
Abstract
A 12-year-old spayed female Siberian husky dog presented with hematuria and weight loss. An abdominal ultrasonographic examination revealed a left renal tumor measuring 8 cm in diameter, and a nephrectomy was performed. The resected kidney contained a cavitated tumor with a white solid region. Histologically, this tumor was composed of large polygonal cells with abundant and cloudy cytoplasm and focal sarcomatoid change. The neoplastic epithelial cells were reactive with colloidal iron staining; Dolichos biflorus agglutinin, peanut agglutinin, and Ulex europaeus agglutinin I lectins; and cluster of differentiation 10 and c-KIT antigens but not for periodic acid-Schiff or vimentin stain. Neoplastic sarcomatoid cells stained positive for vimentin. Because these histopathologic features are identical to those of human chromophobe renal cell carcinoma, the present case was diagnosed as canine chromophobe renal cell carcinoma.
In dogs, primary renal tumors are uncommon. The prevalence of primary renal neoplasia is estimated to be 0.3-1.5% of all the canine neoplasms. 13 The most common histologic type of renal tumor is renal cell carcinoma (RCC). Although RCCs in dogs have been classified previously as several subtypes, based on their histologic (papillary, tubular, and solid type) and cytologic (chromophobic, eosinophilic, and clear cell type) patterns, the differences in the biologic behaviors of these subtypes remain to be elucidated. 12 Human RCCs are classified as clear cell, papillary, chromophobe, and collecting duct carcinoma based on the histopathology and molecular biologic properties. 17
Chromophobe RCC accounts for approximately 5–8% of human RCCs and has a better prognosis than other subtypes. 14,15 A 1974 study first described RCC as a chemically inducible tumor in rats, caused by nitrosomorpholine. 2 Subsequently, the first chromophobe RCC in humans, composed of tumor cells with cloudy, weakly eosinophilic and reticular cytoplasm, was reported. 18 Human chromophobe RCC and renal oncocytoma are intimately related 3,5,14 ; however, oncocytomas have been reported in dogs. 4,6,19 In the present study, a canine renal neoplasm with characteristic histopathologic, histochemical, and immunohistochemical features similar to the human chromophobe RCC is described.
A 12-year-old spayed female Siberian husky dog was referred to a veterinary hospital with hematuria and weight loss. Urinalysis revealed hematuria, proteinuria, and increased numbers of leukocytes. A hematologic examination indicated hypercalcemia (14.9 mg/dl; reference interval: 9.3-12.1 mg/dl) and anemia; however, there was no azotemia. An abdominal ultrasonographic examination revealed a mass in the left kidney measuring 8 cm in diameter. In spite of left radical nephrectomy, the dog progressively lost weight, developed anorexia, and died 3 months after surgery. A necropsy was not permitted.
The resected kidney had been immediately fixed in 10% neutral buffered formalin solution, and selected tissue sections were processed, embedded in paraffin, and cut into 4-μm-thick sections for histologic examination. The sections were stained with hematoxylin and eosin, periodic acid-Schiff (PAS), and Hale colloidal iron. For further characterization of the tumor cells, lectin histochemistry and immunohistochemistry were performed using serial paraffin sections, as previously reported. 9
Tissue sections used in lectin histochemistry were incubated with biotinylated lectins at room temperature for 3 hr. The following lectins were used: Dolichos biflorus agglutinin a (DBA, 1:100), peanut agglutinin 1 (PNA, 1:100), and Ulex europaeus agglutinin I a (UEA-I, 1:100). The adsorbed lectins were detected by incubation with peroxidase-conjugated streptavidin, followed by 3,3′-diaminobenzidine (DAB) chromogen reaction.
The following primary antibodies were used for immunohistochemical stains: anti-cluster of differentiation (CD)10 b (1:50, clone 56C6), anti-c-KIT c (1:50, polyclonal), and anti-vimentin c (1:100, clone V9). The labeled antigens were detected using the streptavidin-biotin method with a commercial kit, d followed by DAB. Samples from radical nephrectomy were processed in an identical manner and used to compare the reactivity of neoplastic cells with nonneoplastic renal tissue.
The resected kidney showed a bulging, 8 cm in diameter, cavitated gray-white mass filled with a dark brown fluid at its caudal pole and extended from the medulla to the cortex. Histologically, the tumor was composed of solid cellular sheets with occasional glandular spaces, separated by a desmoplastic stroma. Hemorrhage and necrosis were observed, and the vascular density was low. The neoplastic epithelial cells had a large polygonal appearance with an abundant and cloudy eosinophilic cytoplasm (Fig. 1). Tumor cell nuclei were variable in size, ranging from an irregular to an oval shape with occasional multinucleated cells. Foci of sarcomatoid change were characterized by spindle-shaped cells arranged in interlacing bundles (Fig. 2).
Reactivities of differentiation markers compared with human RCCs and normal canine kidney are summarized in Table 1. In the normal kidney, reactive PAS staining was limited to glomerular and tubular basement membranes, and colloidal iron staining was positive in mesangium and glomerular basement membrane. The proximal tubules were positive for CD10. Reactivity with DBA, UEA-I, and PNA was detected in the distal tubules and collecting ducts. Notably, DBA was reactive only with the collecting ducts and in the portion of the collecting tubule that was continuous with the collecting ducts. 9 Vimentin was positive in both the mesangium and vascular endothelium. Immunohistochemical detection of c-KIT was positive only in the stromal mast cells.
In contrast to the normal kidney tissue, the tumor cells had intense diffuse granular positivity for colloidal iron staining (Fig. 3) but not for PAS. Positive reactivity to DBA, UEA-I, and PNA was noted on the cell membrane and in the cytoplasm of the tumor cells. Tumor cells also had membranous and cytoplasmic positivity for c-KIT. A subpopulation of these cells was positive for CD10, and only the neoplastic sarcomatoid cells were positive for vimentin (Fig. 4). Based on these results, the tumor was diagnosed as chromophobe RCC with sarcomatoid change.
Human RCCs were classified according to their histopathologic and molecular biologic characteristics. 17 The majority of human RCCs are the clear cell type, which is derived from the proximal tubule epithelium. 15,17 In contrast, chromophobe RCC, collecting ducts carcinoma, and oncocytomas are derived from the collecting ducts. 3,5,15 Chromophobe RCC is composed of large and polygonal cells that possess irregularly shaped nuclei and a cloudy cytoplasm. Unlike chromophobe RCC, the tumor cells in oncocytoma are small and possess round nuclei and an eosinophilic granular cytoplasm. These 2 tumor types share many morphologic features, and their diagnosis is therefore sometimes difficult, particularly between the eosinophilic variant of chromophobe RCC and oncocytoma. 7,14,15 Because the prognosis and treatment of these tumors differ, a correct diagnosis is important. Differentiation of these tumors requires immunohistochemistry. 7 The tumor cells of human chromophobe RCC and oncocytoma retain lectin histochemical and immunohistochemical properties that are similar to those of the collecting ducts, whereas clear cell RCC retains the properties of the proximal tubule. 14,15
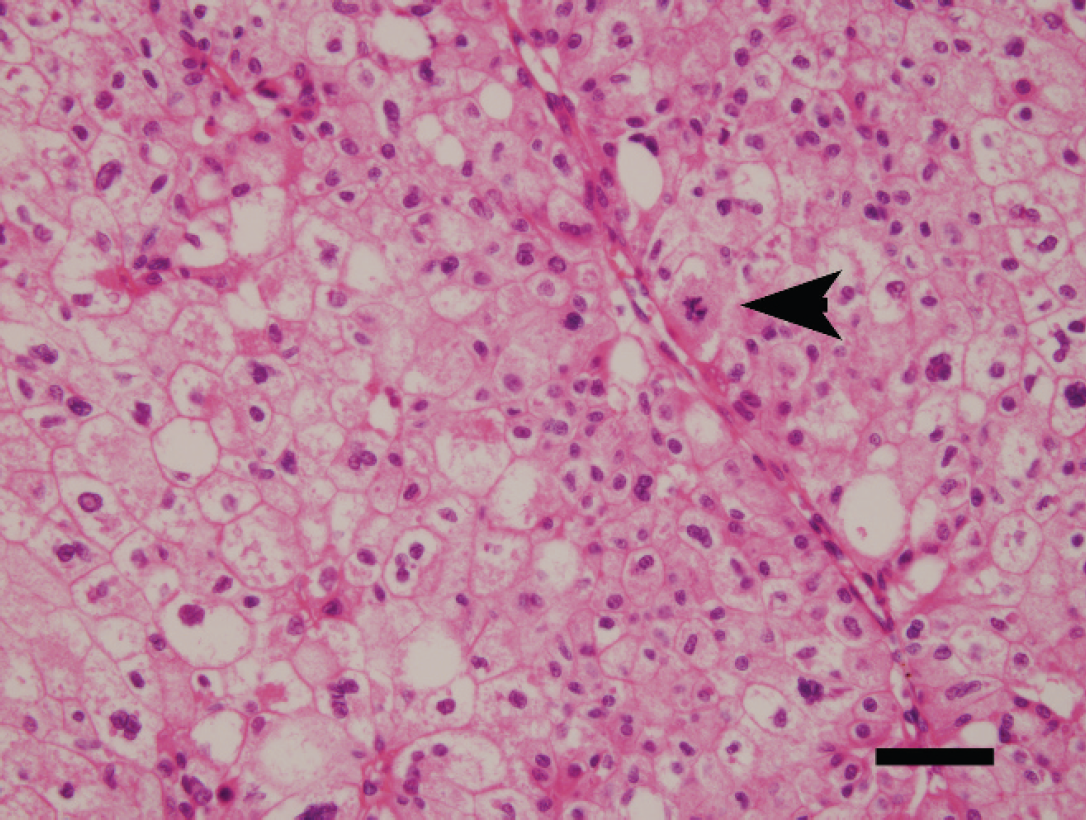
Kidney; dog. Chromophobe renal cell carcinoma. The tumor is composed of large polygonal cells with an abundant and cloudy cytoplasm. Arrowhead indicates a mitotic figure. Hematoxylin and eosin. Bar = 25 μm.
There are reports of clear cell RCC and oncocytoma in dogs but not of chromophobe RCC. 4,6,12,13,19 The diagnosis of canine renal oncocytoma was previously based on a positive PAS reaction, a positive reaction for cytokeratin immunohistochemistry, and a negative reaction for vimentin immunohistochemistry and on abundant mitochondria with stacked cristae by ultrastructural study. However, unlike previous reports, the diagnostic criteria for human chromophobe RCC were applied to this tumor. Tumor cells showed membrane and cytoplasmic positivity for c-KIT, a receptor-type tyrosine kinase for stem cell factor. 7 In this regard, previous studies have demonstrated overexpression of c-KIT in human chromophobe RCC and oncocytoma by gene expression and immunohistochemical analysis. 16,20 Human clear cell RCCs express vimentin, 1,10,15,17 which was detected in the current case only in the neoplastic sarcomatoid cells. Vimentin was found to be positive in both the desmoplastic stromal cells and sarcomatoid cells. Although sarcomatoid tumor cells and interstitial fibroblasts had relatively similar immunohistochemical pheno-types, tumor cells had atypical morphologic character rather than fibroblast. Based on this point, these 2 populations were thus differentiated. Cluster of differentiation 10 was found to be positive in both the neoplastic epithelial cells and sarcomatoid cells. Immunopositivity for CD10 was evident also in the proximal tubule of the normal kidney and has been previously proposed as a useful biomarker for the differential diagnosis of clear cell RCC. 1 In a previous study, CD10 was positive in 26% of the chromophobe RCCs analyzed, which presented with aggressive behavior. 11 Moreover, human chromophobe RCC with sarcomatoid change is considered dedifferentiated tumors and, therefore, has been associated with an unfavorable prognosis. Thus, sarcomatoid changes are considered a manifestation of dedifferentiation or epithelial-mesenchymal transition and demonstrate or are associated with an increased proliferation and infiltrative capacity.
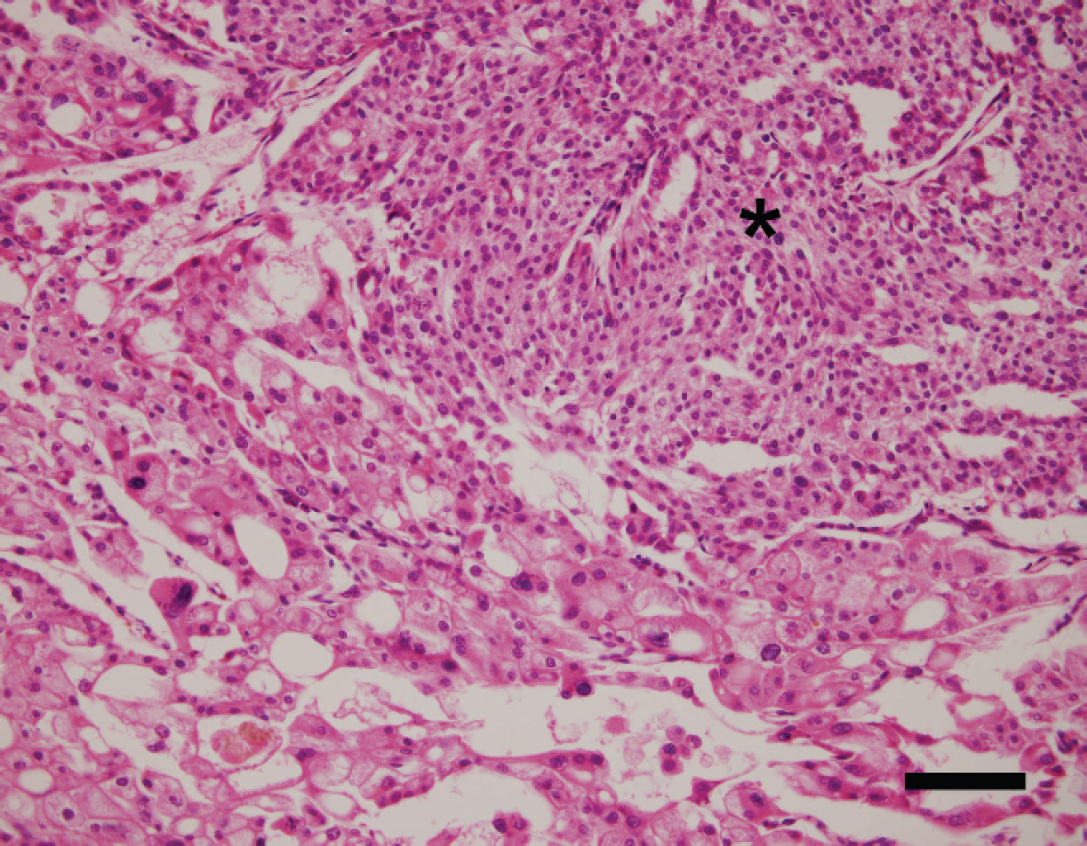
Kidney; dog. Chromophobe renal cell carcinoma. The tumor cells are associated with a sarcomatoid change. Sarcomatoid elements composed of spindle-shaped cells without obvious epithelial arrangement (asterisk). Hematoxylin and eosin. Bar = 50 μm.
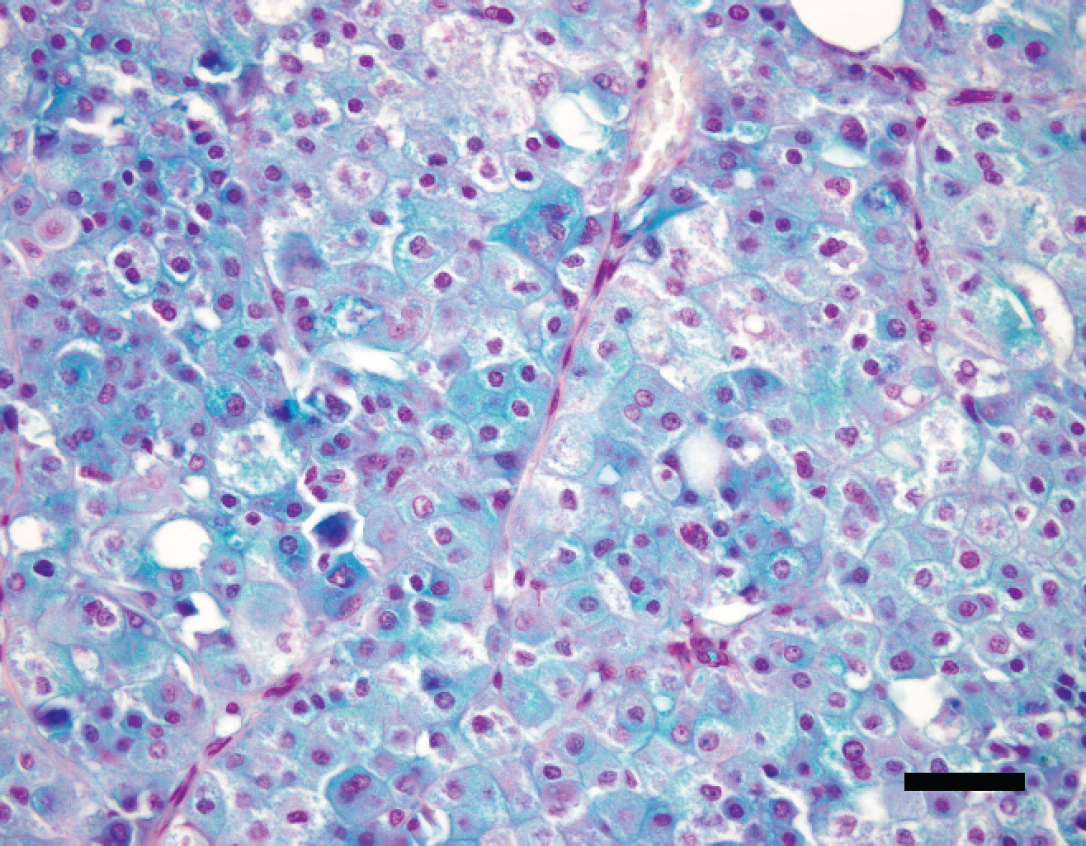
Kidney; dog. Chromophobe renal cell carcinoma. The tumor has intense diffuse granular positivity for colloidal iron staining. Hale colloidal iron method, nuclear fast red counter-staining. Bar = 25 μm.
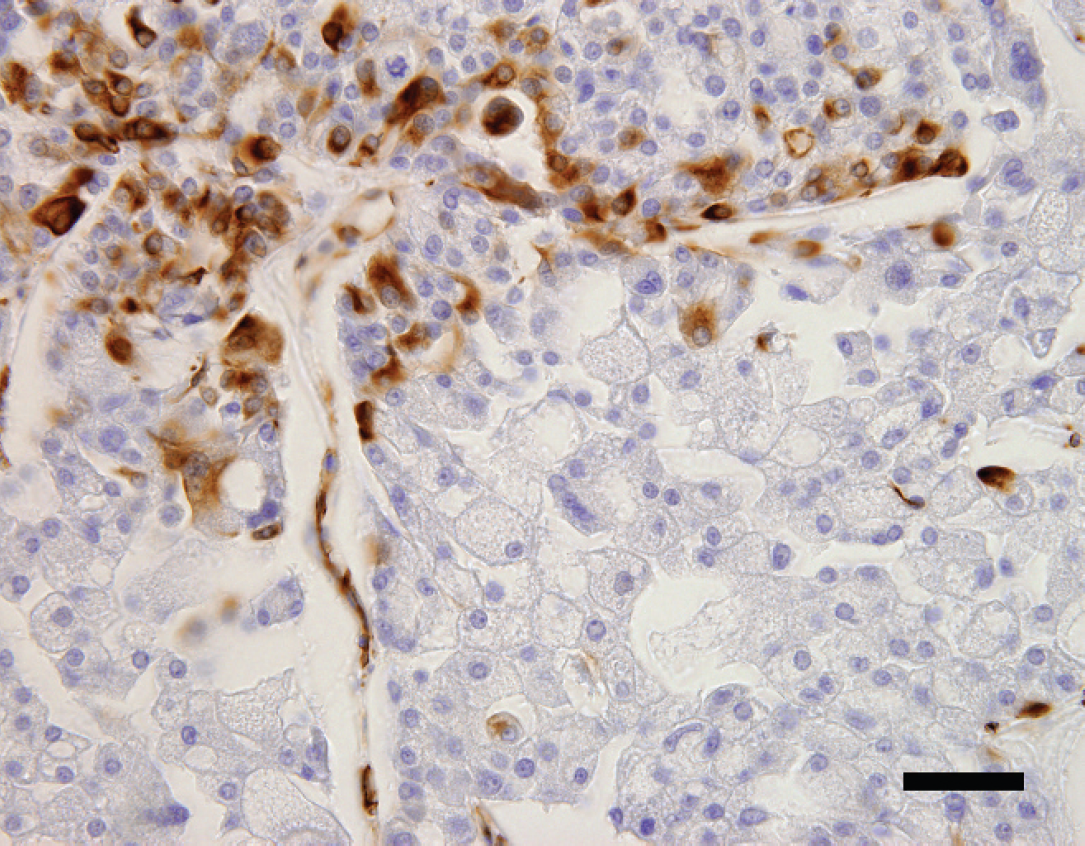
Kidney; dog. Chromophobe renal cell carcinoma. Vimentin is positive only in the neoplastic sarcomatoid cells. Streptavidin-biotin method, hematoxylin counterstaining. Bar = 25 μm.
Reactivities of differentiation markers compared with human renal cell carcinomas (RCCs) and normal canine kidney. *
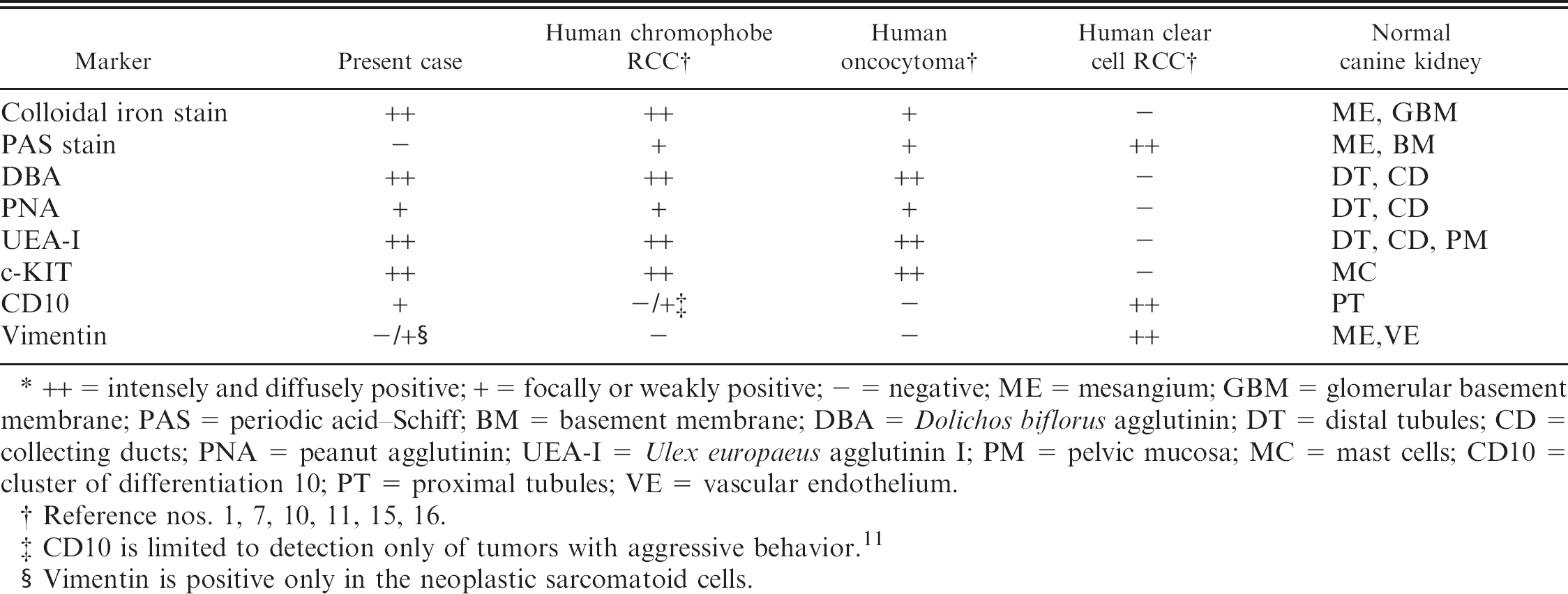
++ = intensely and diffusely positive; + = focally or weakly positive; — = negative; ME = mesangium; GBM = glomerular basement membrane; PAS = periodic acid-Schiff; BM = basement membrane; DBA = Dolichos biflorus agglutinin; DT = distal tubules; CD = collecting ducts; PNA = eanut agglutinin; UEA-I = Ulex europaeus agglutinin I; PM = pelvic mucosa; MC = mast cells; CD10 = cluster of differentiation 10; PT = proximal tubules; VE = vascular endothelium.
Reference nos. 1, 7, 10, 11, 15, 16.
CD10 is limited to detection only of tumors with aggressive behavior. 11
Vimentin is positive only in the neoplastic sarcomatoid cells.
Approximately 20% of human RCC patients have been found to present with signs of a paraneoplastic syndrome, such as hypercalcemia (13.0%). 8 The hypercalcemia observed in the current case may have been associated with the tumor because clinical chemistry data showed no evidence of renal failure.
In conclusion, the reported case of renal neoplasia in a dog is equivalent to human chromophobe RCC. Moreover, because canine chromophobe RCC may previously have been described as an atypical or malignant oncocytoma in dogs, a reevaluation of such cases is required. Future analysis of the histopathologic and molecular biologic abnormalities associated with this type of lesion is warranted.
Acknowledgements. The present work was supported in part by grants from the Japanese Ministry of Education, Culture, Sports and Science, and from Yokohama City University, Yokohama, Japan (YN).
Footnotes
a.
Seikagaku Kogyo Co., Tokyo, Japan.
b.
Novocastra Laboratories Ltd., Newcastle upon Tyne, United Kingdom.
c.
Dako North America Inc., Carpinteria, CA.
d.
Histofine®, Nichirei, Tokyo, Japan.