
Abstract
Shoulder ulcerations can be graded postmortem from 0 to 4 on a pathoanatomical scale. However, veterinarians and farmers express difficulties evaluating the grade of the lesions antemortem. Accurate grading is needed in order to comply with veterinary instruction in relation to the Danish legislation, stating that sows with shoulder ulcers grade 3 or 4 must be kept loose and have access to soft bedding. Thus, the aim of the present study was to evaluate if biopsies from the center of a shoulder ulcer can be used to point out animals for which an intervention must be initiated. Postmortem, a punch biopsy was sampled from the center of the ulceration or from the tissue overlaying the tuber spina scapula. Afterward, the shoulders were cross-sectioned and evaluated grossly and histologically (“gold standard”). In total, 121 shoulders were included in the study, and the diagnostic value of a punch biopsy in grading shoulder ulcerations was evaluated. The results showed a sensitivity of 0.78, a specificity of 0.98, a positive likelihood ratio of 38.36, and a negative likelihood ratio of 0.22. The agreement between the cross-section evaluation and the punch biopsy was found to be 0.90 by calculating the Cohen kappa value. In conclusion, a single punch biopsy from the center of an ulcer is useful for determining the grade of a shoulder ulcer and can be used to facilitate the identification of sows with ulcers requiring an intervention.
Development of shoulder ulcerations in sows is a common finding in the modern swine industry.3,9,16,18 The ulcerations are caused by external pressure against the tuber spina scapula,4,7,12,14 and a 2009 study found shoulder ulcerations to be significantly related to the duration of the sows lying bouts (prolonged recumbency). 22 Shoulder ulcerations in sows are a significant animal welfare problem and constitute a portal of entry for bacteria, leading to increased use of antibiotics and rejection of carcasses at meat inspection.7,12,25
A pathoanatomical scale from 0 to 4 can be used to grade shoulder ulcerations postmortem.11,18 Grade 0 describes shoulders with no lesions or lesions related to inter-pig aggressive behavior; grade 1 contains lesions restricted to the epidermis; grade 2 contains lesions involving the dermis, often characterized by a small amount of granulation tissue and fibrosis; grade 3 describes lesions that involve the subcutis where heavy fibrosis and granulation tissue are often present; and grade 4 describes lesions involving all 3 layers of the skin and the underlying bone, which is necrotic and often shows excessive periosteal bone proliferations.
In Denmark, the instruction in relation to shoulder ulcers implies that sows with shoulder ulcerations grade 3 or 4 must be kept loose and have access to soft bedding, 1 which seems to be curative. 15 However, veterinarians and farmers express difficulties evaluating the pathoanatomical grade of the ulcerations (i.e., the depth of the lesions). These difficulties may be overcome by biopsy sampling the ulcers. The aim of the present study was to evaluate if biopsies from the shoulder can be used as a tool for pointing out animals to which an intervention must be initiated according to the veterinary instruction in relation to the Danish legislation. Therefore, grading based on biopsies is compared with the gold standard giving the true grading (100%), which only can be obtained through cross-sectioning the shoulders. 11
Shoulders were sampled from sows from 7 Danish production herds with a high prevalence of shoulder ulcers during September 2009 to January 2010. The sampling pattern was stratified in order to ensure that shoulders with ulcerations of different grades (<5 cm or ≥5 cm in diameter) and shoulders without ulcerations were included (Table 1). All procedures involving living animals were approved by the Danish Animal Experiments Inspectorate in accordance with the Danish legislation.
Antemortem, the sampling of shoulders was stratified ensuring that shoulders with different grades of ulceration (<5 cm in diameter and ≥5 cm in diameter) were included together with shoulders free of ulcerations.*
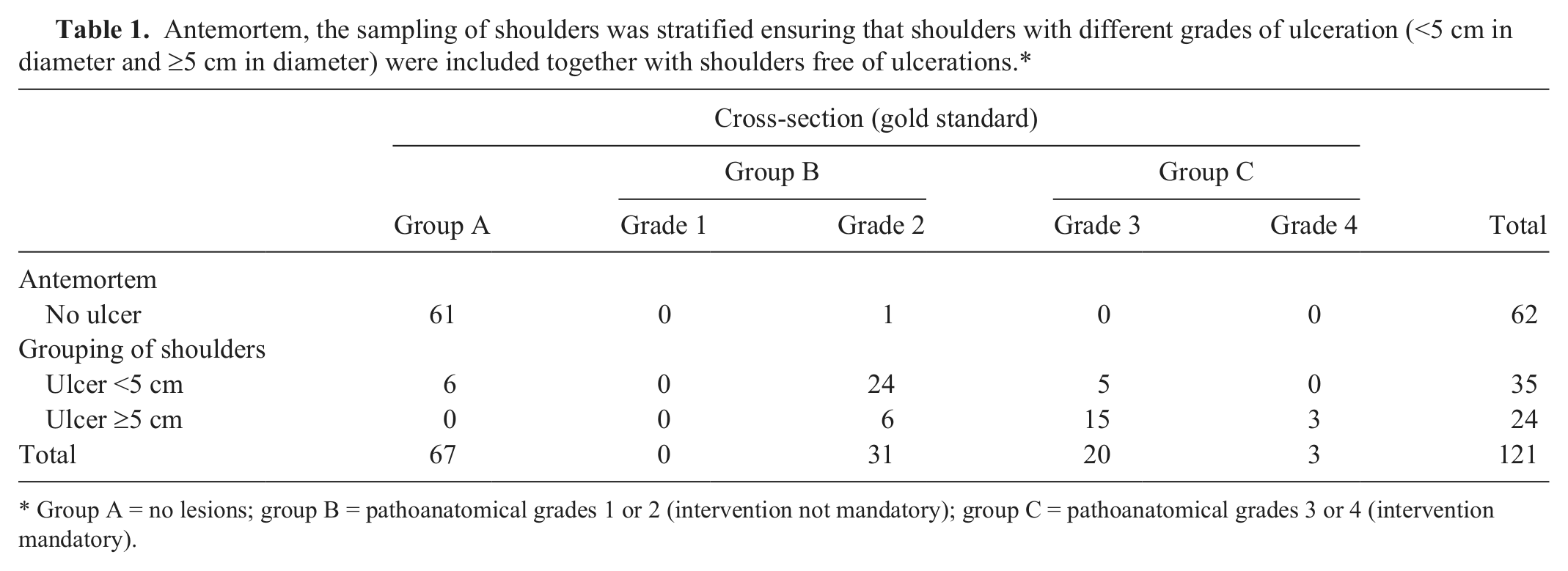
Group A = no lesions; group B = pathoanatomical grades 1 or 2 (intervention not mandatory); group C = pathoanatomical grades 3 or 4 (intervention mandatory).
Postmortem, a punch biopsy (10 mm in diameter) was sampled from the center of the ulceration or, when ulcerations were not present, from the tissue overlaying the tuber spina scapula (Fig. 1). The biopsies were attempted to include all layers of the skin and necrotic bone tissue when present. After sampling of biopsies, the shoulders were cross-sectioned and grossly evaluated as previously described, 11 and tissue was collected for histology (Figs. 2, 3). When an ulcer was present, representative tissue samples were taken in the depth from the central part of the ulcer. In cases without ulcerations, tissue samples were taken from the tissue overlaying the tuber spina scapula (i.e., epidermis, dermis, and subcutis). In all cases, sampling of osseous tissue from the tuber spina scapula for histology was included.
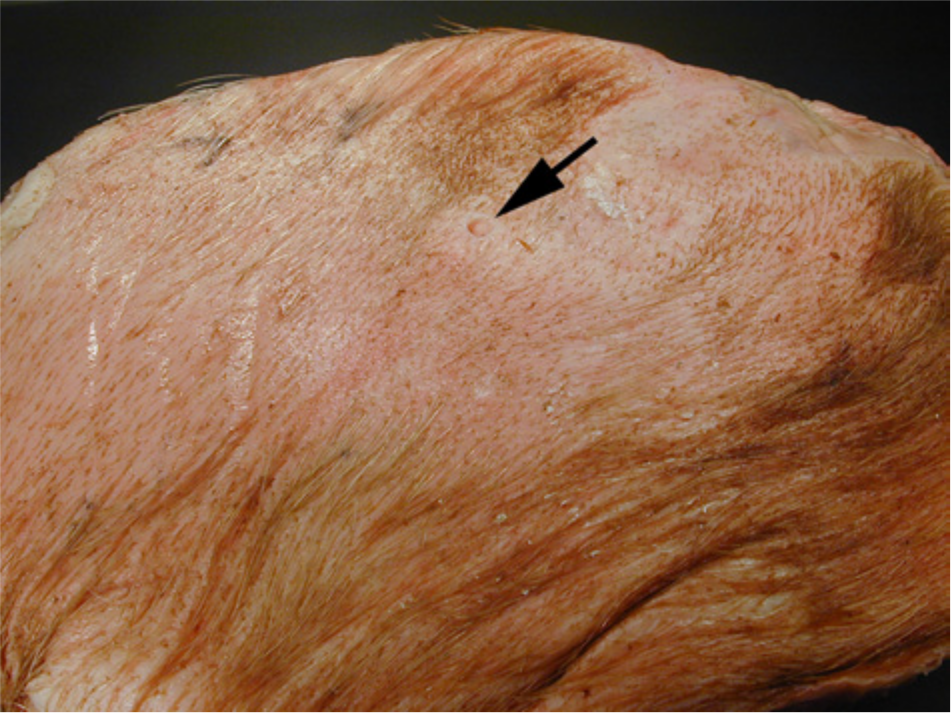
Sow. Shoulder area without ulceration (group A). A biopsy has been taken from the area (arrow).
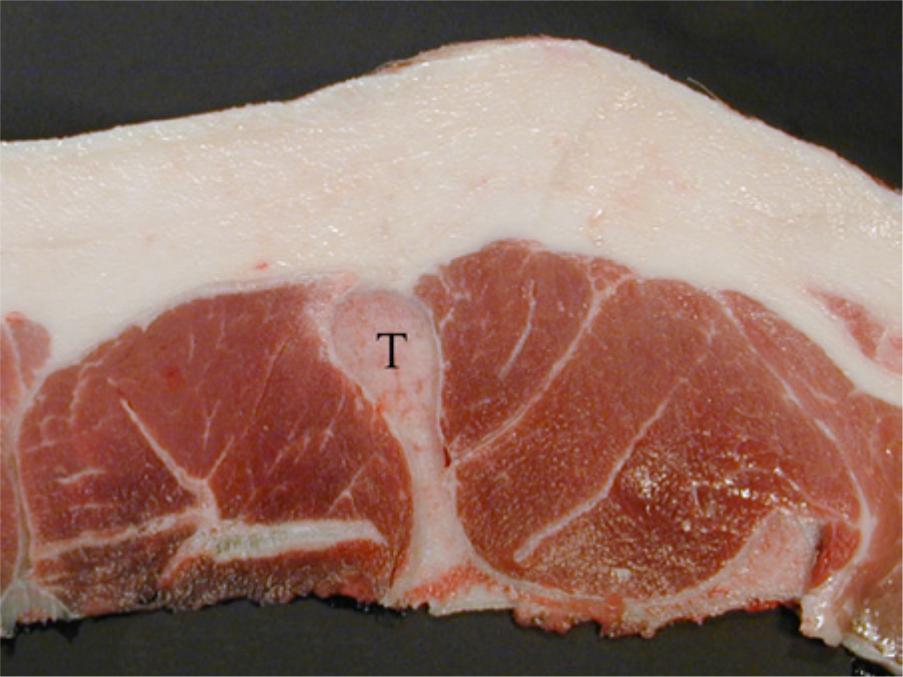
Sow. Cross-section of a shoulder area without ulceration (group A). Lesions are absent in all tissue layers. T = tuber spina scapula.
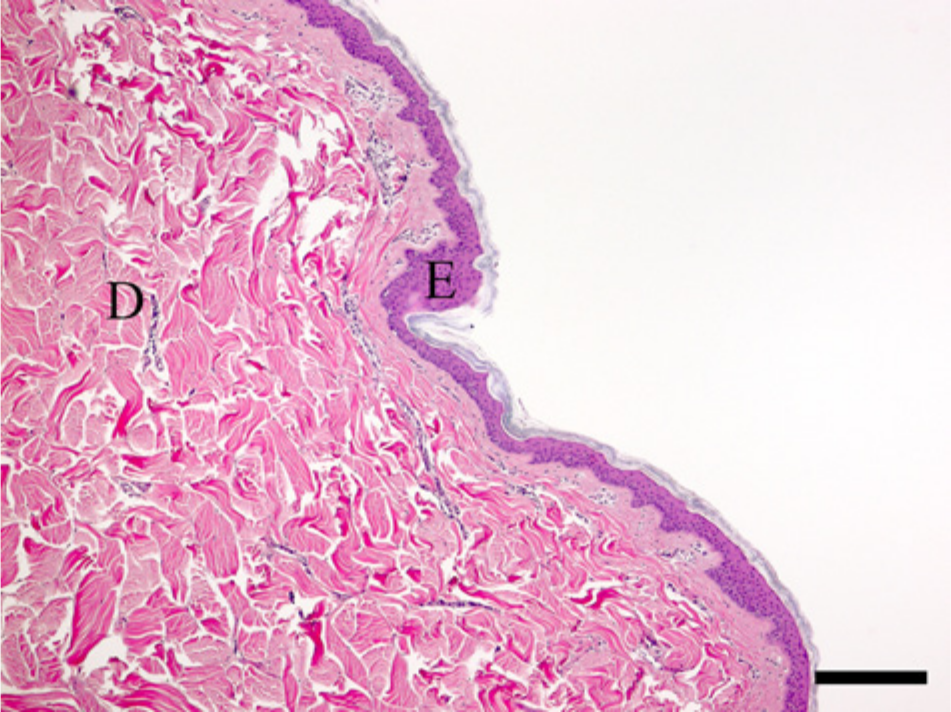
Sow. Shoulder area without ulceration (group A). Both the epidermal (E) and dermal (D) tissue are free of lesions. Hematoxylin and eosin. Bar = 175 µm.
Tissue samples and biopsies were fixed in 10% neutral buffered formalin for at least 3 days, then processed through graded concentrations of ethanol and xylene, and finally embedded in paraffin wax. Tissue sections were cut at 4–5 µm and stained with hematoxylin and eosin. Samples including the tuber spina scapula were decalcified for 3 weeks in 85% formic acid and processed as above.2,5,6,8,13,19,23,24
Based on macroscopic and histological observations on the cross-sectioned shoulders, lesions were grouped as follows: group A = no lesions, group B = pathoanatomical grades 1 or 2 (intervention not mandatory), and group C = pathoanatomical grades 3 or 4 (intervention mandatory) (Figs. 1–9). The result from cross-section evaluation was considered as the gold standard. In addition, the lesions were assigned to group A, B, or C based on the biopsy findings.
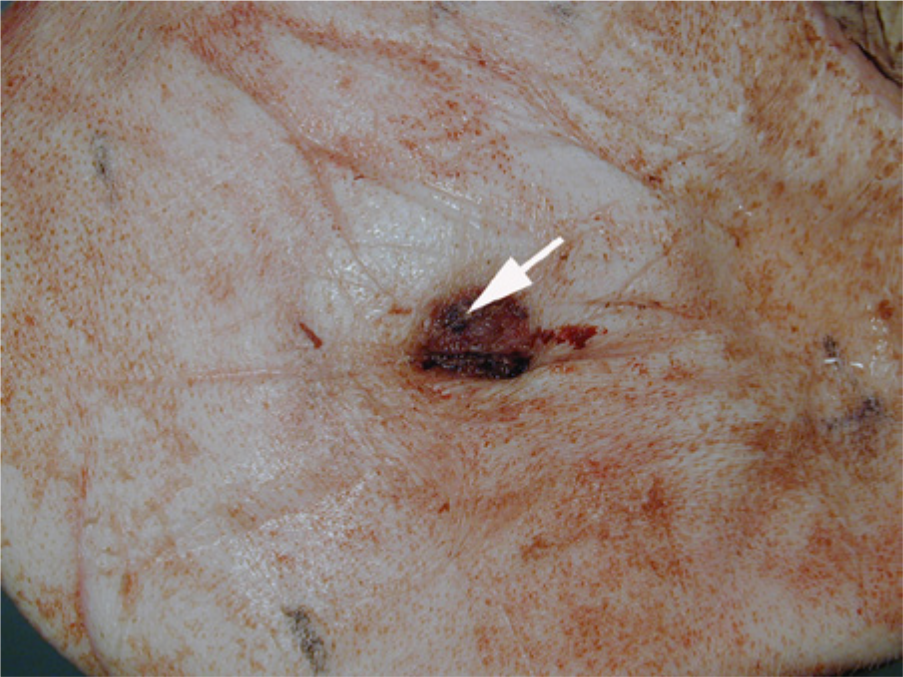
Sow. Shoulder ulcer (group B), intervention not required. A biopsy has been taken from the center of the ulcer (arrow).
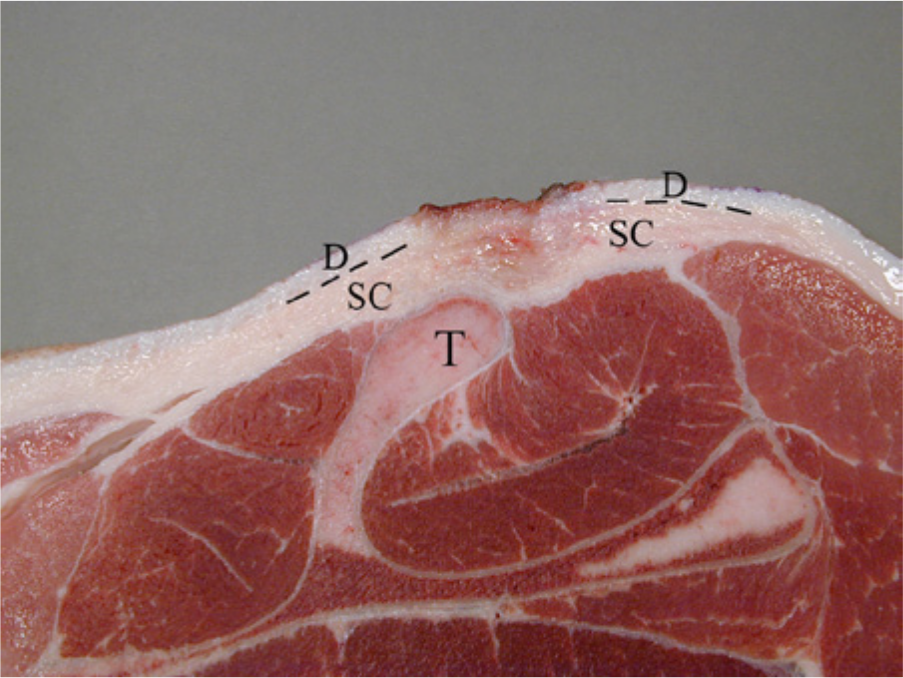
Sow. Shoulder ulcer (group B), intervention not required. In cross-section, the ulceration is seen to extend into the dermis (D). Edema is present beneath the ulceration in the subcutis (SC). The dotted line marks the transition between the dermis and the subcutis. T = tuber spina scapula.
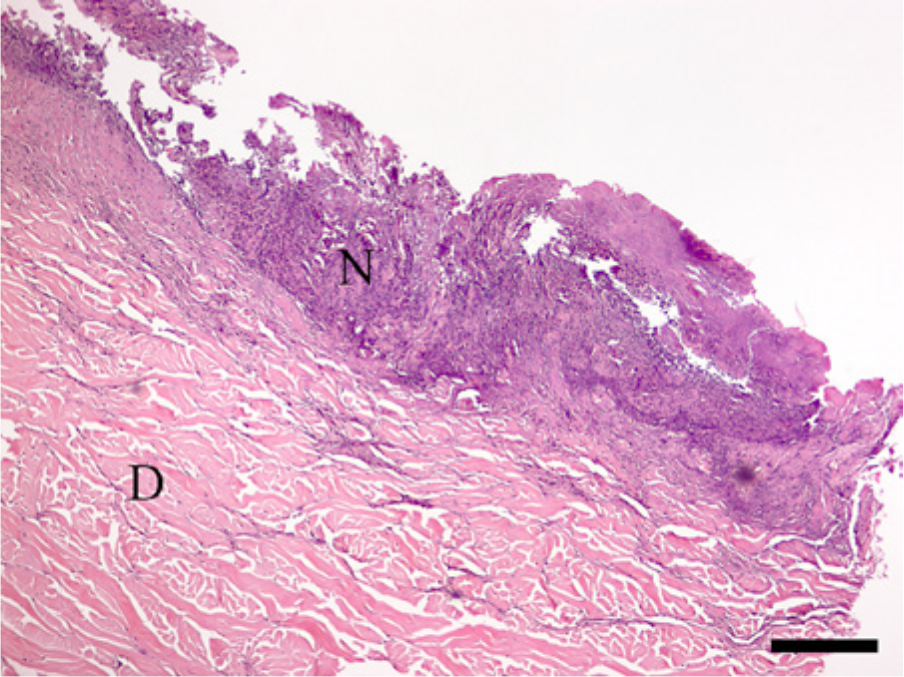
Sow. Shoulder ulcer (group B), intervention not required. The necrotizing ulceration (N) extends into the dermal tissue (D). Hematoxylin and eosin. Bar = 175 µm.

Sow. Shoulder ulcer (group C), intervention required. A biopsy has been taken from the center of the ulcer (arrow).
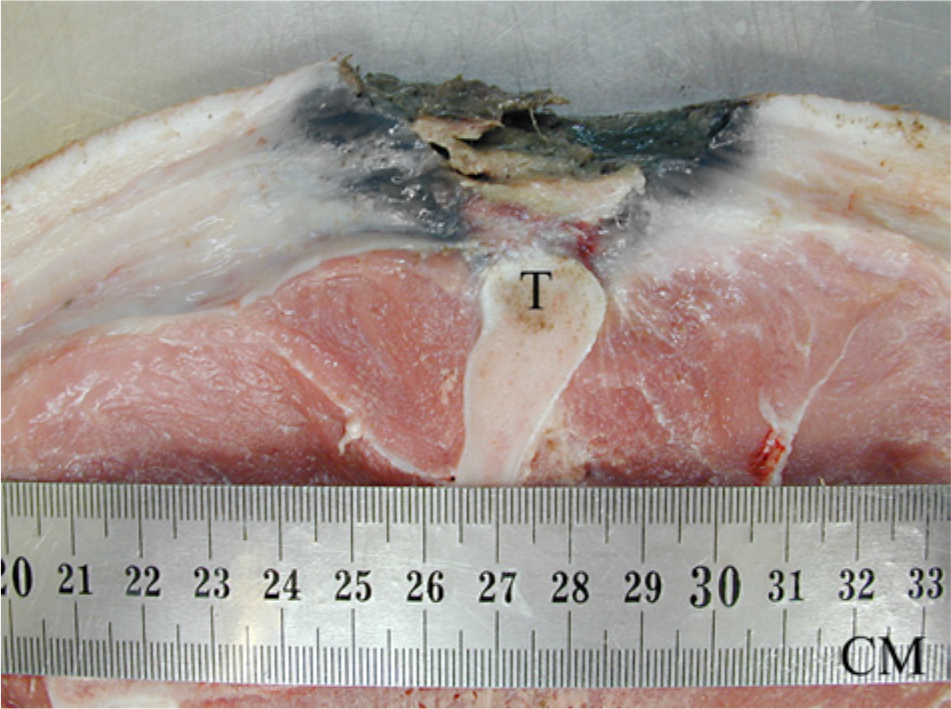
Sow. Shoulder ulcer (group C), intervention required. In cross-section, the ulceration extends into the subcutaneous tissue leaving the tuber spina scapula (T) unaffected.
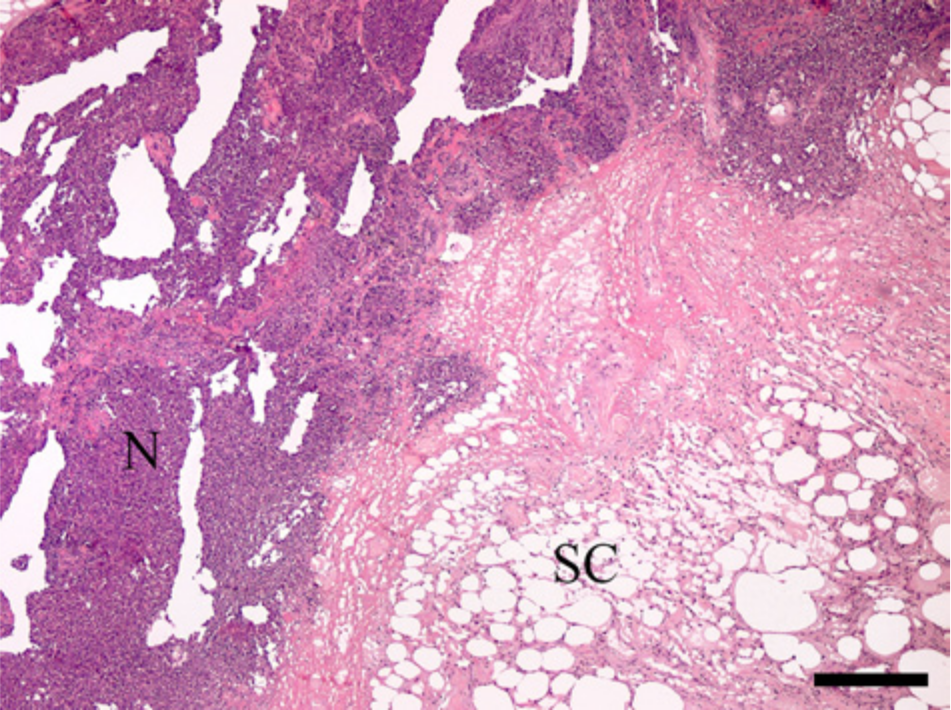
Sow. Shoulder ulcer (group C), intervention required. The necrotizing ulceration (N) extends into the subcutaneous tissue (SC). Hematoxylin and eosin. Bar = 250 µm.
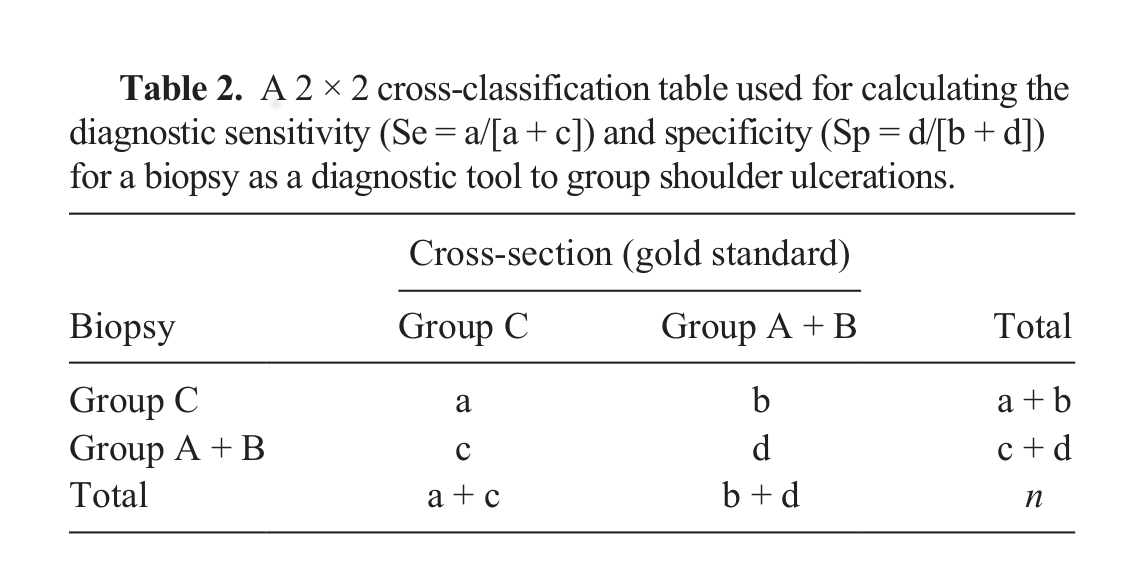
Shoulders in groups A and B were pooled. A 2 × 2 cross-classification table of the biopsy results versus the cross-section results (gold standard) was made (Table 2). The diagnostic sensitivity (Se) and diagnostic specificity (Sp) of the biopsy to group shoulder ulcers were calculated. Sensitivity was calculated as a/[a + c] (Table 2) and defined as the probability that an ulcer, which truly belonged in group C, also would be assigned to group C based on the biopsy. Specificity was calculated as d/[b + d] (Table 2) and defined as the probability that an ulcer truly belonging in group A or B would also be assigned to group A or B based on the biopsy. 20 A confidence interval was calculated for Se and Sp using commercial software. a Positive likelihood ratio (LR+) and negative likelihood ratio (LR–) were calculated using the following formulas: LR+ = Se/(1 − Sp), LR– = (1 − Se)/Sp. 20 In addition, Se, Sp, LR+, and LR– were calculated only based on shoulders in groups B and C, excluding cases without ulcerations (group A).
A 2 × 2 cross-classification table used for calculating the diagnostic sensitivity (Se = a/[a + c]) and specificity (Sp = d/[b + d]) for a biopsy as a diagnostic tool to group shoulder ulcerations.
The agreement between the 2 methods was evaluated by calculating Cohen kappa using commercial software. b The kappa value was calculated based on the data in Table 3, where the 2 tests, cross-section evaluation and punch biopsy, each had 3 possible outcomes: group A, B, or C. In addition, a confidence interval was calculated.
The number of shoulders grouped as A, B, or C based on cross-section evaluation and biopsy findings.*
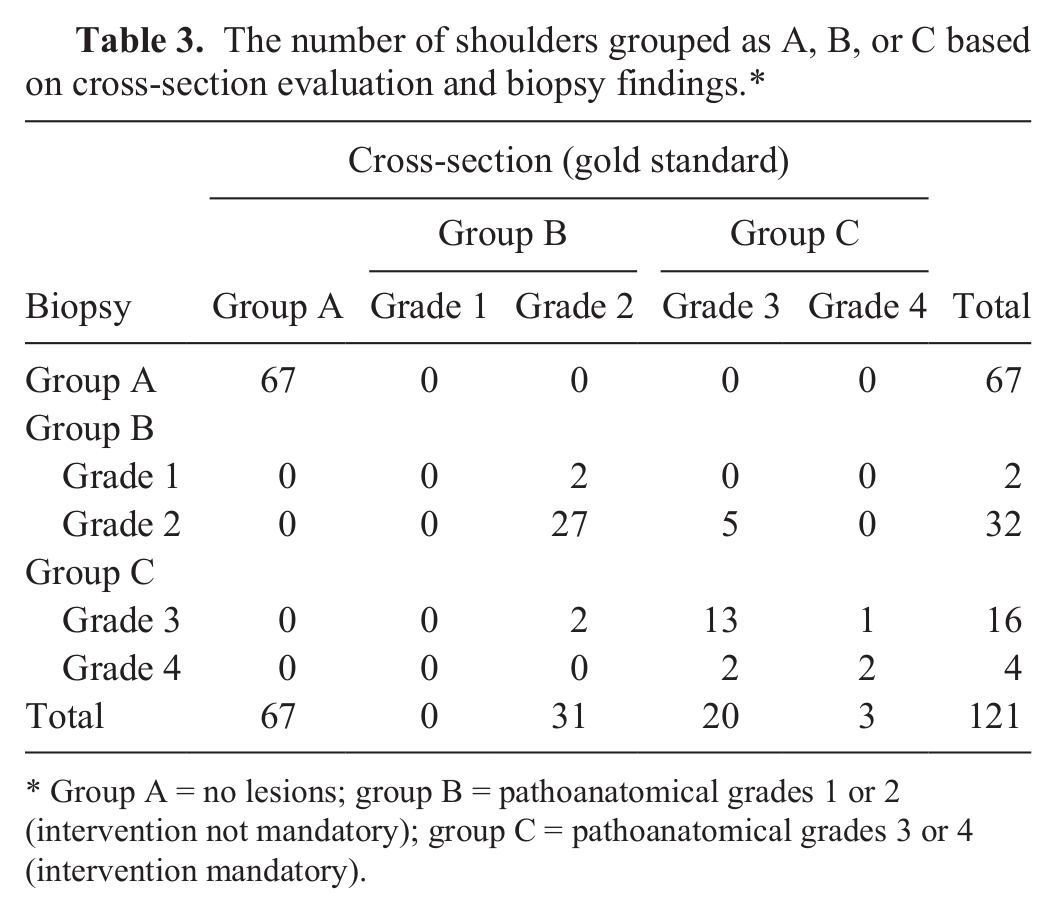
Group A = no lesions; group B = pathoanatomical grades 1 or 2 (intervention not mandatory); group C = pathoanatomical grades 3 or 4 (intervention mandatory).
In total, 159 shoulders were sampled. However, 8 shoulders were excluded due to the lack of biopsy sampling, and 151 biopsies were examined. Of these, 25 biopsies were inconclusive due to incomplete sampling (i.e., not all layers of skin were present in the samples). The excluded biopsies consisted of granulation tissue only, making the grade (depth) of the ulcer impossible to evaluate. In addition, 5 shoulders were excluded due to the lack of a cross-section evaluation. In total, 121 shoulders were included in the study. The grouping of the shoulders is shown in Table 3. Sensitivity, Sp, LR+, and LR– are presented in Table 4. The agreement between the cross-section evaluation and the punch biopsy was found to be 0.90 (95% confidence interval: 0.83–0.97; P < 0.0001) by calculating the Cohen kappa value. The Cohen kappa coefficient (i.e., the agreement between cross-section evaluation and a punch biopsy) was 0.90, which can be interpreted as an almost perfect agreement. 17
The sensitivity, specificity, and positive and negative likelihood ratios for a biopsy as a diagnostic test to grade shoulder ulcerations.*
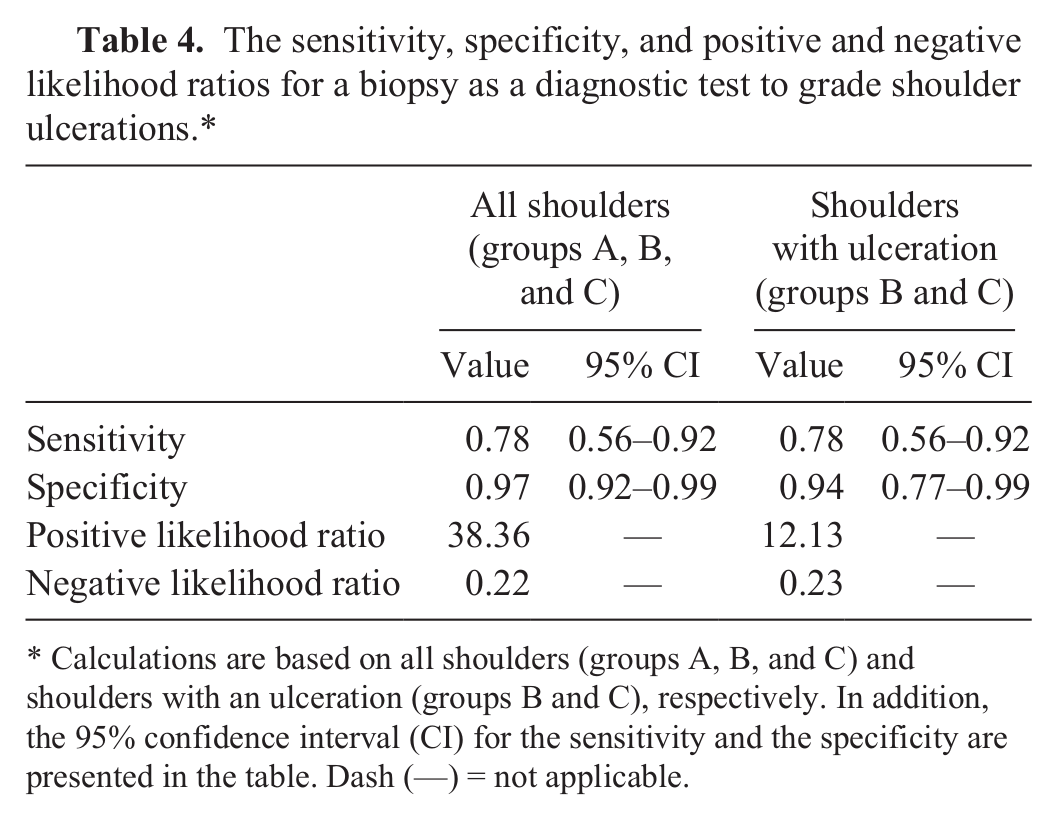
Calculations are based on all shoulders (groups A, B, and C) and shoulders with an ulceration (groups B and C), respectively. In addition, the 95% confidence interval (CI) for the sensitivity and the specificity are presented in the table. Dash (—) = not applicable.
Table 1 indicates the difficulties encountered in determining whether a shoulder ulceration is present or not. From the table, it is seen that 6 out of 67 cases without ulcerations, as determined by cross-sectioning (gold standard) the shoulders, were included due to an assumption of an ulceration being <5 cm in diameter. Table 1 also shows that out of 62 cases chosen as being free of ulcerations, a grade 2 ulceration was diagnosed in a single case at cross-section (gold standard). Therefore, in the present study, the biopsy results were compared to the true grade (i.e., the grading on cross-sections). 11
When pooling groups A and B, the Se of biopsies as a diagnostic tool was 0.78 with a rather broad 95% confidence interval. According to the definition of the Se, 78% of sows with a group C ulcer (grade 3 or 4) will be correctly diagnosed as a group C ulcer based on the biopsy findings. The Sp of the biopsies was 0.98 with a narrow 95% confidence interval. This means that 98% of sows with a group A or B ulcer (grade 0, 1, or 2) will actually be diagnosed as a group A or B ulcer. The sensitivity and specificity indicate that a biopsy is very good at diagnosing ulcers in group A or B (grade 0, 1, or 2), but that 22% of ulcers in group C (grade 3 or 4) will not be diagnosed correctly. In a clinical setting, only sows with ulcerations could pose a management dilemma of whether intervention is needed. Biopsies will not be required in shoulders without ulcerations because the correlation with the gold standard was 100% (Table 3). Therefore, calculating the Se and Sp for a biopsy as a diagnostic test is based only on shoulders with ulcerations (groups B and C). By excluding shoulders without ulceration (group A), the Se is still 0.78, while the Sp is 0.94, and has a broader 95% confidence interval compared to pooling groups A and B. Even though the Sp is lower compared with when group A is included in the data, it still indicates that a biopsy is acceptable for diagnosing ulcers in group B.
The likelihood ratio provides an indication of the value of a positive or negative result irrespective of the prevalence. 21 The LR+ was 38, which means that a biopsy indicative of group C (grade 3 or 4) is very likely to be correct. The LR– was 0.22. A low LR– indicates that an ulcer in group C (grade 3 or 4) is not very likely when the biopsy result indicates a group A or B (grade 0, 1, or 2) ulcer. In general, a LR+ of more than 2 is considered acceptable, while the LR– should be close to zero. 10 On this basis, the LR+ of the current study is very advantageous, while a lower LR– would have been preferred. Excluding group A from the data, the LR+ is 12.13, which still is acceptable. The LR– of 0.23 is only slightly worse compared to the LR– calculated when group A was not excluded from the data.
Obtaining antemortem biopsies from shoulder ulcerations in sows must be done following sedation or general anesthesia of the animal and application of local anesthesia. Before sampling a biopsy from an ulcer, the area must be washed and disinfected. Following sampling of the biopsy, the sampling area must be treated topically with antibiotics. In conclusion, a single punch biopsy taken through all layers of the skin and from the center of an ulcer is useful for determining the grade of a shoulder ulceration, guiding veterinarians to identify ulcers where an intervention is mandatory.
Footnotes
Acknowledgements
The authors wish to thank Anton S. Jensen, Orla Nielsen, Hanne Nissen, Jens Martin Strager, Søren Justesen, and Erik Jørgensen for invaluable technical assistance. Páll S. Leifsson (associated professor, DVM, PhD) and Ole L. Nielsen (associated professor, DVM, PhD), Department of Veterinary Disease Biology, University of Copenhagen, and Peter H. Kvist (senior scientist, DVM, PhD), Novo Nordisk A/S are acknowledged for help with scrutinizing the shoulder specimens for pathological manifestations.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by the Danish Pig Levy Fund, Danish Veterinary and Food Administration, EU and the Rural Development Programme under The Danish Ministry of Food, Agriculture and Fisheries, Pig Research Centre.
a.
Graph Pad Prism 6.0 for Windows, GraphPad Software Inc., La Jolla, CA.
b.
SAS 9.3 for Windows, SAS Institute A/S, Copenhagen K, Denmark.