
Abstract
The current report describes an unusual presentation of uterine endometrial polyp with severe hemorrhage and cystic endometrial hyperplasia—pyometra complex in a 9.5-year-old female Doberman Pinscher. The dog presented with a 2-day history of bloody discharge from the vulva and an enlarged abdomen. The postmortem examination revealed a markedly distended right uterine horn with a large pedunculated mass (17 cm × 9 cm × 4 cm) and blood. Based on the histological findings, the diagnosis of uterine endometrial polyp was made.
A 43-kg, 9.5-year-old, intact, female Doberman Pinscher presented on emergency at the Veterinary Teaching Hospital and Clinic, Louisiana State University (Baton Rouge, LA) for a bloody discharge from the vulva and a severely enlarged abdomen of 2 days' duration. She was housed in an outdoor pen and had never been on heartworm prevention. On physical examination, the dog had markedly pale mucous membranes, tachycardia, dehydration (5–8%), and a bloody discharge from the vulva. A complete blood cell count, serum biochemical panel, heartworm test, a thoracic radiographs, abdominal ultrasonography, and abdominocentesis were performed. Complete blood count results revealed a marked regenerative anemia (red blood cell count, 1.74 × 106/μl, reference [ref.] interval: 5.4–8.4 × 106/μl; hematocrit, 14.2%, ref. interval: 35–54%; absolute reticulocyte count of 280.6 × 109/μl; and moderate to marked polychromasia with anisocytosis) and mild leukocytosis (white blood cell count, 36.3 × 103/μl, ref. interval: 8–14.5 × 103/μl) characterized by mild neutrophilia (23.4 × 103/μl, ref. interval: 3–11.5 × 103/μl), a left shift (band neutrophils, 4.4 × 103/μl, ref. interval: 0–0.3 × 103/μl), and monocytosis (4.4 × 103/μl, ref. interval: 0.1–1.4 × 103/μl). The remaining hematological findings were within reference intervals. The blood coagulation profile revealed increased fibrinogen concentration (554 mg/dl, ref. interval: 150–265 mg/dl), but the remaining coagulation parameters were within reference intervals. Results from the serum biochemical panel revealed moderately increased alanine aminotransferase (295 U/l, ref. interval: 14–63 U/l) and aspartate amino-transferase (150 U/l, ref. interval: 2–38 U/l) activities.
A heartworm test a was strongly positive for heartworm antigen. Radiographic findings of an enlarged pulmonary artery and peripheral vasculature with an interstitial lung pattern were consistent with heartworm disease. Abdominocentesis revealed abundant degenerate neutrophils, moderate numbers of erythrocytes, many bacterial cocci, and moderate numbers of microfilaria. Abdominal ultrasound examination revealed a severely enlarged abdomen with no evidence of free fluid in the abdominal cavity. The right uterine horn (10 cm in diameter) was larger than the left (3 cm in diameter), and both horns were filled with hyperechoic floating debris. A presumptive diagnosis of severe pyometra was made based on the physical examination and diagnostic findings. Because of the poor prognosis, the owner elected euthanasia.
On postmortem examination, the uterus was severely distended with approximately 2–3 liters of opaque red fluid (blood), with the right horn more severely affected (Fig. 1). A 17 cm × 9 cm × 4 cm, unencapsulated, pedunculated, pale tan, soft mass attached to the endometrium by a 2-cm stalk was present in the uterine lumen (Fig. 2). The mass had fluid-filled cystic structures, multifocal hemorrhage, and necrosis, which was visible both externally and on the cut surface. The endometrium was moderately thickened by multiple 3–6-mm fluid-filled cavities (cystic endometrial hyperplasia; Fig. 2, arrow). The pulmonary artery had moderate roughening of the intima (intimal proliferation) and contained more than 50 adult heartworms. Other major gross abnormalities included multifocal pulmonary hemorrhages and hepatic congestion. The differential diagnoses, based on gross necropsy examination, were uterine adenoma, uterine adenomyosis, uterine endometrial polyp, uterine carcinoma, and cystic endometrial hyperplasia—pyometra complex.
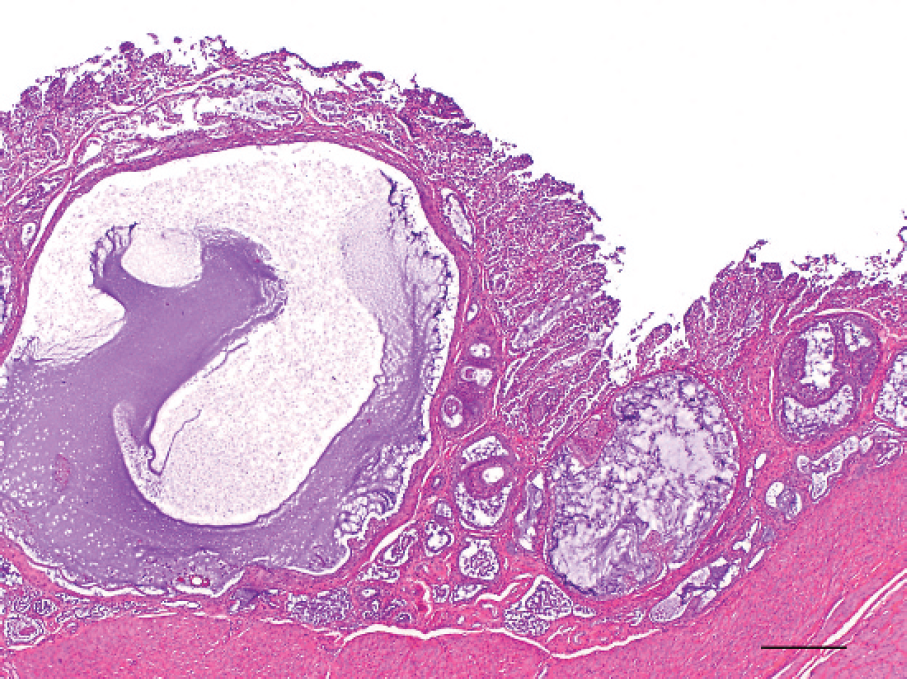
Histologically, the uterine mass was well demarcated, unencapsulated, and moderately cellular and contained many variably sized glandular structures separated by abundant fibrous connective tissue (Fig. 3). The surfaces of the mass and proliferating glands were lined by single layers of columnar epithelial cells (Figs. 4, 5). These epithelial cells had distinct cell borders and a moderate amount of eosinophilic cytoplasm. Nuclei were round to oval with finely stippled chromatin and single nucleoli. Mitoses were rare. The glands were multifocally ectatic and contained moderate amounts of eosinophilic to basophilic material admixed with necrotic cellular debris and degenerate neutrophils (Fig. 5). Multifocally, there was expansion of the stroma with edematous fluid, hemorrhage, and extensive infiltrates of plasma cells, lymphocytes, macrophages, a few neutrophils, and mast cells. The surface of the mass was multifocally ulcerated and infiltrated with large numbers of neutrophils (Fig. 4). The sections from the stalk attaching the mass to the uterine wall had similar histological findings as described above for the uterine mass. The remainder of the endometrium had multifocal dilated glands that contained amorphous eosinophilic to basophilic material admixed with necrotic cellular debris, scattered neutrophils, and few lymphocytes (Fig. 6). The cystic endometrial hyperplasia was classified as stage III, based on Dow's classification system. 8 Histologically, the mass was diagnosed as a uterine endometrial polyp. Multiple corpora lutea were present in both ovaries.
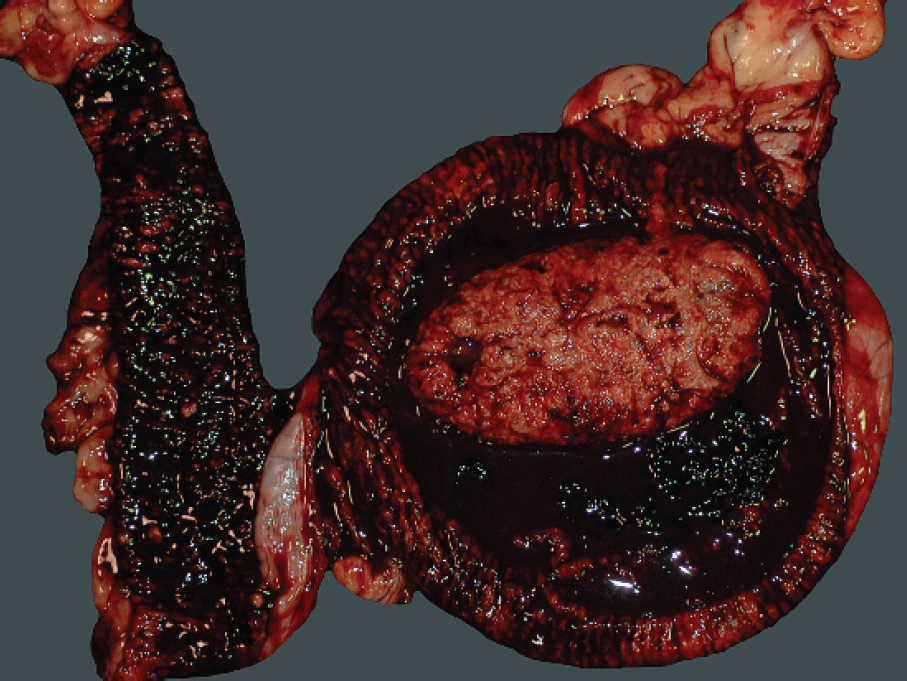
The right uterine horn contains a large amount of blood and a large pedunculated endometrial polyp in the uterine lumen. The right uterine horn was larger than the left uterine horn.
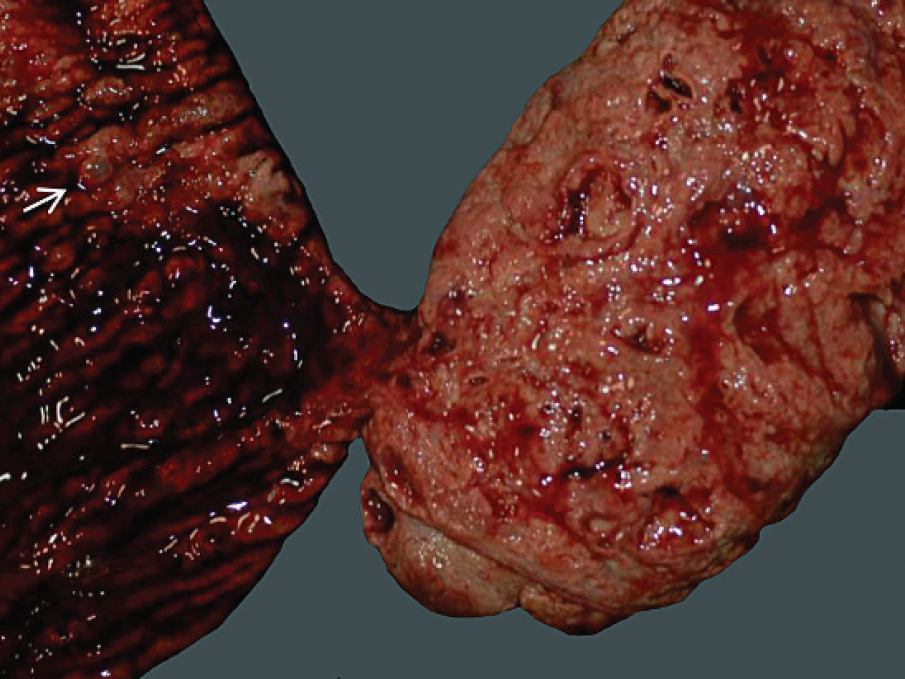
The 17 cm × 9 cm × 4 cm, unencapsulated, pedunculated, uterine polyp is present in the uterine lumen and is attached to the endometrium by a 2-cm stalk. The mass has fluid-filled cystic structures, multifocal hemorrhage, and necrosis. The endometrium is moderately thickened by multiple, fluid-filled cavities (arrow).
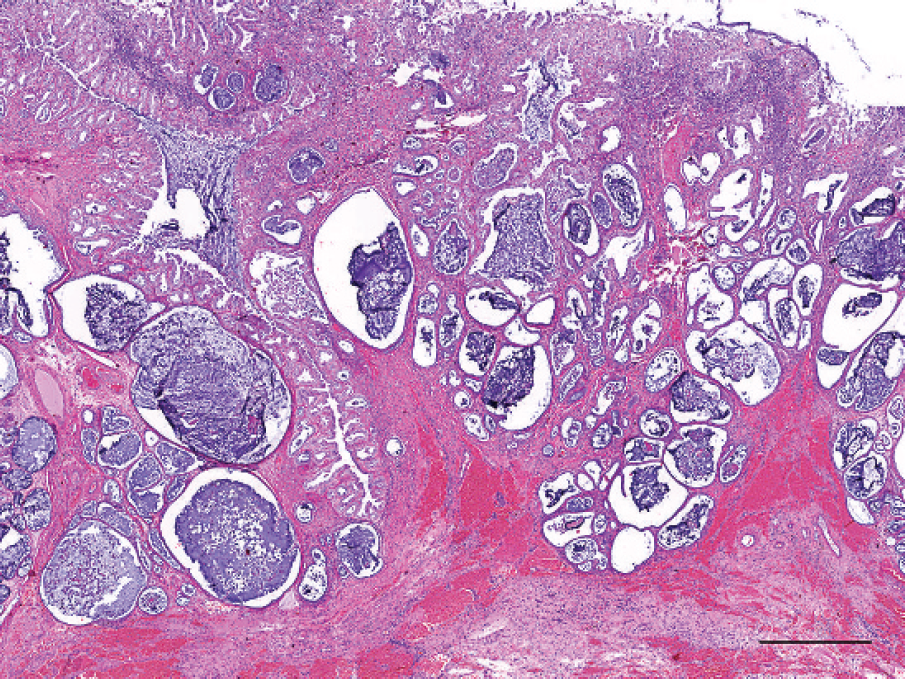
Photomicrograph of a uterine polyp with many glandular structures separated by abundant fibrous connective tissue with multifocal hemorrhage. The surface of the mass is infiltrated with numerous inflammatory cells. Hematoxylin and eosin stain. Bar = 1 mm.
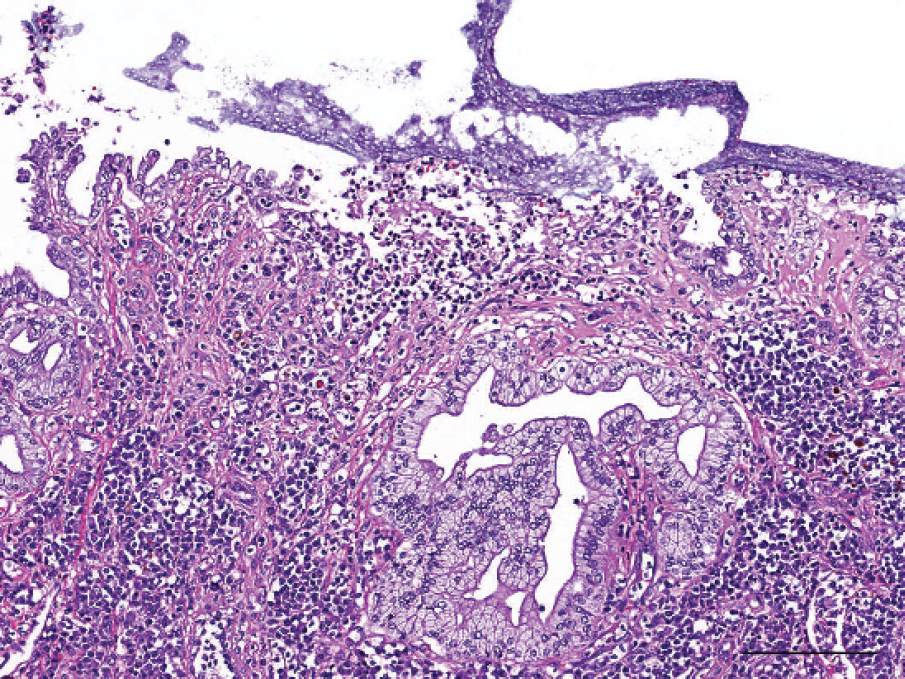
Photomicrograph of endometrial polyp with a necrotic surface that is infiltrated by neutrophils and covered with mucus. Lymphoplasmacytic infiltrates are present in the underlying stroma. Hematoxylin and eosin stain. Bar = 150 μm.
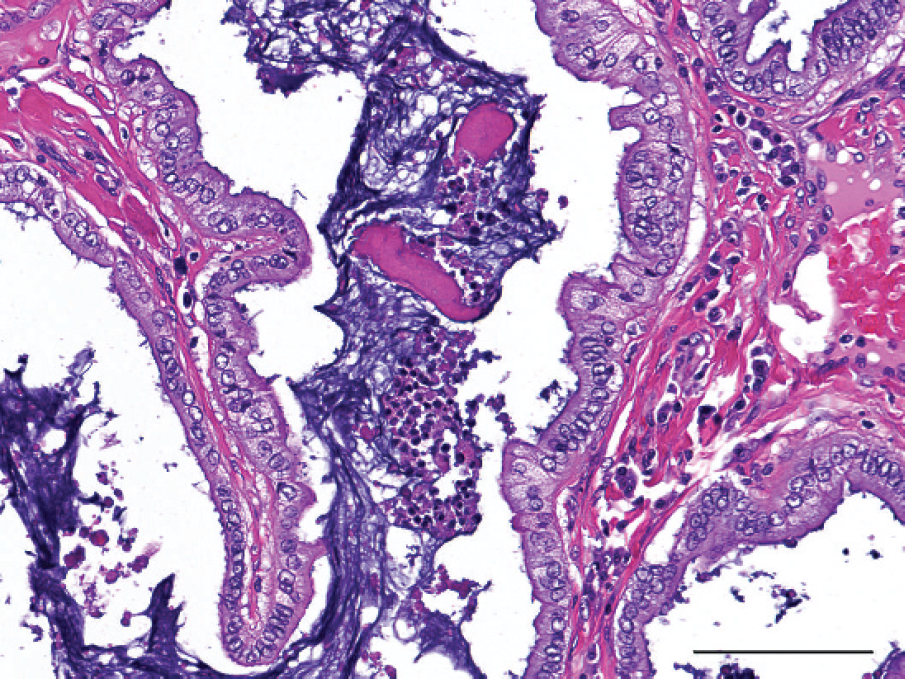
Photomicrograph of a uterine polyp demonstrating ectatic glands containing eosinophilic and basophilic material admixed with necrotic cellular debris admixed with degenerate neutrophils. Hematoxylin and eosin stain. Bar = 100 μm.
Photomicrograph of the endometrium with cystic glands containing basophilic mucoid material and a few neutrophils. Hematoxylin and eosin stain. Bar = 500 μm.
Uterine tumors in the dog are considered rare and account for only 0.3–0.4% of all canine tumors 4,6 and 1–19% of all female genital tract tumors. 10 Leiomyoma is the most common neoplasm, representing more than 90% of all canine uterine tumors. 4 Leiomyosarcoma occurs less frequently. 4,19 Endometrial polyps are solitary, proliferating masses that originate from the endometrium as broad-based sessile masses or pedunculated polyps with stalks. These polyps have been reported in dogs, 5,9,18 cats, 12 horses, 21 mice, 15 hedgehogs, 13 and elephants. 1 The specific etiology of endometrial polyps is largely unknown. However, increased prevalence of endometrial polyps in humans and zoo animals appears to be associated with increasing age and tamoxifen therapy in humans 3 and melengestrol acetate contraceptives treatment in zoo animals. 14 In a previous study, endometrial polyps were detected in mature dogs (mean age, 8.8 years), and most of the affected animals had cystic endometrial hyperplasia, 9 which was consistent with the current study. The origin of the endometrial polyp was likely due to stimulation of cystic endometrial glands leading to increased deposition of interstitial fibrous connective tissue, which expanded and protruded to form the endometrial polyp. 16 In dogs, uterine endometrial polyps are usually small, but occasionally larger polyps can compromise the uterine lumen. 9,16 However, the most significant and unusual lesion in the case reported herein is the presence of a large 17 cm × 9 cm × 4 cm mass with a extensive hemorrhage in the uterus. Histologically, this benign endometrial polyp was composed of proliferative, well-differentiated uterine glands with no evidence of local invasion or metastasis. The diagnosis of a uterine endometrial polyp was based on the nomenclature presented in the Histological Classification of Tumors of the Genital System of Domestic Animals 11 ; however, the explanatory notes did not provide a differential diagnosis for endometrial polyps. Distinction of endometrial masses may be difficult and arbitrary, and the histological findings may overlap. Adenomyosis of the endometrium could also produce focal enlargement of the uterine wall with grossly evident cysts embedded deep within the myometrium, 16 but there was no microscopic evidence of adenomyosis in the present case.
Pyometra caused severe abdominal enlargement in the animal in the current study. The diagnosis of pyometra was difficult because bacterial culture of uterine fluid and endometrium were not performed, and abundant hemorrhage was present in the right uterine horn (Fig. 1). However, the presence of neutrophilic leukocytosis in the blood as well as abundant bacterial cocci and many degenerate neutrophils in the uterine fluid obtained during abdominocentesis was suggestive of cystic endometrial hyperplasia—pyometra complex. Uterine fluid collected during abdominocentesis was erroneously interpreted as peritoneal exudates, but the fluid was actually obtained from the lumen of the uterus. Postpartum subinvolution of placental sites is a common cause of severe uterine bleeding and ellipsoidal enlargements of the uterine horn. 2,7,17 However, the absence of decidual or syncytial trophoblasts in the histological sections excluded subinvolution of placental sites in the present case. Severe hemorrhage has been reported in a dog with cystic endometrial hyperplasia—pyometra complex. 20 Torsion of a pedunculated endometrial polyp also was reported to induce rapid hemorrhagic shock and death of a dog. 9 However, the severe hemorrhage in the present case was apparently due to the presence of multifocal ulcers in the uterine endometrial polyp within the right uterine horn. Cystic endometrial hyperplasia is usually associated with pyometra, 16 which was consistent with the current case. Additional diagnostics that could have been performed in the present case included vaginal cytology and vaginoscopy to determine the stage of estrous cycle, bacterial culture of endometrium and cytologic fluid, and bacterial culture of uterine fluid.
Acknowledgements The authors thank Dr. Daniel. B. Paulsen and an anonymous reviewer for the critical evaluation of this manuscript.
Footnotes
a.
SNAP® 3DX® heartworm test, IDEXX Laboratories Inc., Westbrook, ME.