
Abstract
A 4-year-old, male neutered domestic ferret (Mustela putorius furo) was evaluated for a mass in the left cervical region. The owner elected humane euthanasia, and an autopsy was performed, revealing a neoplasm with infiltration into the left cranial articular fovea of the atlas and cervical vertebrae, with regional compression of the spinal cord. Histologic evaluation was consistent with cervical chordoma. At autopsy, a left cranial lung lobe nodule was observed. Additional sectioning and histologic evaluation revealed multiple foci of metastatic chordoma at this site. A small focus of micrometastasis was also detected in a section from the right lung lobes. Chordoma is the most common musculoskeletal neoplasm of ferrets, arising from remnant fetal notochord. To our knowledge, pulmonary chordoma metastasis has not been previously reported in the ferret. This case demonstrates the potential for visceral metastasis of chordoma in the ferret, as has been reported in other species.
A 4-year-old, male neutered domestic ferret (Mustela putorius furo) was presented with a mass on the neck and a 1-week history of abnormal behavior and abnormal ambulation. No additional relevant clinical history was reported at the time of presentation. On physical examination, a large mass was noted in the left cervical region that almost entirely encircled the circumference of the neck. No other significant abnormalities were noted on physical examination. Because of the extent of the mass and the owner’s reluctance to pursue surgery, humane euthanasia was elected.
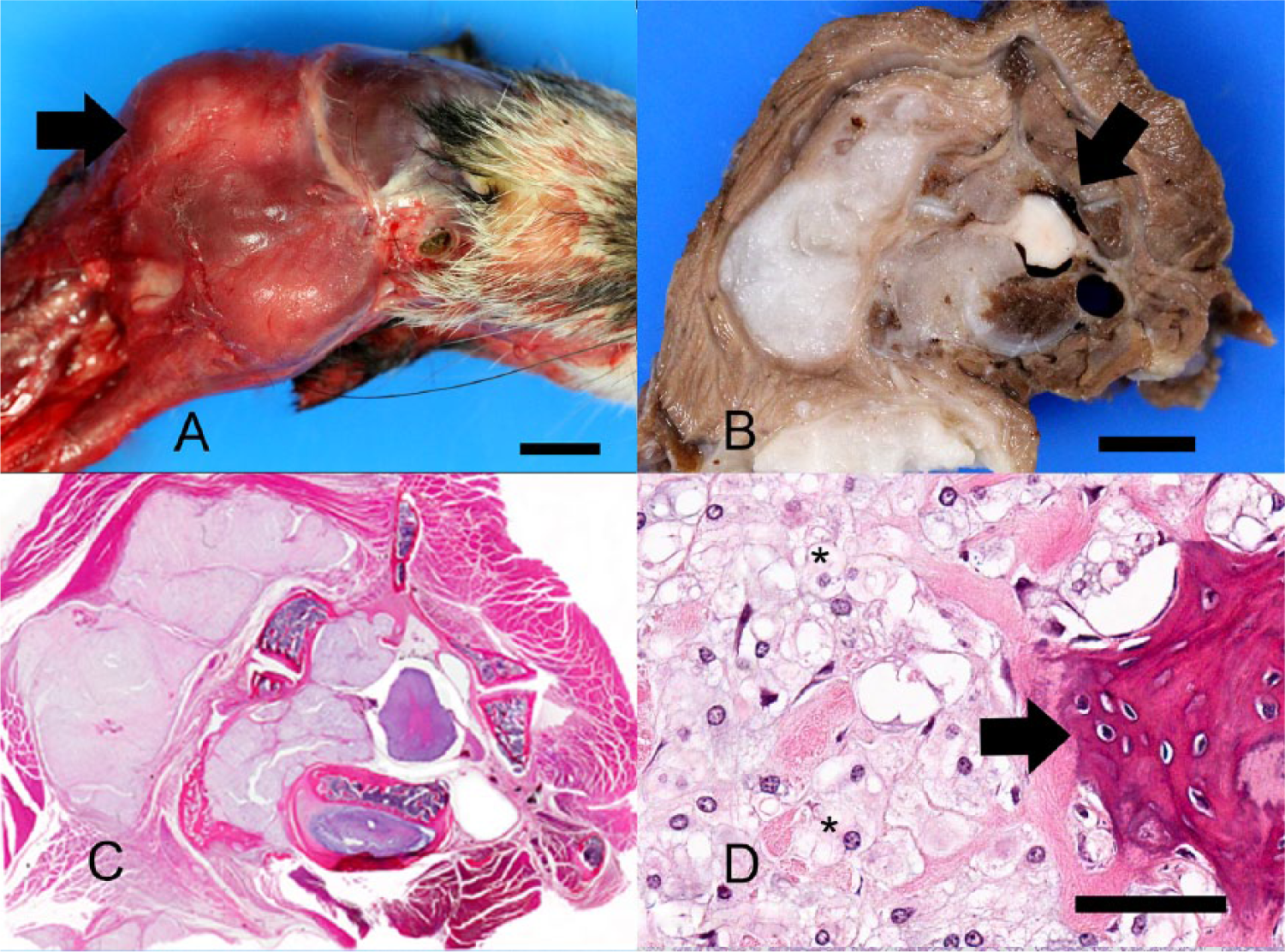
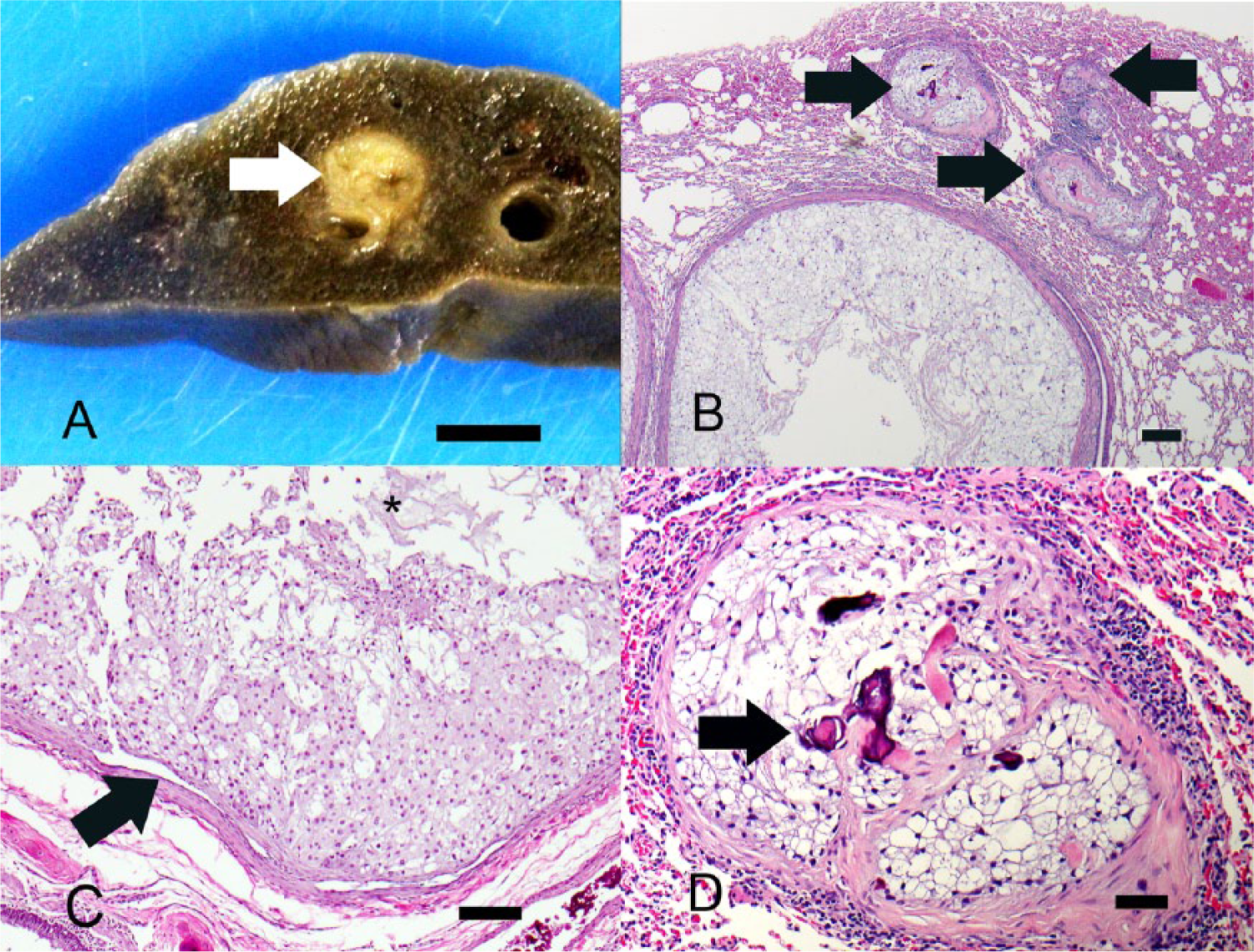
A full autopsy was performed, and a large, firm, multinodular, smooth, white to tan, 5 cm × 3.5 cm × 1.5 cm mass was observed within the skeletal muscle of the neck, just caudal to the skull (Fig. 1A). The mass extended to the left lateroventral neck, was adhered to the first cervical vertebra, and extended caudally to the mid-cervical region (approximately C3/C4). The mass was lateral and ventral to, but was not adhered to, the trachea or esophagus. After removal of the skull, evaluation of C1 revealed infiltration and effacement of the left cranial articular fovea (articular facet of the atlas). The cervical spine was decalcified, and multiple cross sections were obtained, which revealed extension of the mass into the vertebral canal with compression of the regional cervical spinal cord from segments C1 to approximately C3/C4 (Fig. 1B, 1C). The caudal aspect of the left cranial lung lobe contained a 0.5 cm in diameter, firm, smooth, white, round nodule. Additional incidental findings included splenic congestion and 2 cortical renal cysts.
Domestic ferret (Mustela putorius furo).
Tissues collected at autopsy were fixed in 10% neutral buffered formalin, routinely processed, and embedded in paraffin according to accepted histological technique. Five-micrometer-thick sections were stained with hematoxylin and eosin. Histological evaluation of the mass described above revealed a multilobular, fairly well demarcated, compressive to infiltrative neoplasm (Fig. 1C, 1D). The neoplasm compressed and multifocally infiltrated the epaxial musculature, cervical vertebral pedicle, and articular processes, and extended into the vertebral canal with compression of the adjacent cervical spinal cord (Fig. 1C). Lobules were separated by eosinophilic, fibrovascular connective tissue and consisted of large polygonal cells with distinct cell borders and abundant, amphophilic to clear, vacuolated cytoplasm (physaliferous cells), surrounded by variable amounts of amphophilic, mucinous stroma. Nuclei were round to oval and often peripheralized, with finely stippled chromatin and multiple nucleoli. There were zero mitotic figures in 10 high-power (400×) fields. Multifocally, within the center and at the periphery of the lobules, scattered aggregates of cartilage and woven bone were interspersed with the physaliferous cells (Fig. 1D). Chondrocytes were present within a lightly eosinophilic to amphophilic matrix or were occasionally entrapped within bone. Rare binucleated cells were found. Small aggregates of lymphocytes, plasma cells, and macrophages were present at the periphery of the mass. The histological features of this neoplasm were consistent with chordoma.
There was histological evidence of bone resorption. Fragmented, woven (reactive) bone was interspersed with nu-merous plump osteoblasts and fibroblasts. Neoplastic compression of the cervical spinal cord resulted in shifting of the ventral median fissure away from the mass (Fig. 1B, 1C). The white matter of the spinal cord exhibited mild, multifocal vacuolation in the dorsal, lateral, and ventral funiculi, within which were few Gitter cells containing myelin degradation products (myelinophages). Scattered, multifocal swollen axons (spheroids) were present within the ventral and lateral funiculi. Within the epaxial muscles, there was histological evidence of degeneration and regeneration.
Sections of the left cranial lung lobe revealed multiple, variably sized nodules within the parenchyma, composed predominantly of physaliferous cells similar to those described in the cervical vertebral mass (Fig. 2B–2D). Nodules ranged from 60 µm to 4 mm in diameter. The largest nodules had central regions of degeneration and necrosis (Fig. 2C) and contained bone and cartilage. Scattered osteoid matrix was observed in smaller nodules (Fig. 2D). In 1 section, a focal aggregate of neoplastic cells was present within a large artery (Fig. 2C), and neoplastic cells were also observed within smaller arteries. A microscopic metastatic focus was observed in a section from the right lung lobes. These foci were interpreted to represent visceral metastasis of the primary cervical chordoma. Additional findings, unrelated to the neoplasm, included splenic congestion with extramedullary hematopoiesis, chronic enteritis, gastritis, and colitis, as well as chronic cholangiohepatitis and cholecystitis with diffuse hepatocellular vacuolation.
Domestic ferret (Mustela putorius furo).
Chordoma is a neoplasm arising from the intraosseous remnants of fetal notochord.3,7,8,11,19 The notochord arises from embryonic mesoderm, inducing formation of the head and central nervous system. 3 The notochord is predominantly replaced by the developing vertebral column, but persists in adult animals as the nucleus pulposus of the intervertebral discs. 3 Rests of notochord outside of the intervertebral discs are also present, from which chordoma is thought to be derived.3,7,11,19 It is believed that chordomas arise from the notochord mainly because the tumor occurs exclusively in the axial skeleton and that, under both light and electron microscopy, chordoma resembles notochord. 16 Histologically, chordoma is commonly characterized by vacuolated cells known as physaliferous cells arranged in a lobular arrangement. 17 In ferrets, chordoma has a unique appearance with a regular zonal pattern of lobules of physaliferous cells surrounding cartilage with a central core of bone. 7 Chordomas are the most common musculoskeletal neoplasm in ferrets, 2 but are rare in humans and other animals.1,6,9,17 In ferrets, chordomas occur most commonly at the tip of the tail, 2 but they have also been reported in the cervical region in 2 previous cases8,18 and the thoracic vertebrae in 1 case. 14
In humans, there are 3 recognized subtypes of chordoma: classic chordoma, chondroid chordoma, and chordoma with malignant spindle cell component (dedifferentiated).7,13,18 It has been suggested that ferret chordomas may act as an animal model for the chondroid subtype of human chordoma.7,18 Differentiation between classic and chondroid subtypes in humans is significant, as chondroid chordomas are associated with a survival rate 3 times greater than that of classic chordomas.3,11
Chordomas in humans have usually been considered benign or as a neoplasm with low risks due to their slow-growing character and rarity of distant metastasis 17 ; however, a study from 2012 shows that they can exhibit more aggressive behavior such as local infiltration and damage of surrounding structures, recurrence, and metastasis. 19 Complete surgical excision, followed by proton irradiation, is the gold standard of chordoma treatment in humans,9,19 because chordoma is generally considered resistant to regular doses of radiation.6,9 In ferrets, complete surgical excision can be easily achieved in most cases that occur at the distal tail tip; however, neoplasm developing at other locations on the spinal cord may prove more difficult to remove. To our knowledge, proton beam therapy is not yet available for use on privately owned pets.
To our knowledge, chordoma metastasis to a visceral organ has not been previously reported in the domestic ferret. There has been 1 case report of suspected metastatic chordoma to 2 distant cutaneous sites 11 and another case of cervical chordoma metastasis to the adjacent skin. 7 Chordomas are rare in other species and have been reported in the dog, cat, rat, mink, and human.5,7,15,18 Cervical and coccygeal chordomas have been reported in both the dog 12 and cat.4,5 Chordoma metastasis has been reported in the rat, cat, and human.5,15,18 In humans, chordomas have been reported to metastasize to the skeleton, lung, and liver. 17 Skin and lung metastasis has also been reported in rats,13,18 and local lymph node metastasis was seen in 1 cat. 5 In the aforementioned case of chordoma in a ferret with distant metastasis to the skin, 11 the primary coccygeal chordoma was present for a long time period, with steady growth observed over a 4-year time course. The authors hypothesized that the metastatic potential of ferret chordomas may increase over time. In the current case, the owner of the ferret reported that the mass had been present for 1 day; however, the exact time of duration of the mass was unknown, and it is very likely that the mass had been present for a longer period of time. In humans, chordomas usually only metastasize after a long clinical period. 17
In the present case, metastatic cells were present both within vessels and the pulmonary parenchyma. The definition of metastasis is the presence of tumor implants discontinuous with the primary tumor. 10 Pathways of spread include 1) direct seeding of body cavities or surfaces, 2) lymphatic spread, and 3) hematogenous spread. Hematogenous spread was evident in this case.
Ferret chordomas are generally considered benign due to extremely rare metastases, slow growth rate, and the ease of surgical excision at the most common occurrence site at the distal tail tip. The observations in our case demonstrate that chordomas in the ferret have the potential for distant metastasis, including to the lungs and likely other viscera. These findings conflict with previous characterizations of chordoma in the ferret and suggest that surgical removal is warranted. As previously mentioned, chordoma in humans is best treated with surgical resection followed by radiation therapy.6,9,19 Many different chemotherapy regimens have been tried in human cases, but none have been shown to be effective.6,9 In the present case, surgical excision would have been difficult to achieve due to the extent and anatomical location of the mass. It is unclear whether or not radiation therapy would have been helpful in this case as there have been no reported cases of radiation therapy use in ferret chordomas. To clarify this question, radiation therapy should be attempted in future cases of nonresectable chordomas in ferrets to assess tumor response.
Footnotes
Authors’ contributions
Both authors contributed to conception and design of the study; drafted the manuscript; gave final approval; and agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared that they received no financial support for their research and/or authorship of this article. Color images supported by the Schiff Foundation, courtesy of Dr. Philip Fox, the Animal Medical Center.