
Abstract
A syndrome of progressive right-sided heart failure occurred among yearling Holsteins at a heifer-raising facility and 2 dairies on the Colorado Front Range between 2007 and 2011. Most cases were seen at the heifer-raising facility, where the disease ranked second only to pneumonia as a major cause of death in animals aged <1.5 years. The disease resulted in the death or premature sale of 55 animals over the 5-year period. Affected heifers were 4–15 months old when they developed dyspnea, tachycardia, distention and pulsation of jugular veins, lethargy, and weight loss. Clinical progression in most was rapid (2 days to 2 weeks). Ten cattle with typical clinical signs were examined postmortem between 2008 and 2010. Seven developed clinical signs after transportation 57–238 days earlier from Wisconsin (elevation: < 275 m); the remaining 3 animals were born and raised at an altitude of 1,600 m. At necropsy, the 10 cattle had marked hypertrophy of right ventricular myocardium, dilated right atria, right ventricles, and pulmonary trunks, as well as hepatomegaly, ascites, and serous atrophy of fat. The principal histological change in lungs was hypertrophied tunicae adventitia and media of muscular arteries. Hepatic changes were typical of chronic passive congestion. Ultrastructural changes in heart were consistent with uncomplicated hypertrophy of cardiocytes with no evidence of primary cardiomyopathy. The syndrome most likely represents brisket disease due to pulmonary hypertension at the modest elevation of 1,600 m.
Keywords
Introduction
Cor pulmonale is failure of the right side of the heart that is induced by chronically elevated blood pressure in the pulmonary arterial tree. 39 A common cause of bovine cor pulmonale in montane areas worldwide is hypoxia due to high altitude disease (brisket disease; mal de altura crónico). 21 Brisket disease becomes relatively common above elevations of 2,500–3,500 m (8,200–11,480 feet). Stockmen in the United States began to recognize the disease in the 1880s, leading to documentation of its clinical features in 2 classic reports published in 1915 and 1918 (Glover GH, Newsom IE: 1915, Brisket disease (dropsy at high altitude). Preliminary report. Colorado Agricultural Experiment Station Bulletin 204:3–24. Available at: http://cospl.coalliance.org/fez/eserv/co:8257/ucsu2023204internet.pdf ). 19 Collaboration between veterinary pathologists and medical cardiologists in the 1950s and 1960s identified the key lesion of brisket disease as muscularization of muscular intrapulmonary arteries with functional vascular pruning.2,3 A similar syndrome affects people at high altitudes.5,42 The disease in livestock can be reversed early in its clinical course by moving affected cattle to lower elevations.4,29,40 In the United States, brisket disease generally affects beef breeds, particularly Angus and Shorthorn cattle. Cow–calf operations are most likely to be found at high elevations. There appears to be no detailed English language account of brisket disease in dairy cattle, although Holstein cattle are said to be particularly susceptible. 39 Several published reports list affected Holsteins.3,40 In addition to elevation and genetic predisposition, known or suspected risk factors for brisket disease are age, pregnancy, cold weather, rapid weight gain, intercurrent pulmonary diseases, and exposure to endotoxins, swainsonine, monocrotaline, and ionophores.6,7,22–25,31,50 Brisket-like disease may also occur in cattle at low elevations.9,39,41 Forms of cor pulmonale that mimic brisket disease include inherited dilated cardiomyopathy and heart failure secondary to acute and chronic pneumonia, bronchiectasis, disseminated pulmonary abscesses, pulmonary fibrosis, emphysema, parasitic pneumonia, and some intoxications.8,10,12,16,17,28,33,38–41
Brisket disease presents clinically as severe right-sided heart failure. 25 Affected cattle exhibit lethargy, weight loss, persistent coughing, diarrhea, distended and/or pulsating jugular veins, ventral edema, and pneumonia over a clinical course of 1–12 weeks.21,40 Morphological confirmation is based on recognizing characteristic gross and microscopic findings in heart, lung, and liver. Major gross findings are hypertrophied right ventricular myocardium; dilated right atrium, right ventricle, right pulmonary trunk, and arteries; and hepatomegaly due to chronic passive venous congestion.1,31 Diagnostic microscopic lesions in lung are hypertrophy of tunica media, adventitia in muscular pulmonary arteries. and muscularized pulmonary arterioles.3,31,48
A syndrome of right-sided heart failure in young Holstein cattle was recognized on the Colorado Front Range. Evidence is presented in the following confirming the diagnosis of brisket disease, occurring at the modest elevation of 1,600 m.
Materials and methods
Case histories
Over 5 years (2007–2011), 55 Holstein heifer calves with clinical signs of right-sided heart failure were identified in a replacement heifer-raising facility in the Colorado Front Range at an elevation of 1,600 m (site A). The facility began operation in 2005. At any one time it contained 1,000–4,000 head. Most animals dying on site were examined postmortem by a veterinarian. No cases of right-sided heart failure were recognized in the first 2 years of operation. Thereafter, cases were seen in each of the following 5 years, representing the second most common cause of mortality, after bovine respiratory disease complex (Table 1). Mortality of all causes was low in the well-managed facility (1.32%; 2007–2011). This underestimates cases of cardiac disease, as some cattle with early right-sided heart failure were sold once staff became proficient at recognizing early clinical signs. Two additional cases of right-sided heart failure were identified in commercial dairies at the same elevation. In 1 dairy (site B), annual mortality of all causes was unusually high (11.4–30.9%; 2005–2010), with 1 case of right-sided heart failure recognized in 2008. In the other dairy (site C), limited information was available about annual mortalities, with 1 case identified in 2010.
Population size, morbidity, mortality, and losses attributed to right-sided heart failure in site A (2000–2011).*
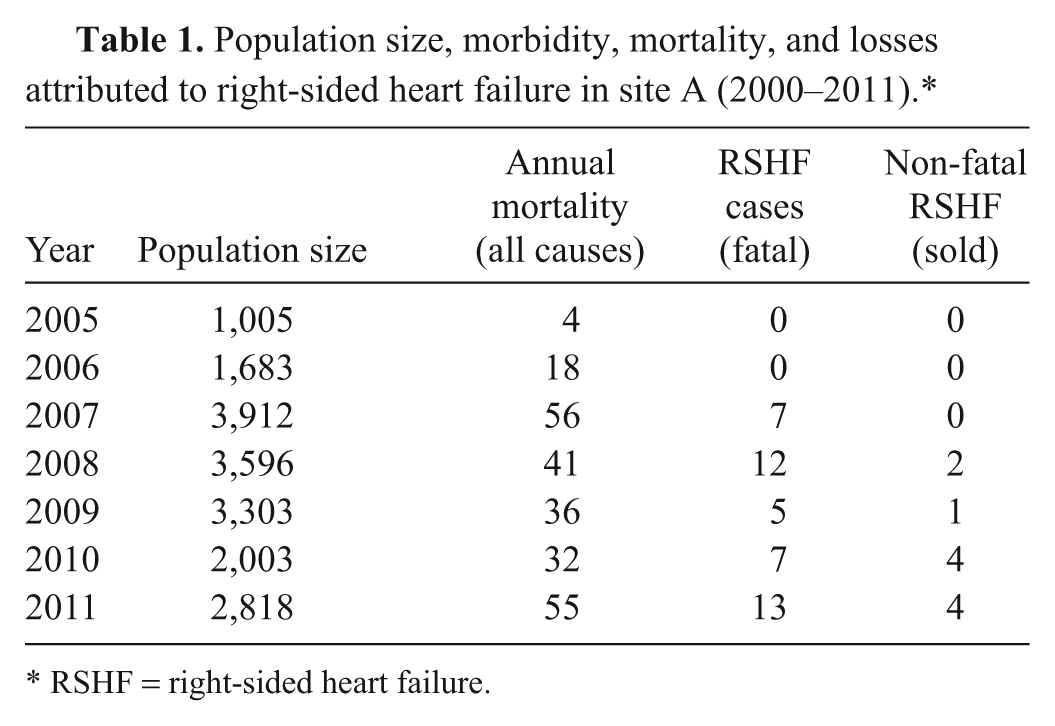
RSHF = right-sided heart failure.
Clinical examination
Physical examinations were performed on heifers that had clinical signs suggestive of heart failure. Body condition score was estimated, heart and lungs were auscultated, the presence or absence of a jugular pulse or jugular distention was recorded, and abdomens were palpated for signs of enlarged livers. Heifers were examined per rectum if sufficiently mature. Abdominocentesis was performed in individual cases where heifers had abdominal distension. Intermandibular tissue and the brisket area were palpated for evidence of edema.
Pathology
Ten Holstein heifers aged 4–15 months with typical clinical signs of right-sided heart failure were examined postmortem on site (Table 1). Whole hearts and lungs or lung samples were submitted to the Wyoming State Veterinary Laboratory (Laramie, Wyoming). In 9 out of 10 heifers, hearts were dissected and component parts weighed to establish the ratio of right ventricular free wall to total ventricular myocardium (RV/T). 20 When entire plucks were submitted to the laboratory, the proportion of pulmonary parenchyma affected by atelectasis and/or pneumonia was estimated and recorded. Samples of right and left ventricular free wall, interventricular septum, and right and left atrium were processed for histology along with pieces of lung and liver. Sections were stained with hematoxylin and eosin. Additional tissues, including kidney and brain, were processed from individual animals. Selected tissues were stained to demonstrate elastin and connective tissue (Verhoeff–Van Gieson; trichrome), 27 calcium (Von Kossa), 11 and carbohydrate (periodic acid–Schiff ). 46 The severity of vascular lesions in lung were scored semiquantitatively based on severity (0 = no lesion; +1 = mild; +2 = moderate; +3 = severe). For transmission electron microscopy, samples were taken from right ventricular myocardium of 1 affected heifer (no. 5; Table 2) within an hour of euthanasia. Minced myocardium were immersed in 2% glutaraldehyde–2% paraformaldehyde in sodium phosphate buffer (pH 7.4), post-fixed in 1% osmium tetroxide (pH 7.4), dehydrated in ethanol, and embedded in resin. Ultrathin sections were stained with uranyl acetate and lead citrate and examined using an electron microscope.
Clinical details of 10 affected Holstein heifers with right-sided heart failure.*
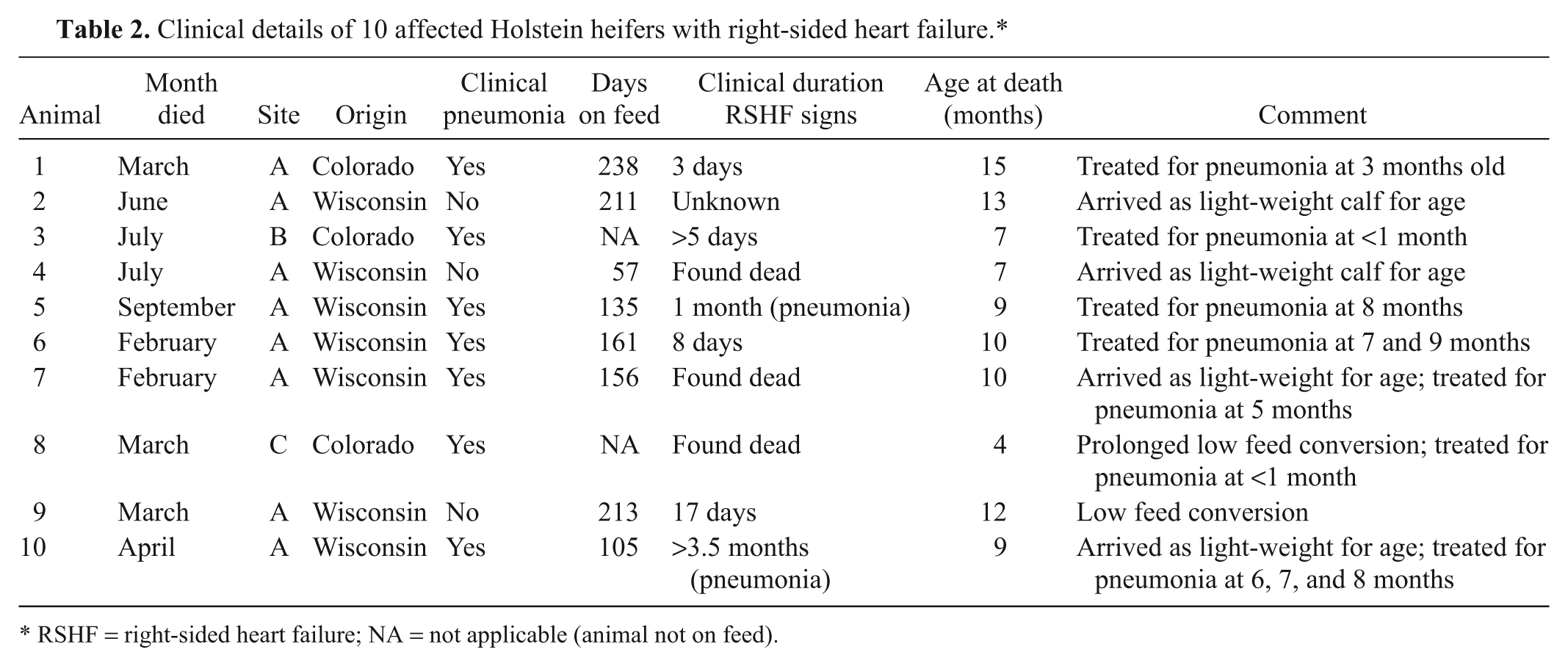
RSHF = right-sided heart failure; NA = not applicable (animal not on feed).
Morphometry of pulmonary vessels
Multiple sections of lung were examined from 10 affected cattle (= test group). Image acquisition software a was used to measure the cross-sectional area of tunica adventitia, tunica media, bronchiolar lumen, bronchiolar smooth muscle, and total arterial area in 10 arteries and their accompanying bronchioles for each of affected cattle (see Fig. 4). Muscular arteries in the 200–500-µm diameter size range were selected due to their selective involvement in brisket disease. The arteries were compared to similar measurements (10 arteries and bronchioles/animal) from lungs of 10 young cattle that died of diseases other than brisket disease; the animals were free of gross and microscopic lesions in lung and heart (= negative control group). Also measured were arteries and bronchioles from 10 beef cattle (10 arteries and bronchioles/animal) with typical gross and microscopic lesions of brisket disease (= positive control group). 3 The negative control group included both genders (3 male, 6 female, 1 unknown) and 7 locations in Wyoming plus 1 from Nebraska. The control animals were from elevations of 1,453–2,220 m, with 2 cattle breeds represented (Angus/Angus-cross and Charolais) along with 1 animal of unspecified breed. Among the negative control animals were 7 heifers with known causes of death and 1 heifer with an undetermined cause of death. The positive control group represented both genders (6 male, 3 female, 1 unknown) and were from 7 locations in Wyoming. The positive control animals were from elevations of 1,453–2,485 m, and only 1 breed (Angus) was represented. As animals in the positive and negative groups had the potential to be more variable than affected Holsteins, preliminary tests were performed to establish whether additional variables should be included in the final set of analyses. Assessments involved testing of age, elevation, and weight as possible covariates in the analyses, as well as including gender as a factor in the model. From this it was determined that gender should be considered along with the 3 treatment groups in a 2-factor factorial analysis of variance with a missing treatment combination set in a completely randomized design. 34 The missing treatment combination was male Holsteins exhibiting cor pulmonale. Using this design, the null hypothesis was tested that the response for positive and negative control groups, averaged over both genders, was the same as the average response for Holstein heifers versus the alternate, which was that at least 2 were different. Also tested was the null hypothesis that the response of females averaged over 3 treatment groups was the same as the response of males averaged over 2 control groups, versus the alternate, which was that the responses were different. The null hypothesis was tested for an interaction term that the average responses among treatment groups were not influenced by gender versus the alternate, which was that they were.
Variables tested were ratios of total arterial area-to-tunica adventitia area, arterial tunica media-to-bronchiolar lumen area, and arterial tunica media area-to-bronchiolar smooth muscle area as well as animal age, weight, and elevations at which animals were kept. Tests were conducted at the 0.05 level of type I error. Statistical computations were facilitated through use of the GLM procedure of the Statistical Analysis System. b Mean separations were conducted by using Fisher protected least significance difference via the MEANS or LSMEANS statements of the GLM procedure.
Genetic analysis
Three generations of pedigree information was obtained for the 10 affected heifers (animals no. 1–10) using the online ancestry search tool of the Holstein Association USA. c Chi-square analysis was performed to identify overrepresented sires (i.e., unequal proportions of sires) in the pedigrees.
Results
Clinical findings
When the syndrome was first recognized in 2007, the treatment crew initially assumed that affected heifers had chronic pneumonia. Such animals often presented with low-grade fever and were treated 1 or more times for pneumonia, prior to veterinary examination. Seven out of 10 cattle examined postmortem developed clinical signs after transportation 57–238 days earlier from Wisconsin (elevation: <275 m); the remaining 3 animals were born and raised at 1,600 m (Table 2). Clinical findings were distended abdomen, poor body condition, jugular pulse or distended jugular veins, a palpably enlarged liver, cardiac murmur over tricuspid or mitral valves, and submandibular and brisket edema of varying severity. Cattle with milder or earlier signs of cardiac disease were flagged for veterinary examination as the work crew became more experienced at distinguishing heart failure from chronic pneumonia; no treatment was attempted once cor pulmonale was diagnosed. Affected cattle were euthanized or sold, depending on marketability.
Pathology
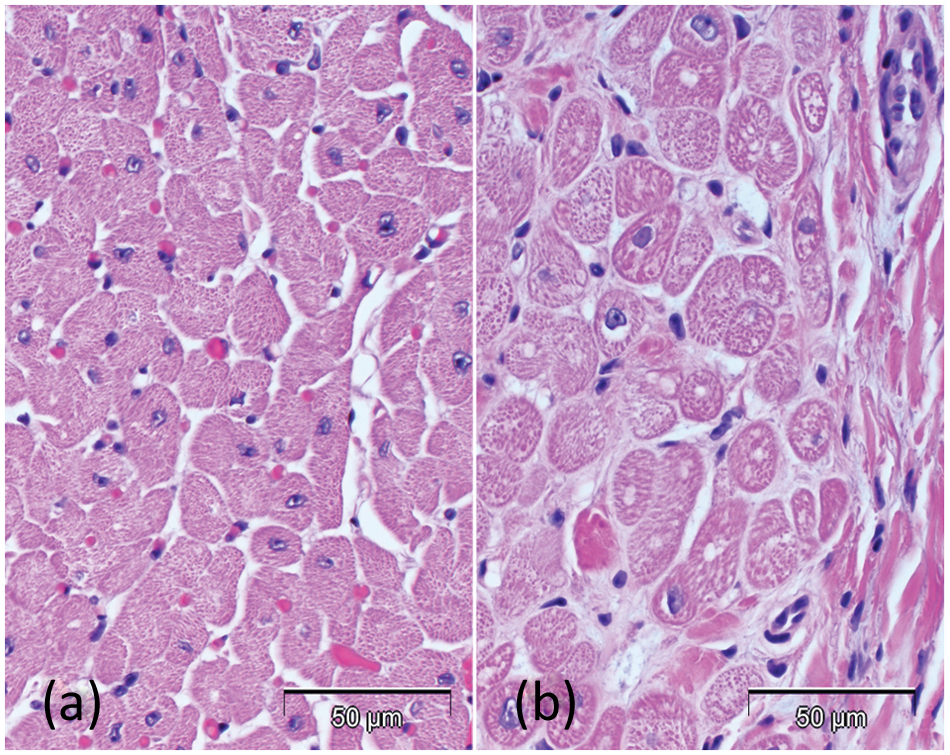
The 10 affected heifers were thin with serous atrophy of pericardial, mesenteric, and perirenal fat. Moderate edema affected dependent areas such as the intermandibular space and the brisket. The main necropsy findings were severe hypertrophy of right atrial and ventricular myocardium, dilated pulmonary trunk, right atrium and right ventricle (Figs. 1, 2), hepatomegaly (Fig. 3), ascites, and edema of abomasal mucosa, mesentery, and mesocolon. Gross lesions affected the lungs of 9 of 10 cattle. These consisted of anteroventral atelectasis with exudative pneumonia, atelectasis alone, or bronchiectasis. Pulmonary lesions involved 1–35% of pulmonary parenchyma (Table 3). The mean ratio of right ventricle myocardium to total ventricular weight was 0.37 (range: 0.35–0.49; reference range: 0.25 ± 0.011).1,2 Cross-sectioned hearts revealed hypertrophy of right ventricular myocardium. No myocardial necrosis or fibrosis, valvular disease, subaortic stenosis, or hypertrophy of left ventricular myocardium was found. Hepatic changes were severe and comprised atrophy and loss of centrilobular hepatocytes, with fibrosis of central vein and central-central bridging fibrosis (chronic passive congestion). Histological change affected the pulmonary vascular tree, involved muscular arteries, and was generally modest; such lesions were restricted to the lungs (Table 3). The most consistent vascular feature was expanded tunica adventitia with microvascular proliferation (Figs. 4, 5). Less consistent features included intimal fibrosis and medial hyperplasia (3/10 and 6/10 animals, respectively), occlusive thrombosis (2/10), and disrupted and mineralized inner elastic lamina (1/10; Fig. 6). Muscularized arterioles were found in 4 out of 10 animals (Fig. 7). One animal had marked vascular change, which comprised hypertrophic tunica media and adventitia, with pronounced intimal hyperplasia (Fig. 8). Histologically, cardiocytes in right atrium, right ventricular myocardium, and in interventricular septum were up to twice the diameter of cardiocytes in healthy, age-matched cattle (Fig. 9a, 9b). In 2 affected cattle, there was mild acute multifocal myocardial necrosis in right atrial wall, accompanied by mineralization. Ultrastructurally, cardiocytes contained orderly bundles of actin and myosin filaments with no evidence of myofibrillar lysis (Fig. 10a, 10b). Features that are typical of bovine cardiomyopathy (excessive glycogen, abnormal mitochondria, dilated endoplasmic reticulum, invaginated basal laminae, streaming Z-disks, increased endomysial matrix) were absent.
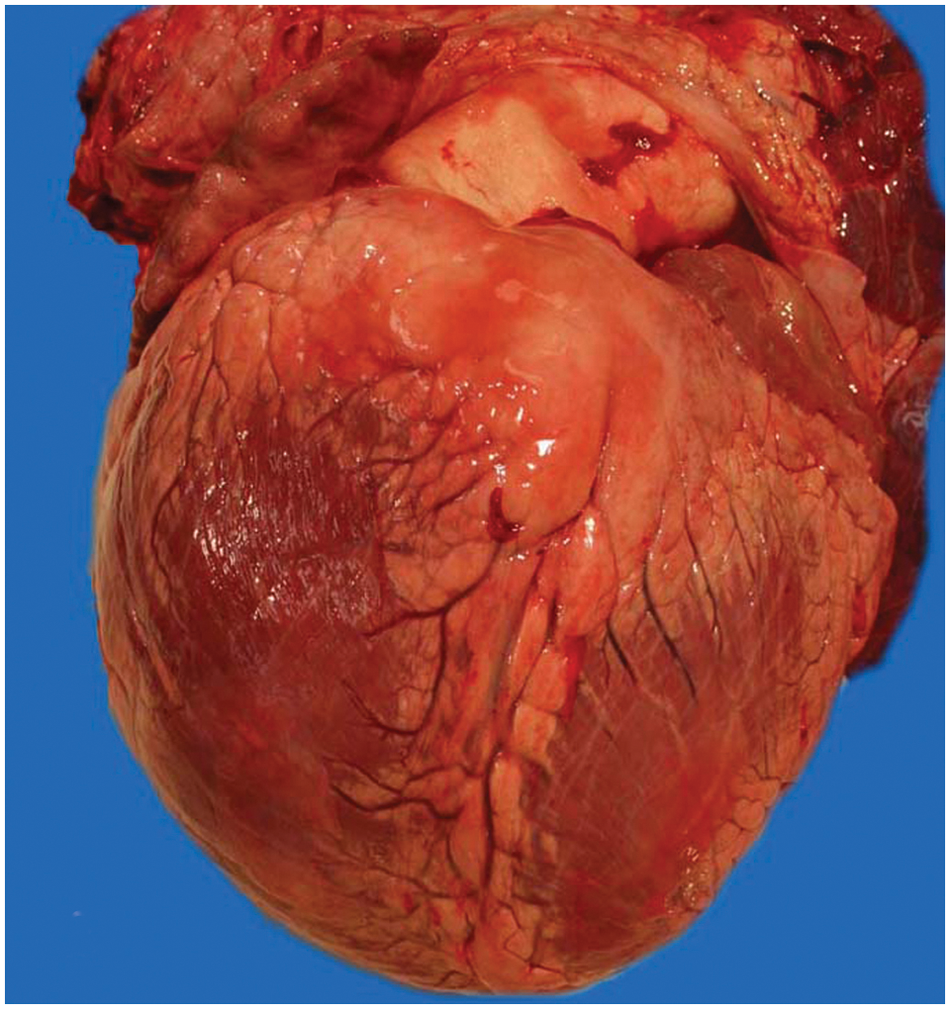
Animal no. 9; bovine heart. Typical gross appearance of heart in 1-year-old heifer with observed clinical signs for 17 days. Note hypertrophy of right ventricular myocardium. Some serous atrophy of adipose tissue is present.
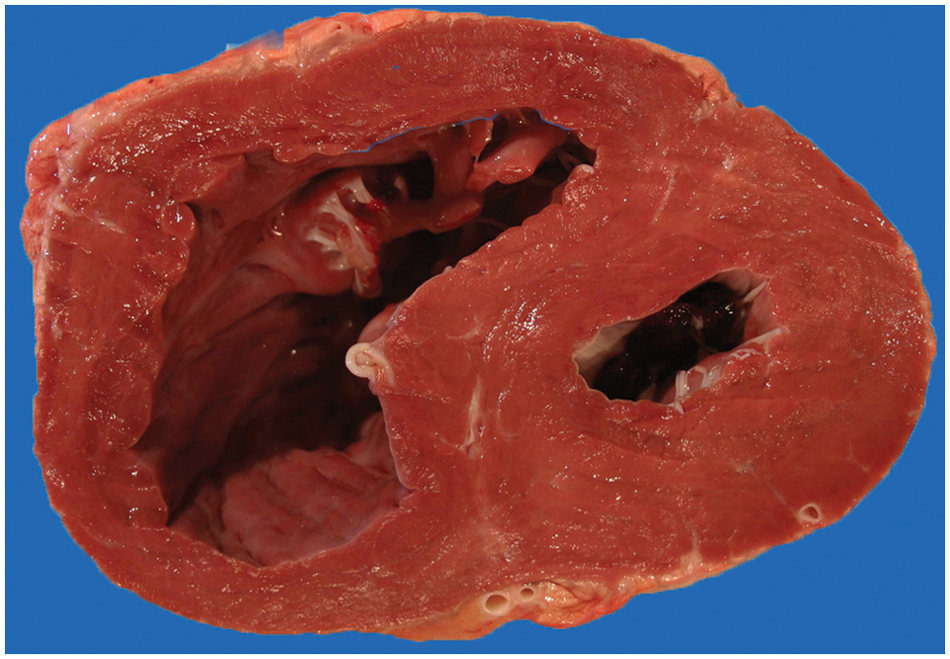
Animal no. 9; bovine heart. Marked hypertrophy of right ventricular myocardium. There is no gross evidence of myocarditis or fibrosis.
Pulmonary and cardiac lesions in 10 affected Holstein heifers with right-sided heart failure.
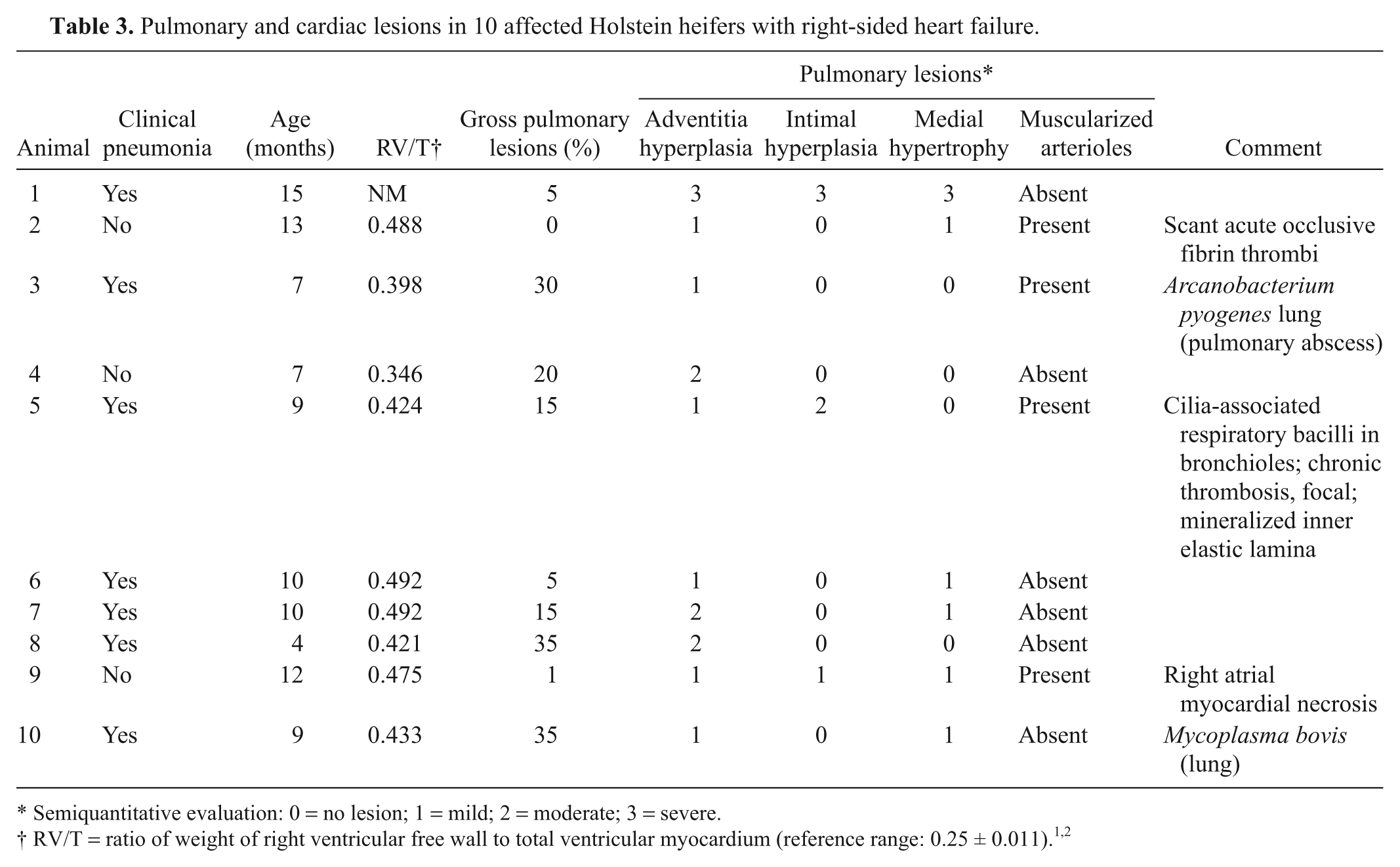
Semiquantitative evaluation: 0 = no lesion; 1 = mild; 2 = moderate; 3 = severe.
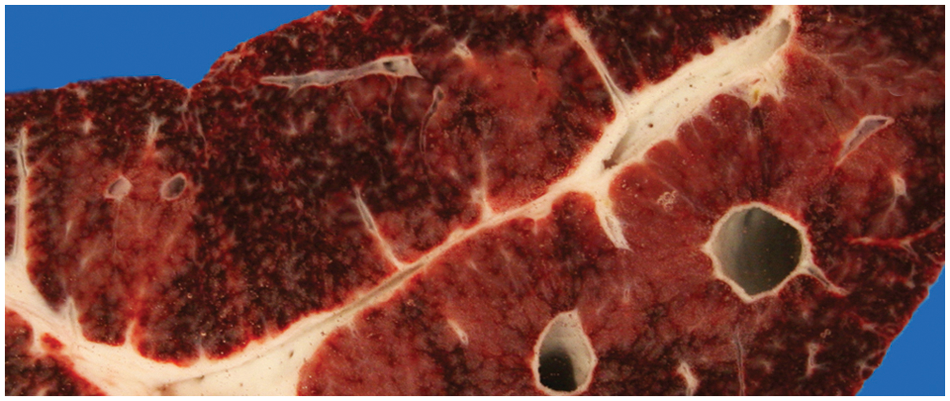
Animal no. 9; bovine liver. Marked diffuse chronic passive congestion (nutmeg liver).
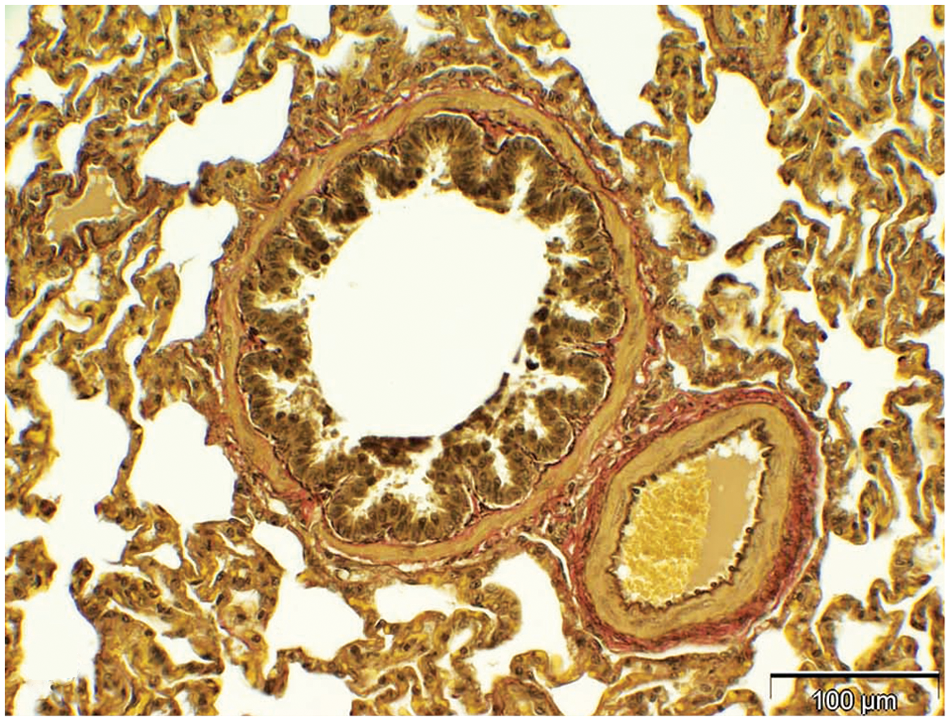
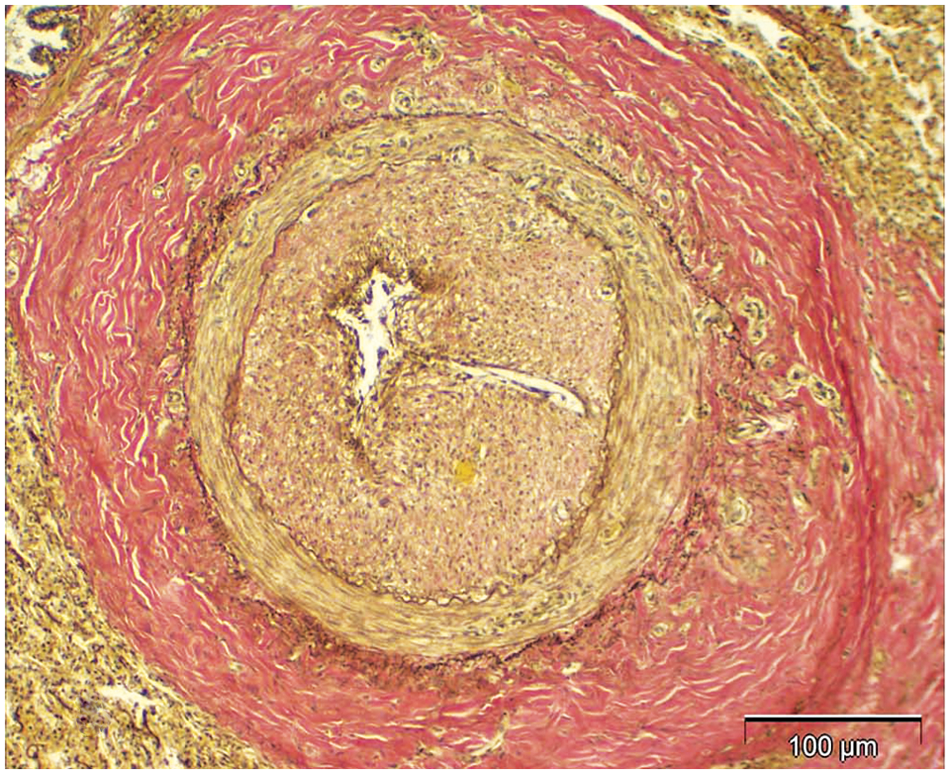
Control yearling; bovine lung. Normal bronchiole with associated muscular artery. In normal cattle, the muscular artery is smaller than the bronchiole with which it is partnered, and the tunica adventitia is inconspicuous. Verhoeff–Van Gieson stain. Bar = 100 µm.
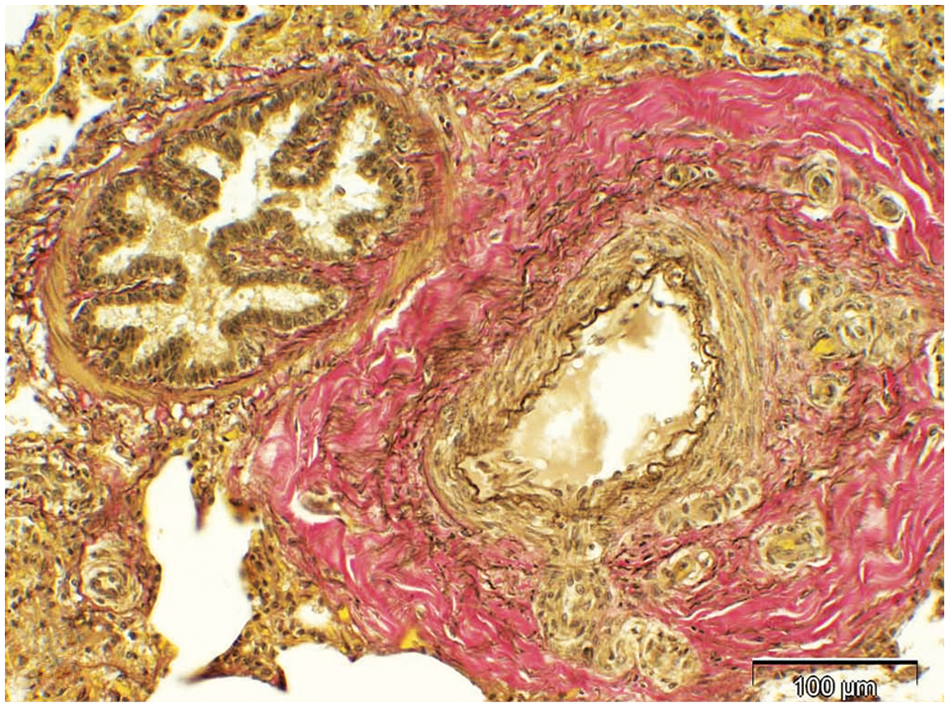
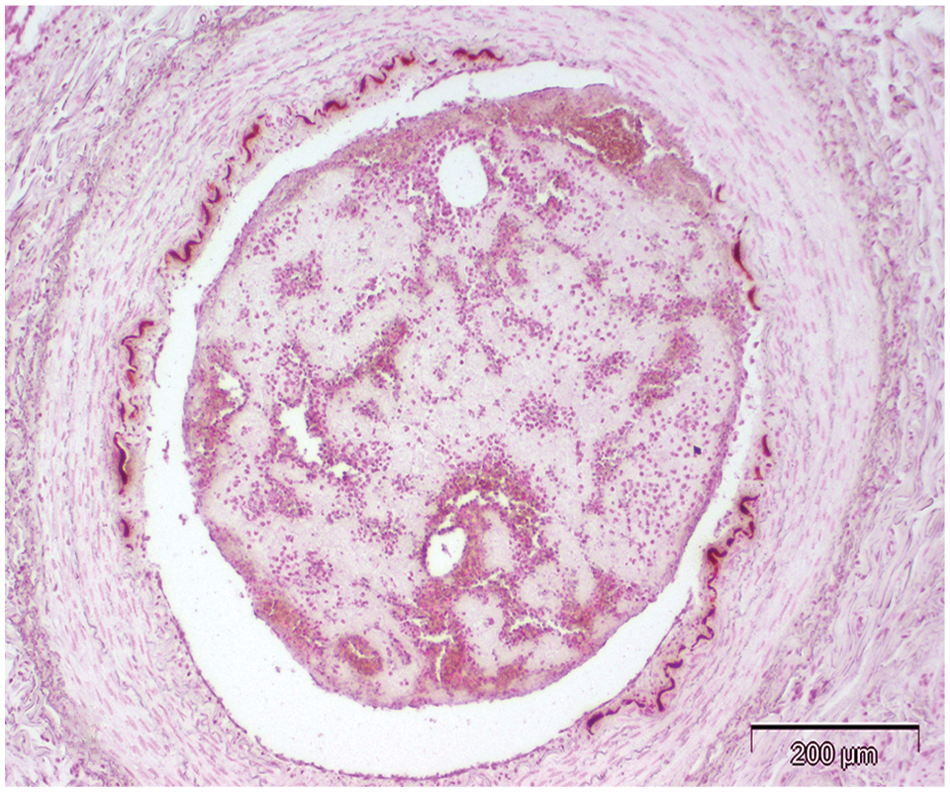
Animal no. 7; bovine lung. Bronchiole with associated muscular artery. In contrast to normal lung (Fig. 4), the artery is larger than adjacent bronchiole. Tunica adventitia is expanded and contains associated small vessels; 3+ (severe) lesion. Tunica media is hypertrophied. Verhoeff–Van Gieson stain. Bar = 100 µm.
Animal no. 5; bovine lung. Focal calcification of inner elastic lamina. Intimal hyperplasia graded as a moderate (1+) severity lesion. There is an intraluminal fibrin thrombus. Von Kossa stain. Bar = 200 µm.
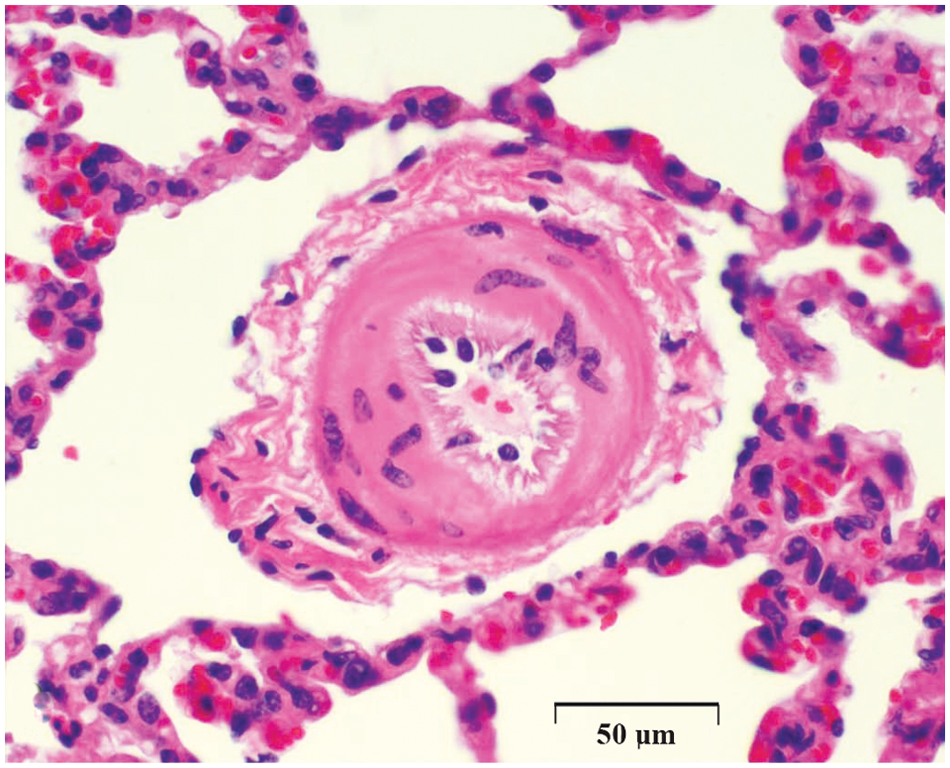
Animal no. 5; bovine lung. Hypertrophic tunica media of pulmonary arteriole, resulting in reduced luminal caliber. Hematoxylin and eosin. Bar = 50 µm.
Animal no. 1; bovine lung. Severe arterial hyperplasia involving intima, media, and adventitia; graded as severe (3+) lesion. Verhoeff–Van Gieson stain. Bar = 100 µm.
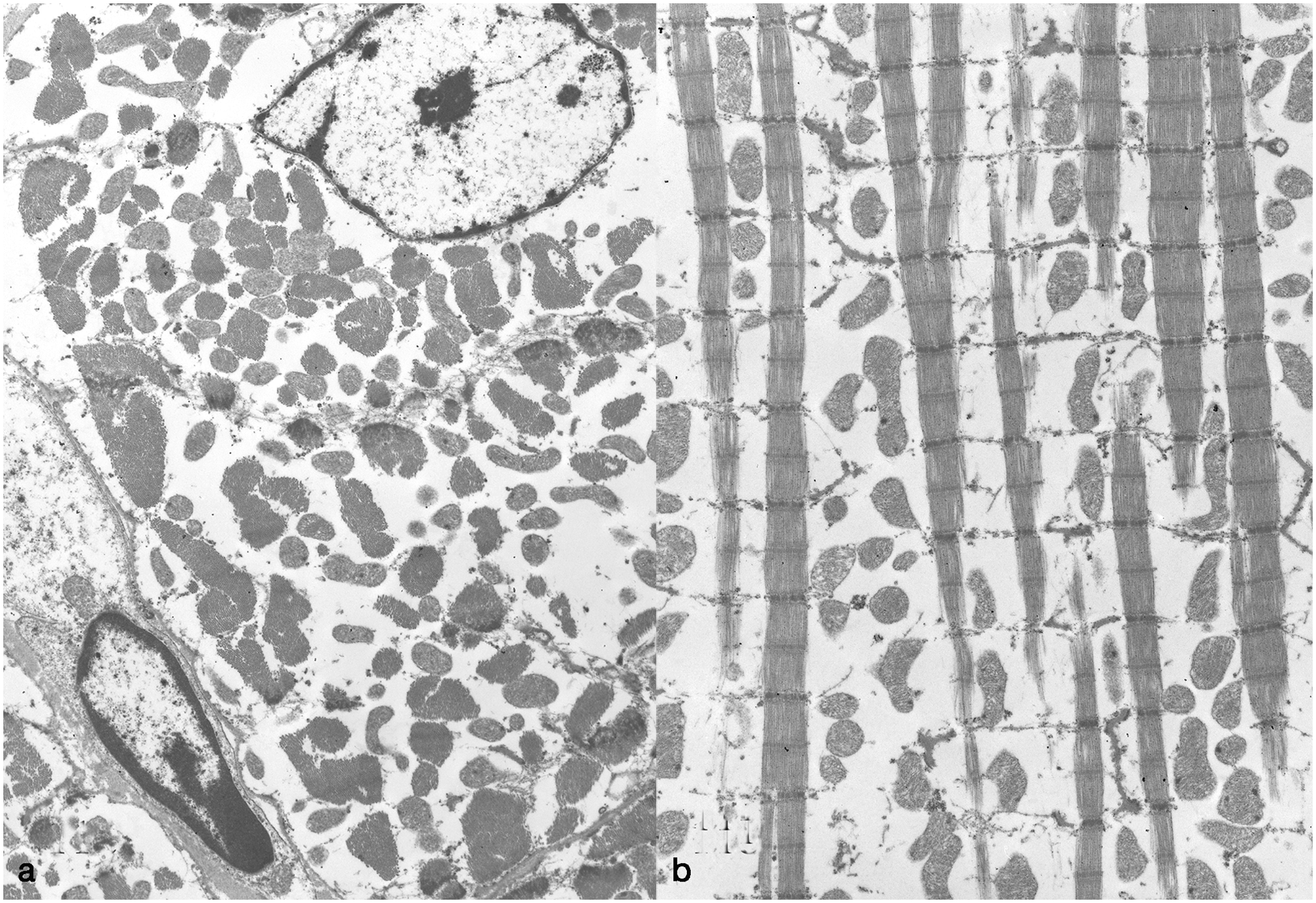
Animal no. 5; bovine heart.
Morphometry
Results indicated that no differences occurred among treatment groups or the 2 genders for animal age or weight, plus no treatment × gender interaction occurred (P > 0.05). For elevation, however, there was a significant treatment effect, F(2, 22 = 11.19, P = 0.0004) with positive (2,057 m) and negative (1,884.8 m) control groups having been kept at significantly greater elevations than the Holstein heifers with cor pulmonale (1,554.4 m). As a precaution, elevation was used as a covariate in the 2-factor factorial to see whether the results should be adjusted for elevation. Results from fitting the covariate in the analyses for total arterial area-to-tunica adventitia area, arterial tunica media-to-bronchiolar lumen area, and arterial tunica media area-to-bronchiolar smooth muscle area ratios indicated that it was not significant (P > 0.05), so elevation as a covariate was dropped from the model. Resulting tests for total arterial area-to-tunica adventitia ratios indicated that differences occurred among the treatment groups, F(2, 22 = 4.07, P = 0.0312) with the relative percentage of tunica adventitia for the positive control group being significantly greater than that of the negative control group; average adventitial area in Holstein heifers was intermediate (Fig. 11). Neither a gender effect nor a treatment × gender interaction was apparent for this variable (P > 0.05). Analyses for total arterial area-to-bronchiolar lumen area ratios indicated that a significant treatment × gender interaction had occurred, F(1, 22 = 4.33, P = 0.0494). Mean separations among treatments, conducted separately by gender, indicated arterial tunica media-to-bronchiolar lumen area for the positive control and Holstein heifer groups were greater than the negative controls (Fig. 12). In addition, there was no difference between the positive control and Holstein heifer groups. For the males, however, the positive and negative control group averages were the same (Fig. 13). Analyses for arterial tunica media-to-bronchiolar smooth muscle area ratios again indicated that a significant treatment × gender interaction was present, F(1, 22 = 4.37, P = 0.0494). Mean separations among treatments, conducted separately by gender, indicated that average arterial tunica media area-to-bronchiolar smooth muscle area ratios were greater for the positive control and Holstein heifer groups than for the negative control group. In addition, there was no difference between the positive control and Holstein heifer groups. For the males, however, the positive and negative control group averages were the same.
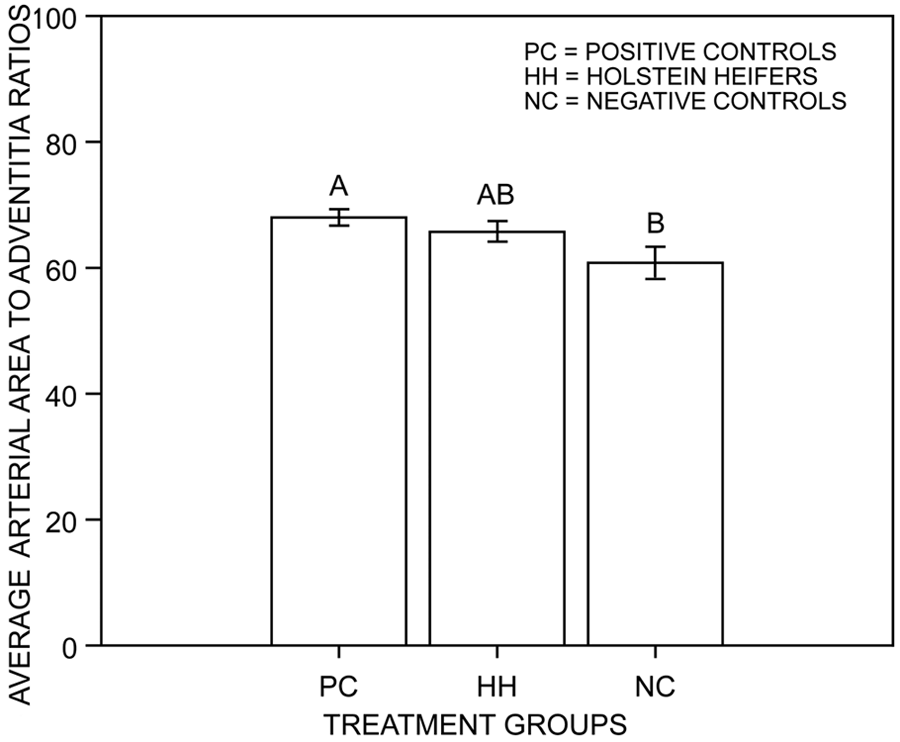
Average ratios for total arterial area-to-tunica adventitia area in each of 3 treatment groups. Positive controls were animals that died of brisket disease; negative controls were animals that did not die of brisket disease, and Holstein heifers were animals with cor pulmonale. Bars associated with the same letters were not significantly different at the 0.05 level of type I error (Fisher protected least significance difference).
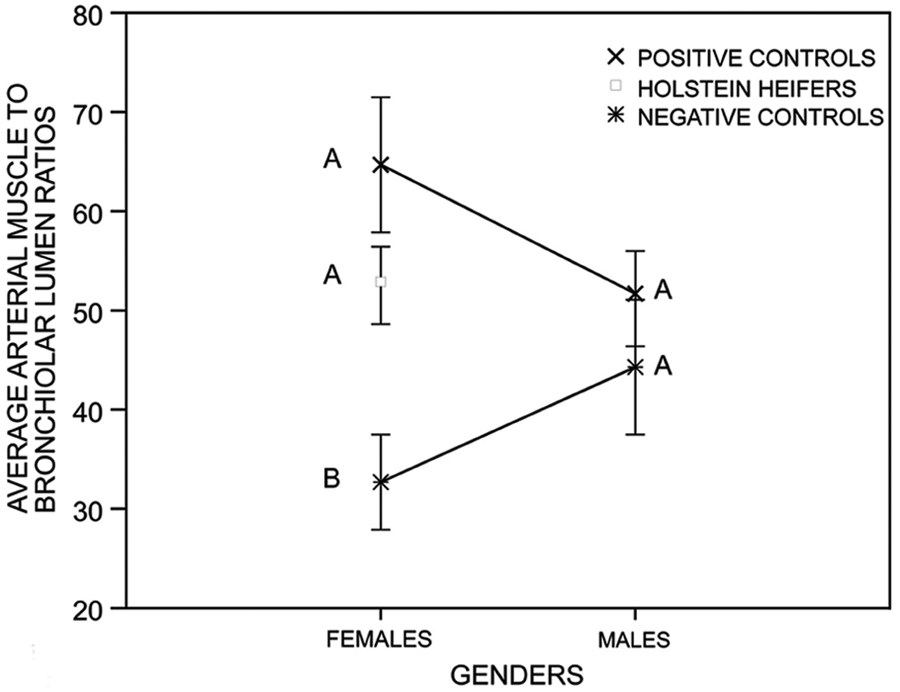
Average ratios for total arterial tunica media-to-bronchiolar lumen area for each of 3 treatment groups, separated by gender. Positive controls were animals that died of brisket disease; negative controls were animals that did not die of brisket disease, and Holstein heifers were animals with from cor pulmonale. Symbols within gender followed by the same letter are not significantly different at the 0.05 level of type I error (Fisher protected least significance difference).
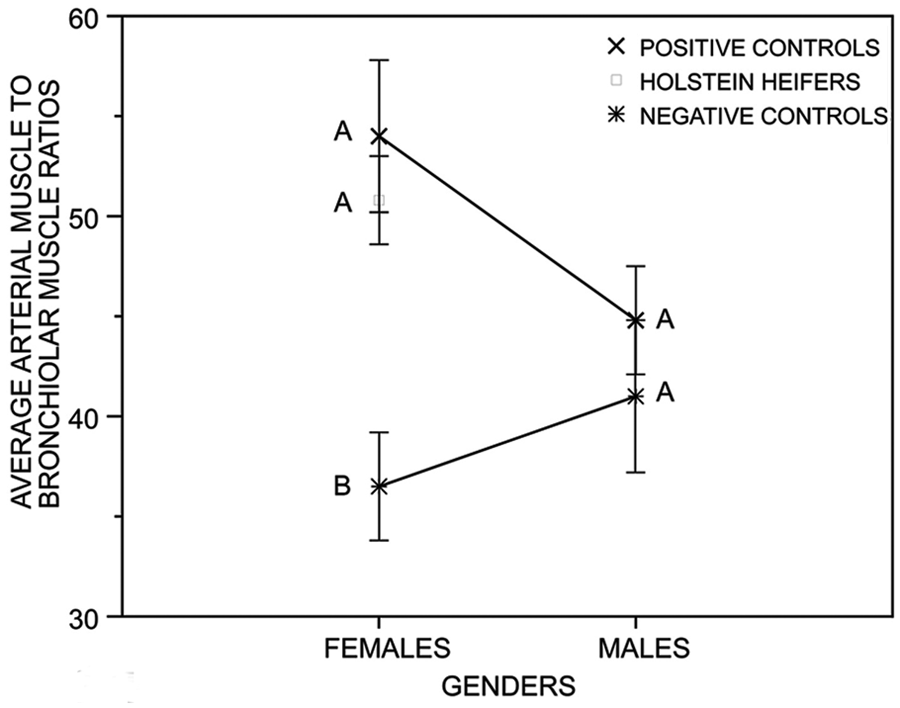
Average ratios for total arterial tunica media-to-bronchiolar smooth muscle area for each of 3 treatment groups, separated by gender. Positive controls were animals that died of brisket disease; negative controls were animals that did not die of brisket disease and Holstein heifers with cor pulmonale. Symbols within gender followed by the same letter are not significantly different at the 0.05 level of type I error (Fisher protected least significance difference).
Genetic analysis of pedigrees of affected cattle
No sire was represented more than 4 times in the pedigree. Holstein–Friesian sires that are common ancestors for dilated cardiomyopathy (i.e., ABC Reflection Sovereign, Montwick Red Apple Sovereign) 30 were present in pedigrees. Only 1 full-sibling pair was affected in the pedigree. However, without pedigree information on unaffected related calves, the potential for a genetic influence on right ventricular hypertrophy cannot be discounted.
Discussion
Clinical signs and lesions in this syndrome are consistent with brisket disease, albeit with more subtle histological changes in pulmonary arteries than those seen in beef cattle that die of right-sided heart failure at high elevations. The most likely explanation for the difference in severity is prompt clinical identification in dairy cattle. The Holsteins were euthanized shortly after a clinical diagnosis was made by veterinarians, whereas tissues from beef cattle with brisket disease tend to be submitted by owners for laboratory examination after a longer clinical course. Morphological changes in arteries are a consequence of reflex vasoconstriction. A longer clinical course is more likely to result in overt lesions. 4
The 10 Holstein cattle had 1 or more of the characteristic intrapulmonary vascular lesions of brisket disease, the most consistent of which was adventitial hyperplasia. Arteriolar muscularization was present in some affected cattle and was minimal or absent in others. All 10 had moderate to severe right-sided hypertrophy, as defined by the ratio of the weight of the right ventricular free wall to total ventricular myocardium. The mean RV/T ratio in affected Holsteins was comparable to that of beef cattle dying of brisket disease. 1 There was no evidence of cardiomyopathy, valvular disease, or other condition that might account for right-sided heart failure. Cor pulmonale can occur secondary to pneumonia and/or atelectasis, and 1 or both lesions were present in 9 out of 10 cattle examined. Pneumonia was generally mild in most affected Holsteins and interpreted to be a consequence, rather than a cause, of right-sided heart failure.
It is unlikely this disease is dilated cardiomyopathy of Holstein–Friesian cattle,30,31 which is characterized by clinical signs that are largely attributable to right-sided heart failure with histological features including hypertrophy of intra-pulmonary vessels. 30 Unlike Holstein–Friesian cardiomyopathy, however, there was no evidence that Holsteins in Colorado had lesions in the left ventricular myocardium. Other features of bovine cardiomyopathy, such as widespread necrosis, vacuolation of cardiocytes, and endomysial–perimysial fibrosis,10,36 were absent in the 10 Holsteins. Reported ultrastructural features in cardiocytes in cardiomyopathy cattle include intracytoplasmic membrane-bound vacuoles 10 and mitochondrial change. 18 Neither feature was found in 1 heifer examined ultrastructurally in the current study. The changes seen were more consistent with uncomplicated cardiocyte hypertrophy. 14 The pedigrees of the 10 animals were free of foundation sires of Holstein–Friesian cardiomyopathy as recognized in Europe,10,30 Japan, 18 Australia, 32 and Canada (Baird JD: 1988, Dilated cardiomyopathy in Holstein cattle. Clinical and genetic aspects. In: Proceedings of the sixth annual Veterinary Medical Forum, Am Coll Vet Int Med, pp. 175–177. Washington DC). Affected Colorado cattle were not tested for the optic atrophy 3 (OPA3) gene mutation now considered responsible for late-onset dilated bovine cardiomyopathy 37 ; the mutation was reported after the present morphological study was completed. No DNA was banked to examine for this or other possible causative mutations.
An underappreciated aspect of intra-pulmonary vascular lesions in brisket disease is their subtlety. The hallmark lesion of brisket disease is medial hypertrophy in muscular arteries and arterioles and occurs in most but not all affected cattle. 3 Other vascular changes, such as adventitial hyperplasia, intimal mineralization, thrombosis, and mineralization of inner elastic lamina, affect <50% of brisket disease cases. 3 Adventitial hyperplasia was the most consistent pulmonary finding in the current study (10/10; 100%). In most, it was mild, with severe change occurring in only 1 animal. Other lesions were medial hypertrophy of muscular arteries and arterioles (90%), intimal hyperplasia (30%), mineralization of inner elastic lamina (10%), and thrombosis (20%). It can be difficult to make an unequivocal diagnosis of brisket disease in some beef cattle based on histological examination of lung alone. Confirmation requires the presence of typical lesions in right and left atria and ventricles of the heart, evidence of severe chronic passive congestion in liver, a history that animals were at high elevation, and absence of other lesions to account for cor pulmonale.
Premises with affected Holsteins were at 1,600 m. Brisket disease is generally a problem at elevations above 2,000 m. Some published reviews make categorical statements about the altitude above which cattle are prone to develop brisket disease. 31 Elevations below 1,500 m (<5,000 feet) are generally considered safe, which is why affected cattle can be salvaged by moving them to that elevation. 40 Nevertheless, brisket disease affects a small proportion of cattle at 1,000 m. This was well recognized in feedlots on the Colorado high plains. One survey of feedlot cattle at 1,600 m reported that brisket disease accounted for 5.8% of all deaths. 26 The heifer-raising facility investigated herein was at 1,600 m, and brisket-like disease accounted for 21.8% of all deaths over 7 years. It would have been ideal to measure pulmonary arterial pressures in the 10 affected cattle, but this is not a service offered by diagnostic laboratories.
Recognized causes of pulmonary hypertension in people are more numerous than in cattle.15,43,45 At present, the most important diagnostic rule-out for right-sided heart failure in cattle at high elevations is brisket disease. According to the current human classification, disease in these cattle fell under the ambit of group 3: pulmonary arterial hypertension due to alveolar hypoxia and residence at high altitude. It was not possible to conclusively exclude underlying genetic or other environmental factors, but no common parentage was detected in the 10 cattle examined. Brisket disease has a modest genetic component.13,44,47,49 Inability to identify a common bloodline in the present study could be due to the presence of genetic susceptibility in multiple Holstein pedigrees and/or the small number of pedigrees examined. Germline or de novo mutations in members of the transforming growth factor β signaling family are associated with a high proportion of idiopathic and heritable pulmonary hypertension cases among people. 15 Comparable mutations in cattle might account for the development of disease in a small proportion of animals moved to the modest elevation of 1,600 m. It is noteworthy that mutations in the genes for human transforming growth factor β are necessary but insufficient alone to induce disease; unidentified modifier genes, epigenetic factors, and/or environmental co-factors are required to trigger clinical expression. 15 There was no exposure to recognized or suspected toxic risk factors for pulmonary hypertension in people, such as toxic rapeseed oil and St. John’s wort. Several connective tissue disorders such as systemic sclerosis can predispose people to pulmonary hypertension. Other risk factors are chronic viral infections, portal hypertension, congenital systemic-to-pulmonary shunts, parasitism, chronic hereditary and acquired hemolytic anemias, chronic myeloproliferation, pulmonary veno-occlusive disease, left heart disease, chronic pulmonary thromboembolism, some storage diseases, hypothyroidism, and hyperthyroidism. 15 Most can be excluded as risk factors in the cattle described herein, given the absence of appropriate gross or microscopic lesions.
In summary, a brisket-like disease occurred in Holstein cattle backgrounded at elevations of 1,600 m. Histological changes in lung were similar to, but milder than, brisket disease in beef cattle grazed at higher altitudes.
Footnotes
Acknowledgements
Paula Jaeger, Mercedes Thelen, Breanna Bonner, and Katy Fambrough assisted with necropsy examination and histological preparations. Thanks are extended to colleagues Drs Greg Goodell, Scott T. Smith, and Chris Koeller for performing clinical examination of some affected cattle
a.
MicroSuite Basic Edition, Olympus America Inc., Center Valley, PA.
b.
SAS version 9.2, SAS Institute Inc., Cary, NC.
c.
Holstein Association USA Inc., Brattleboro, VT (http://www.holsteinusa.com/services?action=displayPage&pagename=/extendedPedigree.html).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Portions of this work were supported by the USDA Animal Health program WYO-397-05, which funded the work of Jana Marquard while a pre-veterinary student at the University of Wyoming.