
Abstract
An 18-month-old, female, spayed domestic ferret (Mustela putorius furo) was presented for progressive hind limb paresis of 1 week duration. The ferret was mentally appropriate but cachexic and ataxic with neurological deficits, which localized the lesion to the lumbosacral region. A depression in the lumbosacral spine was associated with discomfort on palpation. Results of whole body radiographs were consistent with an abnormal angle between vertebrae L6 and S1, which resulted in hyperflexion of the spine. The ferret was euthanized, and histopathological examination revealed an intramedullary lumbosacral teratoma effacing much of the spine in the region of the mass.
Teratomas are germ cell neoplasms derived from 2 or more of the totipotential cell lines (ectoderm, mesoderm, endoderm). 5 The gonads are the most common location for development of teratomas in human beings and animals; however, these tumors can also develop at extragonadal locations, usually along the midline axis of the body.5,13 Extragonadal teratomas have been infrequently reported in wild and domestic animals involving cutaneous structures, the alimentary tract, the kidneys, and retroperitoneal space, as well as other systems.2,8,15,21
Descriptions of teratomas of the central nervous system are rare in both human beings and animals. 17 Spinal teratomas in human beings are more common in pediatric patients, in whom they are typically observed in the sacrococcygeal region.10,11,17 These tumors tend to be cystic, extradural structures localized proximal to the sacrum. In contrast, teratomas of the spinal cord in adults are usually found in the thoracolumbar spine. 17 Intraspinal teratomas account for 3%–9% of all intraspinal tumors in children, and although it is not possible to determine their incidence in domestic animals, reports of these conditions are exceedingly rare. 4 A recent report described a cervical spinal cord teratoma in a Giant Schnauzer and summarized the literature on canine intraspinal teratomas. 25
In the ferret, teratomas have been described in the ovaries, uterus, and adrenal glands (Williams B: 1996, Bilateral adrenal teratomas in a domestic ferret (Mustela putorius furo). Vet Pathol 33:587. Abstract).3,19,24 The current report describes the clinical, radiographic, and microscopic features of an intramedullary teratoma in a domestic ferret.
An 18-month old, female, spayed domestic ferret (Mustela putorius furo) weighing 415 g presented to the University of Wisconsin, School of Veterinary Medicine (UWVMTH; Madison, Wisconsin) with a 2-week history of anorexia and lethargy. The ferret was fed a commercial ferret diet and lived in a large cage with 6 other ferrets. The owners reported that 1 week prior to presentation, the ferret seemed weak in the hind legs and could no longer climb. The ferret had been examined by the referring veterinarian (RDVM) 5 days prior to presentation for diarrhea, which coincided with the onset of hind limb paresis. The results of a plasma biochemistry panel determined by the RDVM were consistent with a mild hypoalbuminemia (2.6 g/dl, reference interval: 3.4–4.8 g/dl) and mild hyperglobulinemia (3.2 g/dl, reference interval: 0.2–2.4 g/dl). The results of a complete blood cell count (CBC) were unremarkable. The RDVM prescribed metronidazole (22 mg/kg orally every 12 hr) for the diarrhea. Despite medical therapy, there was no significant improvement in clinical signs, and the ataxia progressed.
On presentation to the UWVMTH, the ferret was alert and mentally appropriate but small for its age and cachexic (body condition score of 1.5/9), with pronounced generalized muscle wasting. The perineal skin was hyperemic and wet from urine scalding, and the anus was swollen. Both pelvic limbs were subjectively slightly cool to the touch. There were conscious proprioceptive deficits associated with both rear limbs and no purposeful hind leg movement as the ferret ambulated around the examination room. Superficial sensation was present in the left but not the right hind limb; however, no withdrawal reflexes were present in either hind limb. The remainder of neurological examination was unremarkable. During palpation of the spine, there was a 3–4-mm ventral depression over the lumbosacral junction, and gentle pressure in this area elicited discomfort. Results of abdominal palpation revealed a moderately distended urinary bladder, despite several episodes of urination during the examination. Other than moderate generalized dental tartar and mild gingivitis, no other physical examination abnormalities were observed.
The ferret was sedated with butorphanol a (0.25 mg/kg intramuscularly) and midazolam b (0.25 mg/kg intramuscularly) for additional diagnostics. A blood sample was collected from the cranial vena cava, and the only abnormality was hypoglycemia (57 mg/dl, reference range: 80–117 mg/dl), suggestive of either malnutrition or an insulinoma. A cystocentesis followed by urine dipstick analysis and cytology revealed trace red blood cells and a decreased urine-specific gravity (1.007, reference interval: 1.015–1.055). A fecal flotation and direct smear were negative for ova and parasites. Results of whole body radiographs demonstrated poor serosal detail attributable to the animal’s emaciation, an enlarged urinary bladder, and an abnormal angle between L6 and S1 resulting in hyperflexion of the spine (Fig. 1). A mild, generalized bronchial pattern was also observed in the lung fields. Physical examination findings led to a neurolocalization of L4-S3 myelopathy. Differential diagnoses included trauma resulting in L6-S1 instability, exacerbation of a congenital anomaly, degenerative myelopathy, infection, and neoplasia. To investigate these differentials, additional 3D imaging (computed tomography scan and magnetic resonance imaging) and cerebrospinal fluid analysis were recommended. However, due to the progressive nature of the signs and associated perineal trauma from urine and fecal matter scalding, severe cachexia despite dietary supplementation, and overall poor prognosis, the owners elected to euthanize the ferret. The ferret was placed under general anesthesia with isoflurane and euthanized by intravenous administration of pentobarbital. c
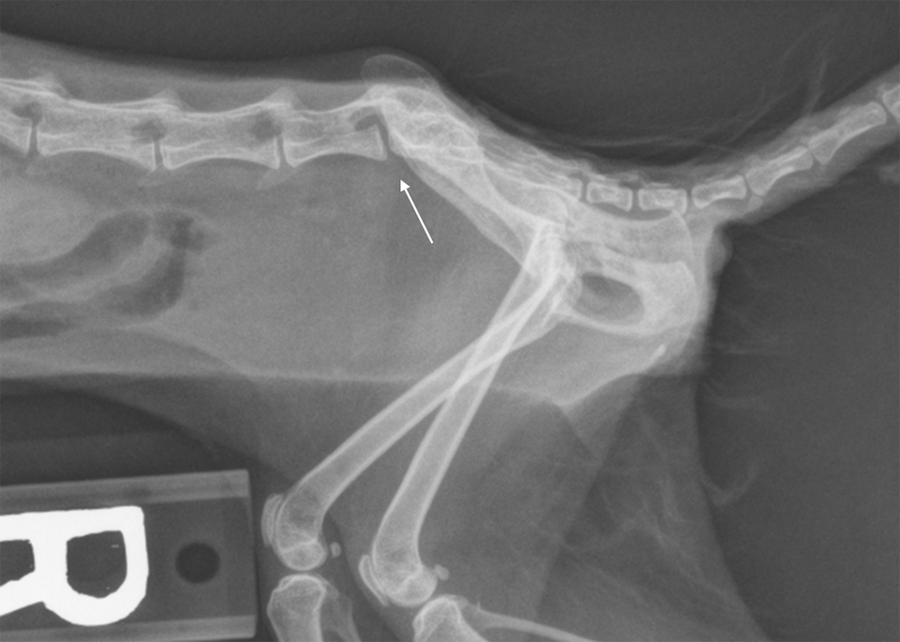
Domestic ferret (Mustela putorius furo). Lateral view of the lumbosacral spine. Arrow indicates the hyperflexion of the spine observed at L6-S1. An enlarged urinary bladder palpated on physical examination was not observed as this image was obtained after cystocentesis.
During the postmortem examination, significant findings included multifocal pulmonary and hepatic nodules and cardiomegaly. Due to small body size, the spine with cord was fixed and mildly decalcified in toto in a formic acid formalin solution d to preserve changes for histological evaluation. Remaining tissues were fixed in 10% buffered formalin and submitted for histopathological examination.
Histopathological results consisted of pulmonary congestion, atelectasis, and protein-rich edema in many alveoli, bronchioles, and some bronchi, which were consistent with pulmonary changes observed grossly. Lesions in the liver included mild lymphoplasmacytic portal inflammation, vascular congestion, and mild hepatocellular lipidosis. There was no evidence of neoplasia in either tissue. The myocardium had mild, multifocal myofiber size variation and necrosis confirming cardiomyopathy. No pathological changes were observed in any endocrine organs. The sciatic nerves and adjacent muscle and adipose tissue were also normal. The most striking changes were observed during examination of the lumbosacral spinal cord. On sagittal section of the sacrum, an unencapsulated mass was found within the cord. The mass replaced much of the normal tissue of the cord in this region. Derivatives of all 3 germ cell layers were observed at various sites within the mass (Fig. 2). Endoderm was represented by apocrine glands and mesoderm was represented by adipose tissue, vascular channels, collagenous connective tissue, cartilage, and bone, whereas ectoderm-derived tissues included hair follicles and keratinizing epithelium forming cyst-like spaces with occasional sebaceous glands. In addition, tubular structures lined with ciliated columnar epithelium and mucus-containing crypts were also observed, likely derived from endoderm. No morphological evidence of malignancy was present microscopically in any of the identifiable tissue types. The spinal cord and associated nerve roots in the affected area of the teratoma were markedly atrophic and peripheralized. The mass extended to all but the caudal-most section of the lumbar spine, which was free of neoplastic material.
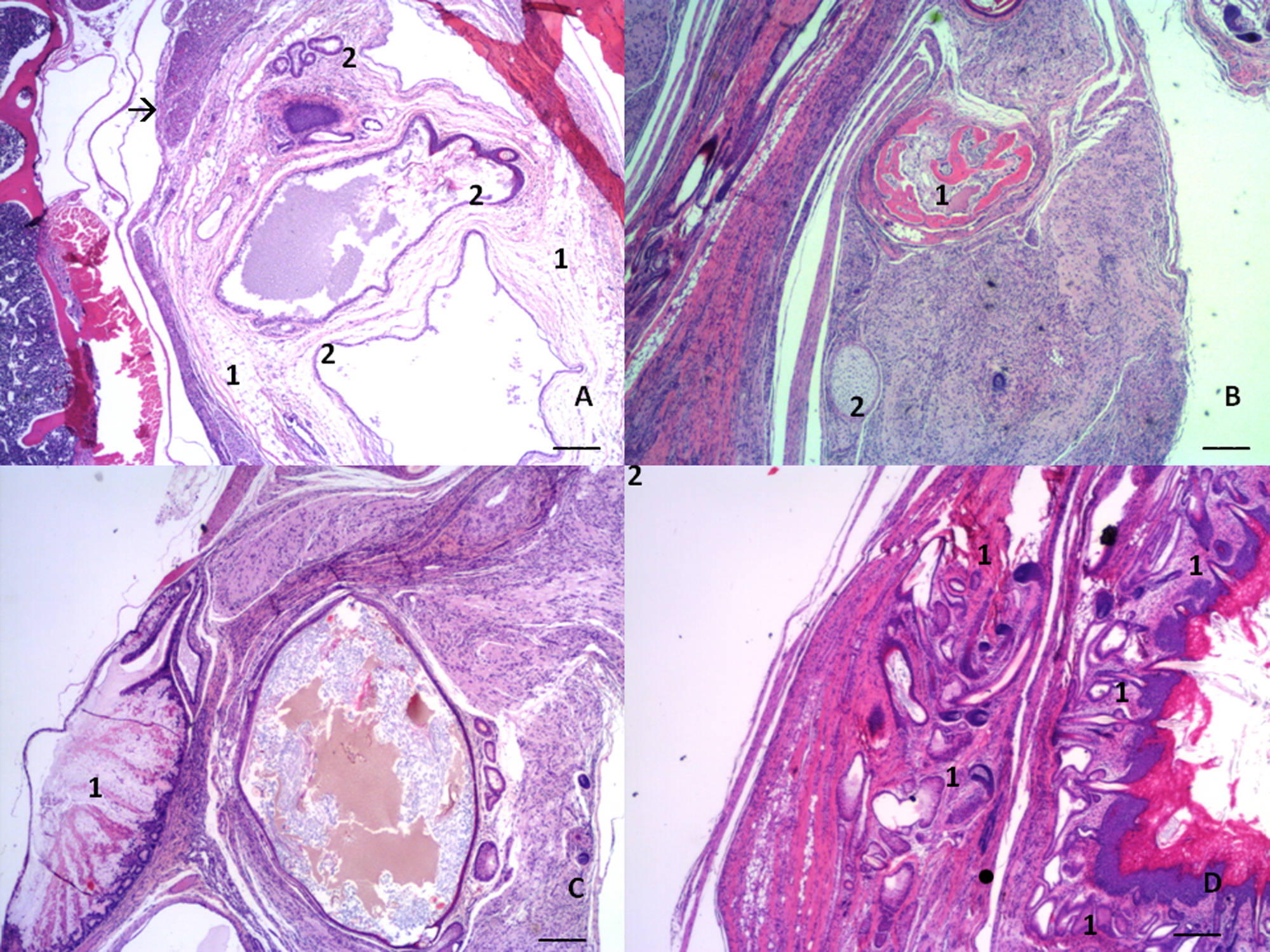
Domestic ferret (Mustela putorius furo). Intramedullary teratoma. Hematoxylin and eosin stain. Bar = 1,000 µm.
The incidence of neoplasia in the pet ferret was once thought to be lower than in other companion animals; however, the prevalence of neoplastic diseases in domestic ferrets appears to be similar to that of other household pets. 7 The most common tumors in ferrets are insulinoma, adrenocortical neoplasms, and lymphoma, although those derived from endocrine tissue are more prevalent than other types. 22 Chordomas are the most frequent spinal tumor in ferrets.6,9 Chordomas are derived from notochord (mesoderm) and, in ferrets, tend to localize to the distal tail, although these tumors have been seen in the cervical and thoracic regions.6,9,18
Thus far, reports of teratomas in ferrets have been limited to the reproductive system and the adrenal glands (Williams B: 1996, Bilateral adrenal teratomas).3,19,24 The origin of teratomas remains controversial. The traditional theory holds that teratomas are derived from rests of primitive germ cells from the yolk sac, which have aberrantly migrated and developed into germ cell tumors. The alternative dysembryogenic theory suggests that teratomas may originate from undifferentiated mesenchymal cells present in the developing primitive streak of embryos that undergo mutations or abnormal development under inappropriate inductive signaling. The latter theory is supported by the fact that in human beings, teratomas have often been found in association with other myelodysplastic disorders, such as spina bifida. 12 In the case of the ferret presented herein, no congenital defects were observed in association with the tumor.
Most descriptions of teratomas in the veterinary literature are of benign tumors, although malignant tumors are also reported.2,16 A malignant teratoma is one in which non–germ cell tissue has transformed, and typical characteristics of malignancy are then observed in the area of transformation. 20 In people, intramedullary tumors tend to be benign, 23 and this was true for the teratoma reported herein. Although complete surgical resection of intramedullary tumors in human patients tends to be associated with good outcomes and low recurrence rates, it is unlikely that the tumor in the ferret in the present study could have been resected completely given the lack of a tumor capsule and the large size of the tumor.
Hind limb paresis can be a nonspecific sign of both infectious and noninfectious disease in ferrets, and for the ferret in the current study, trauma, metabolic disease, intervertebral disc disease, fibrocartilaginous embolus, and metastatic or primary neoplasia were considered appropriate differential diagnoses.1,14 Although undoubtedly rare, a differential diagnosis of spinal teratoma should be considered by clinicians when dealing with a ferret presenting with paresis or paralysis.
Footnotes
a.
Butorphanol tartrate, Hospira Inc., Lake Forest, IL.
b.
Midazolam hydrochloride, Hospira Inc., Lake Forest, IL.
c.
Beuthanasia®-D Special, Intervet-Schering, Union, NJ.
d.
Formical–4™, Decal Chemical Corp., Tallman, NY.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.