
Abstract
Clinical information supplied to diagnostic laboratories through biopsy submission forms is crucial to accurate, timely diagnosis and to clinicopathologic correlation between microscopic findings and the clinical condition of the patient. The current study attempts to quantify the prevalence of deficient and inadequate submissions in veterinary biopsy service and to determine whether form characteristics, such as the open or closed nature of the form and the presence of specific prompts, influence reporting of essential case information. The hypotheses of this study are, first, that deficient and inadequate biopsy submissions do occur in veterinary medicine and, second, that open-type biopsy submission forms elicit quantitatively and qualitatively more complete case information overall, and in specific content areas, compared to closed-type biopsy submission forms. Three percent of submissions reviewed were information deficient, devoid of information beyond patient signalment, and more than 88% of forms supplied inadequate clinical information in at least 1 key content area. Both form type and specific prompts significantly influenced reporting of important clinical information. This study demonstrates the need and lays the foundation for informational completeness research in veterinary medicine.
Introduction
Thorough and accurate clinical case information presented to a pathologist through the biopsy submission form is vital for correct and timely diagnosis in biopsy service both in human and veterinary medicine.2,7,12,14,19,23 Information presented on a laboratory submission form serves to “frame the case” for pathologists, alerting them to the major concerns of the clinician for the case at hand and aiding recall of similar disease patterns from previously encountered cases. 6 A consensus statement recently released by a group of veterinary pathologists and oncologists to provide guidelines for biopsy submission went so far as to call the biopsy submission form “mandatory since it is the essential communication piece between the clinician, laboratory personnel, and pathologist.” 12 In effect, the respondent completing a submission form “serves as the eyes for the pathologist,” 8 as the pathologist is usually remote to the patient, and communication between clinician and pathologist is predominately limited solely to written reports.10,11
There is ample evidence that both clinicians and pathologists are aware of the necessity of presenting clinical information with specimens through laboratory submission forms.2,7,9,16,18-20,23,25 By one estimate in human biopsy requisition, however, “deficiencies related to missing or incorrect information account for approximately 80% of all deficiencies” 17 encountered in biopsy specimen acquisition. Furthermore, missing and inaccurate clinical information in biopsy submission has been shown to contribute to significant time delays, increased costs related to additional staining procedures or sectioning to reach a diagnosis, misdiagnosis leading to poor patient outcomes, and legal action related to the aforementioned issues.3,5,16,17,19,22,25 For instance, in one human medical study, 16 32% of cases with recognized inadequacies in requisition form information at the time of accession resulted in time delays, and half of these cases had reporting delays of greater than 1 day. It has also been estimated that roughly 1 out of 5 diagnostic errors recognized in legal malpractice cases related to human biopsy resulted from failure of the pathologist to rectify missing or inadequate information presented during biopsy submission. 16 Numerous potential causes have been suggested for submission of inadequate clinical information, such as clinician time constraints and lack of clinician awareness about the importance of information at accession, as well as certain characteristics of the biopsy form itself.19,20,22,23 In human dermatopathology, for example, researchers have theorized that the “open-ended nature” of the submission form may, in fact, hinder the clinician’s ability to report precise clinical information needed by the pathologist. 23 Regardless of the cause, any absence or ambiguity in clinical information presented on the biopsy submission form has the potential to result in serious cognitive errors by the pathologist with the capacity to create detrimental case outcomes for the client and patient. 17 Thus, it becomes critical for both human and veterinary medical professions to seek to minimize inadequate biopsy requisitions through informational completeness research and through regulatory oversight of biopsy submission form informational content.
In the United States, human biopsy requisition form content has been regulated since the passage of the Clinical Laboratory Improvement Amendments in 1988. 10 The resultant standardization of laboratory requisition forms to include prompts for basic clinical information—patient demographics, clinical case information, and working clinical diagnosis—simultaneously created a basis for research into informational completeness, or the amount and quality of clinical information present, in the requisition forms. This line of research has since led to the development of 2 national databases called Q-Probe and Q-Tracks to compile test requisition information for large-scale quality control studies involving upwards of 1 million or more forms16,17,25-27 and to the endorsement of a model biopsy requisition form by the College of American Pathologists. 25 Furthermore, through informational completeness research, it has been possible to quantify rates of inadequate and deficient submissions to human diagnostic laboratories. Submission rates of inadequate and deficient requisition forms across human laboratory tests range widely, from 0% to 67% of cases submitted,4,16-19 depending upon the purpose for the submission (radiology, biopsy, Pap test, etc.), the respondent (specialist vs. generalist), and the mode of requisition form submission (electronic vs. paper) being studied. However, the range for routine general human biopsy service is narrower; between 2.4% 16 and 6% 17 of requisition forms in routine human biopsy service have been found to be information deficient, that is, devoid of clinical information beyond patient demographics, the equivalent of patient signalment in veterinary medicine. Therefore, in a relatively short period of time, regulation and research of informational completeness in laboratory requisitions have already been integrated into human medical practice and laboratory quality control mechanisms and deficiencies in clinical information received with human biopsy requisitions have been documented and quantified.
Despite over 2 decades of regulation and research regarding informational completeness of laboratory requisition forms in human medicine, there has been no corresponding regulation or research for veterinary laboratory requisitions, including biopsy submissions. Therefore, the prevalence and causes of incomplete and inadequate clinical information in veterinary biopsy accession are largely unknown, though there have been anecdotal remarks that inadequate information is encountered in veterinary biopsy submission as in human medicine. 15 At present, large-scale research into informational completeness in biopsy submissions would not even be possible in veterinary medicine because there are no centralized national databases for veterinary laboratory submissions unlike in human medicine and no standards exist for submission form content in current veterinary laboratory regulatory documents issued by the American Association of Veterinary Laboratory Diagnosticians (AAVLD: 2009, Requirements for an accredited veterinary medical diagnostic laboratory. AC-201, Version 4.3:1–23. Available at: http://www.aavld.org/assets/documents/Requirements%20v5%200%2009-16-10.pdf. Accessed on July 23, 2012) and the Office International des Epizooties (World Organization for Animal Health). 24 As such, the authors have observed that biopsy submission forms vary considerably in content and layout between, and even within, veterinary diagnostic laboratories at present (data not shown). Despite this variability in form structure, the intended purpose of all biopsy forms is to solicit standard information regarding the signalment and clinical condition of the patient and the gross appearance and physical location of the specimen in each case. Additionally, though individual laboratory forms vary, in the authors’ experience, 2 general types of biopsy submission forms have emerged for use in veterinary biopsy:
1. Open-type biopsy submission forms. Biopsy-centric forms consisting predominately of open-ended prompts (i.e., “Clinical history”) with abundant open space for independent response. Respondents provide most of the information in their own words (Fig. 1).
2. Closed-type biopsy submission forms. Either general diagnostic or biopsy-centric forms consisting predominately of closed-ended prompts (i.e., checklists compiled by the laboratory) with little open space for independent response. The majority of responses must be selected from within a defined set of options preselected by the laboratory (Fig. 2).
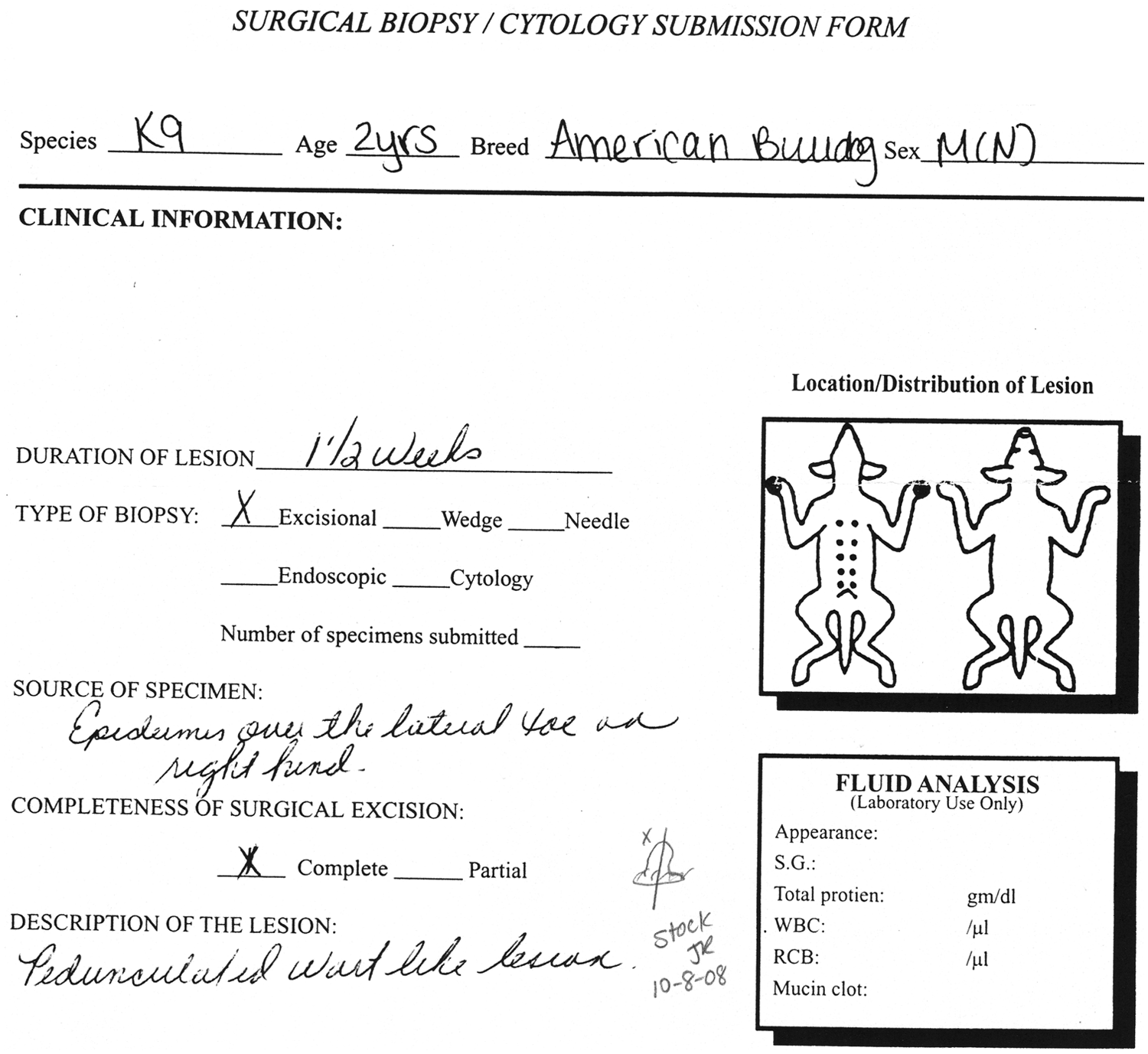
Typical open-type biopsy submission form. Open-type forms are composed mainly of open-ended prompts (i.e., “Clinical information”) with abundant space for independent response to prompts. To protect the privacy of those involved in form submission, all identifiable laboratory, hospital, client, and patient information has been removed from the image.
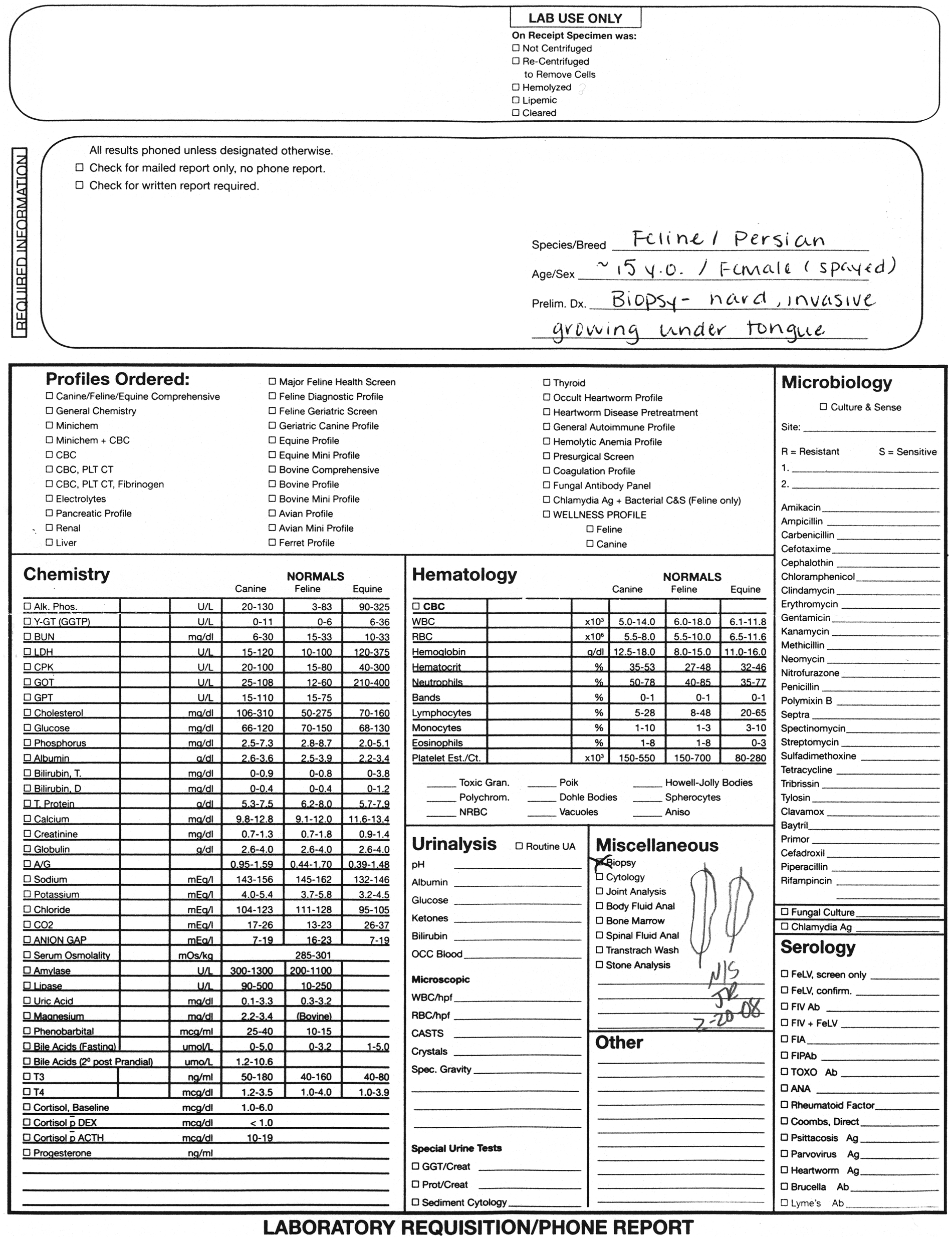
Typical closed-type biopsy submission form. Closed-type forms are composed mainly of closed-ended prompts (i.e., checklists) with little space for independent response. The majority of potential responses are supplied by the diagnostic laboratory rather than by the respondent. To protect the privacy of those involved in form submission, all identifiable laboratory, hospital, client, and patient information has been removed from the image.
Thus, both the informational content and the type of biopsy submission forms can serve as a basis for comparison between disparate forms for informational completeness studies in veterinary medicine until that day when form variability can be controlled through regulatory oversight and the development of large-scale requisition databases. Though informational content has yet to be studied or regulated in veterinary laboratory requisitions, both a need and a basis (form content and type) for this line of research already exist in veterinary medicine.
Veterinary clinicians, pathologists, and diagnostic laboratories can no longer ignore the potential for informational deficits in biopsy submission, nor can the veterinary professional community afford to wait until all form variables can be controlled to engage in informational completeness research. Fortunately, in the authors’ experience, few submissions encountered by veterinary pathologists in the course of routine biopsy practice are truly information deficient, as defined by the aforementioned human medical standards. On the other hand, it has also been the authors’ experience that inadequate submissions occur relatively commonly. Key case information regarding the signalment of the patient, clinical history, gross appearance of the specimen submitted, and/or physical location of the specimen (tissue or organ and anatomic site) is frequently omitted or ambiguous. Furthermore, in direct contradiction to the conjectures put forward for human dermatopathology requisitions, 23 the authors have circumstantially observed that open-type biopsy submission forms utilized in veterinary biopsy tend to provide more thorough clinical information than closed-type forms and are, thus, more useful for the purposes of diagnosis and clinical correlation in the accompanying specimen.
Though “much of the information on a requisition slip is not necessary for accurate reporting of results, there are many instances in which deficient or inaccurate information could lead to an erroneous diagnosis,” 17 and an attempt should be made by the pathologist to rectify informational deficits prior to diagnosis and subsequent issuance of the pathology report in cases where deficiencies occur. Alas, for veterinary diagnostic laboratories unlike in human laboratories, there is usually no physical connection between the pathology laboratory and submitting clinic, no direct access for the pathologist to medical records, and no recourse for returning specimens received with inadequate information to rectify informational deficits when they arise. 25 Consequently, problems encountered with inadequate submission of information in veterinary laboratory requisitions could potentially have more serious ramifications than in human medicine, where procedural mechanisms are in place to correct informational deficits prior to specimen diagnosis. The time has come to formally document and quantify the problem of deficient information and to determine potential causes for informational deficits in laboratory requisitions, including biopsy, through informational completeness research in veterinary medicine.
Thus, the purpose of the current study is to undertake a systematic study of informational completeness in veterinary laboratory submissions in the United States, specifically concerning information obtained in veterinary biopsy submission forms. The hypotheses of this study are, first, that deficient and inadequate biopsy submissions do occur in veterinary medicine and, second, that open-type biopsy submission forms elicit quantitatively and qualitatively more complete case information than closed-type biopsy submission forms both overall and within specific content areas. Though the scope of the study is limited to analysis of veterinary biopsy submission forms, it is the authors’ fervent hope that this research will open the way for additional informational completeness research both for biopsy and for other laboratory test submission forms in veterinary medicine.
Materials and methods
Submission form collection, classification, and selection
A single veterinary anatomic pathologist (1 of the authors) collected all submission forms received during the course of routine general biopsy service for 3 diagnostic laboratories (1 national referral laboratory and 2 private regional Midwestern laboratories) between 2007 and 2009. The 6,622 forms collected during this period were sorted by laboratory and form layout. Each unique form layout was then classified as either open-type or closed-type depending on whether the majority (≥50%) or minority (<50%) of the useable form area (i.e., area devoted to collecting clinical information about the patient and specimen) was devoted to open-ended prompts with space for independent clinical response, respectively. Each laboratory had at least 1 open- and 1 closed-type biopsy form in use throughout the time period, allowing for comparison of form types within laboratories. Permission was obtained from all laboratories to analyze the informational content of the forms on the stipulation that no identifying laboratory, client, or patient information would be released beyond the researchers involved in the study. Through a preliminary study utilizing the scoring system outlined below, it was determined that a sample size of 50 or more forms per group would allow greater than 80% power to detect a difference of 1.7 in mean completeness scores with a common standard deviation of 2.2 at α = 0.05. A larger final sample of 525 submission forms, or 75 forms from each group, was selected in the event of form exclusion from analysis based upon submission of a non-visualized specimen (i.e., mare endometrial biopsy or ultrasound-guided biopsy). Form selection was randomized through the use of random number sequence generation in each layout group.
Scoring
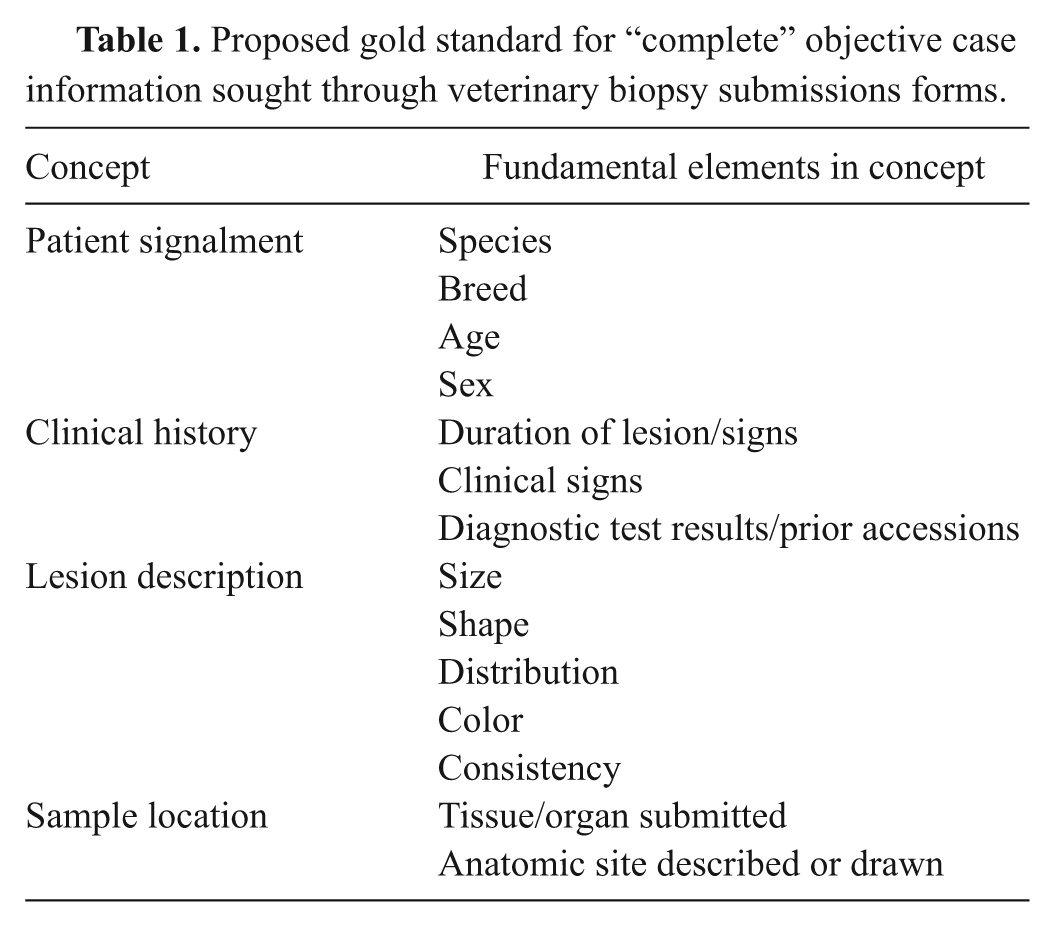
As no standards for informational completeness were available in the veterinary literature, the scoring system utilized in the current study was developed in consultation with veterinary pathology and surgical reference texts (Brannick EM: 2010, Assessing informational completeness in veterinary biopsy submission forms. Master’s thesis, publication number: osu1290628085. The Ohio State University, Columbus, OH) and through modifications to research standards available in human informational completeness literature.1,4,13,21 First, a gold standard of 14 essential elements of objective clinical information (Table 1) was constructed from review of veterinary literature (Brannick 2010), as no consensus opinion regarding submission information standards was available until after this research was completed. 12 Forms were retrospectively analyzed and scored by a single reviewer in an unblinded fashion for both the quantity and quality of objective case information received in fulfillment of elements of the gold standard. Information supplied by laboratory technicians during specimen accession was excluded from analysis.
Proposed gold standard for “complete” objective case information sought through veterinary biopsysubmissions forms.
Quantitative completeness score
For quantitative analysis, form responses were objectively reviewed for either the absence (scored as 0) or presence (scored as 1) of each element of the grading scheme and a quantitative completeness score was calculated for each form as the sum of all elements present on the form. In cases where multiple specimens were submitted using a single form, scoring was based upon the information provided for the first sample listed, as it has previously been determined in human biopsy that clinicians tend to submit equivalent information across samples in a multi-tissue submission, either reporting an element for all tissues submitted or for none. 23 To determine total length of response, a word count was tallied that included all words written or typed in response to prompts. Patient signalment were excluded in order to prevent bias against those forms using checkboxes to solicit signalment information. Information provided by the histotechnician was excluded from analysis.
For qualitative analysis, a subjective evaluation of the coherence of case information for each concept (signalment, clinical history, lesion description, and sample location) was performed using the following grading scales to minimize reviewer bias (modified from human informational completeness studies4,21).
Signalment, clinical history, and lesion description scores
0 = deficient: additional information needed (all elements missing); no basis upon which to form a coherent concept;
1 = inadequate: additional information needed (1 or more elements missing); information presented is ambiguous or insufficient to form a coherent concept;
2 = adequate: additional information needed (1 or more elements missing); information presented is sufficient to form a coherent concept;
3 = complete: no additional information needed (all elements present); information presented is clear and forms a complete concept.
Sample location score
A 3-point scale was utilized for sample location because the absence of information regarding either the tissue sampled or the anatomic location of the sample would render the response inadequate.
0 = deficient: no information provided; no basis upon which to form a concept of sample location;
1 = inadequate: information presented is ambiguous or insufficient to form a coherent concept of sample location;
2 = complete: information presented is sufficient to form a complete concept of sample location.
Qualitative completeness and overall completeness scores
A qualitative completeness score was calculated for each form as the summation of the 4 concept scores. For the purposes of statistical analysis, an overall completeness score was also calculated for each form as the sum of the quantitative and qualitative completeness scores for that form.
Statistical analysis
Descriptive statistics, such as overall reporting rates and reporting rates for each grading scheme element, were listed, and the two-tailed Fisher exact test was used to compare the rates between form types and between forms with and without specific prompts for an element. Two-way analysis of variance method using a generalized linear model was utilized to assess the effects of form layout and laboratory, and the interaction between the two, for all completeness and word count scores. In this analysis, a P value of 0.05 was considered to be significant. When significant interaction between form layout and laboratory was detected, analysis required further sliced testing. In sliced testing, the mean difference between open and closed forms was analyzed within each of the 3 laboratories rather than between all open and all closed forms. The resulting P values were corrected for multiple (3) comparisons using the Bonferroni procedure with family-wise type I error controlled at 0.05.
Results
A total of 510 of the 525 forms from the study sample were included in statistical analysis. Fifteen forms were excluded on the basis of submission of a non-visualized sample (i.e., blind-guided biopsy). Quantitative completeness scores followed a normal distribution, ranging from 1 (least complete) to 14 (most complete; Fig. 3). Complete clinical information, fulfilling all elements of the gold standard, was only present in 9 out of 510 forms, or less than 2% of cases. An additional 9% of forms (49 forms) lacked only 1 or 2 informational elements. Therefore, in the vast majority (>88%) of cases, important information was inadequate in at least 1 key content area. Moreover, approximately 1 in every 3 submissions (187/510 forms, 37%) could be considered information-poor, lacking at least half of the pertinent background information for the specimen (quantitative completeness score ≤ 7). Of these, 17 forms were entirely information deficient, providing no clinical information beyond patient signalment, which yielded an overall absolute deficiency rate of 3%. An additional 7% of forms (35/510 forms) contributed merely a single informational element beyond patient signalment, typically information regarding either sample location or clinical signs in the patient.
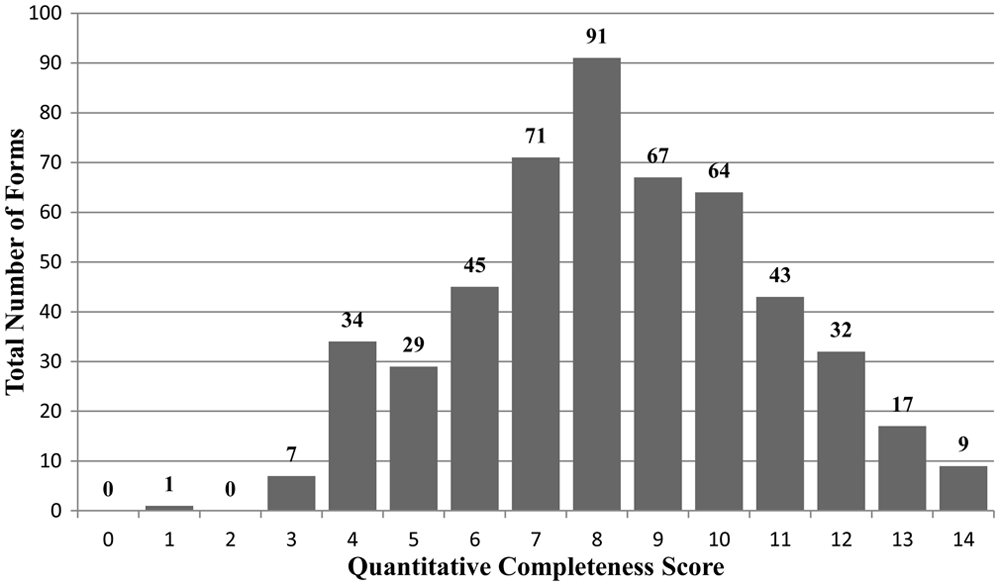
Distribution of submission form quantitative completeness scores (0 = no information given, 14 = most complete). Though a small number of forms provided all or most informational elements (scores of 13 or 14) in the gold standard for the accompanying specimen, the majority of submissions were information deficient in at least 1 key area. Approximately 1 in every 3 forms supplied half or less (scores ≤ 7) of the pertinent clinical information expected by the pathologist.
Regarding completeness score analysis, the maximum quantitative and qualitative completeness scores for both open and closed forms reached the maximum of the score scales, indicating that both open and closed forms had the potential for submission of thorough and high-quality case information. A significant interaction was detected between form type and laboratory for all score variables except clinical history and word count (see http://vdi.sagepub.com/supplemental). As such, a direct comparison could only be made between all open and all closed forms for these 2 variables. The difference in the mean clinical history scores between open and closed forms was significant (P < 0.0001) and positive (i.e., open forms having a higher mean score than closed forms indicating higher quality information from the open-type forms) at α = 0.05. Likewise, the difference between mean word count scores was significant (P < 0.0001) and positive between open and closed forms for word count, indicating that responses in open forms tended to be longer than in closed forms. Open-type forms had an average word count almost twice that of closed-type forms—20 words on average compared to 11 words for closed-type forms—though both form types had similar word count ranges (1–69 and 0–78 words for open- and closed-type forms, respectively).
Following sliced testing with correction for multiple comparisons in the remaining variables, the difference in the mean scores between open and closed forms remained significant (α = 0.017) within each of the 3 laboratories for overall completeness, qualitative completeness, quantitative completeness, and lesion description scores. As such, there is convincing evidence to conclude that a significant difference in these scores exists between open and closed forms regardless of the impact of different laboratories. In each of these comparisons, the difference in the mean scores was also positive, that is, the mean score for the open-type forms was greater than that for the closed-type forms, indicating that more and higher quality information was received through open-type forms. Patient signalment and lesion description did not completely fit this pattern. For patient signalment, a significant difference was only detected in open versus closed form mean scores for 2 of the 3 laboratories, but the direction of the difference was dichotomous-negative (i.e., closed forms having a higher mean score, and thus better quality of signalment information, than open forms) for the national referral laboratory, but positive for one of the regional diagnostic laboratories. A significant difference was only detected in the mean sample location scores between open and closed forms for 1 laboratory, with open forms having higher mean scores than closed forms in this laboratory. In the remaining laboratories, there was no detectable difference between mean sample location scores, and the average response equated to an adequate grade on the scale for both open- and closed-type forms.
In comparison of reporting rates, or the percentage of respondents that provided information to satisfy each element on a given form, open-type forms had significantly higher reporting rates than closed-type for all informational elements except for patient species, age, and sex. These 3 elements had consistently high reporting rates (>96% reporting across forms) and, interestingly, corresponded to the only 3 prompts universal to all form layouts included in the study. Subsequent comparison of reporting rates between forms with and without specific prompts for each element (Table 2), regardless of form type, demonstrated that reporting rates were significantly higher for forms with prompts for duration, size, distribution, and consistency. Conversely, reporting rates regarding prior testing or accessions were significantly higher for forms without prompts for this information. There was no significant difference in reporting for clinical signs or for organ or tissue sampled, as both were consistently reported regardless of form prompt (>73% reporting across forms). In the remaining elements, no comparison was possible because forms universally included the prompt (patient species, age, and sex) or lacked the prompt (lesion shape, color, and site).
Comparison of reporting rates for informational elements presented on biopsy submission forms with or without specific prompts for each element.
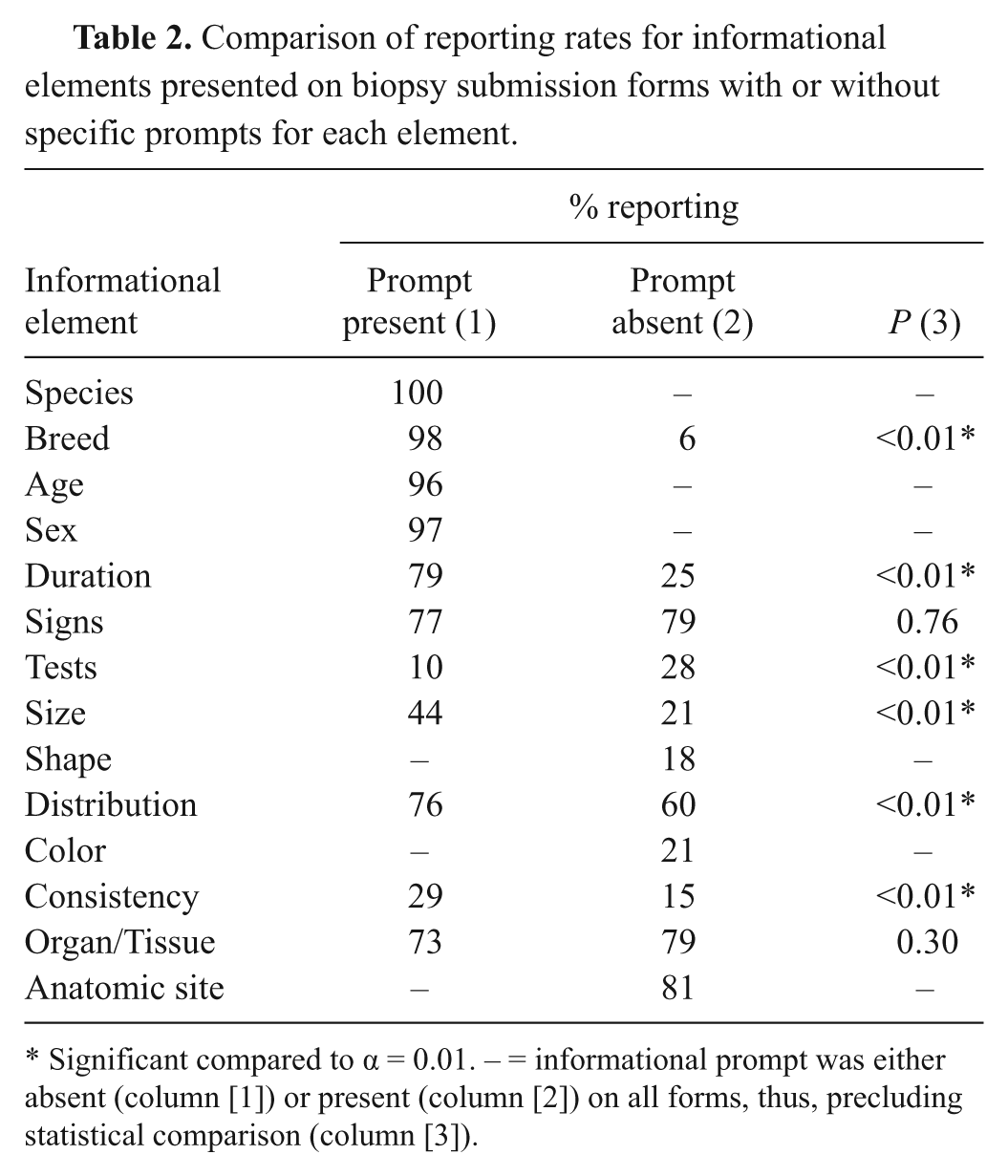
Significant compared to α = 0.01. – = informational prompt was either absent (column [1]) or present (column [2]) on all forms, thus, precluding statistical comparison (column [3]).
Discussion
The results of the current study on informational completeness in veterinary biopsy submission forms clearly demonstrate that deficient submissions do occur in veterinary medicine like in human medicine, as hypothesized. Fortunately, the deficiency rate for routine veterinary biopsy forms evaluated in the present study is low (3%) and roughly equivalent to reported deficiency rates for accession forms in human biopsy service (range: 2.4–6%).16,17 More disconcerting, however, are the rates of inadequate submissions in veterinary biopsy service. The majority of forms (>88%) encountered in the present study were missing more than 2 key informational elements, and in approximately 1 out of 3 submissions, less than half of the pertinent case information was presented. A sobering example of inadequacy identified through this study is that about 1 out of every 5 submissions lacks crucial information regarding either 1) the organ or tissue collected or 2) the specific anatomic location of the specimen, both of which can be critical to the pathologist’s understanding and interpretation of the biopsy specimen. Considering that any informational deficiency or inadequacy has the potential to cause serious cognitive errors by the pathologist, these findings are truly disturbing. With this new understanding of the prevalence of information deficits in veterinary biopsy service, it becomes necessary to determine possible causes for omission or inadequate relay of information in the biopsy submission form.
The causes for deficient and inadequate submissions in veterinary biopsy are likely numerous and complex, stemming from factors at both the veterinary clinic and the diagnostic laboratory level. This study demonstrates conclusively that characteristics of the submission form, such as form type and prompts, are among the factors under the control of the diagnostic laboratory that can affect both the amount and the quality of clinical information provided with biopsy specimens. First, the open or closed nature of the submission forms proves to be a major factor in informational completeness in biopsy submission. Through comparison of the maximum completeness scores assigned during form analysis, the current study has demonstrated that either open-type or closed-type biopsy forms have the potential to transmit thorough and meaningful case information when used appropriately. However, as hypothesized, open-type forms tend to elicit longer responses providing more, and better quality, case information on average than closed-type biopsy forms, based upon the comparison of mean scores. This was true both for overall information provided (total completeness, quantitative completeness, and qualitative completeness scores) and within specific content areas (clinical history and lesion description). Therefore, submission form type is one of the critical factors in soliciting biopsy case information that can be shaped and determined by the diagnostic laboratory.
On the other hand, the study hypothesis did not hold true for patient signalment and sample location in all laboratories, indicating that some information is affected by factors other than form type, which may be outside the influence of the diagnostic laboratory. For instance, closed-type forms had significantly higher mean scores for patient signalment than open-type forms in the national laboratory. This finding can be explained by failure of clinicians to respond to all signalment prompts provided on the open forms. Certainly the onus of responding to form prompts rests with the individual respondent and is beyond the influence of the diagnostic laboratory. In another example, there was no detectable difference in mean scores for sample location between open- and closed-type forms in 2 of the laboratories. On further inspection, it was determined that this was because the average specimen location response written on both open and closed forms conveyed adequate information to those laboratories. Thus, while the use of open-type forms tends to impel more and better quality information than closed-type forms, factors outside of laboratory control, such as respondent reluctance or willingness to provide information, can negate this effect.
Beyond the completeness of information received, it is also now evident that form type and prompts are among the laboratory-controlled factors that influence reporting rates for specific elements of case information. In the present study, open forms demonstrated higher reporting than closed forms for all information assessed, except for prior diagnostic testing (inverse relationship) and for patient species, age, and sex (no significant difference), which correspond to the only 3 prompts universal to all forms in the study. In addition to the high reporting rates for information requested through universal signalment prompts, study results also demonstrate unequivocally that the presence or absence of explicit prompts on the biopsy submission form can significantly impact whether or not important clinical information is reported to the pathologist. The most striking example of the prompt phenomenon in the present study regards reporting of patient breed, for which 98% of respondents provided the information when prompted but only 6% reported breed information when not prompted by the laboratory. Form prompts also significantly influenced reporting of information about the duration of disease or lesion and the lesion size, distribution, and consistency. Counterintuitively, forms without a prompt for prior diagnostic testing or accession actually had significantly higher reporting rates than forms with prompts for such information (28% reporting for forms without prompts vs. 10% with prompts). This again indicates that the ultimate decision to provide case information lies with the individual respondent who can elect not to respond to prompts defined by the diagnostic laboratory.
Furthermore, merely responding to a prompt does not guarantee adequate clinical information for microscopic diagnosis and clinicopathologic correlation by the pathologist if the response provided is ambiguous or erroneous. As such, reporting of clinical information may also be affected by the knowledge level and experience of the respondent; the authors suspect that clinicians commonly task their technicians or assistants with completing the biopsy submission form even though staff members may not understand the importance of complete information or be trained to respond to all of the prompts accurately. Therefore, though form type and specific form prompts provided by the laboratory can influence reporting of important case information in veterinary biopsy, the effects of clinical factors, such as respondent attitude toward necessity of information in biopsy submission and interpretation of form prompts, have yet to be elucidated.
The current research is intended solely as a sentinel study to demonstrate the need for a new line of research into informational completeness in veterinary diagnostics and to provide a foundation for that research. Large-scale studies involving prospective analyses or with a wider sample base would require standardization of submission forms among veterinary laboratories and the creation of national databases for laboratory submission information, which are not available at present in veterinary medicine. Though both endeavors would be ideal for the purposes of future informational completeness research, the authors are sensible about the impracticality of such an undertaking in the foreseeable future given the disparate nature of veterinary diagnostic laboratories and the clinics they serve. Factors beyond submission form type and prompts (i.e., clinician vs. technician or specialist vs. generalist completion of forms, respondent attitudes toward the necessity of providing information in biopsy submission, etc.) that may also influence informational completeness can only be speculated upon at present. Substantial future research efforts will be required to determine the influence of these and other factors on informational reporting in veterinary biopsy and in veterinary diagnostic submissions beyond biopsy. Despite present limitations to informational completeness research in veterinary medicine, the potential for future research along these lines is vast and, as yet, uncharted.In summary, deficient and inadequate biopsy submissions do occur in veterinary medicine as in human medicine. Biopsy submission form characteristics, including the type of form and the presence of specific prompts, are among the factors that both significantly influence reporting of clinical case information during biopsy accession and are under the purview of the diagnostic laboratory. As such, it becomes imperative for veterinary diagnostic laboratories to regularly evaluate and redesign biopsy submission forms as needed to better solicit case information when deficiencies are encountered during routine biopsy service. The results of the present study further indicate that providing biopsy-specific forms with abundant space for response introduced by specific, but open-ended, prompts for case information should improve the amount and quality of clinical information provided with biopsy specimens. It is important for diagnostic laboratories to understand that a biopsy is a subjective evaluation of disease patterns requiring considerable judgment on the part of the pathologist that may be assisted by complete case information. A biopsy is not an objectively measured continuous variable performed by a machine like a complete blood cell count that a respondent can simply check off on a list of such tests. The total patient evaluation principle, in which a diagnosis is not rendered until all of the relevant information available to the veterinarian has been considered, applies to diagnostic pathology just as it does to the practice of clinical medicine. In the current culture of veterinary medicine, total patient evaluation depends upon the clinician to provide all important information for the pathologist to weigh before final diagnosis. A submission form that guides the clinician as to what information is desired potentiates the likelihood of a total patient evaluation by the pathologist. Additionally, form revision should be executed in consultation with the pathologist or pathologists who are the end-users of the information received on the biopsy submission form and, as such, have first-hand knowledge of common informational deficits. Now that the problem, prevalence, and certain causes of inadequate submissions have been systematically documented through this research, it is possible to take corrective action to improve future biopsy submissions.
The veterinary medical community can no longer ignore the problem of missing and inadequate information in laboratory accessions, including biopsy submissions. Though veterinary medicine lags 2 decades behind human medicine in regulating and studying informational completeness in laboratory requisition forms, human medical researchers have provided a framework for launching similar efforts in veterinary medicine, as outlined in the present study. Evidential proof that deficient and inadequate submissions do occur in veterinary biopsy practice and that biopsy submission form characteristics can influence reporting of important clinical information during specimen accession is provided in the current study. It now becomes the responsibility of all veterinary clinicians, pathologists, and diagnostic laboratories to work together to rectify problems of inadequate information in laboratory submissions and to research other causes of informational deficits for the benefit of the veterinary medical field and the clients and patients it serves.
Footnotes
Acknowledgements
The authors would like to sincerely thank the diagnostic laboratories that contributed case material for use in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through release time resources available to Dr. Stromberg through the Department of Veterinary Biosciences at The Ohio State University, Columbus, Ohio.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.