
Abstract
A captive bred red tail boa (Boa constrictor constrictor) was presented with a large intraoral mass originating from the buccal gingiva, attached to the right dentary teeth row. Based on the clinical features and histological examination, the diagnosis of a peripheral odontogenic fibromyxoma was made. Sections of liver biopsies and circulating lymphocytes contained relatively few eosinophilic intracytoplasmic inclusion bodies, indistinguishable from those observed in inclusion body disease–affected snakes. Inclusion bodies were not observed in cells comprising the neoplastic mass. Using reverse transcription polymerase chain reaction (RT-PCR), arenavirus was detected in the neoplastic tissue. Two years after surgical removal of the mass, recurrence of the neoplastic lesion was observed. Numerous large inclusion body disease inclusions were abundantly present in the neoplastic cells of the recurrent fibromyxoma. Sections of liver biopsies and circulating lymphocytes contained relatively few intracytoplasmic inclusions. The RT-PCR revealed the presence of arenavirus in blood, a liver biopsy, and neoplastic tissue. The present case describes the co-occurrence of an arenavirus infection and an odontogenic fibromyxoma in a red tail boa.
Inclusion body disease (IBD) is a transmissible and progressive disease that may eradicate entire captive boid collections and is considered to be the most important multisystemic viral infection affecting boas and pythons worldwide.3,4 Clinical signs observed in affected snakes include central nervous symptoms, stomatitis, regurgitation, pneumonia, lymphoproliferative disorders, and neoplasia.4,8,15,18 None of these clinical signs are pathognomonic for IBD, making it difficult to attribute observed clinical signs and lesions in IBD-positive snakes to the disease. 4 Moreover, it is generally accepted that IBD inclusions can be demonstrated in asymptomatically infected snakes, especially adult boas.3,4 Nevertheless, the disease is considered to be fatal, and affected animals often succumb to secondary infections.4,15,18 Impaired function of white blood cells and myelopoietic cells leading to immunosuppression is presumably the major cause of secondary infections. 4 Although several viruses, including retroviral agents, have been identified and isolated from snakes with IBD,4,11,19 it was not until 2012 that arenaviruses have been put forward as the etiological agents of IBD based on fulfillment of Koch postulates in vitro. 16 Transmission studies in live snakes, however, will be required to formally designate arenaviruses as the exact cause of IBD.1,3,16
A 1.6-kg captive bred, 6-year-old, male red tail boa (Boa constrictor constrictor) was presented with a large intraoral mass. The snake was part of a private collection consisting of 26 adult red tail boas. The owner bought the snake from a snake breeder 5 years prior to presentation. The boas were kept per pair in glass tanks of 100 cm × 80 cm × 80 cm with coconut husk as substrate. Temperature was maintained at 28–30°C during a 12-hr photo period and 23–25°C at night. All snakes were fed live, adult rats. Physical examination revealed a general good body condition and no other clinical signs. Three months prior to presentation, the owner had noticed the presence of a small intraoral nodule of approximately 5 mm in diameter. Following a progressive but slow growth, the mass interfered with normal food intake. The pedunculated intraoral mass had a relatively thin base and originated from the mandibular buccal gingiva, attached to the right dentary teeth row. Grossly, the mass was relatively soft and had a pale pink color. Furthermore, the mass was painless, ovoid, and measured approximately 2.5 cm in diameter (Fig. 1). Because of the large size, the mass bulged out of the oral cavity making the tissue prone to external insult. Consequently, superficial abrasions were visible.

Pedunculated peripheral odontogenic fibromyxoma in a red tail boa (Boa constrictor constrictor) originating from the mandibular buccal gingiva, attached to the right dentary teeth row.
A blood sample was collected by cardiocentesis in a heparinized tube. Blood and buffy coat smears were prepared and stained with hematoxylin and eosin (HE). The results of the complete blood cell count and the examination of the buffy coat smear revealed leukocytosis (31 × 103/µL) and lymphocytosis (29 × 103/µL) when compared with appropriate reference intervals. 5 Round to oval eosinophilic intracytoplasmic inclusions were observed in several lymphocytes, indistinguishable from those described for IBD in boid snakes.4,15,16,19 Serum biochemistry test results were within physiological reference intervals. 5 Surgical excision of the mass, including a narrow margin of the healthy appearing gingival tissue, was performed during propofol anesthesia a (10 mg/kg, intravenously). Two dislocated teeth were present at the base of the mass. As the detection of IBD inclusions in HE-stained histological slides in addition to blood smears is still considered as the current gold standard for diagnosing IBD, 4 a percutaneous ultrasound-guided liver biopsy was collected following the protocol as described previously. 10 Sections of the mass and liver biopsy were collected for histologic evaluation. The tissues were fixed in 10% neutral buffered formalin, processed routinely, embedded in paraffin, and stained with HE. Histological sections of the mass revealed spindle-shaped cells embedded within a loosely arranged fibromyxomous stroma. The stroma contained collagen fibers as confirmed by Von Gieson staining and acid mucopolysaccharides as shown by alcian blue staining. Immunohistochemical staining showed that the tumor cells contained vimentin-positive intermediate filaments in their cytoplasm. The moderately sized neoplastic cells contained large, centrally located, oval nuclei with a fine granular chromatin, several nucleoli, and an eosinophilic cytoplasm. Proliferating cell nuclear antigen immunostaining showed that approximately 50% of the tumor cell nuclei were positively labeled. Furthermore, anisokaryosis was common, and mitosis was infrequent. A few cells were binucleated. Superficial ulceration and multifocal infiltration of lymphocytes, plasma cells, and macrophages containing hemosiderin were noted. Intracytoplasmic inclusion bodies were not observed in the neoplastic cells. Histological sections derived from the liver biopsy displayed moderate cytoplasmic vacuolization of hepatocytes and the presence of a limited number of small eosinophilic intracytoplasmic inclusions within hepatocytes.
One week after surgery, the gingival tissue at the site where the neoplastic mass was previously entrenched had regained a normal appearance. The boa exhibited normal activity as well as feeding behavior and was discharged. The HE-stained buffy coat smears were prepared from blood samples obtained from the other 25 red tail boas belonging to the same private collection. All snakes appeared to be clinically healthy, but intracytoplasmic inclusion bodies consistent with those observed in boids with IBD were observed in 11 out of 25 snakes. In addition, liver biopsy specimens were collected from 3 IBD-positive and 3 IBD-negative boas. Intracytoplasmic IBD inclusions were detected in the hepatocytes of the IBD-positive but not in the IBD-negative snakes. One and 2 years later, examination of HE-stained buffy coat smears of the 24 remaining boas of the same private collection revealed that the IBD status and clinical condition of the group of snakes had not changed. However, 6 months after the principal diagnosis of the fibromyxoma in the described case, 1 IBD-positive boa from the collection was presented with a large coelomic swelling in the caudal third of the body. A presumptive diagnosis of an intestinal lymphoma was made following cytological and ultrasound investigation. Postmortem histological examination confirmed the latter diagnosis. Based on histological examination, intracytoplasmic inclusion bodies were not observed in cells compromising the lymphoma.
As arenaviruses were not yet associated with IBD at that time, blood samples or liver biopsy specimens obtained from the boa with the peripheral fibromyxoma and the remaining boas of this collection were not submitted for arenavirus reverse transcription polymerase chain reaction (RT-PCR). Tissue samples consisting of the peripheral fibromyxoma and the intestinal lymphoma, however, had been deposited in our repository and were eventually submitted to arenavirus RT-PCR and sequencing as previously described. 16 All samples collected during the current study that were submitted to arenavirus RT-PCR and sequencing were analyzed by a commercial facility. b The latter testing revealed the presence of arenavirus in both neoplastic tissues. A search of the GenBank database through BLAST revealed that the sequences of the amplified viral fragments extracted from both neoplastic tissues had the highest similarity to nucleotide sequences of a previously identified arenavirus in boid snakes from the United States (California Academy of Sciences [CAS] virus isolate ATB segment S). 16
Approximately 2.5 years after the initial diagnosis, the boa was presented because of recurrence of the intraoral neoplasia. A few days earlier, the owner had noticed a small nodule of approximately 4 mm in diameter at the exact location as the previously resected mass. The boa weighed 2 kg, and physical examination was unremarkable. Whole blood was collected for blood biochemistry and a complete blood cell count, and HE-stained buffy coat sections were prepared. Again, leukocytosis (27 × 103/µL), lymphocytosis (25 × 103/µL), and the presence of relatively few small intracytoplasmic inclusions in lymphocytes were demonstrated. Serum biochemistry test results were within physiological reference intervals. 5 Skull radiographs revealed a normal appearance of the right mandibula, excluding a central origin of the odontogenic fibromyxoma. The mass was excised, and a liver biopsy was collected following the same protocol as previously described. The small mass was encapsulated by normally appearing gingival tissue. It could be seen during resection that the gray-white, moderately firm mass arose from the connective tissue of the dental papillae, and 3 severely displaced and 1 loose tooth were present within the base of the mass. Tissues were fixed and prepared as described above. Seven days after surgery, the boa proved to be fully recovered. During a 4-month follow-up period, no recurrence of the mass was observed, and the boa displayed excellent health.
The histological features of the recurrent neoplasia were identical to that of the first excised fibromyxoma. A large number of the neoplastic cells of the recurrent fibromyxoma, however, possessed 1or more large eosinophilic intracytoplasmic inclusion bodies typical of IBD (Fig. 2). A limited number of small eosinophilic intracytoplasmic inclusions were detected within hepatocytes in histological sections derived from the liver biopsy.
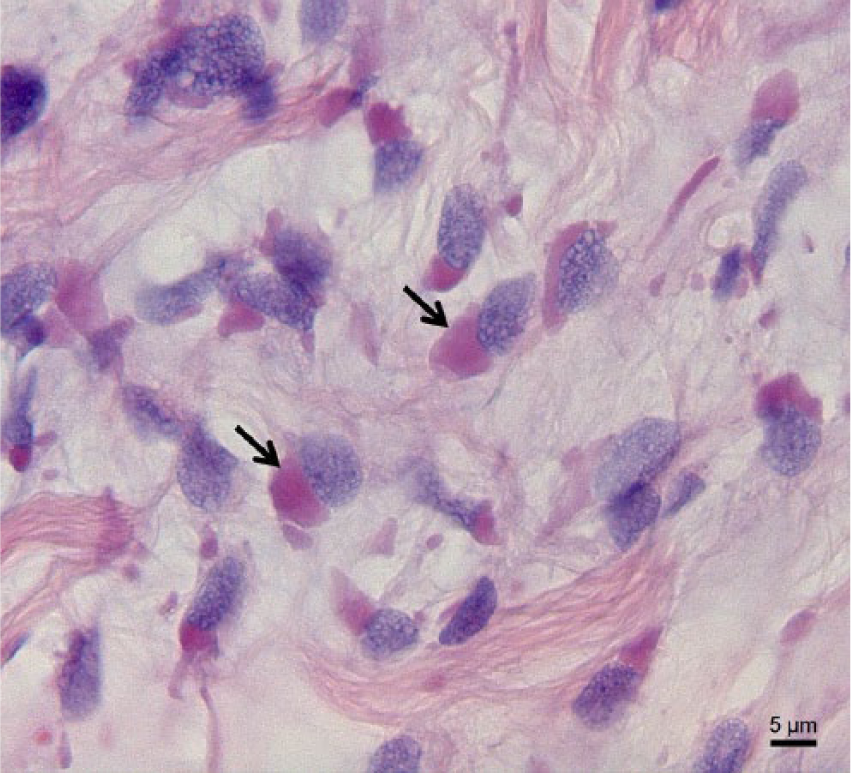
Intracytoplasmic eosinophilic inclusion bodies (arrows) detected in neoplastic cells compromising a peripheral odontogenic fibromyxoma in a red tail boa (Boa constrictor constrictor). Reverse transcription polymerase chain reaction revealed the presence of arenavirus in the neoplastic tissue. Hematoxylin and eosin. Bar = 5 µm.
Arenavirus RT-PCR and sequencing was performed on whole blood, a liver biopsy, and tissue compromising the recurrent neoplastic mass, as previously described. 16 Arenaviral RNA was detected in all tested samples. As for the first excised fibromyxoma and the intestinal lymphoma, nucleotide BLAST searches demonstrated the highest similarity of the revealed arenaviral sequences to the CAS virus isolate (ATB segment S). 16
Based on the histologic features of the neoplasia in the boa in the current study and taking into account the connective tissue of the dental papillae as the presumed site of origin of the mass as well as the involvement of teeth, a definitive diagnosis of a peripheral odontogenic fibromyxoma was made. To the authors’ knowledge, this type of tumor has not yet been reported in reptiles. Pericardial, renal, and distal forelimb fibromyxoma, however, have been documented in a Russell’s viper (Daboia russelli), a green sea turtle (Chelonia mydas), and a free-ranging American alligator (Alligator mississippiensis), respectively.6,13,20 In general, odontogenic fibromyxoma is a locally aggressive tumor of odontogenic origin characterized by slow growth and usually shows no tendency to metastasize. 7 The predominant slow growth and a 2-year interval before recurrence of the neoplasia as noted in the boa described herein correspond to the clinical behavior of odontogenic fibromyxoma in human beings and mammals.7,12 Presumably, this type of neoplasia arises from the connective tissue of the dental papilla. It is highly unusual that the mandibula or maxilla is the site of origin of a true fibromyxoma. 7 In human beings, odontogenic fibromyxoma is almost entirely restricted to tooth-bearing areas and is associated with dental abnormalities such as unerupted or displaced teeth. 7 It is unclear if the displaced teeth found in the mass of this boa were primarily associated with the neoplastic process or if the mass may have disturbed normal tissue architecture and caused subsequent displacement of the involved teeth.
Eosinophilic intracytoplasmic inclusion bodies were observed in lymphocytes, hepatocytes, and neoplastic cells compromising the recurrent peripheral fibromyxoma. By light microscopic investigation, these inclusions were identical to those observed in confirmed cases of IBD and arena-virus infection.1,3,8,15,16,19 Neoplastic disorders such as lymphoma and undifferentiated sarcoma have previously been documented in boids with concurrent IBD.14,17 To the authors’ knowledge, however, neoplastic cells containing intracytoplasmic IBD-like inclusions in a snake have not previously been reported. As the first excised fibromyxoma and the intestinal lymphoma did not contain IBD inclusions but were positive for arenavirus based on RT-PCR testing, it may be of particular interest to test neoplastic and other tissues in boid snakes for arenavirus infection even if histological examination does not reveal intracytoplasmic IBD inclusions. Circulating lymphocytes and hepatocytes contained remarkably few and smaller inclusions in comparison to the numerous and large IBD inclusions that were abundantly present in the neoplastic cells of the recurrent fibromyxoma. The neoplastic cells may be more permissive for viral replication and may promote dissemination of viral infection. Similar considerations were established for oncornavirus (C-type–like retrovirus)-associated neoplasms in pythons. 2
In particular, tissue-specific retroviruses have previously been associated with neoplastic diseases in snakes.2,9 As for the present case, however, the relationship of the intraneoplastic arenaviruses to the etiology of the neoplasias was uncertain.2,9 That neoplastic disorders are more likely to develop in arenavirus infected snakes remains a supposition.
As observed for the described collection, it is not uncommon to find unusually high numbers of subclinically infected snakes in captive boid collections.3,4 Although the sensitivity of blood smears to screen suspected cases for the presence of IBD inclusions is considered to be low,4,14 the results of repeated buffy coat smear examinations corresponded with the examinations of the liver biopsy sections for the boas belonging to this collection. All other IBD-positive snakes in the affected collection displayed excellent health during a 2-year follow-up period. It is not known, however, which percentage of persistently infected snakes will eventually develop clinical signs of IBD. 4
In the present report, the co-occurrence of arenavirus infection and a peripheral odontogenic fibromyxoma in a red tail boa with IBD is described. The possible absence of intracytoplasmic IBD inclusions in histological sections of arenavirus-infected neoplastic tissues is a noteworthy finding.
Footnotes
a.
Propovet, Ecuphar NV/SA, Oostkamp, Belgium.
b.
Pinmoore Animal Laboratory Services Ltd, Cheshire, United Kingdom.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared that they received no financial support for their research and/or authorship of this article.