
Abstract
Neoplastic disorders are frequently encountered in the practice of reptile medicine. Herein we report the clinical behavior, antemortem diagnosis, and histopathologic characteristics of a recurrent intraoral keratinizing basal cell carcinoma (BCC) and a metastatic BCC of the carapace in 2 Hermann’s tortoises (Testudo hermanni). Although squamous cell carcinomas (SCCs) in tortoises show similar predilection sites and gross pathologic features, the BCCs described in our report were characterized by a remarkably fast and highly infiltrative growth in comparison to SCCs. Accordingly, early diagnosis including reliable discrimination from SCC is essential toward the management of this neoplastic entity in tortoises.
Although neoplastic disorders are frequently reported in captive squamates and turtles, these conditions seem less common in tortoises and are rarely described in crocodilians. 7 Neoplasms of the skin, gastrointestinal tract, and hematopoietic system are the most frequently encountered within the class Reptilia, with cutaneous and intraoral squamous cell carcinoma (SCC) being one of the most commonly diagnosed neoplasms.3,7,9,16
In humans, cutaneous basal cell carcinoma (BCC) is the most common malignant neoplastic disorder of all non-melanoma skin cancers.12,15 Intraoral BCC is considered an extremely rare, controversial neoplastic entity in humans and is often confused with peripheral ameloblastoma. 20 In domestic animals, BCCs are rare. Most basal cell tumors previously diagnosed in dogs and cats have been reclassified as benign trichoblastomas in dogs and sweat gland neoplasms in cats.2,8 Although neoplasms of the integumentary system are relatively common in avian species, BCCs are extremely rare in birds. 17 We describe the clinical behavior, antemortem diagnosis, and histopathologic characteristics of a recurrent oral BCC and a metastatic carapacial BCC in 2 Hermann’s tortoises (Testudo hermanni).
An ∼50-year-old, 1.25 kg, female Hermann’s tortoise was presented with a large shell defect. Two years before presentation, the shell lesion was first noted by the owner as a small erosion on the right lateral side of the carapace. Although the lesion progressed to a large shell defect, the owner did not seek medical advice because the animal remained active and showed a normal appetite. The tortoise was kept in the owners’ garden and hibernated outside. Physical examination revealed that the tortoise was in poor body condition but showed active and alert behavior. At the right side of the carapace, a large irregular shell defect was present at the second and third pleural scute (Fig. 1) with a size of 5 × 3.8 × 7 cm. The defect was demarcated by a thick layer of necrotic tissue. Survey radiographs revealed a radiolucent zone at the site of the shell defect bordered by a heterogenic band of soft tissue that created a mass effect, causing displacement of the internal organs toward the left part of the coelomic cavity. Ultrasound revealed the presence of multiple, relatively large, hyperechoic nodules embedded in the liver parenchyma. Blood was collected from the dorsal coccygeal plexus for a serum biochemistry profile and hematologic evaluation at the time of the physical examination. Serum biochemistry test results and the results of the complete blood cell count were within physiological reference intervals, 1 except for a marked rise in aspartate transaminase (AST) activity and pronounced leukocytosis with heterophilia. The leukocytosis was deemed to result from the inflammation associated with the mass. The elevated AST was considered to be a consequence of hepatic damage.

Following debridement of the necrotic tissue under alfaxalone a anesthesia (10 mg/kg, intravenously), a large, pink-to-red, unencapsulated, demarcated mass was exposed with a relatively hard, irregular surface. Three biopsies of the mass were collected for histologic evaluation. The tissues were fixed in 10% neutral buffered formalin, processed routinely, embedded in paraffin, and stained with hematoxylin and eosin. Histologic sections of the mass revealed a well-demarcated, nonencapsulated, cell-rich, and infiltrative mass originating from the epidermis. Cords and trabeculae of relatively small cuboidal to polygonal cells were present in a scant amount of strongly vascularized fibrous tissue stroma, infiltrated by a limited number of heterophils (Fig. 2). The neoplastic cells possessed a large, round, moderately vesicular, centrally located nucleus and a moderate amount of slightly basophilic cytoplasm. There was mild to moderate anisocytosis and anisokaryosis. The mitotic index was 1–3 per high power field (HPF). The epidermis was severely ulcerated and was covered with a thick serocellular crust. A diagnosis of BCC was made. Because of the extensiveness of the malignant and presumably metastatic mass, the tortoise was euthanized with embutramide mebenzoniumiodide tetracaine b hydrochloride following intravenous administration of alfaxalone (20 mg/kg).
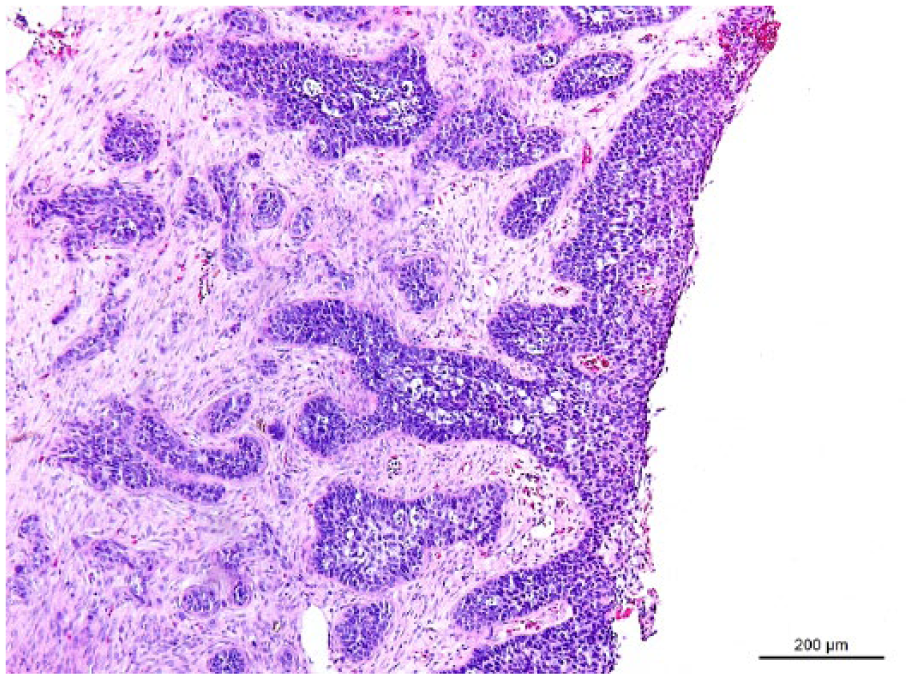
Carapacial basal cell carcinoma in a Hermann’s tortoise (Testudo hermanni). Basaloid epithelial cells are organized in cords and trabeculae in a scant amount of strongly vascularized fibrous tissue stroma. Hematoxylin and eosin. Bar = 100 µm.
During autopsy, the neoplastic mass was found to occupy approximately one-third of the coelomic cavity and extended from the level of the pectoral girdle to the inguinal fossa and the midline (Fig. 1). Because of the size of the mass, the liver was displaced cranially, and the gastrointestinal tract and urinary bladder were displaced to the left part of the coelomic cavity. On cut section, the mass was white and firm. Large, white, nodular lesions with an average diameter of 0.5 cm were present within the parenchyma of the liver (Fig. 1B) and the spleen. In addition, small, white nodular lesions were observed in the liver and ventricular myocardium. Tissue samples were collected for histologic evaluation and processed as described above. Histologic examination revealed metastases in the liver, ventricular wall, and spleen, displaying identical histopathologic characteristics as observed for the primary mass. The nests and cords of neoplastic cells invading the hepatic parenchyma were embedded in an abundant amount of tumor-associated fibrous stroma. Hyperplasia of melanomacrophages was apparent. A thrombus, locally infiltrated by neoplastic cells, was observed in a myocardial blood vessel. Normal splenic parenchyma was largely replaced by neoplastic tissue consisting of several cysts and disorganized nests of neoplastic cells with elaborate vascular and red pulp invasion. The scant amount of remaining splenic tissue was infiltrated with nests of melanomacrophages and granulocytes.
A 60-year-old, 945 g, male Hermann’s tortoise was presented with signs of dysphagia of 2-wk duration. During physical examination, the tortoise was in general good condition, and was alert and active. An intraoral, pedunculated, 1.5 cm diameter, white-to-pink, unencapsulated mass was located at the interchoanal region (Fig. 3). An externally visible, mild but firm swelling was noted in the right maxillary region. Blood was collected from the jugular vein for a serum biochemistry profile and hematologic evaluation. Abnormal findings included leukocytosis with heterophilia, mildly elevated AST activity, and mild hyperglycemia. These findings were presumed to be secondary to inflammation associated with the mass.

Pedunculated, unencapsulated intraoral basal cell carcinoma in a Hermann’s tortoise (Testudo hermanni) located at the interchoanal region.
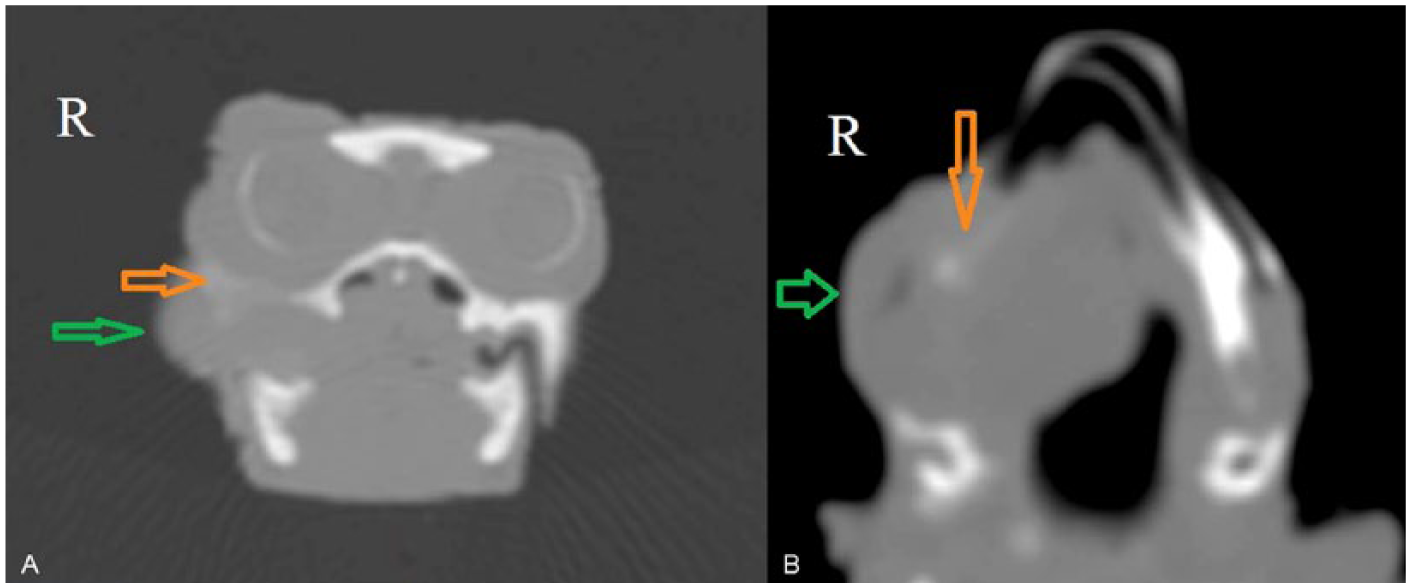
Based on the appearance of the mass and the presumed infiltrative growth in the maxillary region, dorsoventral and lateral orthogonal radiographs of the skull and body, and full body ultrasound, a computed tomography scan was performed following the administration of alfaxalone (15 mg/kg, intravenously). The computed tomography scan showed a mass infiltrating the retrobulbar region and masseter muscle with deformation and destruction of the right maxilla and the zygomatic arch (Fig. 4). Imaging did not reveal the presence of metastases.
The tortoise was intubated with an uncuffed 2.5 mm inner diameter endotracheal tube, c and anesthesia was maintained with 2.5% isoflurane d and 1 L of oxygen per minute with intermittent positive pressure ventilation. The mass was excised at the base, which was located at the insertion of the right mandibular adductor muscle. The removed tissue was processed routinely for histologic examination as described above. Recovery from anesthesia was uneventful, and the tortoise subsequently showed normal appetite.
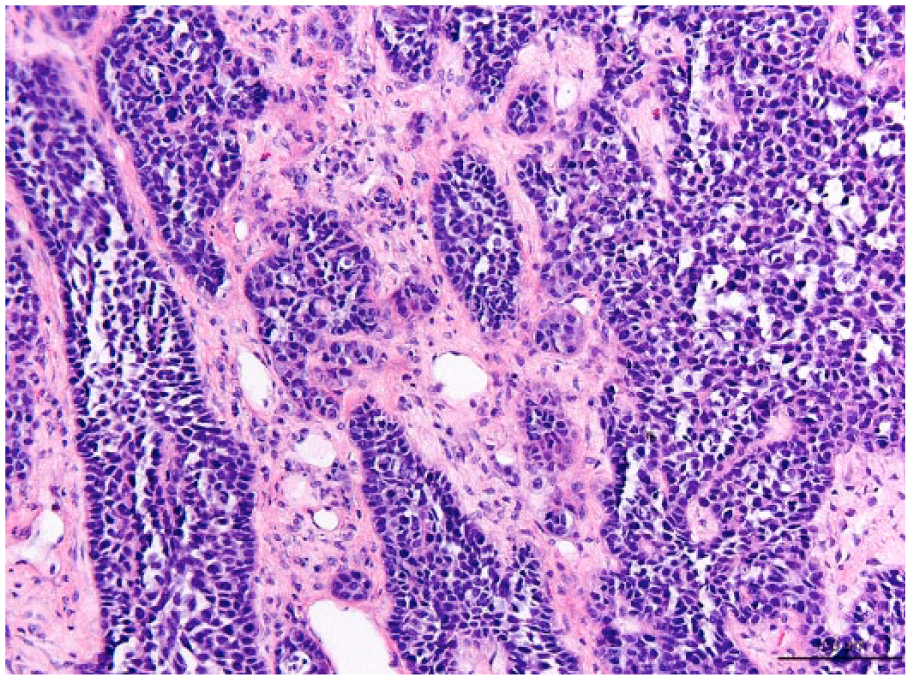
Histologic examination revealed the presence of a cell-rich, unencapsulated, multilobulated, expansile epithelial mass. Basaloid cells were organized in nests and lobules in a scant amount of fibrous stroma. The basaloid cells were cuboidal to oval, had a scant amount of slightly basophilic cytoplasm, and contained a centrally located, round to columnar, relatively large nucleus with finely granular chromatin and 1–2 prominent nucleoli. There was mild to moderate anisocytosis and anisokaryosis. The mitotic index was 2–3 per HPF. Multifocally within the epithelial nests, single cell necrosis was observed (Fig. 5). Within the stroma, there was multifocal perivascular infiltration of lymphocytes and a few granulocytes. Multifocal hemorrhages were observed within the surrounding tissue. A histologic diagnosis of BCC was made.
Section of an intraoral keratinizing basal cell carcinoma in a Hermann’s tortoise (Testudo hermanni). Note the predominant basaloid epithelial cells in a scant amount of fibrous tissue stroma and the connection with the overlying mucosal epithelium. Hematoxylin and eosin. Bar = 200 µm.
Approximately 18 months after initial diagnosis, the tortoise was presented with recurrence of the neoplastic intraoral mass. The mass was ∼2 cm in diameter and caused mechanical interference with food intake. Surgical removal of the recurrent mass was performed as previously described, and neoplastic tissue was submitted for histologic examination. Histologic characteristics of the recurrent mass were identical to those of the original neoplasm. Given the invasiveness of the neoplastic tissue and the anatomic location, complete surgical excision of the mass with healthy margins was deemed impossible, and control visits were recommended at least every 6 months to monitor recurrence of the intraoral neoplasia and the general clinical condition of the tortoise. Repeated surgical resection was required at 24 and 30 months after initial diagnosis. Given the relatively prompt recurrence of the neoplasm, the incomplete surgical resection, and based on the safe and highly effective use of intralesional 5-fluorouracil (5-FU) as a nonsurgical treatment of BCC in humans, 13 we attempted chemotherapy in the tortoise. Following the fourth surgical removal of the intraoral neoplasm (i.e., 30 months after initial diagnosis), 0.25 mL of 5-FUe was injected with a 26-gauge needle fixed to a syringe, c 3 times weekly over 2 weeks, in multiple sites at the location where the surgically removed pedunculated mass had been entrenched. The day following each injection, the injection site showed transient erythema but no other local adverse effects. During a 3-month follow-up period, no significant clinical, biochemical, or hematologic treatment-related adverse effects occurred; biopsies were collected from the injection site. Biopsies taken 1, 2, and 3 months after the last 5-FU injection comprised neoplastic tissue with a histopathologic appearance identical to the primary and recurrent intraoral BCCs. Surgical removal of the recurrent intraoral masses was required on average every 6 months prior to intralesional 5-FU treatment to prevent the occurrence of dysphagia in the tortoise; however, the first surgical removal of the recurrent mass was not required until ∼9 months after the start of chemotherapy (i.e., after the previous surgical removal of the intraoral BCC).
Although once considered uncommon, neoplastic disorders are now identified routinely in the practice of reptile medicine.7,9,16 The increasing life spans of captive reptiles, resulting from optimization of applied captive husbandry, may at least partly explain the increasing incidence of neoplasia in reptiles.
Although age, trauma, and immunosuppression are considered factors promoting the development of BCC, exposure to ultraviolet (UV) radiation is known to be the major cause of cutaneous BCC in humans.4,6 In contrast to cutaneous SCC, however, BCC seems to be associated with intermittent rather than continuous exposure to UV radiation during childhood and adolescence.6,11 In reptiles, providing adequate sources of UV radiation is considered an essential part of the appropriate captive care of many of these species. Nevertheless, UV radiation has also been proposed as a predisposing environmental factor in the development of SCC in bearded dragons (Pogona vitticeps). 9 The true role of artificial UV radiation as an etiologic factor in the development of neoplasms in captive reptiles, however, remains to be further investigated. For the BCC of the carapace described in the present report, a causal relationship with exposure to UV radiation seems highly debatable given the temperate climatologic conditions experienced in the country where the tortoise was kept as a pet for several decades, without access to sources of artificial UV radiation. Testudo spp. typically are known to be able to reach long lifespans. 19 The relatively advanced age of both tortoises with BCC may be considered a potential factor in the development of this neoplastic disorder.
Every presumed case of SCC in tortoises should be differentiated from BCC because the predilection sites and gross pathologic features for both neoplasms are similar. Although SCCs in reptiles have been usually shown to be locally invasive,7,9,10,18 the BCCs described in our report showed remarkably fast and highly infiltrative growth in comparison to SCCs. Accordingly, an early diagnosis including reliable discrimination from SCC is essential for management of this neoplasm in tortoises. The lack of surface epithelial dysplasia in the histologic sections derived from BCCs in tortoises supports the basal cell layer as the origin of the tumors. 20 Immunohistochemistry is a valuable tool for differentiation of BCCs and SCCs in humans.5,20 Attempts to characterize SCCs by immunohostochemistry in reptiles, however, have failed. 14
Footnotes
Authors’ contributions
T Hellebuyck contributed to conception and design of the study; contributed to acquisition, analysis, and interpretation of data; and drafted the manuscript. R Ducatelle contributed to conception and design of the study; contributed to analysis and interpretation of data; and drafted the manuscript. L Bosseler, A Van Caelenberg, H Versnaeyen, and A Martel contributed to design of the study and to interpretation of data. K Chiers contributed to conception of the study and to interpretation of data. All authors critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
a.
Alfaxan, Jurox Ltd., Malvern, Worcestershire, United Kingdom.
b.
T61, IV, MSD Animal Health BVBA, Brussels, Belgium.
c.
Vygon, Brussels, Belgium.
d.
IsoFlo, Abbott Animal Health, Waver, Belgium.
e.
Fluracedyl, Teva Pharma, Wilrijk, Belgium.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.