
Abstract
Canine mammary gland tumor (CMT) and human breast cancer (HBC) share many similarities regarding their risk factors, histological features, and behavior. Despite the increasing evidence of molecular marker expression as a prognostic indicator for HBC, few studies have applied this approach to CMT. The aim of the present study is to evaluate the significance of the expression of estrogen receptor–alpha (ERα), human epidermal growth factor receptor 2 (HER2), and caveolin-1 (CAV1) to the behavior and the clinical outcome of CMT. Additionally, the correlation between subtype classification (luminal A, luminal B, HER2-overexpressing, basal-like, and normal-like) and tumor behavior prognosis were assessed. Canine mammary gland tissues were immunohistochemically stained for ERα, HER2, and CAV1 and evaluated and classified into 5 subtypes on the basis of immunoreactivity. Although there were no statistically significant differences in the molecular marker immunoreactivity of different subtypes, the degree of positive staining for ERα, extranuclear ERα, HER2, and CAV1 showed significant correlations (P < 0.05) with the behavior and prognosis of the tumor. The current study indicates the prognostic value of immunohistochemical staining status of ERα, HER2, and CAV1 for CMT. In addition, some trends were seen in subtype classification on the prognosis of the tumor, implying that, although further analysis is needed, there is potential clinical application of 5-subtype classification for CMT.
Introduction
Canine mammary gland tumor (CMT) and human breast cancer (HBC) are characterized as highly heterogeneous neoplasms. Although histomorphological features may differ between the human and canine forms of the disease, a number of studies have shown similarities relating to molecular marker expression, histomorphological pattern, and prognosis.7,21,31,32 Despite a number of attempts to investigate prognostic factors for CMT and HBC, corresponding, definitive indicators of clinical outcomes of these tumors are not well defined.
Based on molecular marker expression patterns, HBC has been categorized into 5 subtypes that appear to have some level of correlation with the tumor behavior in terms of clinical outcome and prognosis.8,11,13,35,39 The molecular markers that have been used include hormone receptors (HRs), estrogen receptor–alpha (ERα), and progesterone receptor (PR), as well as nonhormonal receptors, such as human epidermal growth factor receptor 2 (HER2) and basal-like markers. The molecular marker–based classification system categorizes HBC into luminal A subtype (HR+, HER2–, basal markers +/–); luminal B subtypes (HR+, HER2+, basal markers +/–); HER2-overexpressing subtype (HR–, HER2+, basal makers +/–); and normal-like subtype (negative for all the markers).8,11,13,35,39 To the authors’ knowledge, very few studies have applied this system to classify CMT.4,21,32
Previous studies focusing on the molecular expression of ERα and PR in HBC have shown the behavior of the 2 molecules to be very similar, possibly because PR expression is strongly dependent on ERα.14,19,25 In addition, immunohistochemical (IHC) staining for PR is less consistent compared to ERα. 18 In the current study, ERα was used as an indicator for HR expression. For example, it is well known that ERα+ HBC has significantly better outcomes when treated with selective estrogen receptor modulators and aromatase inhibitors.3,12,15,38 Thus, more research in needed on both HBC and CMT to understand the relationship between ERα expression and tumor behavior.
Estrogen receptor–alpha localizes in the nucleus, plasma membrane, and cytoplasm. 26 Nuclear ERα (ERαN) regulates gene transcription by 2 pathways: 1) the direct and/or classical pathway in which ERαN binds to the estrogen-responsive element in the promoter region; 2) the indirect and/or nonclassical pathway where it binds to a non–estrogen-responsive element thus indirectly regulating gene transcription. Extranuclear ERα (ERαC) in the plasma membrane or cytoplasm is activated by ligand binding and is then translocated to the nucleus, initiating a signaling cascade to activate ERαN.27,40
Human epidermal growth factor receptor 2 is a member of the HER family, which also includes HER1, HER3, and HER4. Under physiological conditions, ligand binding initiates dimerization of HER family receptor molecules followed by activation of signaling pathways relevant for cell proliferation and survival. Overexpression leads to excessive non–ligand-dependent HER2 dimerizations, hence playing a role in tumor growth and drug resistance exhibited by many tumors.2,24 As such, the level of HER2 expression in certain cancers has been used to predict prognosis and response to chemotherapy. In human medicine, for example, trastuzumab, a HER2 antagonist, has been shown to significantly improve prognosis when used as a chemotherapeutic agent and adjuvant treatment for HER2-overexpressing metastatic HBC.13,21,32
Caveolins are plasma membrane proteins that control cell signaling by regulating membrane binding and intercellular transport of essential molecules, such as albumin, cholesterol, endothelial nitric oxide synthase, growth hormone, and insulin. 10 Caveolin-1 (CAV1) is thought to have a significant role in tumorigenesis and is highly expressed in myoepithelial cells, endothelial cells, and adipocytes.10,33 Many HBC studies have found associations between CAV1 expression and basal-like subtypes.16–18 In the current study, the significance and degree of ERα, HER2, and CAV1 expression was evaluated in CMT using IHC and related to the clinical behavior and prognosis of CMT.
Materials and methods
Tissue samples
Used in the present study were tissue specimens from 73 canine mammary gland surgical biopsies submitted to Colorado State University Veterinary Diagnostic Laboratory (CSU-VDL; Fort Collins, Colorado) from May 31, 2001 to July 30, 2003 that were originally fixed in 10% buffered formalin and embedded into paraffin using standard procedures. These specimens were subsequently diagnosed as CMT. The paraffin-embedded tissue specimens were cut into 5-μm sections, mounted on glass slides, and routinely stained with hematoxylin and eosin by the CSU-VDL. All photomicrographs were taken using an inverted microscope with an ORCA-ER cooled interline charge-coupled device camera. a
History
The primary report for each case was reviewed for sex, age at the time of surgery, and alteration status. In addition, a follow-up survey to assess patient prognosis was obtained from the referring veterinarian, which included recurrence of the tumor and the time of death.
Immunohistochemical staining
Canine mammary gland tumor tissues were stained by IHC for ERα, HER2, and CAV1. The following primary antibodies were used: mouse anti-human ERα b monoclonal antibody (mAb), polyclonal rabbit anti-human HER2, c and polyclonal rabbit anti-human CAV1. d Canine uterine tissue, human mammary carcinoma, and capillary endothelial cells were used as positive controls for ERα, HER2, and CAV1, respectively. The incubation with the corresponding primary antibody was omitted to provide a negative control for each sample.
For the ERα IHC, sections were deparaffinized, cleared in xylene, and rehydrated in descending concentrations of ethanol (100%, 95%, 75%, 50%). The ERα antigen was retrieved using antigen retrieval solution (pH 9.0) e in a pressure cooker f for 1 min. at 125°C. Slides were cooled in distilled water (dH2O) for 1 min and placed in an incubator at 37°C for 15 min. g Commercial background blocking reagent h and hydrogen peroxide at 37°C for 20 min was used to prevent nonspecific binding. Following an overnight incubation with mouse anti-human ERα b mAb diluted 1:50 in antibody diluent e at 4°C, slides were washed in Tris buffered saline 0.005% Triton adjusted pH 7.6. After which, the slides were reacted with secondary antibodies to conjugated horseradish peroxide–labeled polymer, i and the 3,3′-diaminobenzidine (DAB) j system was used to visualize the reaction after counterstaining with Gill hematoxylin. Finally, the slides were dehydrated in ascending concentrations of ethanol (50%, 75%, 95%, 100%), cleared in xylene, and then mounted, and coverslipped. All procedures were performed at room temperature unless indicated.
Description of the immunohistochemical evaluation for the target ERα
In evaluation of target ERα, each sample was examined for the expression of both the nuclear and extranuclear ERα components. Tissues positivity was determined as a percentage of positively stained nuclei. This percentage was determined by counting the positive and negative nuclei in 10 representative fields per section. Tissues were considered positive for ERαN and/or ERαC when ≥5% of tumor cells were stained for nuclei and membrane and/or cytoplasm, respectively. This scoring system is the most commonly used method for IHC studies on CMT.28,31 The status for ERαN staining was used as described in the HBC 5-subtype classification.4,8,13,28,29,32
For the HER2 and CAV1 IHC, after the sections were deparaffinized and rehydrated in xylene and in descending concentrations of ethanol as described above, HER2 and CAV1 antigens were retrieved with antigen retrieval solution k by microwaving for 2 min 30 sec at 700 W and then for 10 min at 200 W. Following this step, the slides were cooled in dH2O and incubated for 15 min at 37°C. l Slides were incubated with 1.5% goat serum m and hydrogen peroxide at 37°C for 20 min to prevent nonspecific binding, and then labeled with 1:500 diluted polyclonal rabbit anti-human HER2 c or 1:100 diluted polyclonal rabbit anti-human CAV1 d for 15 min. Following antibody labeling, CAV1 and HER2 slides were washed for 5 min in buffered saline. The CAV1 and HER2 slides were then incubated for 30 min at 37°C with goat anti-rabbit biotinylated secondary antibody. n Following primary antibody labeling, CAV1 and HER2 slides were washed with buffered saline. The CAV1 and HER2 slides were then incubated with avidin biotinylated horseradish peroxidase complex o for 30 min at 37°C. Slides were visualized with 3-amino-9-ethyl carbazole p and counterstained with hematoxylin for 25 sec as a nuclear counterstain. Slides were then washed for 15 min under dH20 and coverslipped.
Description of the immunohistochemical evaluation for the target HER2
The Food and Drug Administration–approved scoring system for HBC, which is utilized in the HER2 expression Hercep test, q was used to evaluate overexpression of HER2. The scoring system interprets IHC as HER2 positive (3+) for intense membrane staining of >30% of tumor cells, equivocal (2+) for complete membrane staining that is either nonuniform or weak in intensity but with obvious circumferential distribution in ≥10% of tumor cells, and negative (0 or 1+) for no staining or weak and/or incomplete membrane staining regardless of the distribution of stained tumor cells. In the present study, 3+-stained samples were classified as positive and 2+, 1+, and 0 samples as negative.
Description of the immunohistochemical evaluation for the target CAV1
Slides were evaluated for CAV1 expression using the semiquantitative scoring system described previously. 33 Samples were evaluated for staining intensity (0, none; 1, weakly positive; 2, moderately positive; and 3, strongly positive) and the distribution of positively stained tumor cells (0: <1%; 1: 1–9%; 2: 10–24%; 3: 25–49%; and 4: 50–100%). The samples were considered positive if the sum of the scores for the staining intensity and the distribution of stained tumor cells were ≥4. This scoring system was described as being more significantly related to the survival period than methods used in other studies. 30 On the basis of histomorphology and of the 3 molecular markers (ERα, HER2, and CAV1), all tumors were classified into 5 subtypes (Table 5).
Histologic evaluation
Slides were evaluated for growth pattern (ductular, papillary, or solid), invasion pattern (expansile, local, regional, nodal, or vascular), percent necrosis, mitotic index (number of cells with mitotic figure per 10 high-power fields from the neoplastic area with mitotic activity), degree of scirrhous reaction, degree of anaplasia, and degree of inflammation (0: none; 1: mild; 2: moderate; and 3: marked). The morphologic diagnosis of the CMT was based on the classification system developed previously. 5 Based on this method, the classification of benign mammary tumors includes adenoma simple (AdS), adenoma complex (AdC), benign mixed (BM), lobular hyperplasia (LH), ductular hyperplasia (DH), and ductular papilloma (DP). The malignant classification includes adenocarcinoma simple (AS), adenocarcinoma complex (AC), ductular carcinoma (DC), and ductular papillary carcinoma (DPC). Tumors that were too poorly differentiated to be diagnosed morphologically were classified as solid carcinoma (SC). Simple adenoma and/or adenoenocarcinoma has either an epithelial or a myoepithelial component, and complex adenoma and/or adenocarcinoma has both an epithelial and myoepithelial component. All samples were also classified according to their morphologic origin, either lobular or ductular in origin. Lobular origin includes AdS, AdC, BM, LH, AS, and AC. Ductular origin includes DH, DP, DC, and DPC. Solid carcinoma was excluded from either origin. 5 All microscopic evaluations were carried out by 2 board-certified veterinary pathologists.
Statistical analysis
In the current study, 2 different perspectives—1) positive immunoreactivity of each molecular marker and 2) a 5-subtype classification scheme—were used to analyze the correlation with the behavior and prognosis of the tumors. All statistical analyses were performed using commercial software. r To analyze the correlation with the positivity of each marker, Mann–Whitney test and Fisher exact test were used, and the correlation with the 5 subtypes were analyzed by analysis of variance (Kruskal–Wallis test) with Dunnett posttest. The Kaplan–Meier survival curve with log-rank test was used to analyze the disease-free interval and the overall survival. The level of significance was fixed at P < 0.05.
Results
History
All 73 cases were females, 21 (29%) spayed and 52 (71%) intact. There were more intact than spayed females regardless of molecular marker staining or tumor subtype. The age of onset was obtained from 67 cases. The mean age was 8.6 years, and there was no significant age difference between marker positivity and among subtypes (Table 1).
Five-subtype classification.*
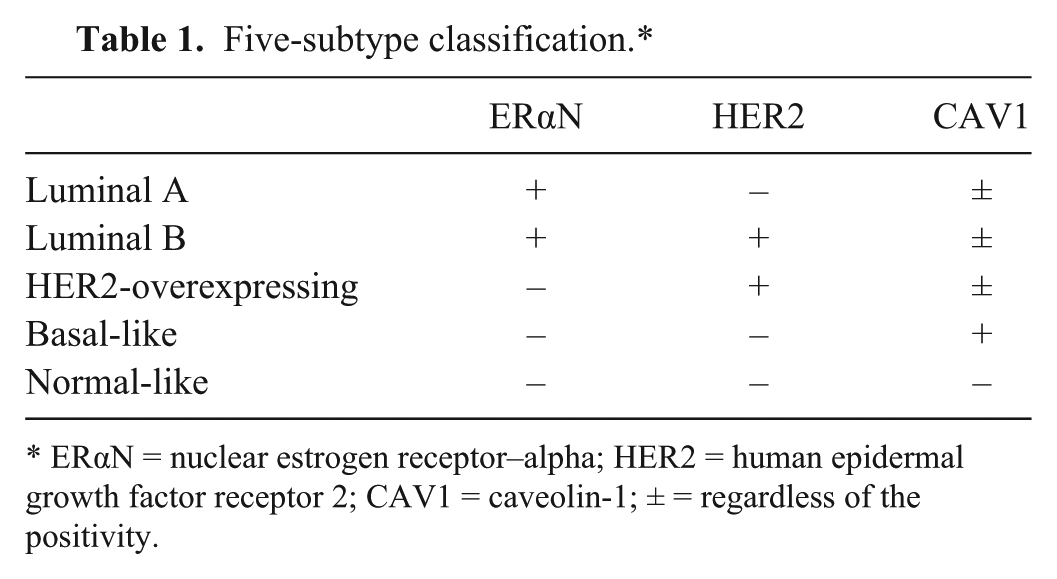
ERαN = nuclear estrogen receptor–alpha; HER2 = human epidermal growth factor receptor 2; CAV1 = caveolin-1; ± = regardless of the positivity.
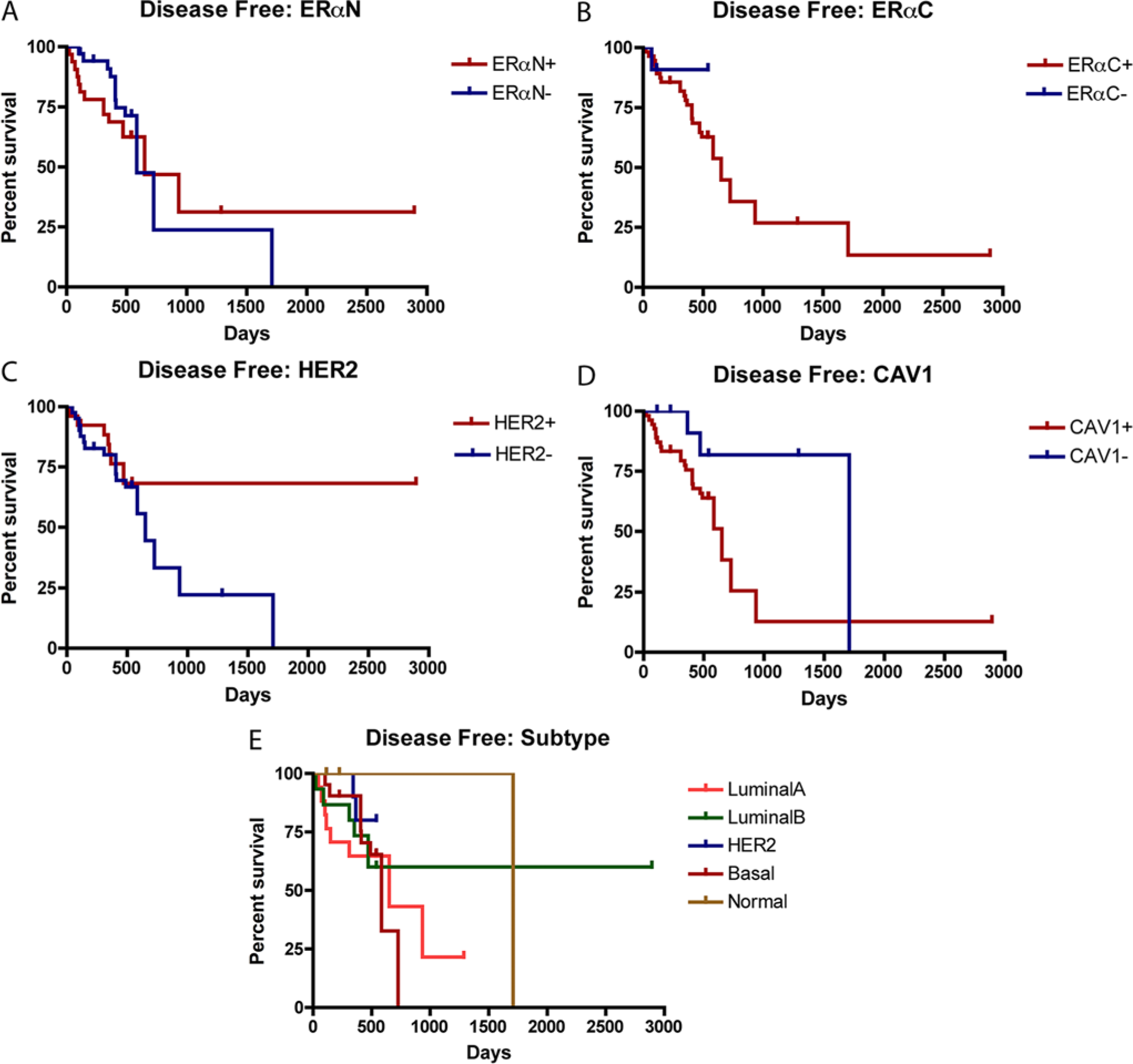
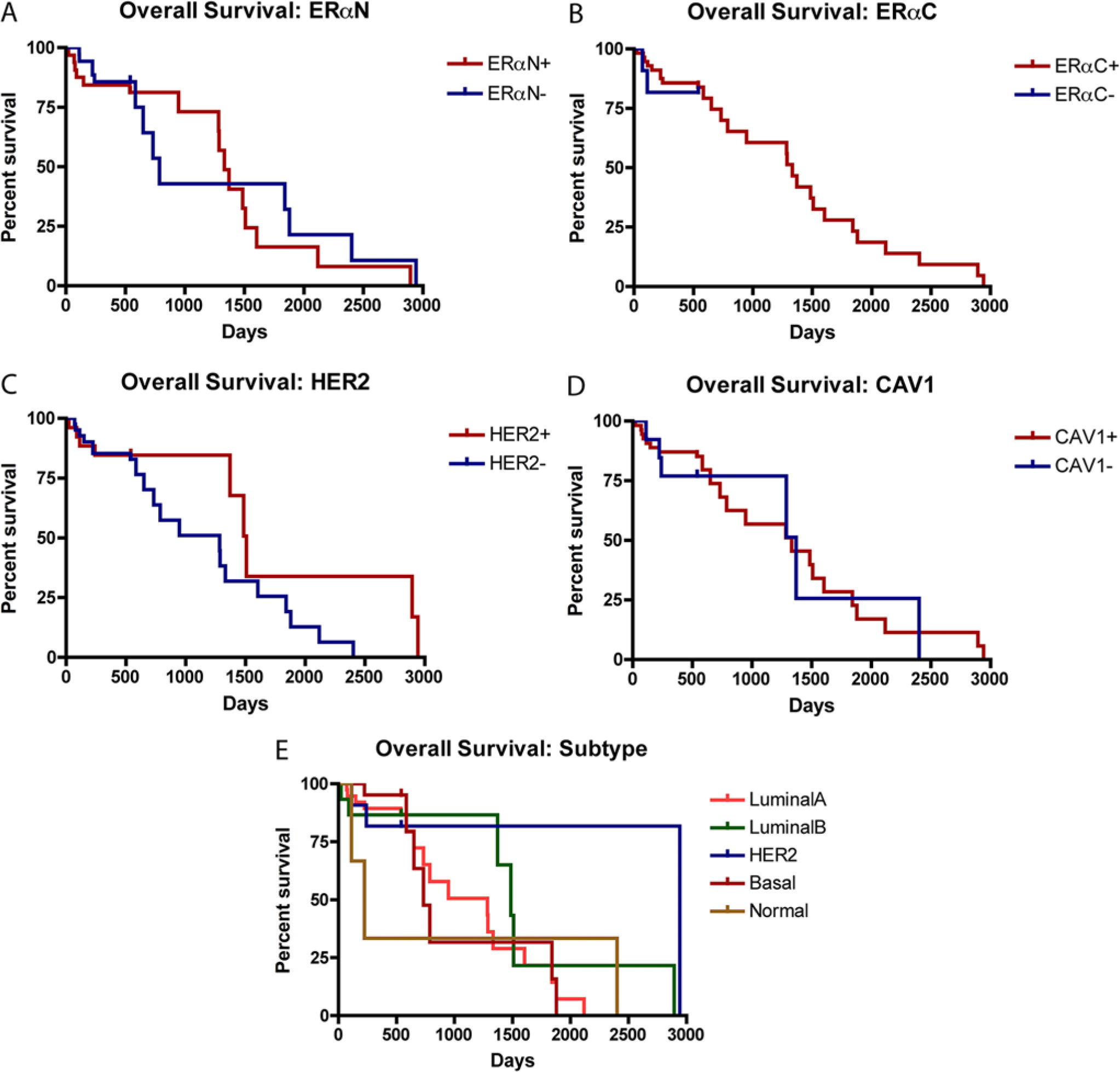
Follow-up surveys were obtained from 69 cases (94.5% of total cases) with the longest follow-up period of 2,942 days after diagnosis. Out of these cases, 27 cases (39%) had recurrence of mammary tumors and 31 (42%) cases were deceased at the time of the report. ERαC+ tumors (44%) had significantly higher (P = 0.011) recurrence rate than ERαC– tumors (8%), and HER2+ tumors (29%) had significantly lower (P = 0.019) recurrence rate than HER2– tumors (43%). There were no significant differences in percentage of recurrence among other markers or among the subtypes. The median (50%) disease-free interval and the median (50%) overall survival for all 69 cases were 650 days and 1,333 days, respectively. ERαN– tumors had the shortest (584 days) and CAV1– tumors had the longest (1,709 days) median (50%) disease-free interval. ERαN– tumors had the shortest (788 days) and HER2+ tumors had the longest (1,509 days) median (50%) overall survival (Table 2). In terms of subtype, HER2 subtype had the lowest percentage of recurrence (18%), basal-like subtype had the shortest (584 days), and normal-like subtype had the longest (1,709 days) median (50%) disease-free interval. Normal-like subtype had the shortest (224 days) and HER2 subtype had the longest (2,942 days) median (50%) overall survival (Table 1). There were no significant differences between the positivity of markers among the subtypes (Figs. 1, 2).
History and follow-up information marker status.*
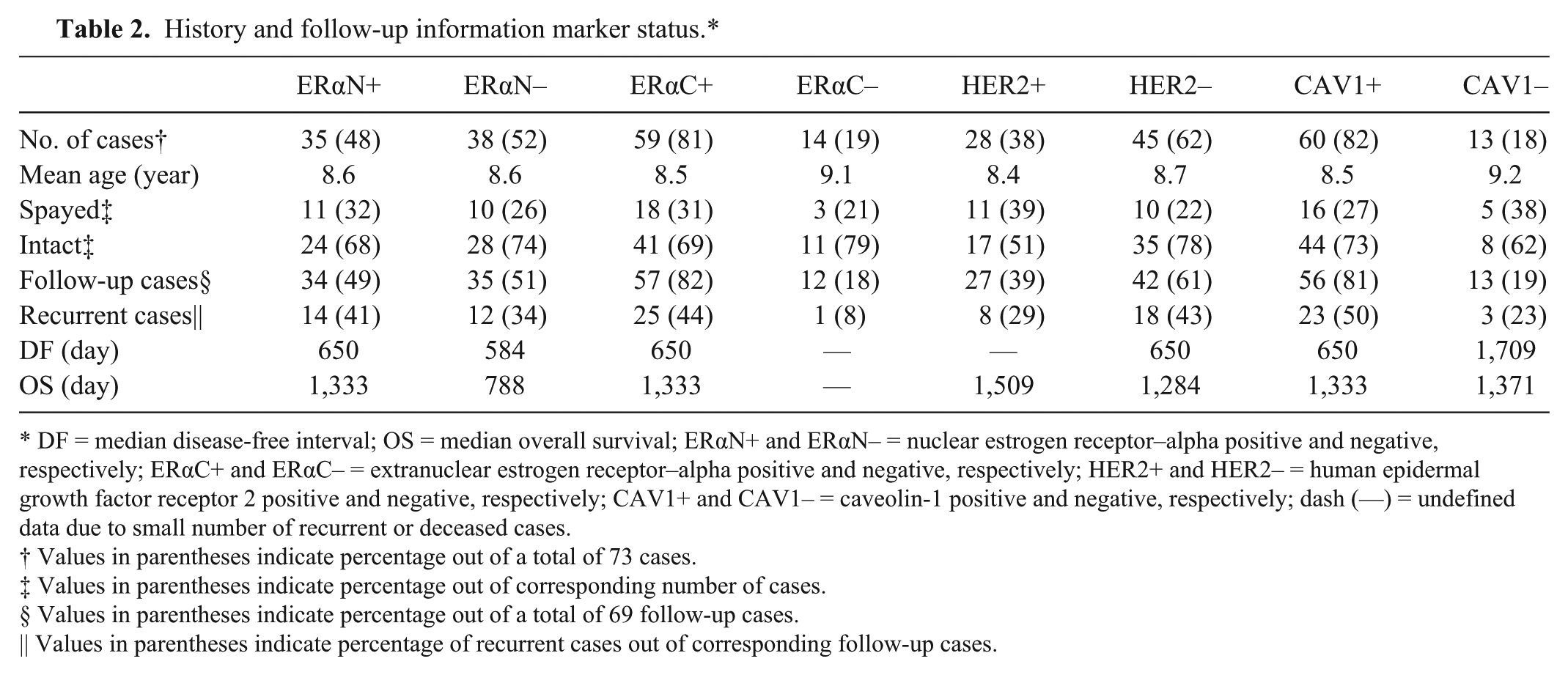
DF = median disease-free interval; OS = median overall survival; ERαN+ and ERαN– = nuclear estrogen receptor–alpha positive and negative, respectively; ERαC+ and ERαC– = extranuclear estrogen receptor–alpha positive and negative, respectively; HER2+ and HER2– = human epidermal growth factor receptor 2 positive and negative, respectively; CAV1+ and CAV1– = caveolin-1 positive and negative, respectively; dash (—) = undefined data due to small number of recurrent or deceased cases.
Values in parentheses indicate percentage out of a total of 73 cases.
Values in parentheses indicate percentage out of corresponding number of cases.
Values in parentheses indicate percentage out of a total of 69 follow-up cases.
Values in parentheses indicate percentage of recurrent cases out of corresponding follow-up cases.
Disease-free interval.
Overall survival.
Immunohistochemical staining
Seventy-three cases were examined for ERα, HER2, and CAV1 (Fig. 3). Thirty-five cases (48%) were ERαN+, and 38 cases (52%) were ERαN–. Fifty-nine cases (81%) were ERαC+, and 14 cases (19%) were ERαC–. Twenty-eight cases (38%) were HER2+, and 45 cases (52%) were HER2–. Sixty cases (82%) were CAV1+, and 13 cases (18%) were (CAV1–; Table 2). Extranuclear ERα staining was either completely positive or completely negative.

Immunohistochemical staining status of canine mammary gland tumor. Bars = 50 μm.
Seventy-three cases were classified into 5 molecular subtypes according to the expression of 3 markers; this subtype classification scheme is a modification of the published HBC scheme13,18,20 and used ERα markers for HR in CMT samples instead of ERα and PR used for HRs in evaluating HBC. Eighteen cases (25%) were classified as luminal A subtype, 17 cases (23%) were classified as luminal B subtype, 11 cases (15%) were classified as HER2-overexpressing subtype, 24 cases (33%) were classified as basal-like subtype, and 3 cases (4%) were classified as normal-like subtype (Table 3).
History and follow-up information subtype.*
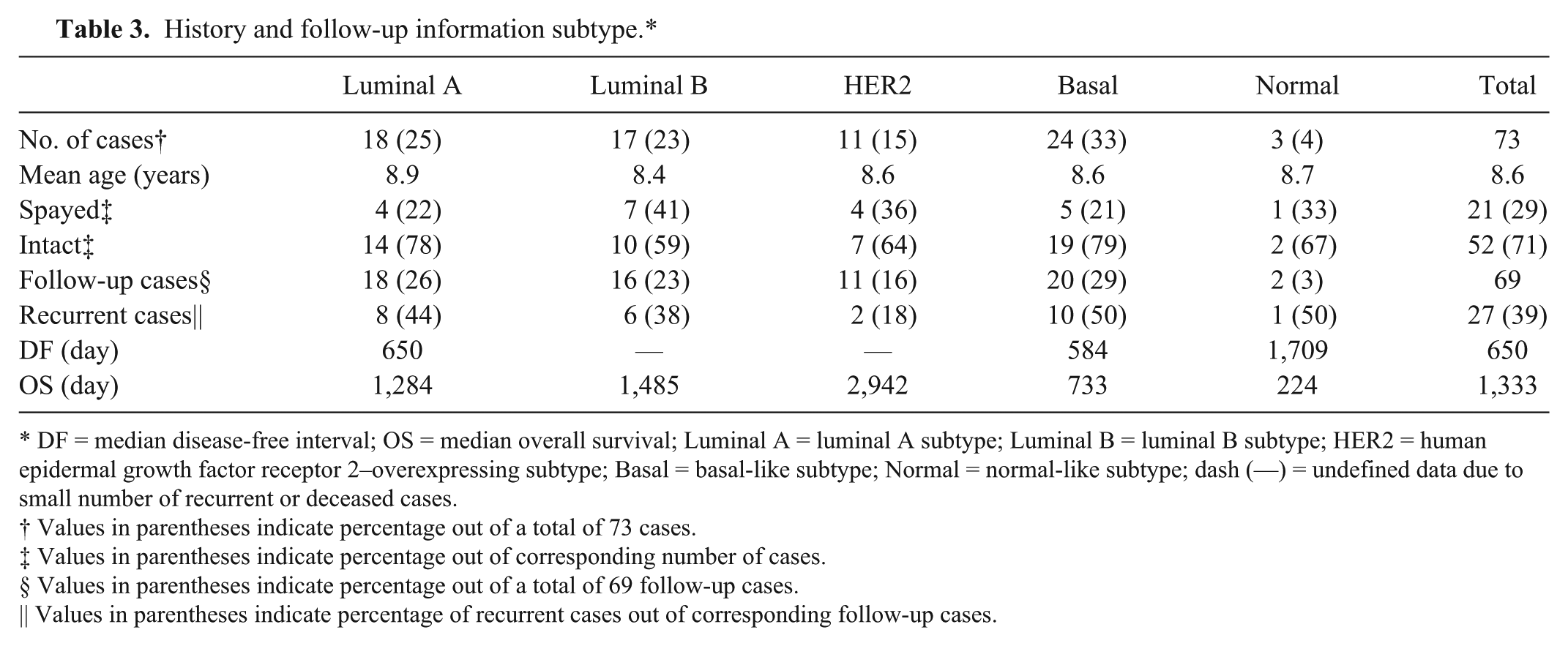
DF = median disease-free interval; OS = median overall survival; Luminal A = luminal A subtype; Luminal B = luminal B subtype; HER2 = human epidermal growth factor receptor 2–overexpressing subtype; Basal = basal-like subtype; Normal = normal-like subtype; dash (—) = undefined data due to small number of recurrent or deceased cases.
Values in parentheses indicate percentage out of a total of 73 cases.
Values in parentheses indicate percentage out of corresponding number of cases.
Values in parentheses indicate percentage out of a total of 69 follow-up cases.
Values in parentheses indicate percentage of recurrent cases out of corresponding follow-up cases.
Morphologic classification
Adenocarcinoma simple was the most common morphological type among the 73 samples. There were significant differences in the trend of morphological pattern for positivity of ERαN (P < 0.001) and ERαC (P < 0.0001; Table 4; Fig. 4). ERαN+ had higher distribution of AdC, DPC, and SC, whereas ERαN– had higher distribution of LH, AS, and DC. Extranuclear estrogen receptor–alpha positive had higher distribution of AdS, AdC, DH, DC, and DPC, and ERαC– had higher distribution of LH, DP, AS, and SC. There were no significant differences among subtypes regarding the morphological pattern (Table 5; Fig. 5). When differentiating the morphological patterns into lobular or ductular origin, the lobular origin had much higher percentage overall, regardless of the markers’ positivity or subtypes (Tables 4, 5; Figs. 4, 5). The distribution of benign tumors was slightly lower than that of malignant tumor without regard to the positivity of the markers or subtypes, though no statistical significance was observed (Tables 4, 5; Figs. 4, 5).
Histologic evaluation marker status.*
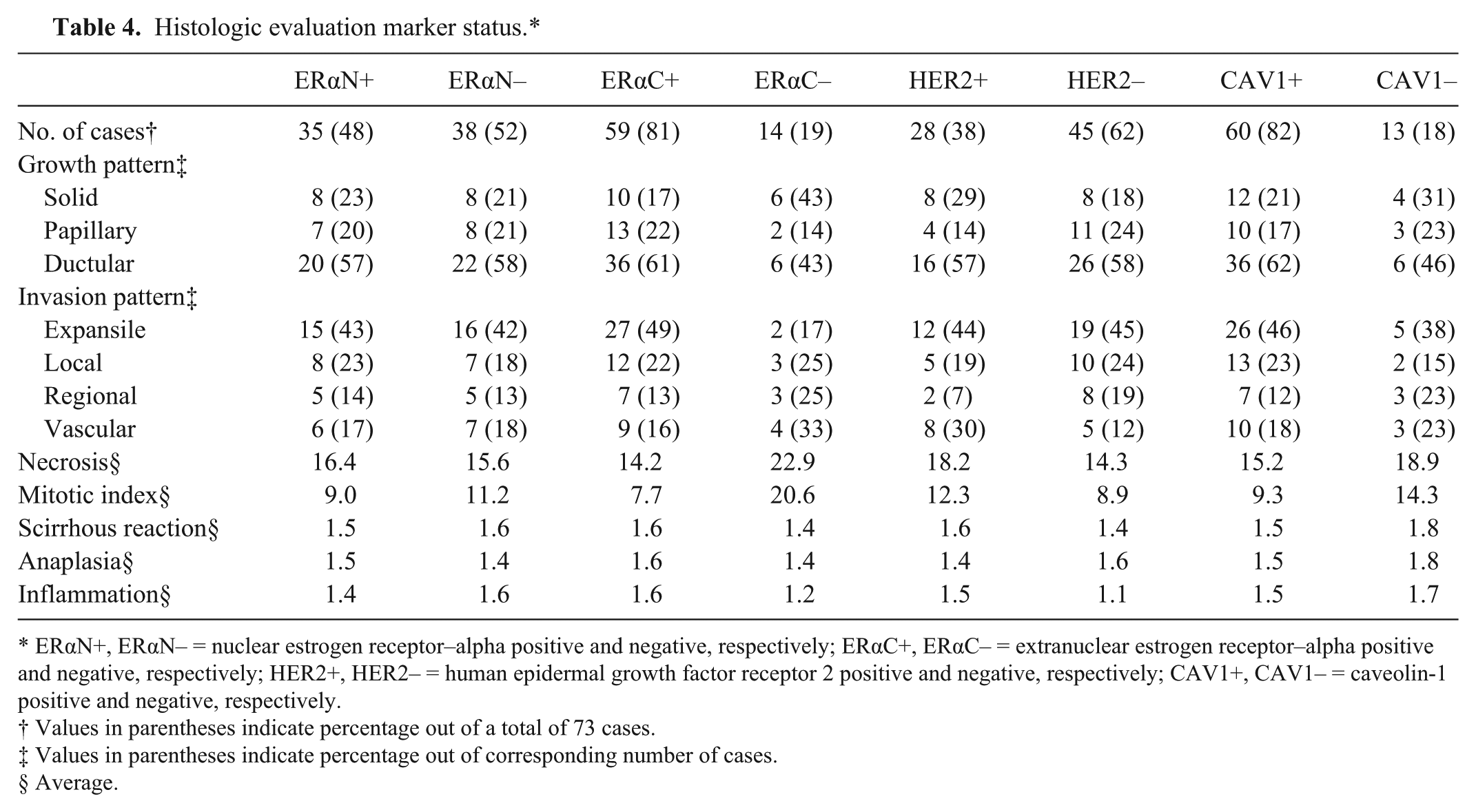
ERαN+, ERαN– = nuclear estrogen receptor–alpha positive and negative, respectively; ERαC+, ERαC– = extranuclear estrogen receptor–alpha positive and negative, respectively; HER2+, HER2– = human epidermal growth factor receptor 2 positive and negative, respectively; CAV1+, CAV1– = caveolin-1 positive and negative, respectively.
Values in parentheses indicate percentage out of a total of 73 cases.
Values in parentheses indicate percentage out of corresponding number of cases.
Average.
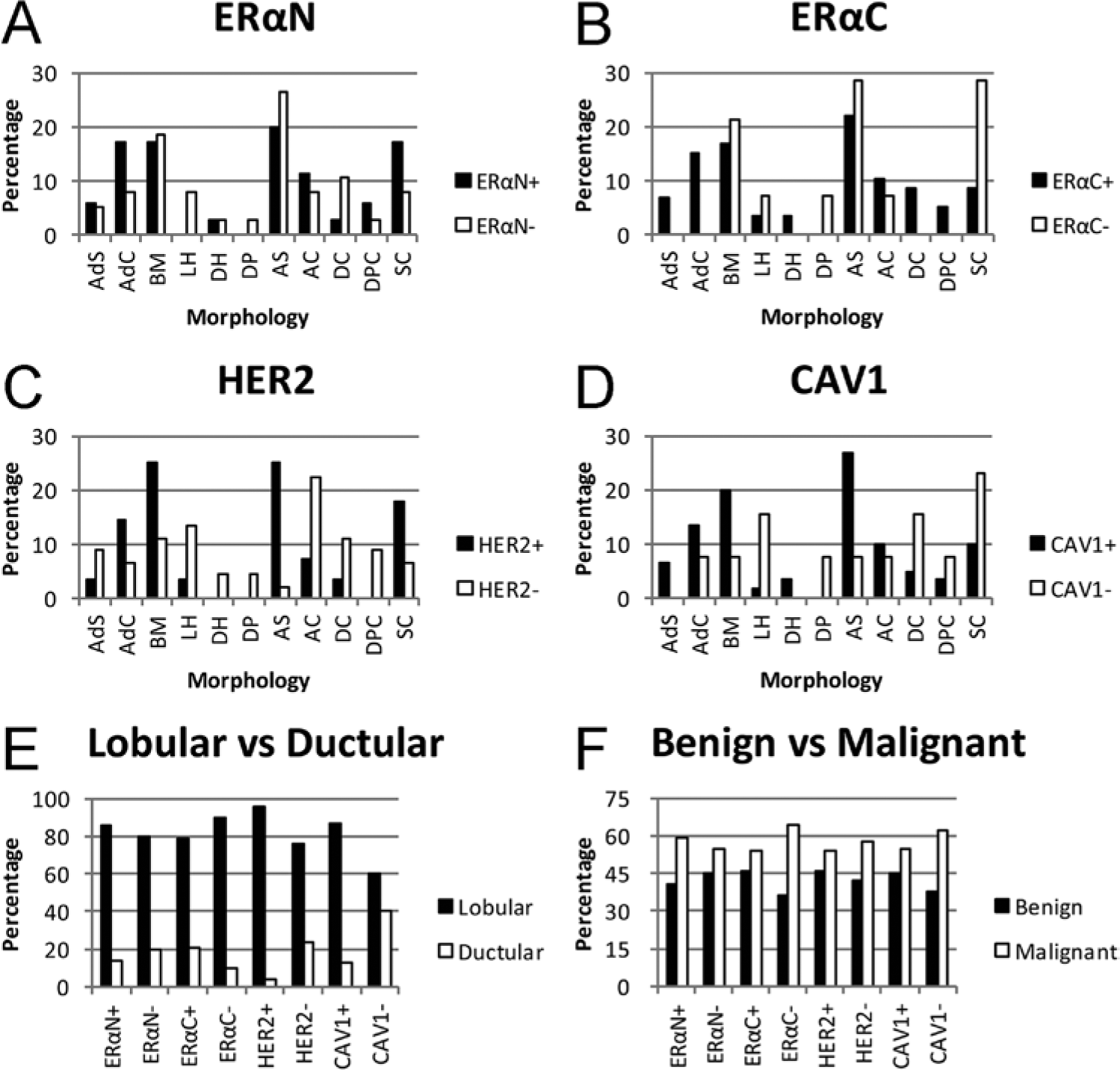
Morphological evaluation according to molecular marker: distribution of morphological classification.
Histologic evaluation subtypes.*
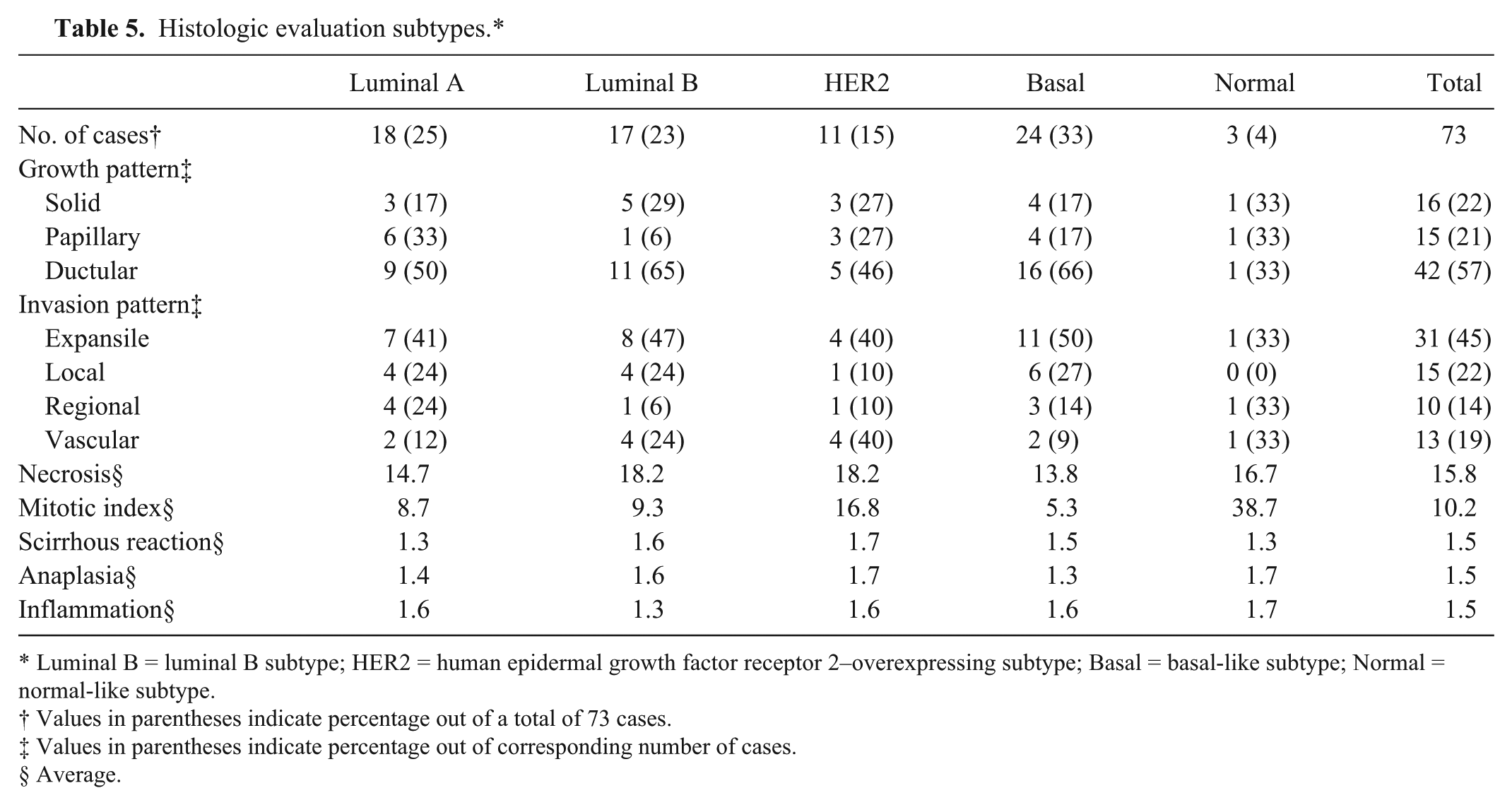
Luminal B = luminal B subtype; HER2 = human epidermal growth factor receptor 2–overexpressing subtype; Basal = basal-like subtype; Normal = normal-like subtype.
Values in parentheses indicate percentage out of a total of 73 cases.
Values in parentheses indicate percentage out of corresponding number of cases.
Average.
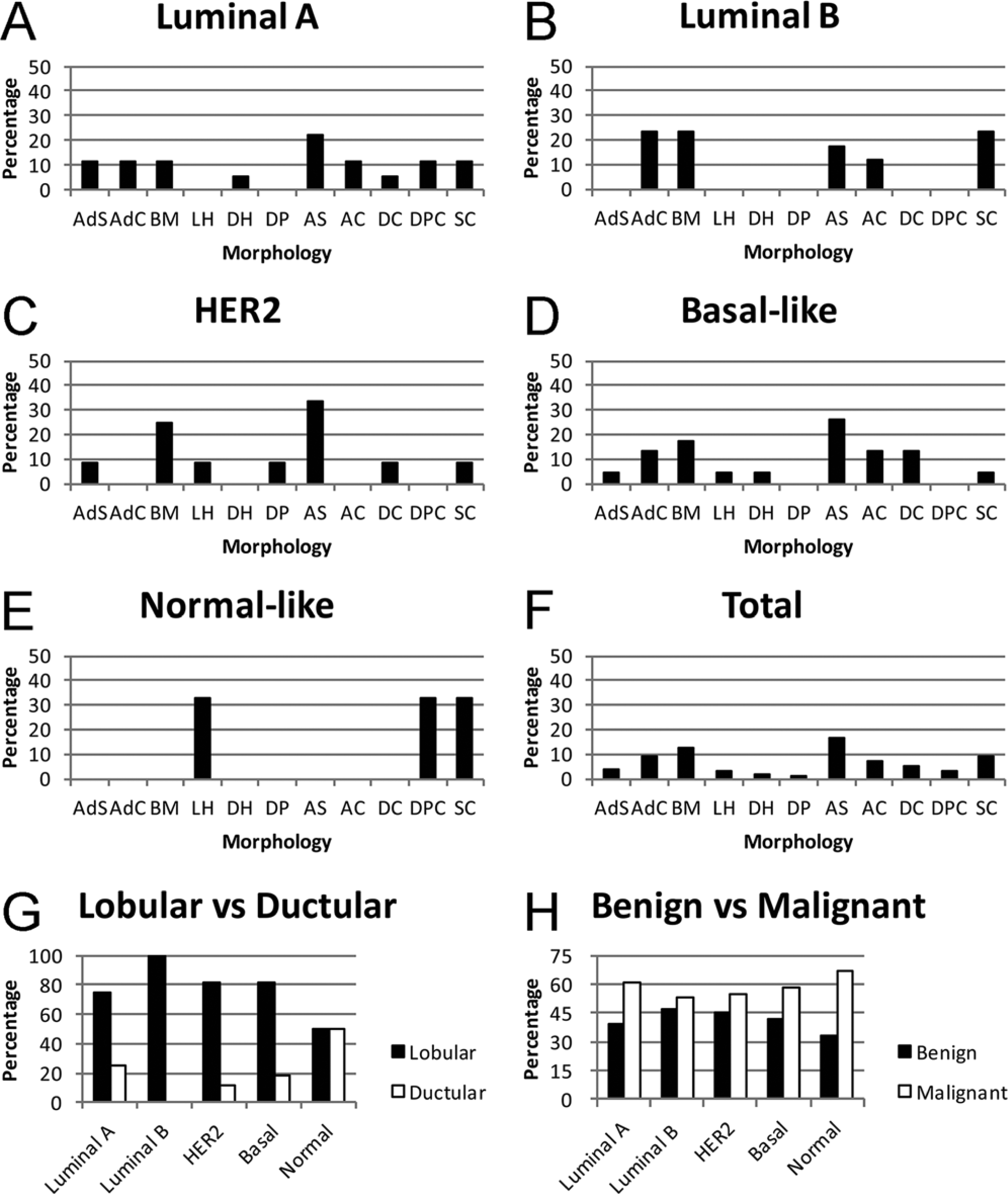
Morphological evaluation according to 5 subtypes: distribution of morphological classification.
Histologic evaluation
Analysis of growth pattern showed the highest percentage was of the ductular pattern regardless of the positivity of the markers. For invasion, the expansile pattern was the most common except for the ERαC– tumors, which did not appear to have a distinctive dominant pattern (Tables 1–6). Luminal A subtype (50%), luminal B subtype (65%), HER2+ subtype (46%), and basal-like subtype (66%) had the ductular pattern as the highest percentage. Luminal A subtype (41%), luminal B subtype (47%), and basal-like subtype (50%) had the largest distribution of the expansile pattern, and HER2 subtype had expansile (40%) and vascular (40%) as the predominant invasion patterns (Table 7). There were no significant differences in the growth and invasion pattern between the positivity of the markers and among the subtypes. The percentage necrosis of ERαC+ (7.7%) was significantly lower (P = 0.048) than that of ERαC– tumors (20.6%). On the other hand, the degree of anaplasia was significantly lower (P = 0.041) in CAV1+ than CAV1– tumors. There were no significant differences between the positivity of markers and among the 5 subtypes based on other histologic criteria.
Distribution of morphological type indicated in percentage out of corresponding marker status.*
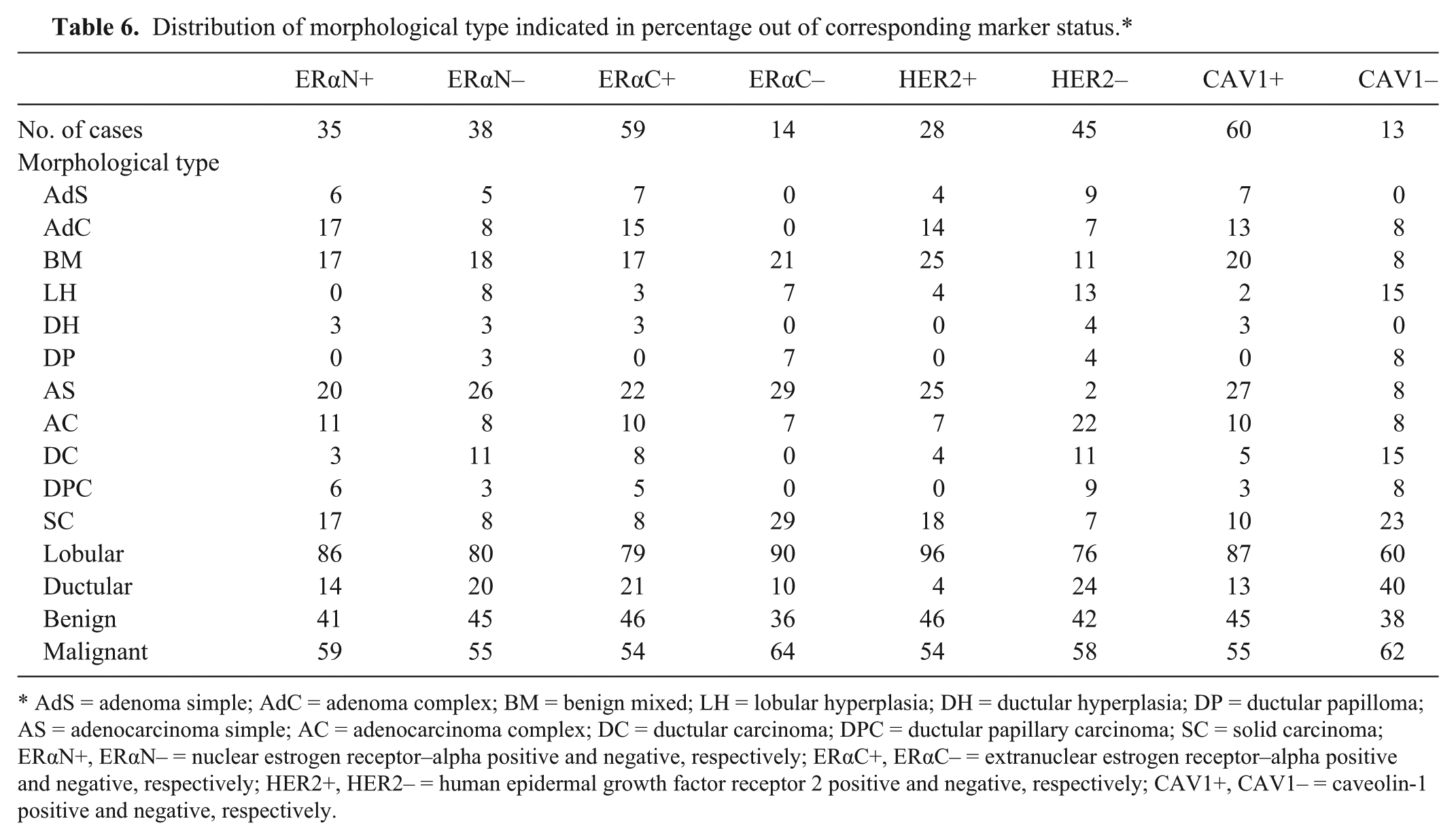
AdS = adenoma simple; AdC = adenoma complex; BM = benign mixed; LH = lobular hyperplasia; DH = ductular hyperplasia; DP = ductular papilloma; AS = adenocarcinoma simple; AC = adenocarcinoma complex; DC = ductular carcinoma; DPC = ductular papillary carcinoma; SC = solid carcinoma; ERαN+, ERαN– = nuclear estrogen receptor–alpha positive and negative, respectively; ERαC+, ERαC– = extranuclear estrogen receptor–alpha positive and negative, respectively; HER2+, HER2– = human epidermal growth factor receptor 2 positive and negative, respectively; CAV1+, CAV1– = caveolin-1 positive and negative, respectively.
Distribution of morphological type indicated in percentage out of corresponding subtype.*
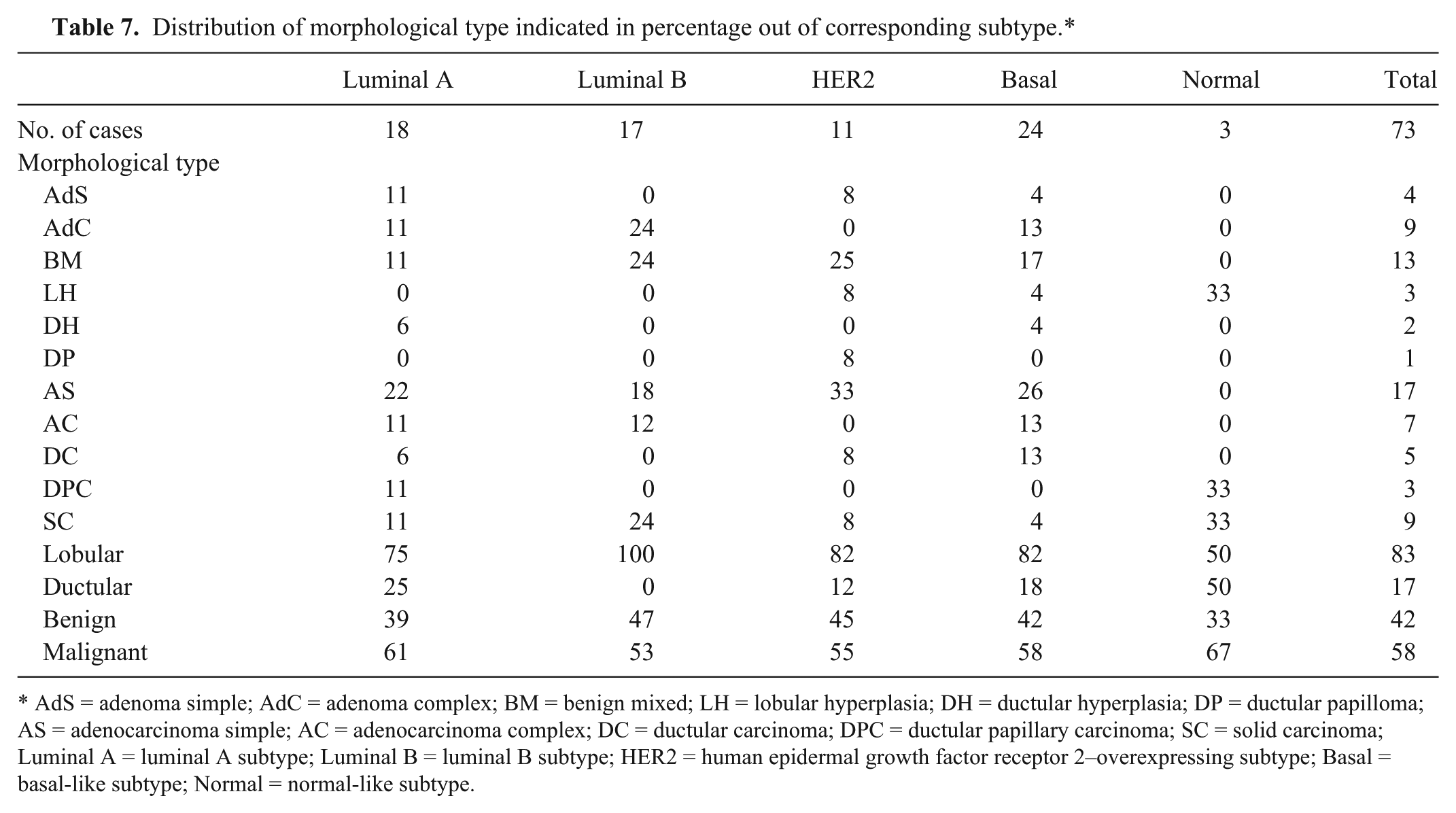
AdS = adenoma simple; AdC = adenoma complex; BM = benign mixed; LH = lobular hyperplasia; DH = ductular hyperplasia; DP = ductular papilloma; AS = adenocarcinoma simple; AC = adenocarcinoma complex; DC = ductular carcinoma; DPC = ductular papillary carcinoma; SC = solid carcinoma; Luminal A = luminal A subtype; Luminal B = luminal B subtype; HER2 = human epidermal growth factor receptor 2–overexpressing subtype; Basal = basal-like subtype; Normal = normal-like subtype.
Discussion
Results of the current study showed a high proportion of ERαC+ staining at 82%, and the distribution of positively stained neoplastic cells of ERαN at 48%, HER2 at 38%, and CAV1 at 82% were consistent with previous IHC studies on CMT.2,7,29 However, to the authors’ knowledge, there is no canine study reporting IHC for ERαC. When the tumors were classified into 5 subtypes according to IHC, the basal-like subtype (24 cases, 33%) was the most common, followed by luminal A subtype (18 cases, 25%), luminal B subtype (17 cases, 23%), HER2-overexpressing subtype (11 cases, 15%), and normal-like subtype (3 cases, 4%). Among the few CMT studies that have used a subtype classification with IHC, only ERα was used as the hormone receptor. 21 The distribution of CMT for each subtype in a study performed previously, 21 was 44.8% for luminal A subtype, 13.5% for luminal B subtype, 8.3% for HER2 subtype, 29.2% for basal-like subtype, and 4.2% for negative/null (equivalent to normal-like in this study). 21 Compared with previous studies4,21,31,32 the present data shows a lower distribution of luminal A subtype and higher distribution of luminal B subtype. This could be explained by the higher immunoreactivity of HER2 (38%) seen in the present study unlike that reported previously. 21 This discrepancy could also be attributed to the use of primary antibodies from different manufacturers, though both studies used the same scoring system. The factors contributing to the variance in subtype distribution may be different basal cell markers. “Basal-like” was named originally for HBC, which indicates its transcriptome is similar to that of basal/myoepithelial cells. 16 However, there are a number of candidates for this particular subtype because of the abundance of markers for this cell type. For example, previous studies on CMT used P-cadherin, 21 CK 5/6,4,32 CK14, 21 and p63. 32 The lack of consistency in markers used for basal-like subtype has been discussed previously, but there is no set definition despite the pursuit to identify the molecule that represents this subtype. 36 In the present study, CAV1 was used as the marker for basal-like subtype because it is strongly expressed in myoepithelial and epithelial cells of normal human breast and canine mammary tissue.1,30 Many human and canine studies found that the correlation between CAV1 expression and prognosis varies among tumor types, showing that CAV1 overexpression indicates either better or worse prognosis depending on the type of cancer.1,30,33 CAV1 is one of the components of caveolae, which is the membrane invaginations for various cell types. CAV1 acts as an anchor for many signaling molecules and regulates important cellular signaling cascades that relate to cell proliferation and survival. 10 The data from the present study suggests that loss of CAV1 expression is significantly associated with a higher degree of anaplasia, as seen in Figure 2. Loss of CAV1 function may lead to disruption of organized signaling pathway(s) that are important in cell growth and metabolism, which results in loss of cellular differentiation and organization. A previous study 30 evaluated the IHC characteristics of CAV1 in different cell types in CMT and found that the molecular marker is expressed in luminal epithelial cells or myoepithelial cells depending on the level of malignancy of the tumor. 30 Data obtained in the present study did not distinguish the type of cells that were stained for CAV1. However, differentiating cell types with CAV1 immunoreactivity status may uncover stronger associations of CMT with CAV1 expression and/or subtypes. Another possible factor that plays into the lower population of luminal subtypes in the results of the present study compared to previous studies4,21,31,32 may be the use of ERα as the sole HR marker. Many studies use ERα and PR expression when evaluating HR status in CMTs. However, in human medicine, ERα is the only HR with proven significant effect on clinical treatment and prognosis for HBC. 15 Moreover, the behavior of PR strongly depends on ER, and the status of PR is less consistent.18,25 Hence, it is logical to use ERα as the indicator of HR.
Estrogen receptor–alpha status showed strong statistical significance (ERαN: P < 0.001; ERαC: P < 0.0001) to the distribution of CMT morphological types. Another study 37 stated that human beings, dogs, and cats share the same major binding site for ERα to its endogenous ligands and selective estrogen receptor modulators. 37 The strong association between ERα and morphology may suggest the possibility of determining ERα status by routine microscopic diagnosis for future prognostic determination or treatment decision for CMT. The result of the follow-up survey revealed that the shortest median disease-free interval and median overall survival was for tumor staining ERαN–. The loss of hormone dependency corresponding to unfavorable outcome in CMT has been previously described, as tumors with ERαN expression have a shorter disease-free interval 29 and overall survival. 28 The evaluation of positivity of the ERαC indicated that ERαC+ had significantly lower percentage necrosis and significantly higher recurrence rate that ERαC–. There is evidence that membrane ERα interacts with transmembrane receptor, which trigger signaling cascade that contributes to phosphorylation of enzymes and ligand-independent activation of ERαN. 27 In addition, cytoplasmic ERα prevents intrinsic cell death that is initiated by mitochondrial disruption. 27 Thus, it can be predicted that the presence of ERαC contributes to the integrity of tumor cells and that overexpression of this marker might lead to higher susceptibility and loss of control of the cell cycle, perhaps leading to a higher recurrence rate. The importance of ERαC function in HBC is attracting more attention in human research, but the results are controversial.22,27 Studies have shown that membrane ERα may set in caveolae, and therefore function of this marker might be related to CAV1 activity.6,9 Nevertheless, there is no research either regarding the relationship between ERα and CAV1 or the cross-talk between ERαN and ERαC in CMTs. Results in the current study did not show correlation between the expression of these markers. Revealing the behavior and interaction between these molecular markers would open a new understanding on CMT diagnosis and treatment.
The recurrence rate for HER2+ tumors was significantly lower for HER2– masses. In addition, HER2-overexpressing subtype had the lowest recurrence rate (18%) than any other subtype (luminal A: 44%; luminal B: 38%; basal-like: 50%; normal-like: 50%). Such results contradict HBC research, where HER2-overexpressing HBC has poor prognosis, including higher recurrence rates. 34 However, IHC studies on CMT revealed HER2 expression was associated with a better prognosis.20,23 This disparity leads to the possibility of different roles for HER2 between HBC and CMT.
Although some trends were seen, the present data was not statistically strong enough to support the correlation between the 5 subtypes and behavior or prognosis of CMT. However, further assessment of the expression of 3 makers in association with CMT is still needed. Finally, some contradicting results between HBC and CMT lead the authors to postulate careful interpretation of CMT research when used as a model for HBC, though these 2 species share many common features regarding neoplasia.21,28,33
Footnotes
a.
Zeiss 200M, Hamamatsu Photonics, Hamamatsu City, Japan.
b.
Monoclonal mouse anti-human ERα (clone-1D5), Dako North America Inc., Carpinteria, CA.
c.
Polyclonal rabbit anti-human HER2 (C-18), Santa Cruz Biotechnology Inc., Dallas, TX.
d.
Polyclonal rabbit anti-human CAV-1 (N-20), Santa Cruz Biotechnology Inc., Dallas, TX.
e.
Antigen retrieval solution pH 9.0, Dako North America Inc., Carpinteria, CA.
f.
Decloaking chamber, Biocare Medical, Concord, CA.
g.
Sequenza system, Thermo Fisher Scientific, Waltham, MA.
h.
Background sniper, Biocare Medical, Concord, CA.
i.
EnVision+ dual link system-HRP, Dako North America Inc., Carpinteria, CA.
j.
DAB, Vector Laboratories Inc., Burlingame, CA.
k.
Citra solution, BioGenex Laboratories Inc., San Ramon, CA.
l.
Hi Pro slide incubator, Thermo Fisher Scientific, Waltham, MA.
m.
Vector Elite diluted goat serum (Vector Elite), Vector Laboratories Inc., Burlingame, CA.
n.
Vector Elite biotinylated anti-mouse/rabbit secondary antibody, Vector Laboratories Inc., Burlingame, CA.
o.
Vector Elite avidin Biotinylated horseradish peroxidase complex, Vector Laboratories Inc., Burlingame, CA.
p.
AEC, Biomeda, Foster City, CA.
q.
Dako North America Inc., Carpinteria, CA.
r.
GraphPad Prism version 4.00, GraphPad Software Inc., San Diego CA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The funding for this project was provided by the Center for Environmental Medicine and the Animal Cancer Center.