
Abstract
A newborn male Romagnola calf, who had died a few hours after birth, was submitted for postmortem examination. Necropsy revealed a 23 cm × 22 cm × 5 cm, pale pink, lobulated, elastic, partially fluctuant mass that protruded from the dorsal retroperitoneal space into the abdominal cavity, extending from the diaphragm to the left kidney. The mass consisted of mature pulmonary tissue and was consistent with a pulmonary choristoma. The gross and microscopic appearance of this rare tumor-like congenital lesion and the possible pathogenesis are discussed.
A newborn male Romagnola calf, who had died a few hours after birth, underwent necropsy as part of the surveillance program for the so-called “congenital paunch calf syndrome.” 15 However, the lack of skeletal malformations, ascites, and liver lesions excluded this diagnosis at the initial postmortem examination.
Necropsy showed a 23 cm × 22 cm × 5 cm, pale pink, lobulated, elastic, partially fluctuant mass that protruded from the dorsal retroperitoneal space into the abdominal cavity, extending from the diaphragm to the left kidney (Fig. 1). The mass was surrounded by a thick, white fibrous wall. It was adjacent to the renal fascia caudally and to the splenic capsule cranioventrally, slightly to the left. There were no adhesions, and the mass was not contiguous with any other abdominal organs or structures.
Incision of the wall revealed that the mass did not have any parenchymal continuity with the kidney or the adrenal gland. On cut section, the parenchyma had a soft, elastic consistency. The cut surface was lobulated and pale pink. A cystic cavity 5 cm in diameter, containing a red—brown fluid, was present in the mass (Fig. 2). The total weight of the mass was 1.8 kg.
On the basis of the above-mentioned findings, the mass was thought to be an embryonal neoplasm (i.e., nephroblastoma) with the gross appearance of pulmonary tissue but without any apparent communication with the lungs. Representative samples from the mass were collected, fixed in 10% buffered formalin, embedded in paraffin, and routinely processed for histologic examination. Five-micron sections stained with hematoxylin and eosin revealed normal pulmonary architecture and structures (Fig. 3). Alveoli were dilated, but there was no evidence of protein-rich liquid within. Bronchioles were lined with a single layer of cuboidal and ciliated respiratory epithelium and were surrounded by smooth muscle fibers. There was no evidence of bronchi or cartilaginous rings. The interstitium consisted of connective tissue septa and blood vessels. On the basis of its microscopic appearance, the abdominal mass was diagnosed as a pulmonary choristoma.
A choristoma is a rare congenital tumor-like lesion reported in human beings and other animal species consisting of histologically normal mature tissue located in an anatomic position different from its proper site. 9 A pulmonary choristoma is a solitary nonfunctioning mass of pulmonary tissue 7,9,10,14 that is composed of normal lung parenchyma but lacks communication with the tracheobronchial tree. It receives its arterial supply from the systemic circulation. 5,7,13
In the literature, it is also reported as an ectopic or accessory lung, 2,5,7,11–13 bronchopulmonary foregut malformation, 7 and extralobar pulmonary sequestration. 1,5,7,10,14 In contrast, the term intralobar pulmonary sequestration is used to indicate a nonfunctioning mass of lung tissue located within a normal lobe and lacking its own visceral pleura. 5,10,14 Bronchogenic cysts represent supernumerary lung buds from the primitive foregut, but in contrast to sequestrations, the cysts only rarely contain distal lung parenchyma. 6
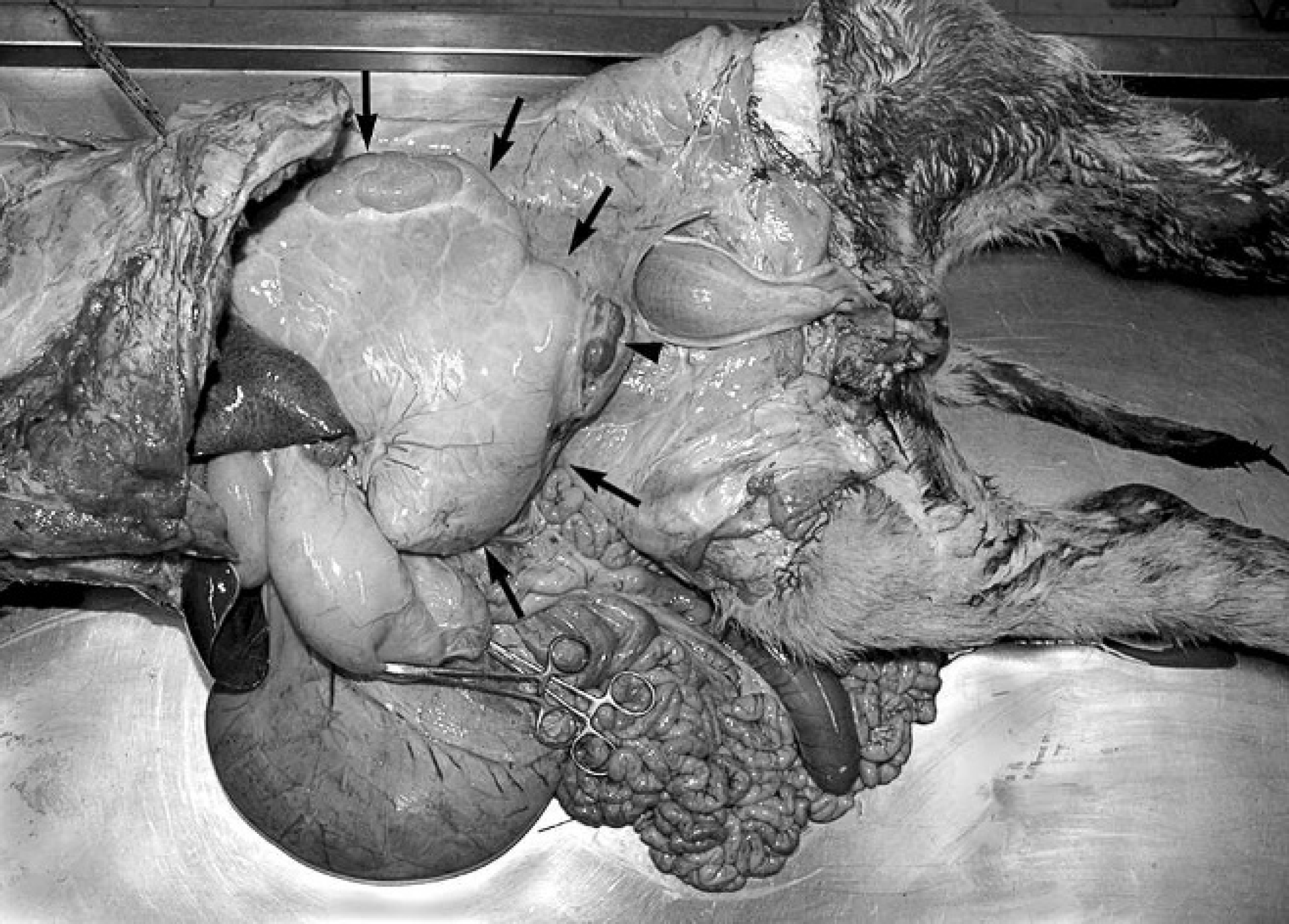
Abdominal cavity of the calf. Note the pulmonary choristoma (arrows) extending from the retroperitoneal region. The arrowhead indicates the kidney after incision of the choristoma wall.
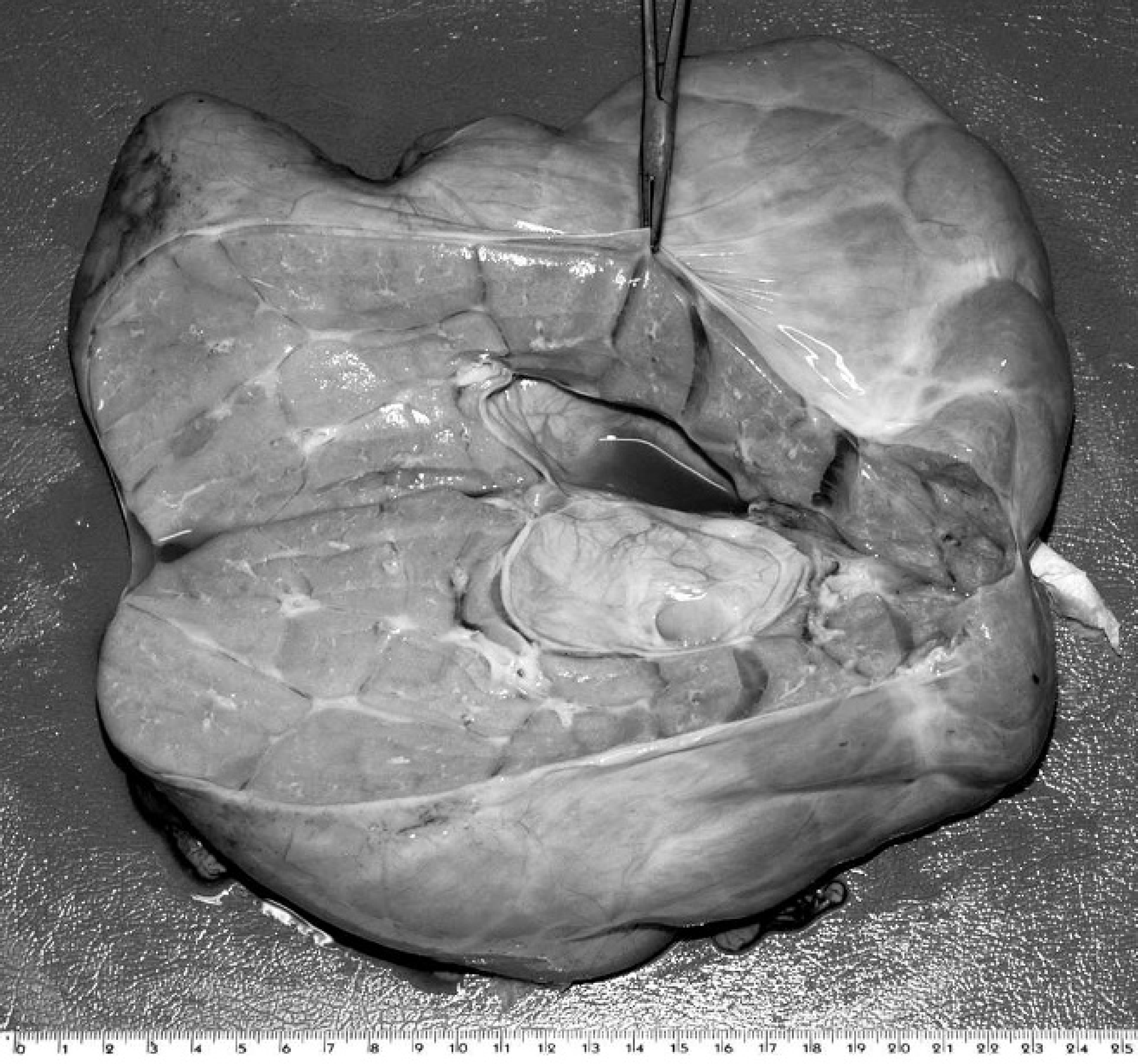
Pulmonary choristoma. Note the lobulated cut surface with a central cystic cavity.
Choristomas can be located in the thoracic cavity (in which case it is separate from the adjacent normal tissue of the lung), the diaphragm, the retroperitoneal and adrenal gland regions, or the subcutaneous tissue. In all these cases, the mass is covered by a distinct pleura. Choristomas occasionally communicate with the digestive tract, usually the esophagus. 7,10
The content of the dilated alveoli is presumed to be entrapped fetal lung fluid. Physiologically, the fetal lung fluid produced by the lung epithelium moves from the potential air spaces to the upper airways, where it is either swallowed or released into the amniotic fluid. 4 The lack of communication with the tracheobronchial structures would have prevented the removal of this liquid. As reported in the literature, the composition of normal fetal lung fluid, high in chloride and almost protein free, 17 could explain its lack of affinity for hematoxylin and eosin stain. In the authors' opinion, the fluid in the cystic cavity likely has the same origin as that in the alveoli.
To the authors' knowledge, pulmonary choristomas have been reported in cattle in the subcutaneous tissue at the level of the frontal region of the skull, 11,13 the zone extending from the occipital bone to the first cervical vertebra, 3 the midline of the lower cervical area, 2 the neck, 12 the shoulders, 16 and the right side of the chest. 1 The abdominal cavity is another location that has been reported. 1,16
A choristoma is believed to be a malformation of the embryonal foregut. The most accepted theory states that an accessory lung bud develops from the caudal aspect of the primitive foregut and migrates caudally along the growing esophagus. 2,6–8,11,12 If this accessory lung bud arises early in embryonic life, before the development of the pleura, it is enclosed within an adjacent lung and becomes an intralobar sequestration; if instead this accessory lung bud develops later, when the pleura has already formed, it grows separately from the adjacent lung, is covered with its own pleura, and forms an extralobar sequestration. 7 Therefore, the type of bronchopulmonary foregut malformation depends on the stage of embryologic development at which the accessory tissue arises and the direction in which the aberrant pulmonary tissue grows. 6
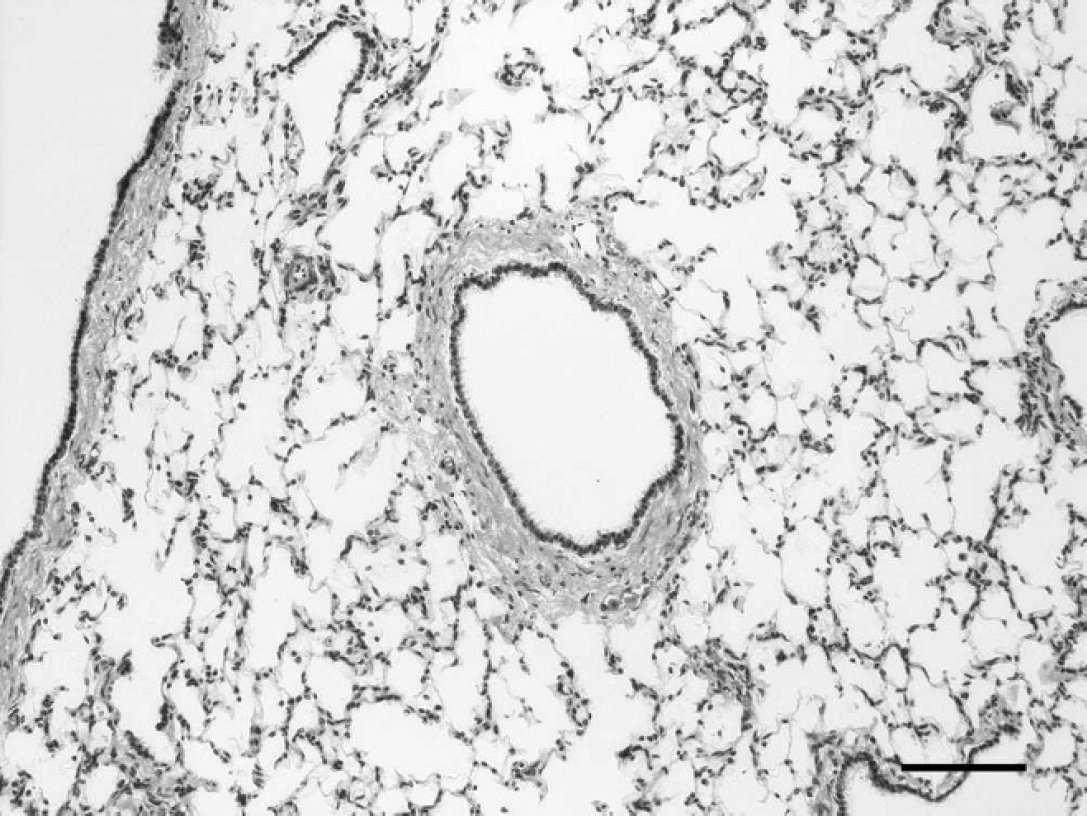
Pulmonary choristoma. Note the alveoli and a central bronchiole lined with ciliated respiratory epithelium. Hematoxylin and eosin. Bar = 100 μm.
Other authors hypothesize that a choristoma originates from ectopic pluripotential cells that develop in the direction of the respiratory tissue. 3,15,18 Another hypothesis suggests that a supernumerary tracheobronchial tube is formed directly from the primitive foregut of the embryo, cranially or caudally to the origin of the normal tracheobronchial tube. 16
Prognosis depends on the location of the choristoma; it is favorable in the case of a subcutaneous location because it can easily be removed surgically. 2,3,13
Theoretically, the diagnosis of a choristoma might be reached antemortem using ultrasonographic techniques, computed tomography, or magnetic resonance imaging, but to the authors' knowledge, there have been no such reports in bovine medicine. The in vivo imaging diagnostics in the bovine cases reported until now are limited to radiologic examinations. 2,3,11,13 However, a final diagnosis can be confirmed only by histopathologic examination. The present case of a pulmonary choristoma located in the retroperitoneal region is thought to add useful knowledge to the existing information available regarding bovine species.