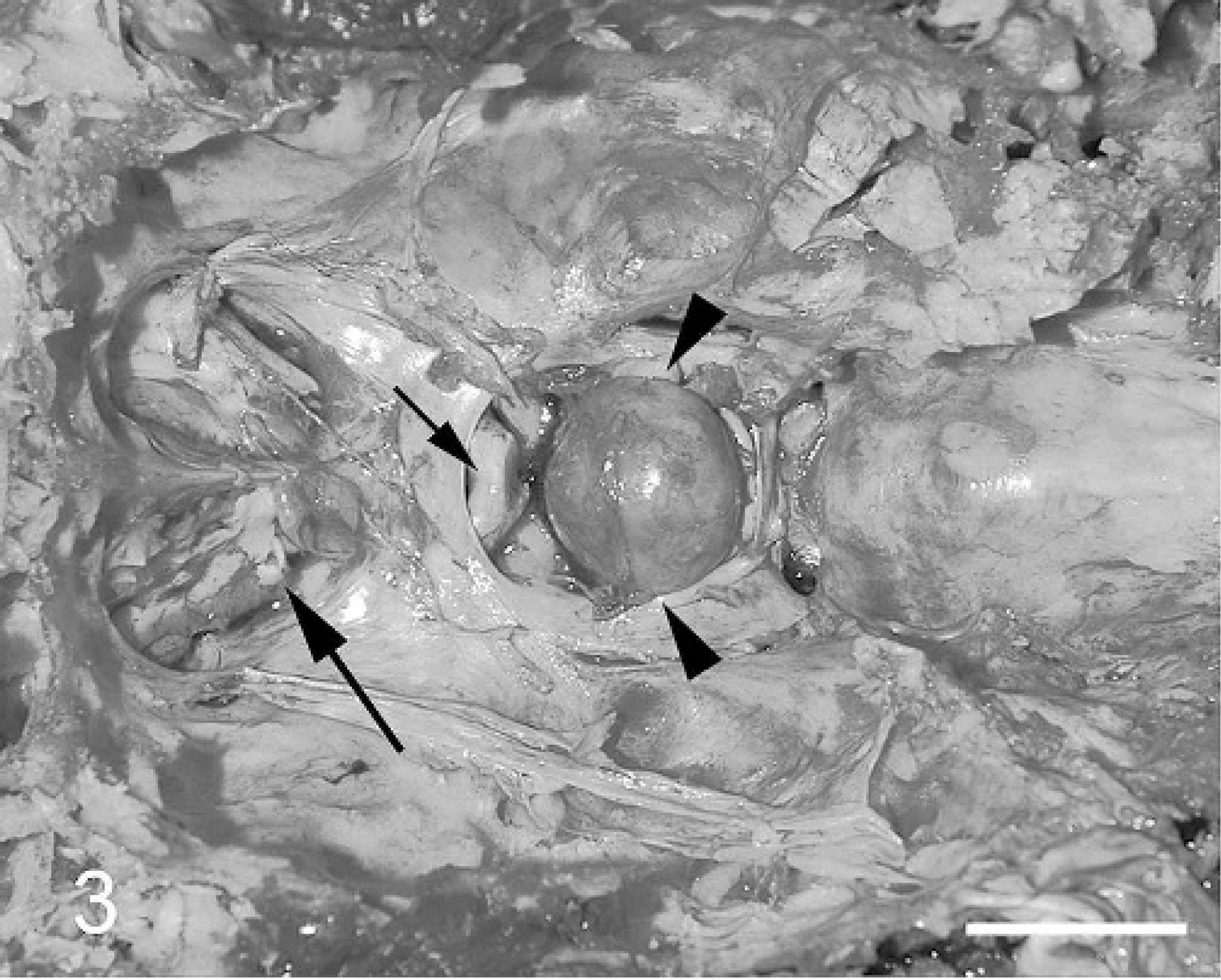
In situ appearance of the pituitary gland, horse. The pituitary gland (arrowheads) bulges from the diaphragma sellae. Optic chiasm (small arrow). Olfactory bulbs (large arrow). Bar = 3 cm.
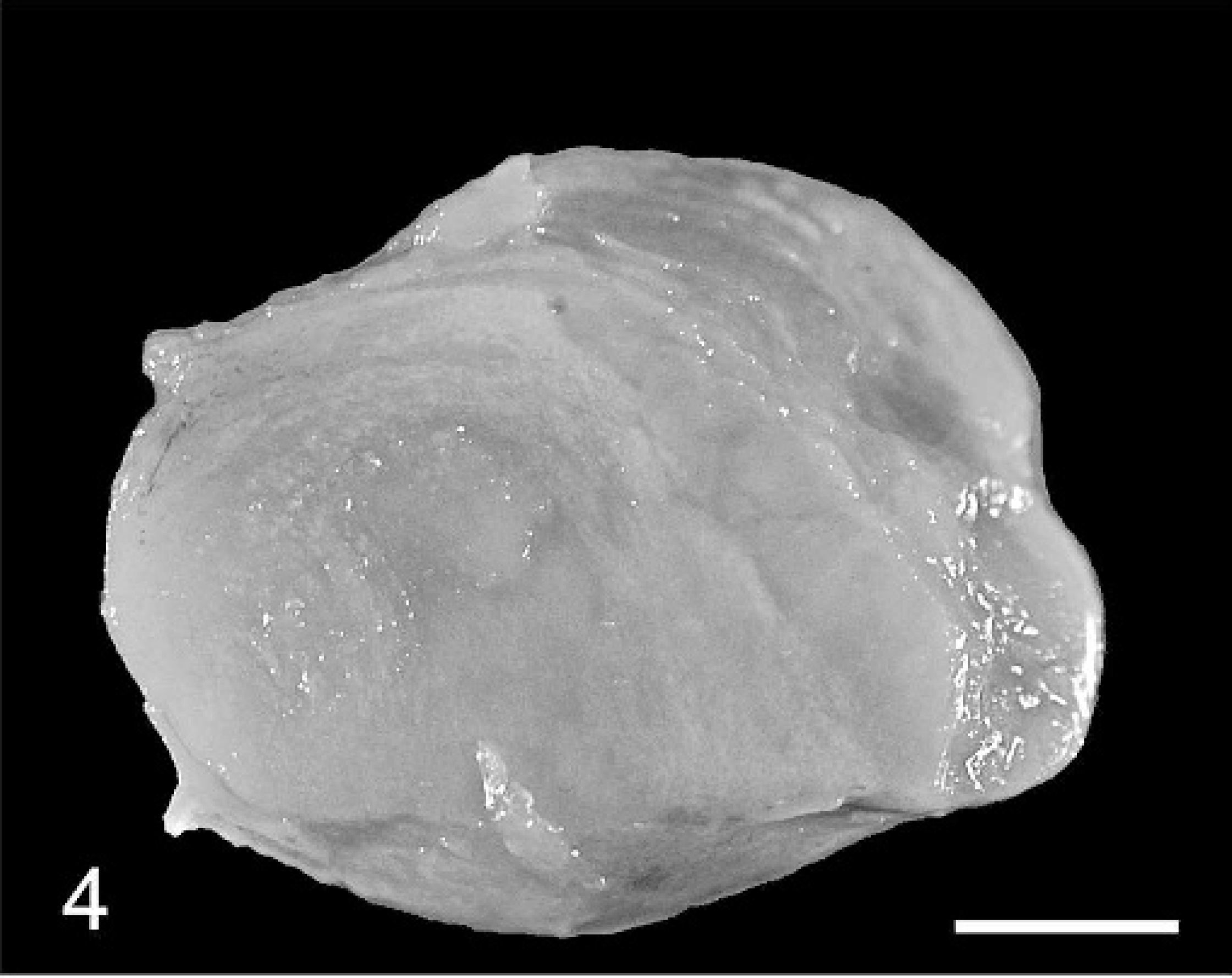
Pituitary gland, horse. The pituitary gland, especially the pars intermedia, is expanded by a 2.5-cm nodule without clear demarcation. Bar = 5 μm.

Pituitary gland, horse. Neoplastic lymphocytes diffusely infiltrate the pars intermedia. Hematoxylin and eosin (HE) stain. Bar = 300 μm.
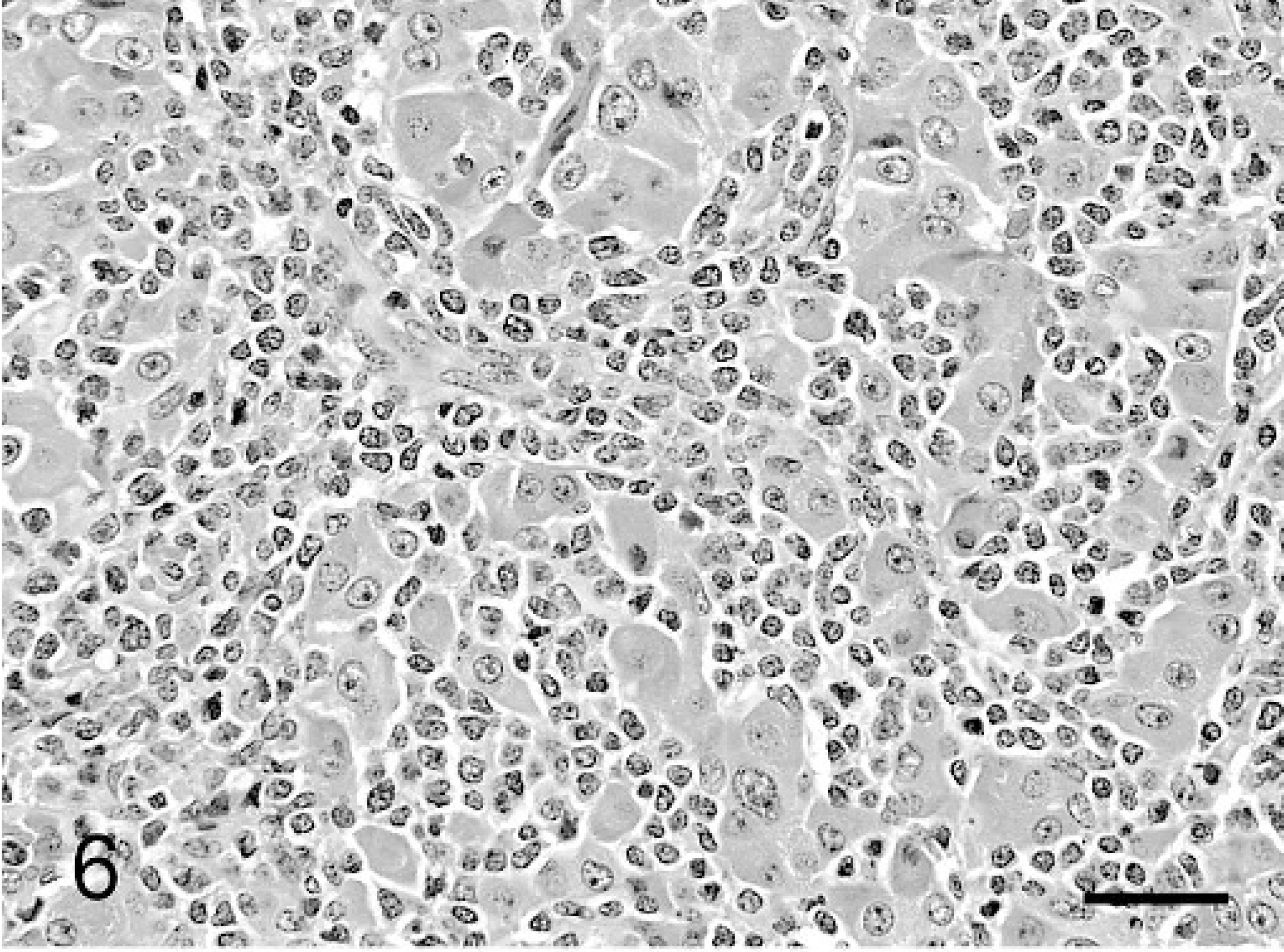
Pituitary gland, horse. Cords of hypertophied epithelial cells of the pars intermedia are separated by numerous infiltrating neoplastic lymphocytes. Hematoxylin and eosin (HE) stain. Bar = 75 μm.
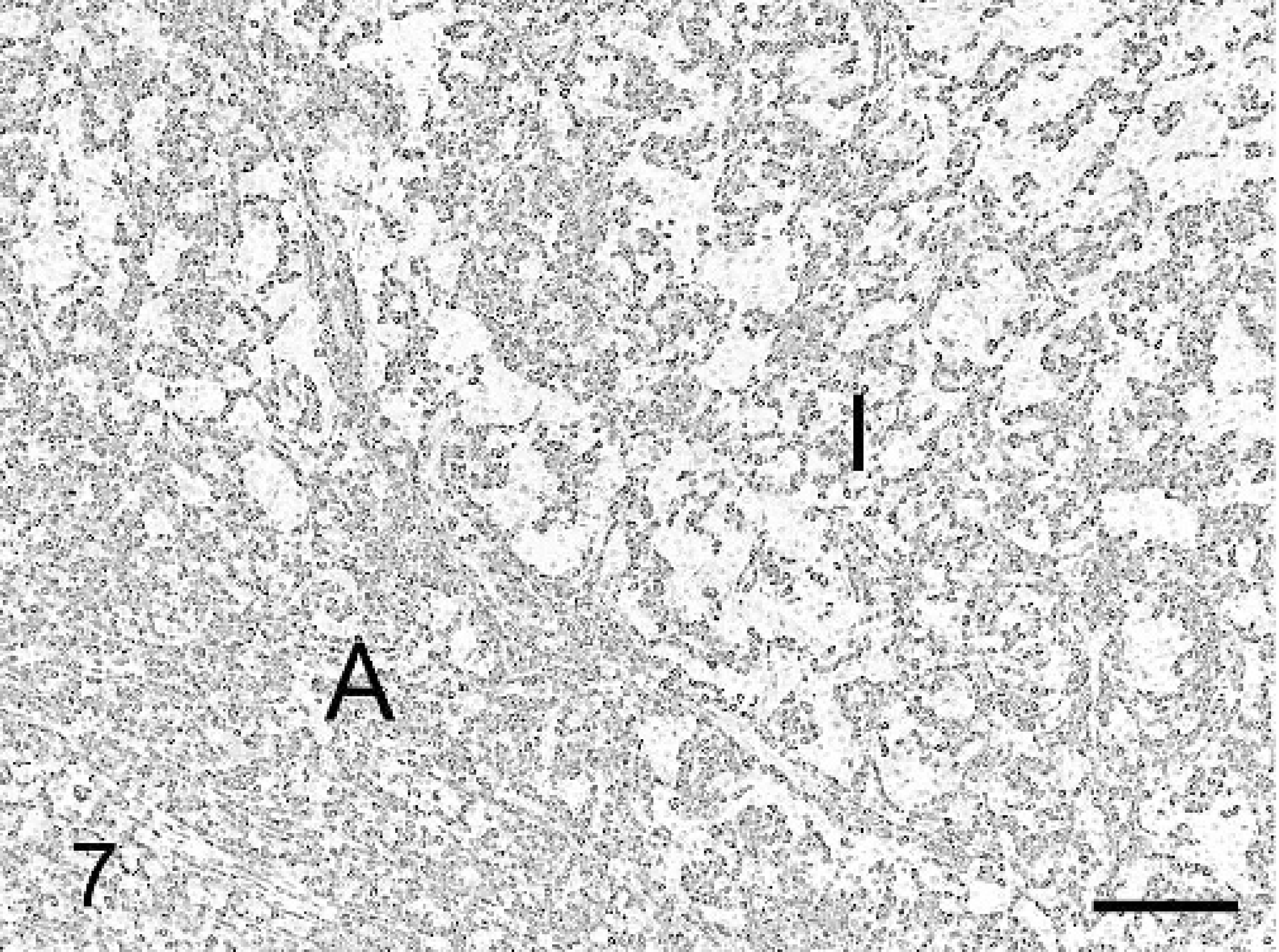
Pituitary gland, horse. Most lymphocytes infiltrating the pituitary gland are positive for CD3. I = pars intermedia. A = pars anterior. Immunoperoxidase for CD3, Mayer's hematoxylin counterstain. Bar = 300 μm.
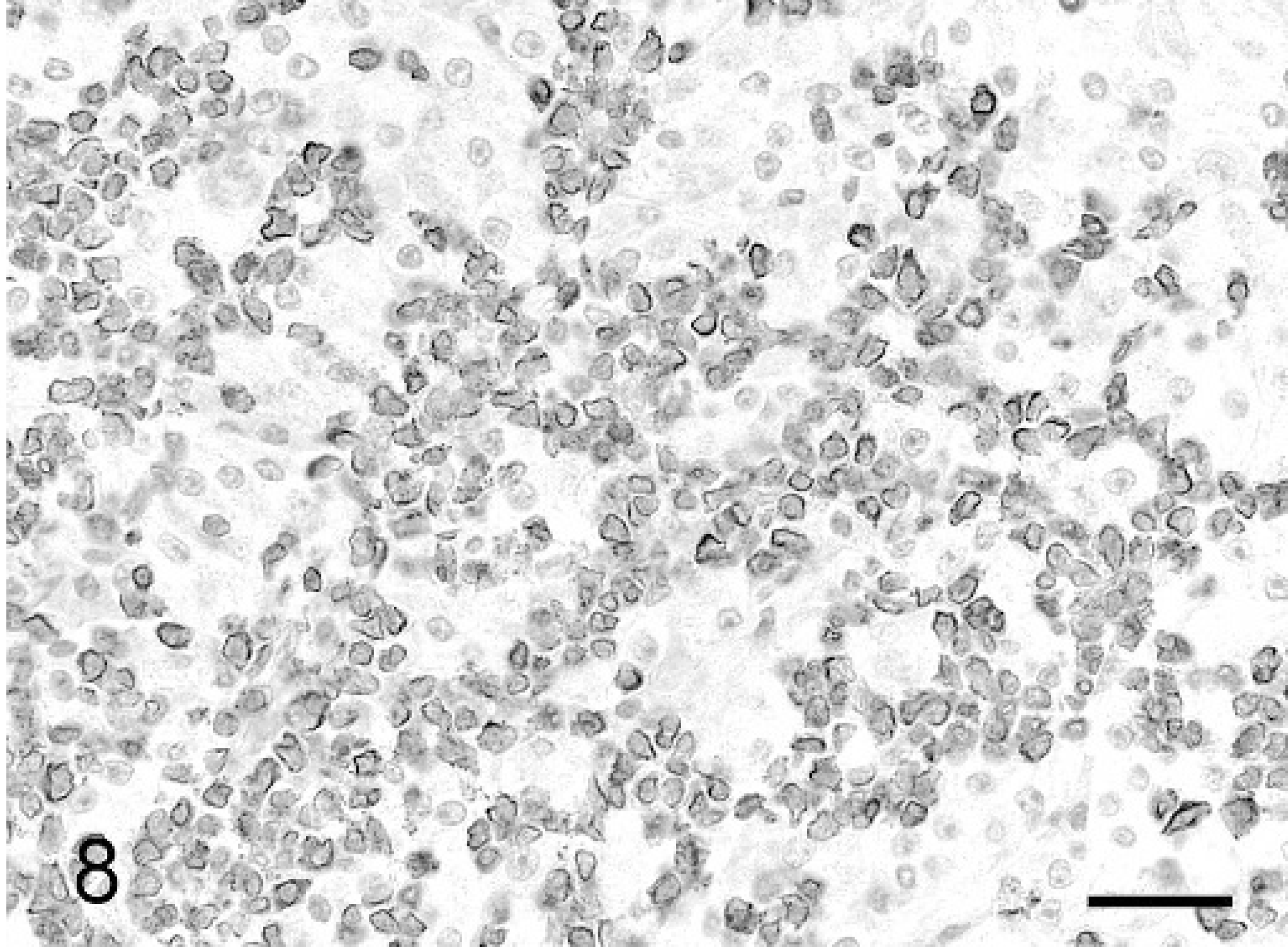
Pituitary gland, horse. Detail of lymphocytes stained with antibody to CD3. Unstained cells are pars intermedia cells. Immunoperoxidase for CD3, Mayer's hematoxylin counterstain. Bar = 75 μm.
Microscopic and immunophenotyping features of neoplastic lymphocytes were similar in both the intestine and pituitary gland. Considering the lack of involvement of other organs and the diffuse involvement of the gastrointestinal tract, it is likely that the pituitary gland involvement was secondary to the alimentary lymphoma.
The diagnosis of PPID is based on clinical and biochemical parameters. 12 Hypertrichosis is a clinical feature of ppid. 8,13,21,22 Pituitary adenoma or adenomatous hyperplasia of the pars intermedia is usually present in PPID. 8,13,21 The exact pathogenesis of PPID-related hypertrichosis is not clear. Hypotheses include 1) excessive adrenocortical production of sex hormones, 2) increased secretion of melanocyte stimulating hormone from the pituitary pars intermedia through loss of dopaminergic inhibition, and 3) mechanical pressure of the pituitary gland on the hypothalamic thermoregulatory center. 2,9,13,19,20,22 PPID was tentatively diagnosed in this mare mainly because of the hypertrichosis, but the owner declined endocrine testing to confirm it. 12 Histologically, adenomatous hyperplasia of pars intermedia was evident along with lymphoma in this case. Hypertrichosis in this mare could have been triggered by both adenomatous hyperplasia of pars intermedia and lymphomatous enlargement of the pituitary gland, resulting in disruption of the hypothalamic dopaminergic tone or disruption of the hypothalamic thermoregulatory center.
Acknowledgement. The authors are indebted to the Animal Disease Diagnostic Laboratory histology laboratory for preparation of slides and immunohistochemistry.
Footnotes
a.
Dako, Carpinteria, CA.
b.
Lab Vision, Freemont, CA.