
Abstract
A 2-year-old, spayed female Vietnamese potbellied pig (Sus scrofa) was evaluated due to polyuria, polydipsia, lethargy, and hyporexia. The pig was obese, and a large abdominal mass was palpated. Additional findings included hypercalcemia, hyperglycemia, glucosuria, and an inflammatory leukogram. At surgery, the abdominal mass was biopsied and found to be bilaterally symmetric adipose tissue with mineralization and granulomatous steatitis. An additional surgery was performed to collect additional diagnostic samples, but the pig died while recovering from anesthesia. A cosmetic necropsy was performed, and lipid emboli were identified microscopically in various tissues. The presence of lipid emboli in the lung and kidney was supported by antifibrinogen immunohistochemistry. Obesity is a common finding in potbellied pigs; however, mineralization and saponification of fat are uncommon, particularly the bilateral symmetrical distribution found in the abdomen of the present case. This may present as a single intra-abdominal mass complicating diagnostic interpretation. Whether mineralization and saponification of fat facilitate the development of fat embolism is undetermined. Lipid emboli should be considered in obese pigs undergoing medical or surgical procedures. Factors that may predispose to the development of fat embolism, such as excessive handling or bruising of fat stores, should be avoided.
A 2-year-old, spayed female Vietnamese potbellied pig (Sus scrofa) with a body condition score of 6 out of 6 and a weight of approximately 113 kg presented for polyuria and polydipsia. There was mild abdominal distention, and the abdomen felt very firm on palpation. The owner also reported lethargy and hyporexia of several weeks’ duration. On presentation, the pig could ambulate normally; body temperature, respiratory rate, and heart rate were within normal limits. The pig was sedated to facilitate thorough physical examination and blood collection for chemistry and cell counts. The most pronounced abnormalities were hypercalcemia (14 mg/dl; normal mean and standard deviation for large white pigs is 11.6 ± 0.8 mg/dl) and hyperglycemia (163 mg/dl; normal mean and standard deviation for large white pigs is 79.3 ± 18.0 mg/dl). 18 There was also an inflammatory leukogram: total leukocytes 23.2 × 103/µl (average 16.4 × 103, minimum 11.6 × 103, maximum 21.0 × 103); neutrophils 70% (average 36%, minimum 28%, maximum 42%); bands 19% (average 0.7%, minimum 0%, maximum 2.0%); lymphocytes 8% (average 54%, minimum 38%, maximum 61%); and monocytes 2% (average 5%, minimum 0%, maximum 9.0%). 17 Upon physical exam, a single large, firm mass approximately 10 cm in diameter was palpated in the caudoventral abdomen. On ultrasound, the mass was well encapsulated and heterogeneous in consistency, with irregular areas of hyperechoic and hypoechoic texture and no obvious vascular component. It was unclear at the time whether the mass was intra-abdominal or extra-abdominal. Radiographs showed a large opacity in the caudal abdomen that displaced the urinary bladder caudoventrally. The opacity was consistent with normal fatty tissue or, less likely, an invasive lipoma or liposarcoma. An exploratory laparotomy revealed the presence of 2 bilateral symmetrical retroperitoneal masses instead of a single mass. Based on intraoperative palpation of these masses and their location, a presumptive diagnosis of mineralized fat deposits and granulomatous steatitis was made, which was confirmed histologically.
Radiographs also revealed lucent areas associated with the cranial vertebral bodies of lumbar vertebrae L4 to L6 and possibly the cranial physis of L4 with mild sclerosis of these areas. The caudal margin of the L7 vertebral body was irregular and also contained focal areas of increased lucency. A preliminary diagnosis of osteomyelitis of the vertebrae was made and thought to be secondary to an infectious disease or, less likely, a metastatic process. Urine culture and brucellosis testing, as well as aspiration of the vertebral lesions under computed tomography guidance, were carried out, and all tests yielded negative results. Urine collected by cystocentesis during surgery had increased levels of glucose (250 mg/dl). A tentative diagnosis of diabetes mellitus was made based upon the concurrent hyperglycemia, glucosuria, and the clinical signs of polyuria, polydipsia, lethargy, and inappetence. However, both the hyperglycemia and glucosuria were within normal ranges the following day. The new working diagnosis was psychogenic polydipsia or nephrogenic diabetes insipidus. A 12-hr water deprivation test showed adequate urine concentration; therefore, psychogenic polydipsia was not eliminated but was regarded as unlikely. Serum parathyroid hormone and its related peptide levels were examined to help identify the cause of the hypercalcemia; both were undetectable, ruling out primary hyperparathyroidism. The pig was anesthetized again for gastroscopy and for a percutaneous liver biopsy but died during recovery from anesthesia and was thereafter submitted for a cosmetic necropsy.
On gross examination, there were multifocal to coalescing, firm, red, well-demarcated areas composing approximately 60% of the lung parenchyma (Fig. 1). The abdomen contained approximately 2 liters of dark red fluid with lipid droplets and clotted blood. Mesenteric and visceral fat was diffusely white, opaque, firm, and nodular. The liver was diffusely tan-brown and friable. On the caudal surface of the right medial lobe was a 5 mm in diameter, depressed area with hemorrhage (presumed biopsy site). Given the cosmetic nature of the necropsy, the brain was not examined, and the parathyroid glands were not identified.

Lung, pig. Gross appearance of the lungs. There are multifocal, well-demarcated, firm, red areas.
On microscopic evaluation, alveolar septa throughout the lung were multifocally expanded by aggregates of large, round, variably sized (25–100 µm), clear vacuoles (lipid droplets; Fig. 2A–2C). In grossly affected areas, there were multifocal, large, well-demarcated areas where alveoli and bronchi contained red blood cells, smooth pale eosinophilic material (edema fluid), and dense fibrillar eosinophilic material (fibrin). In addition, there were increased numbers of alveolar macrophages. There was widespread, multifocal (lobular) thickening of the alveolar septa by type 2 pneumocyte proliferation, early fibroplasia, and macrophages. Although in most bronchi the epithelium was intact, in some areas the bronchial epithelium was ulcerated and replaced with fibrin and erythrocytes. In some medium-sized arteries, the endothelial cells were plump (hypertrophy) and present in increased numbers (hyperplasia).
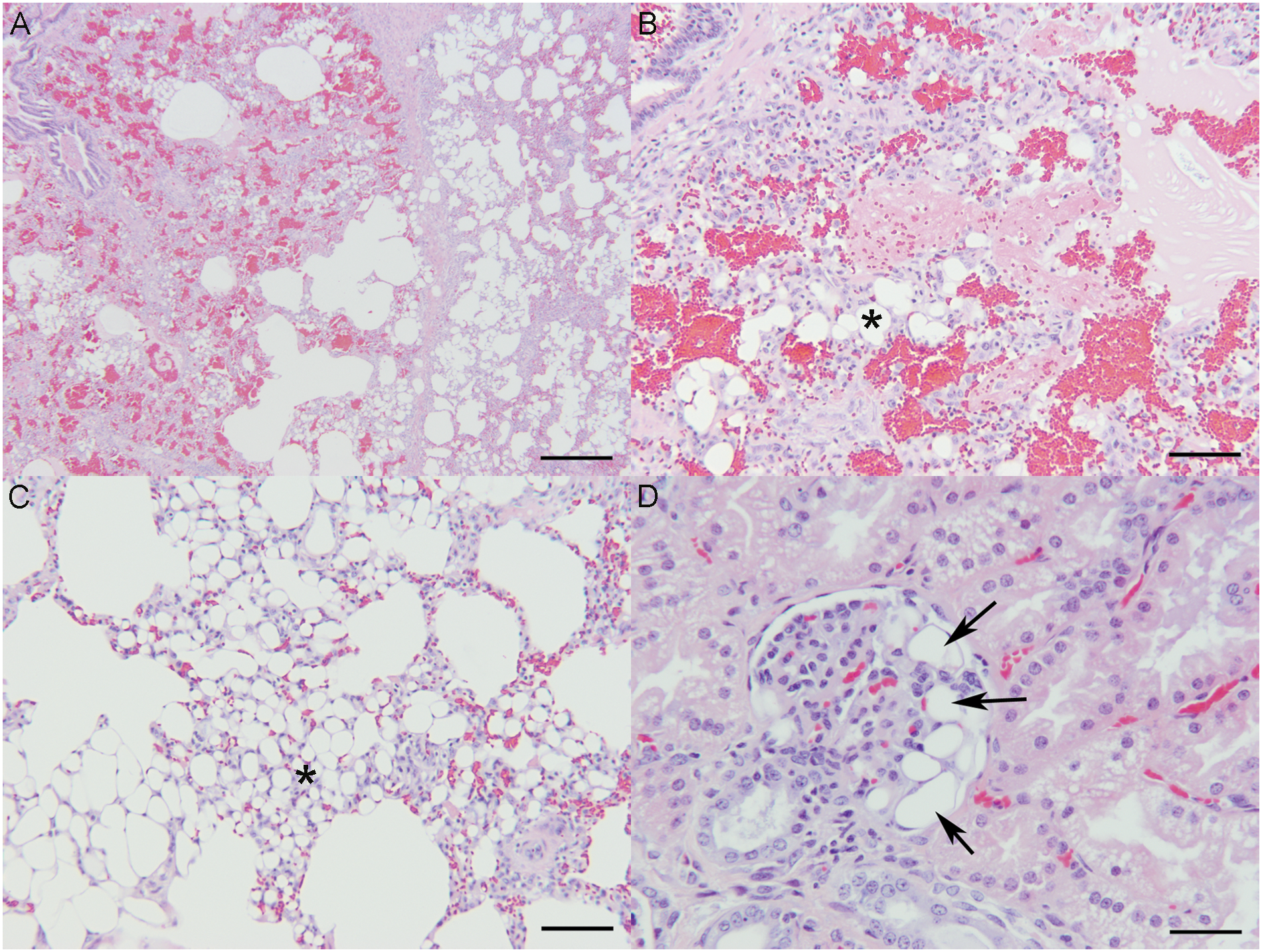
In the kidney, glomerular capillary loops were rarely expanded by variably sized, clear lipid droplets; there was no accompanying hemorrhage, inflammation, or necrosis (Fig. 2D). Other renal changes included mild tubular degeneration, mineralization, and lymphocytic interstitial nephritis. The liver had moderate centrilobular hepatic lipidosis. Rarely, intrahepatic blood vessels contained well-demarcated, variably sized lipid droplets. In the abdominal fat, adipocytes were frequently surrounded by epithelioid macrophages and multinucleated giant cells (granulomatous steatitis). Adipocyte nuclei were frequently absent (necrosis). Within the fat there were multifocal small areas of hemorrhage and mineralization. Dissecting throughout the adipose tissue were interconnecting bands of fibrous connective tissue. The vertebral lesion noted clinically was histologically consistent with osteochondrosis, and there was no evidence of osteomyelitis.
Since no unprocessed tissue was available for Sudan black or oil red O staining to confirm the presence of lipid, immunohistochemistry was performed on formalin-fixed, paraffin-embedded sections of lung and kidney using an antifibrinogen antibody. This immunohistochemical technique to identify lipid emboli has recently been validated in the human literature as a way to confirm lipid emboli in the absence of fresh or formalin-fixed tissues. The principle used in this technique is that when formed, lipid emboli, due to their potent procoagulant and prothrombotic potential, rapidly become covered with platelets, fibrin, and other blood cellular elements. Although the lipid is lost in the routine processing required for paraffin embedding, the adsorbed fibrinogen surrounding the lipid droplet remains intact and is highlighted by the antifibrinogen antibody. 9 Paraffin-embedded sections were covered with 3-aminopropyl-triethoxysilane, a and then a pretreatment was performed (incubation in a proteinase K for 15 min at 20°C) to facilitate antigen retrieval and to increase membrane permeability to the antibody. The primary antibody b was diluted 1:3,000 and incubated for 120 min at 20°C. The detection system used was the labeled streptavidin–biotin kit, c a refined avidin–biotin technique in which a biotinylated secondary antibody reacts with several peroxidase-conjugated streptavidin molecules. The positive reaction was visualized by 3,3′-diaminobenzidine peroxidation, according to standard methods. Then, the sections were counterstained with Mayer hematoxylin, dehydrated, cover slipped, and observed under optical and confocal laser scanning microscopes. Positive controls were human tissues from the previous publication (data not shown). 9 An unrelated Vietnamese potbellied pig that was euthanized due to a hepatocellular carcinoma and a tooth root abscess was used as a negative control (Fig. 3A). Examination of tissues from the current case revealed large amounts of fibrinogen surrounding large lipid droplets (empty spaces) in pulmonary arteries and glomerular capillaries (Fig. 3B, 3C). According to the current histological methods used for grading lipid embolism in pulmonary tissue, the quantitative classification was grade 4 (massive embolism) according to Sevitt 13 or grade 3 (moderate embolism) according to Turillazzi et al. 19

During the initial diagnostic workup, which included abdominal palpation, ultrasound, and radiographs, the firm, somewhat distended abdomen appeared to result from a single mass; neoplasia was suspected. The hypercalcemia found on blood work was interpreted as further evidence for abdominal neoplasia, which prompted the decision for surgical intervention. At surgery, it was discovered that what appeared to be a single mass was actually 2 retroperitoneal areas of mineralized and saponified fat. Although this particular distribution of mineralized fat seems to be uncommon in pigs (medical records, College of Veterinary Medicine, University of Tennessee, Knoxville, Tennessee), mineralized fat should be considered as a differential for abdominal masses in obese pigs.
The cause of the hypercalcemia was not definitively determined, but because granulomatous inflammation can result in hypercalcemia, it was most likely secondary to the granulomatous steatitis. 6 Hypercalcemia was the most likely cause of the polyuria and polydipsia. 2 Undetectable levels of serum parathyroid hormone and its related peptide ruled out hyperparathyroidism.
Conditions that predispose to lipid embolism typically produce discontinuities in the walls of blood vessels, with concurrent adjacent liquid lipid deposits and increased pressure in the surrounding tissues; this combination of events can force lipids into the vascular system. 10 The most common cause of lipid embolism in human beings is bone trauma (injury or surgery related). Lipid embolism is rare in animals and can originate either from bone marrow, as a result of fractures, or from rupture of hepatocytes in cases of severe hepatic lipidosis. 4 Naturally occurring lipid emboli in dogs have been related to total hip replacement surgeries.8,16 In cats, fatal pulmonary lipid embolism has been reported as a result of subcutaneous trauma and during a humeral fracture repair.12,14
Nontraumatic causes of lipid embolism in human beings typically involve fat or bone marrow necrosis (osteomyelitis, pancreatitis, panniculitis, or hepatic lipidosis) and are rarely drug related or iatrogenic (procedure related). 1 Yellow fat disease or nutritional panniculitis is a well-described disease in many species, particularly young horses or ponies. In such cases, a deficiency of vitamin E or the intake of high levels of polyunsaturated fatty acids may play a role. 15 Although the levels of polyunsaturated fatty acids in the diet of the pig in the current study are unknown, based on the dietary information available, it is unlikely that vitamin E deficiency played a role. Furthermore, histologically, nutritional panniculitis is associated with ceroid pigment; no ceroid was present in the current case. 7 In human beings, diabetes mellitus is also associated with lipid emboli. 10 Due to the hyperglycemia and glucosuria noted on initial presentation, diabetes mellitus had been a clinical concern in the current case but was ruled out after additional diagnostics.
Lipid emboli tend to lodge in the capillaries of the brain and lung (obstructive phase), which can result in organ dysfunction or can incite an inflammatory response. One study using pigs induced lipid embolization by retransfusing blood shed during a cardiac bypass procedure; by simultaneously introducing a radioactive marker, this group was able to quantitate the localization of the lipid emboli. That study found the highest levels of radioactivity, and therefore lipid emboli, in the kidney and spleen, with lesser amounts localizing to the lungs, brain, heart, small intestines, and skeletal muscle. 3 In the current case, the majority of the lipid emboli were seen in the lungs; the difference in distribution may be related to the differing pathogeneses of the lipid embolization.
The cause of the lipid emboli in the current case is unclear but could be related to marked fat necrosis, hepatic lipidosis, the exploratory celiotomy or computed tomography–guided bone aspirate 3 weeks previously, or the percutaneous hepatic biopsy performed just prior to death. The duration of the lesions was estimated to be 5–7 days. In human beings, the delay between the inciting event and development of respiratory symptoms (in the case of pulmonary emboli) varies from 36 hr to 3 weeks. 9 In canine studies, pulmonary and systemic lipid embolization can be induced by femoral and tibial canal reaming and pressurization in dogs.5,11 These studies found intravascular lipid in the lungs, brain, and kidneys. In both of these canine studies, less than 1% of the lung was affected by the lipid emboli, which is equivalent to a grade 1 (sporadic presence of emboli) 19 ; at 8 and 72 hr, there was minimal to no evidence of pulmonary edema, inflammation, or hyaline membranes.5,11
The inflammatory response to lipid emboli is thought to be initiated via the action of endothelial lipases that act on the lipid emboli, releasing free fatty acids. Increased serum lipase concentrations are present in human beings with lipid emboli 10 but were not measured in the pig in the present study. The free fatty acids released by the lipases act as toxic intermediates (toxic phase), which damage pneumocytes, cause increased pulmonary endothelial cell permeability, and incite inflammation. Subsequent activation of the coagulation cascade and fibrinolysis can result in disseminated intravascular coagulation and, thus, exacerbate the lung injury. The resulting lung injuries can then progress to acute respiratory distress syndrome 1 and severe hypoxemia. The changes seen in the lung of the current case are all attributable to acute respiratory distress syndrome, 4 and such events likely contributed to the anesthetic death of the pig. There were no signs of respiratory disease on presentation or at any time prior to the anesthetic death. The respiratory rate was normal, and no coughing or nasal discharge was detected. The pig had been housed alone and had no contact with other pigs, making transmissible respiratory diseases less likely.
The obstructive phase of the pulmonary microembolism is also mechanical and can result in pulmonary hypertension, increased afterload of the right heart, and, ultimately, acute right heart failure. 10 This may have also contributed to the acute death of the pig while under anesthesia. The gross findings of an abdominal effusion and centrilobular hepatic lipidosis may support this theory; however, marked centrilobular sinusoidal congestion (acute passive hepatic congestion) was absent.
Although disseminated intravascular coagulation is not specifically associated with lipid emboli, a consumptive coagulopathy with subsequent thrombocytopenia and generalized petechial hemorrhages are diagnostic features of lipid emboli. 10 Such changes were not present in the pig in the current report at necropsy or clinically.
Treatment of pulmonary lipid embolism in human beings consists of high doses of intravenous steroids, to counteract the toxic effects of the free fatty acids, and oxygen in the form of positive pressure ventilation. In cases where a long bone fracture is the inciting cause, immediate application of a tourniquet proximal to the fracture may prevent emboli from entering into the general circulation. 10
Obesity is a common finding in potbellied pigs; however, mineralization and saponification of fat seem uncommon (S. R. VanAmstel, personal observation, 2011), particularly the bilateral symmetrical distribution found in the current case. This fat may present as a single intra-abdominal mass complicating diagnostic interpretation. The mineralization and saponification of fat may facilitate the development of lipid emboli. Lipid emboli should be considered in obese pigs undergoing medical or surgical procedures.
Footnotes
Acknowledgements
The authors thank Misty Bailey for critical review of the manuscript.
a.
3-aminopropyl-triethoxysilane, Fluka, Buchs, Switzerland.
b.
Anti-fibrinogen antibody, Dako, Copenhagen, Denmark.
c.
LSAB+ kit, Dako, Copenhagen, Denmark.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.