
Abstract
Cefoxitin disk diffusion susceptibility testing is a recommended screening method for the detection of methicillin resistance in human isolates of Staphylococcus aureus and coagulase-negative staphylococci. A retrospective analysis of 1,146 clinical isolates of Staphylococcus pseudintermedius from dogs was conducted to determine if screening by the cefoxitin disk method can be similarly useful with S. pseudintermedius. The distribution of cefoxitin growth inhibition zone diameters within this collection was bimodal and correlated well with the results of methicillin resistance gene (mecA) detection by polymerase chain reaction. Of the isolates, 5% had discordant results and, when retested, 84% of these were in agreement. While a greater diversity of isolates and interlaboratory comparisons must be tested, the current study suggests that an epidemiological breakpoint (of approximately ≤30 mm = resistant; ≥31 = susceptible) can be established to predict methicillin resistance in S. pseudintermedius.
Cefoxitin disk diffusion susceptibility testing is a widely used screening method to detect methicillin resistance in Staphylococcus aureus and coagulase-negative staphylococci (CNS) isolated from human beings. 9 “Gold standard” confirmatory tests for detection of methicillin resistance include methicillin gene (mecA) detection by polymerase chain reaction (PCR) and penicillin-binding protein 2a (PBP2a) detection with specific antibody. 9 In studies that included over 200 isolates each, cefoxitin disk diffusion tests for detection of methicillin resistance in S. aureus had sensitivities and specificities ranging from 96.5% to 100% and 99% to 100%, respectively.5,6,16 Unlike similar testing with oxacillin, cefoxitin disk diffusion testing does not require additional supplementation of media or altered incubation conditions. 16 Zones of growth inhibition may also be more clearly demarcated and easier to interpret.9,16
Previous studies have demonstrated that cefoxitin disk diffusion tests using interpretive guidelines recommended for human isolates of S. aureus and CNS were unreliable indicators of methicillin resistance in Staphylococcus pseudintermedius isolates from dogs.3,4,12,15,18 Such tests resulted in unacceptably high levels of very major errors (resistant isolates called susceptible) and low (34–57%) agreement with mecA gene detection by PCR.3,4,15 However, cefoxitin disk diffusion test specificity was high (100%) and correlation with oxacillin disk diffusion was good (R = 0.85). 4 Receiver operating characteristic analysis of one data set suggested that an optimum cefoxitin disk diffusion breakpoint for predicting methicillin resistance in S. pseudintermedius would be ≤33 mm. 4
The current study examined the feasibility of establishing cefoxitin disk diffusion interpretive criteria specific for S. pseudintermedius isolates from dogs. Isolates were from canine clinical samples received at the University of Tennessee Clinical Bacteriology and Mycology Laboratory (Knoxville, Tennessee) between 2006 and 2011. Isolates from each patient were unique with respect to body site of isolation, antimicrobial susceptibility profile, and year of isolation. In some cases, more than 1 isolate came from a patient but each isolate was unique in all of these factors. Results of cefoxitin disk diffusion susceptibility tests and mecA PCR were analyzed retrospectively for those isolates (total of 1,146) that had been subjected to both tests. This was a convenience sample that was not representative of the true distribution of methicillin-susceptible S. pseudintermedius (MSSP) and methicillin-resistant S. pseudintermedius (MRSP) in the local population of clinical isolates. The examined isolates did, however, contain nearly all MRSP from all years of the study, all MSSP from 2006, and approximately 25 MSSP from each quarter in years 2010 and 2011. The population was not entirely restricted in geographic origin to the immediate area of the laboratory, as a small proportion (not determined) of isolates were obtained from samples received from veterinary dermatology and referral practices in Florida, Oregon, and the surrounding states of North Carolina and Kentucky.
Members of the Staphylococcus intermedius group (SIG) consist of the closely related species S. intermedius, S. pseudintermedius, and Staphylococcus delphini. 10 Identification of S. pseudintermedius was performed as previously described using a minimal number of conventional biochemical tests. 3 Isolates having a typical colony morphology with a double zone of hemolysis on blood agar that were tube coagulase positive at 24 hr, that fermented lactose and trehalose in phenol red broth at 18–24 hr, were negative for acetoin production at 48 hr by the Barritt method, and did not ferment maltose in 18 hr on agar medium containing bromcresol purple were presumptively identified as S. pseudintermedius.3,7 Such identification was consistent with generally accepted convention for clinical isolates from dogs, as S. pseudintermedius is the only member of the SIG, identified by traditional means, that has been recovered from dogs.10,14 Identities of isolates that gave equivocal results in any of the expected biochemical reactions were confirmed by phosphate acetyltransferase (pta) gene PCR followed by MboI restriction analysis or by DNA sequencing analysis of 16S ribosomal RNA or pta genes.2,3
Cefoxitin disk diffusion susceptibility tests were performed according to the Clinical and Laboratory Standards Institute standard reference method. 8 Polymerase chain reaction for mecA gene was performed either by conventional or real-time methods.1,3,4
The cefoxitin growth inhibition zone diameters were distributed in a bimodal fashion (Fig. 1), with 2 large peaks separated by a narrow gap, similar to that seen previously with S. aureus. 16 The mecA gene was detected by PCR in 602 isolates. Intermethod agreement was 95% (kappa statistic; κ = 0.89) when an arbitrary epidemiological breakpoint for cefoxitin zone diameter was set at ≤30 mm for resistant and ≥31 for susceptible. 17 Using this interpretive criterion, sensitivity and specificity for predicting methicillin resistance was 97% and 92%, respectively (Table 1). Very major errors were at the upper acceptable limit of 1.5%, and total errors were 5%. 11
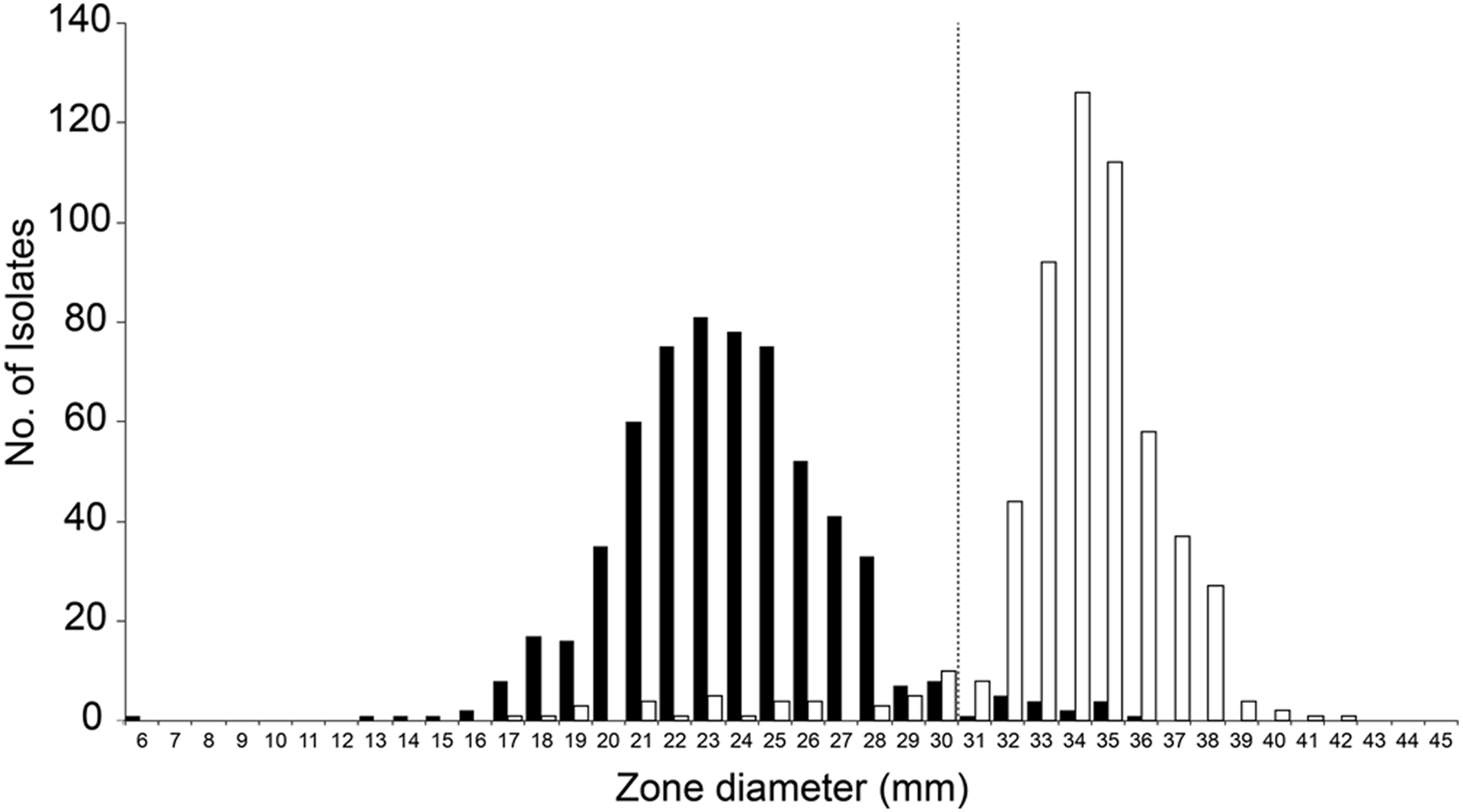
Cefoxitin disk diffusion growth inhibition zone diameters obtained with Staphylococcus pseudintermedius isolates from dogs. Vertical line indicates proposed epidemiological breakpoint. Black bars indicate mecA gene polymerase chain reaction (PCR) positive; white bars indicate mecA gene PCR negative.
Results of the evaluation of the use of cefoxitin disk diffusion as a predictor of methicillin resistance in Staphylococcus pseudintermedius.
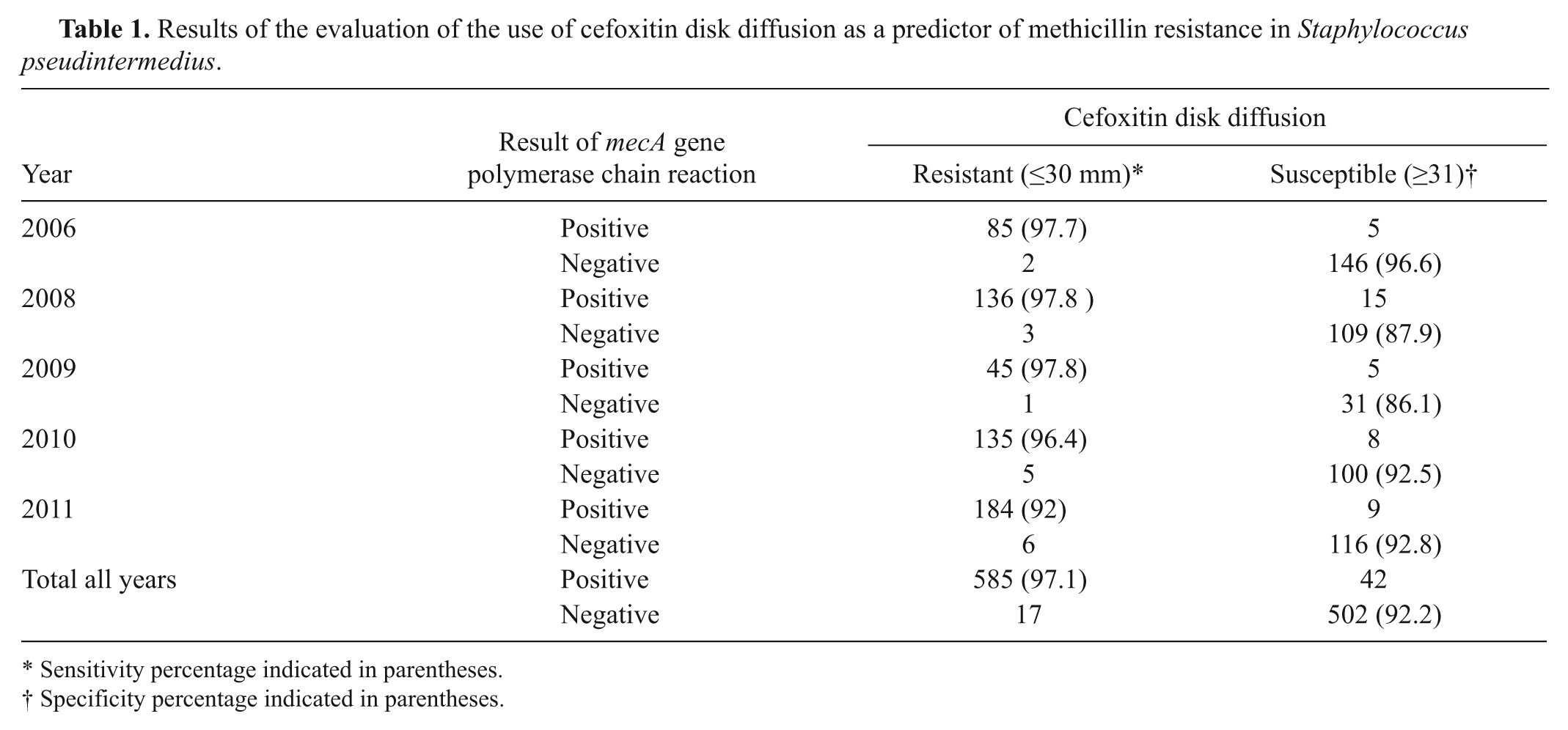
Sensitivity percentage indicated in parentheses.
Specificity percentage indicated in parentheses.
Repeat testing was performed on 59 isolates with discordant results. Stock cultures frozen at −80°C at the time of initial isolation were derived from a single well-isolated colony. Repeat testing was performed in 2012 from frozen stock. The following tests were each separately performed in blinded fashion by single individuals: species verification by pta gene PCR followed by MboI restriction endonuclease analysis; 2 cefoxitin disk diffusion susceptibility testing by the standard reference method; 9 and mecA gene detection by conventional PCR, with previously described primers and procedures. 1 All retested isolates were confirmed as S. pseudintermedius, and results of cefoxitin disk diffusion and mecA gene PCR were in agreement for 84%. Of the remaining 9 discordant isolates, 3 had false-susceptible results with cefoxitin zone diameters of 33 mm or 34 mm. For each of these 3 isolates, mecA was positive and cefoxitin zone diameters differed by no more than 1 mm on both initial and repeated tests. A mechanism for the apparent cefoxitin susceptibility in these isolates is unknown; each was resistant to oxacillin (zone diameters 13 mm or 16 mm). It is worth noting that if both oxacillin and cefoxitin are tested against human isolates of S. aureus and Staphylococcus lugdunensis, and either result is resistant, it is recommended that the organism should be reported as oxacillin (methicillin) resistant. 9 Of 6 isolates with no detectable mecA gene, 3 had cefoxitin zone diameters at the suggested breakpoint of 30 mm. The 3 remaining mecA gene PCR-negative isolates had cefoxitin zone diameters of 25 mm, 26 mm, and 29 mm, respectively. Mechanisms responsible for the apparent reduced susceptibility to cefoxitin in these 3 isolates are not known. Possible explanations might include possession of a novel mecA gene that was undetected by standard PCR assays, or an inducible type of resistance as has been observed in a Macrococcus-like organism. 13
A second retest of the 9 discordant isolates (by the same methods and from frozen stock cultures) resulted in mecA PCR results identical to those of the previous testing. Cefoxitin zone diameter of 1 mecA-negative isolate changed from 29 mm at previous testing to 37 mm (the smaller zone measurement probably reflects technical error because at initial testing this isolate’s cefoxitin zone diameter was 32 mm). A commercial latex agglutination test for PBP2a a was applied to the 9 isolates at final retest. Strong agglutination was observed only with those isolates in which mecA gene was detected by PCR. One mecA PCR-negative isolate with a cefoxitin zone diameter of 28 mm had a weak, equivocal agglutination reaction in the PBP2a assay. Thus, 8 isolates remained discordant.
The overall strong agreement between cefoxitin disk diffusion results and mecA gene detection by PCR is encouraging. The initial testing reported in the present study was performed on routine clinical isolates over multiple years, by multiple individuals and, in the case of species identification (phenotypic vs. molecular) and mecA gene detection (conventional vs. real time), by multiple methods. Both conventional and real-time PCR are valid methods for detection of the mecA gene; use of both for the current study reflects differences in test availability in the laboratory at the time of isolation. Establishment of S. pseudintermedius–specific cefoxitin disk diffusion interpretive criteria is an achievable goal. It is proposed from this study that an epidemiological breakpoint exists at a cefoxitin zone diameter of approximately 30 mm (≤30 mm = resistant). It is not known why a large percentage of isolates went from having discordant results initially to being in agreement on retest. Test result changes at retest that led to agreement were nearly equally distributed between the mecA PCR (56%) and cefoxitin zone diameters (44%). Of the isolates in which cefoxitin zone diameter changes resulted in agreement, 36% had initial cefoxitin zone diameters at the breakpoint (30 mm and 31 mm). With careful measurement of zone diameters and attention to standard testing procedures, it should be possible to increase the sensitivity and specificity of such a screening assay for detection of methicillin resistance. Interlaboratory test comparisons and additional testing with S. pseudintermedius isolates from different geographic regions and from different hosts are needed.
Footnotes
Acknowledgements
The authors thank Mary Jean Bryant, Brian Johnson, Rupal Brahmbhatt, and Anik Vasington for their technical assistance.
a.
Oxoid Penicillin Binding Protein (PBP2’) Latex Agglutination Test, Thermo Fisher Scientific, Pittsburg, PA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Center of Excellence in Livestock Diseases and Human Health, University of Tennessee.