
Abstract
A 2-year-old, female German Shepherd Dog with facial nerve paralysis was diagnosed with acute myelomonocytic leukemia based on clinical, cytologic, and immunologic findings. Proteinuria (urine protein:creatinine ratio = 1.5) occurred in the absence of renal failure. Qualitative assessment of proteinuria by sodium dodecyl sulfate–agarose gel electrophoresis revealed a broad band with a molecular weight of approximately 15 kDa that was compatible with lysozyme (LZM). A diagnosis of tubular proteinuria was made, and a chemical evaluation of LZM in serum and urine samples was performed using a turbidimetric assay. The LZM concentrations were 24.5 mg/l (reference interval: 2.5–8.0 mg/l) and 274.5 mg/l (reference interval: <2 mg/l) in serum and urine, respectively.
Lysozyme (LZM) is an enzyme with a molecular weight (MW) of 15 kDa. 16 In humans, LZM has been detected in the cytoplasm of myeloid leukocytes, monocytes, and macrophages as well as in body fluids, including tears, saliva, milk, and serum. 17 Serum LZM concentrations apparently reflect enzyme release by normal or increased cellular turnover of neutrophils, monocytes, and macrophages. 17 This enzyme is mainly degraded in the kidney; it is filtered through the glomeruli as a low molecular weight (LMW) protein and reabsorbed in the proximal tubules. 13 The absorptive has a maximal threshold above which no further LMW protein absorption occurs. 2 For these reasons, evidence suggests that LZM can be found in the urine of human patients with renal disease when renal tubular absorption is impaired or when the normal renal tubular threshold is exceeded because of high serum LZM concentrations. This last event, known as “overflow lysozymuria,” has been reported in human myeloproliferative disorders, particularly those with monocytic and histiocytic differentiation, and in granulomatous diseases. 6,12,16,18,19 Determination of serum and urine LZM concentrations has been proposed previously as a useful test for the differential diagnosis of acute leukemia, 21 and subsequent classification of some forms of acute leukemia using the French–American–British (FAB) system. 22
In dogs, LZM has been found in macrophages, monocytes, neutrophils, serous cells of exocrine glands associated with respiratory, alimentary, and ocular mucosae, and proximal renal tubular epithelial cells. 17 In 1978, the presence of LZM in canine urine was associated with proximal renal tubular damage, which suggested that lysozymuria could be used as an index of renal tubular damage. 3 However, LZM has been more widely used in veterinary pathology as an immunohistochemical marker for neoplastic and proliferative processes, especially of histiocytic origin. A 1986 study demonstrated that LZM detection was a useful adjunct to conventional morphologic methods to identify histiocytes in systemic histiocytosis, malignant histiocytosis, and granulomatous panniculitis in dogs. 18 In later studies, researchers verified increased serum LZM activity in other neoplastic diseases, such as malignant melanomas, thyroid tumors, soft-tissue sarcomas, mast cell sarcomas, and carcinomas, 5,9 suggesting that measuring serum LZM could be helpful in screening those dogs with suspected malignancies. In those cases, the increased expression of serum LZM was explained as a likely indicator of macrophage-mediated host resistance against neoplastic proliferations. 9
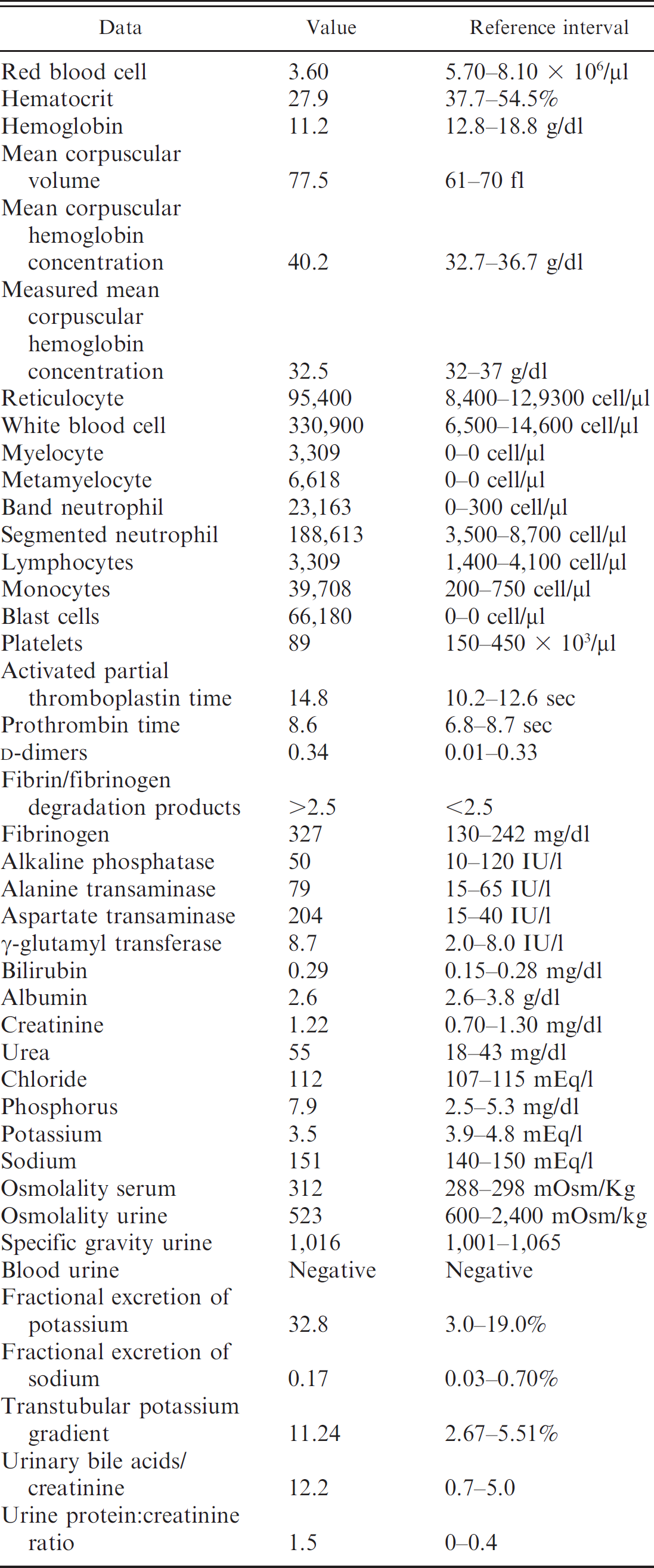
. Hematologic, hemostasis, biochemical, and urinalysis abnormalities in a German Shepherd Dog with acute myelomonocytic leukemia.
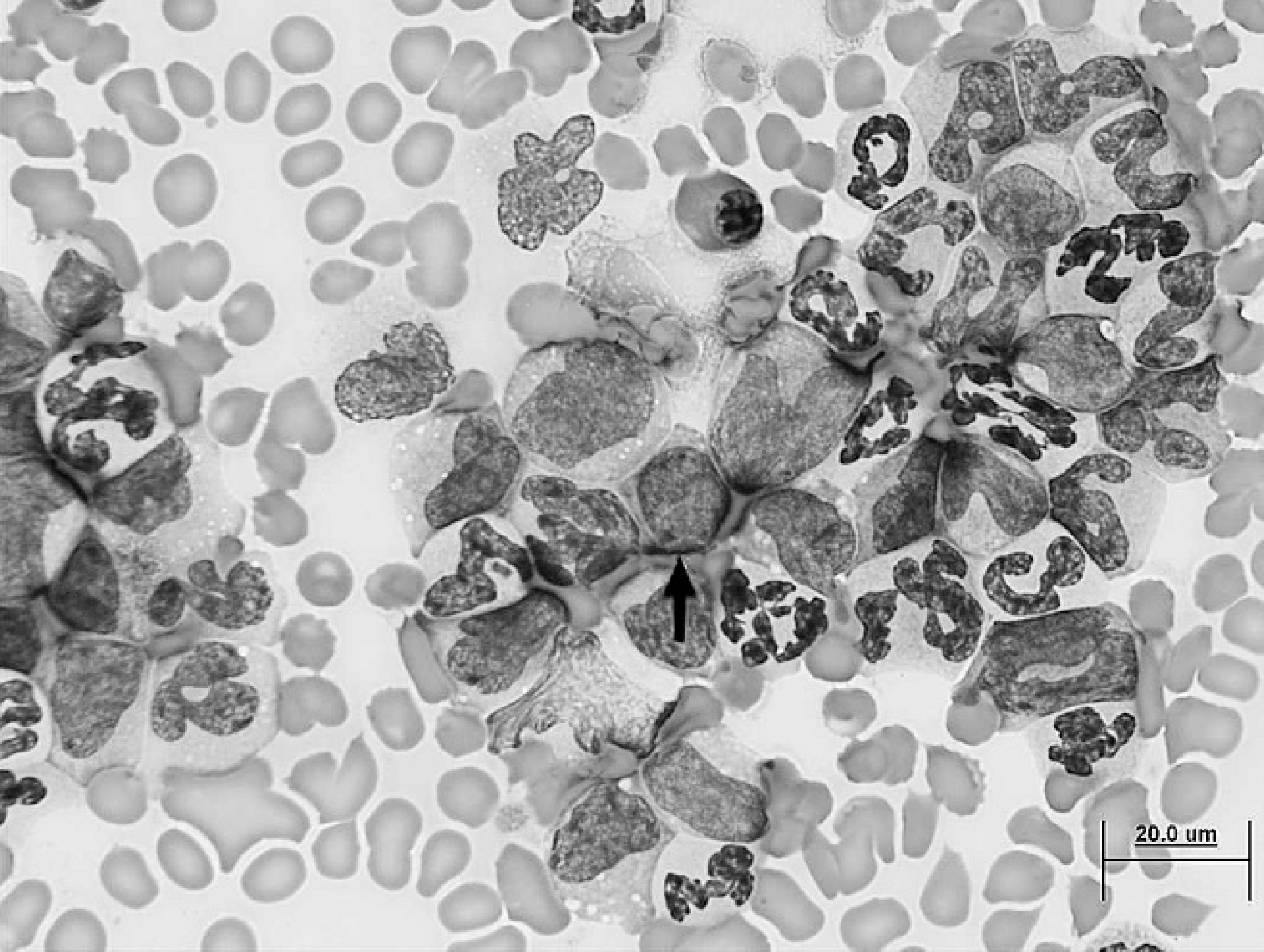
Blood smear. Neutrophils with left shift, monocytes, and many atypical leukocytes. Atypical leukocytes are medium to large round cells with a high nuclear:cytoplasm ratio, finely stippled nuclear chromatin, inconspicuous nucleoli, and moderately abundant basophilic cytoplasm (arrow). Modified Wright stain. 60x magnification. Bar = 20 μm.
Determination of serum and urine LZM concentration as an ancillary test in the diagnosis of acute myeloproliferative disorders in animals is rare. The objective of the current report is to describe a case of canine acute myelomonocytic leukemia (AML-M4) with high serum and urine LZM concentrations.
A 2-year-old, female German Shepherd Dog was presented with a recent history of fever that was not responsive to antibiotics, sporadic vomiting, lethargy, and inappetence. Physical examination revealed ptyalism secondary to facial nerve paralysis and an enlarged spleen on abdominal palpation. A complete blood cell count (CBC), a serum and urine biochemical profiles, b urinalysis, and hemostasis profiles c were performed. The most important test results are listed in Table 1. The CBC revealed a moderate macrocytic normochromic marginally regenerative anemia. Changes in erythrocyte morphology on the stained blood smear included macrocytosis (++) and elliptocytosis (+). The falsely increased mean corpuscular hemoglobin concentration was probably the result of hemolysis. The normal value of measured mean corpuscular hemoglobin concentration, which is a direct (optic) measure of hemoglobin inside the red blood cells, confirmed the normochromic anemia. The inadequate erythrocytic regenerative response was attributed to myelophthisis as based on changes in the leukogram.
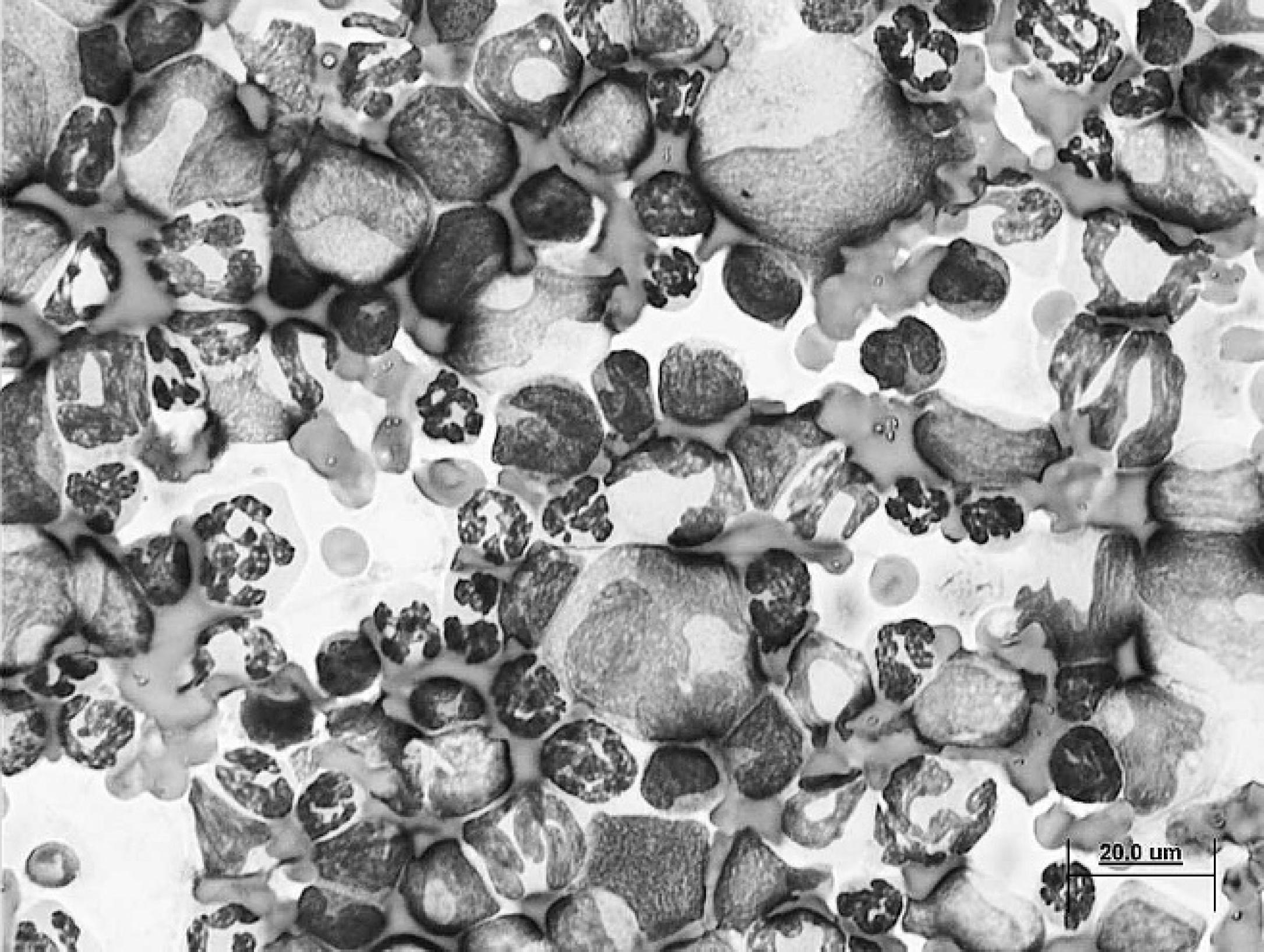
Bone marrow smear. Proliferating neoplastic myeloid cells display granulocytic and monocytic differentiation. Monocytic differentiation is characterized by a large convoluted nucleus and abundant pale basophilic cytoplasm with frequently vacuoles. Modified Wright stain. 60x magnification. Bar = 20 μm.
Severe leukocytosis was characterized by neutrophilia with left shift, monocytosis, and the presence of many atypical leukocytes (Fig. 1). Moderate thrombocytopenia was confirmed by microscopic blood smear examination. Increased hepatic enzyme activities (alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl-transferase), bilirubin concentration, and urine bile acid to urine creatinine ratio 1 were consistent with liver disease, probably associated with diffuse infiltration of the parenchyma by neoplastic leukocytes. Unfortunately, cytologic specimens of liver were not evaluated to confirm this speculation. The mild hyperbilirubinemia was suggestive of cholestasis and/or hemolysis.
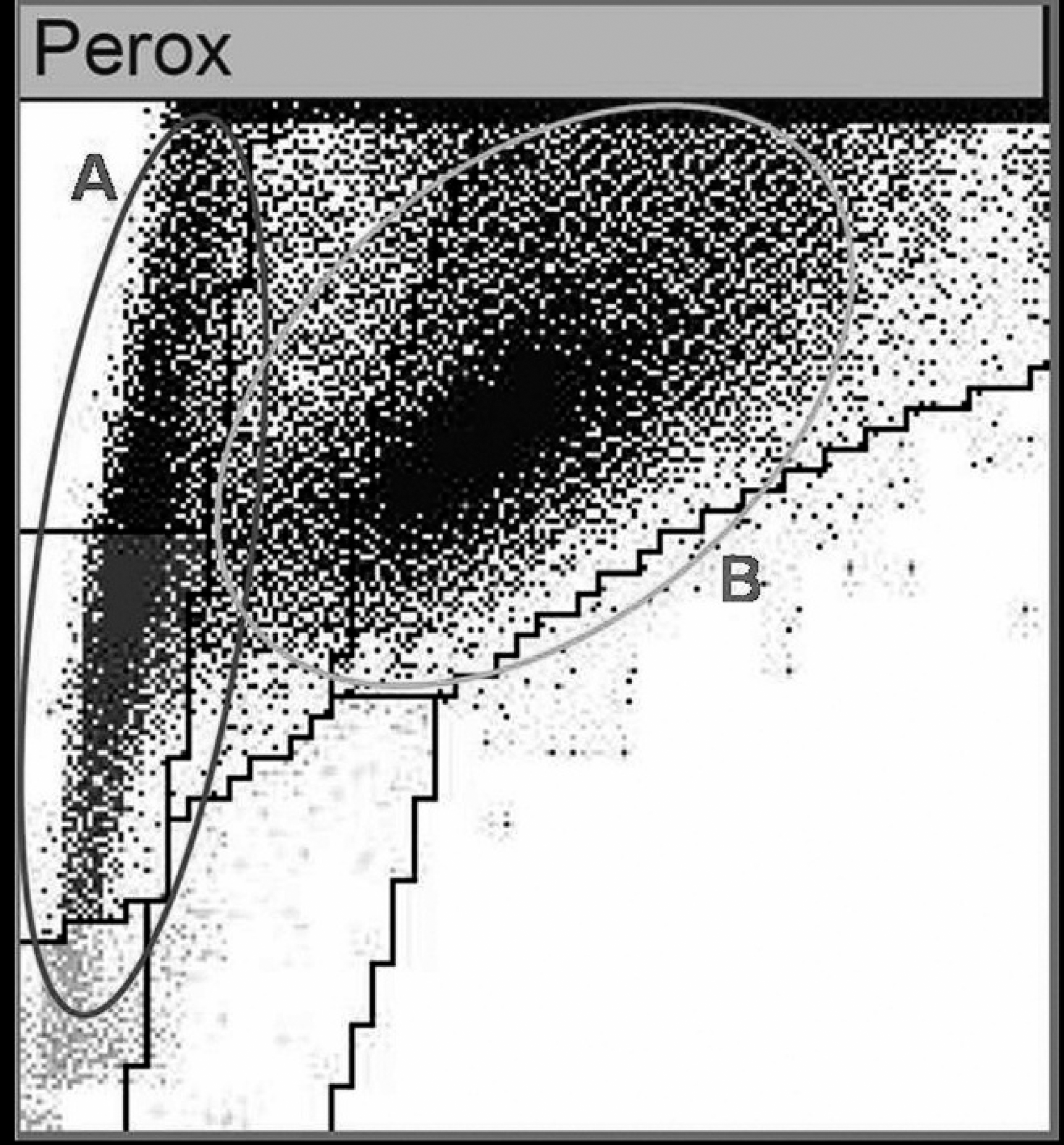
Peroxidase activity detected by a commercial hematology analyzer. The automated cytochemistry channel of the hematology analyzer detects reactive cells according to their size (Y axis) and peroxidase activity (X axis). The “A” oval contains a cluster of cells with very low peroxidase activity, and the “B” oval contains a cluster of cells with strong but heterogeneous peroxidase activity. This pattern is generally indicative of acute myeloid leukemia.
The hemostasis profile was suggestive of compensated disseminated intravascular coagulation (DIC) with hyperfibrinogenemia due to inflammation. Proteinuria (urine protein:creatinine ratio = 1.5) was detected in the absence of renal failure. Azotemia and hyperphosphatemia were compatible with a prerenal disease based on serum and urine osmolality values and specific gravity urine.
Cytologic examination of bone marrow disclosed increased cellularity with a high myeloid:erythroid ratio (50:1) secondary to hyperplasia of granulocytic and monocytic cell lines. Myeloblasts and monoblasts represented more than 30% of all nucleated cells. Neutrophilic series was repre-sented from myeloblasts to mature granulocyte. Monocytic differentiation was mainly characterized by cells with large convoluted nuclei and abundant pale basophilic cytoplasm with frequent vacuolates (Fig. 2). Erythrophagocytosis was frequently observed, confirming the presence of extravascular hemolysis. Erythroid and megakaryocytic cells were decreased, probably because of myelophthisis, with subsequent nonregenerative anemia and thromobocytopenia. 20 The reduction in platelet count could also be explained by platelet consumption due to DIC.
Characteristics of antibodies used in the current study. *
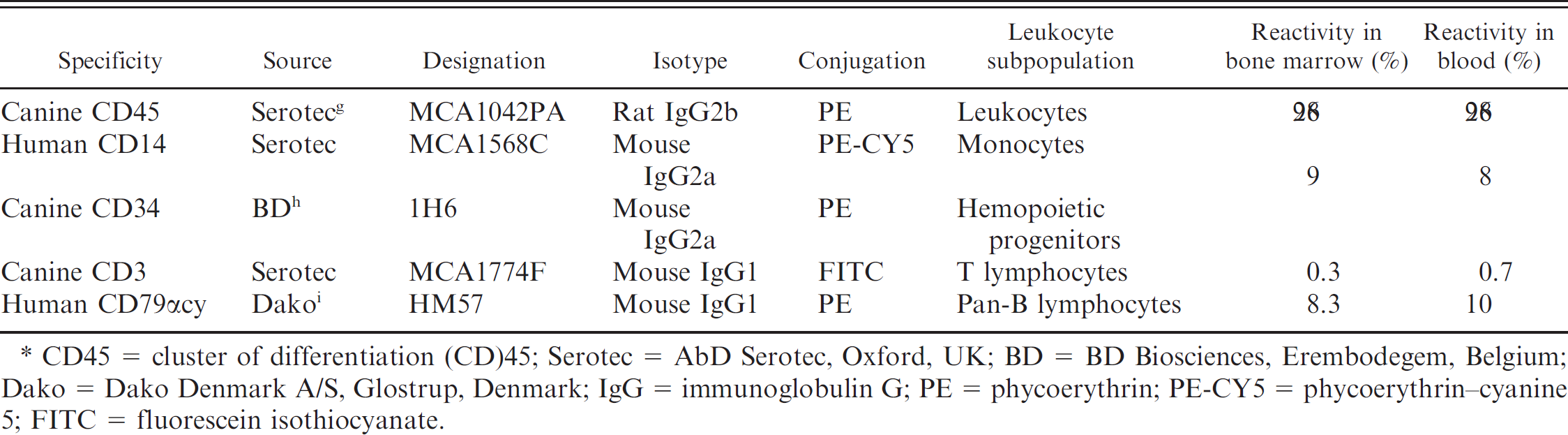
CD45 = cluster of differentiation (CD)45; Serotec = AbD Serotec, Oxford, UK; BD = BD Biosciences, Erembodegem, Belgium; Dako = Dako Denmark A/S, Glostrup, Denmark; IgG = immunoglobulin G; PE = phycoerythrin; PE-CY5 = phycoerythrin–cyanine 5; FITC = fluorescein isothiocyanate.
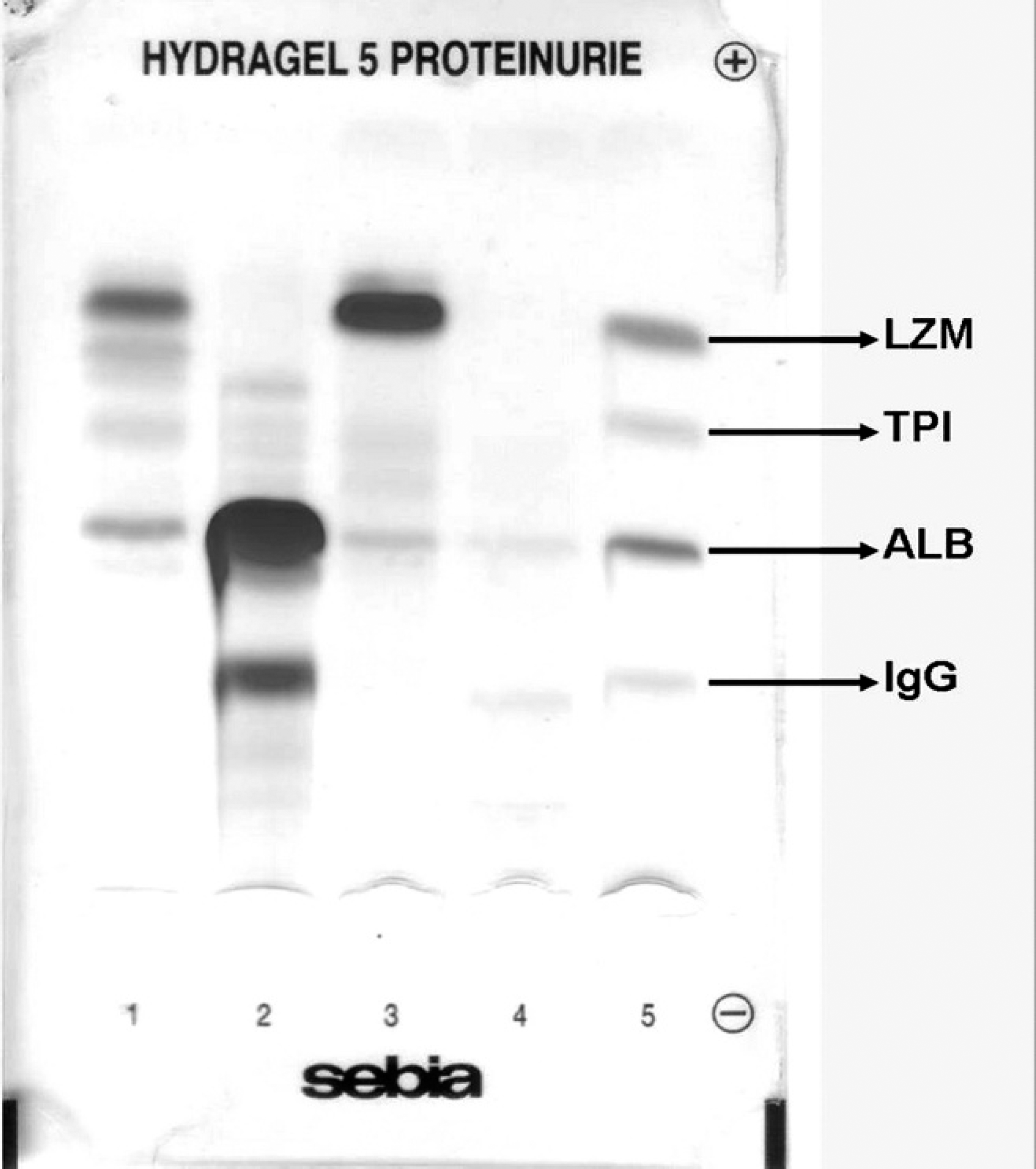
Migration of urinary proteins after sodium dodecyl sulfate–agarose gel electrophoresis. Lanes 1–4 represent electrophoresis of different urinary specimens. Lanes 1, 2, and 4: routine laboratory diagnostic samples; lane 3: dog with acute myeloid leukemia; lane 5: molecular weight control (MWC) where known proteins are underlined. LZM = lysozyme 15 kDa; TPI = triose phosphate isomerase (27 kDa); Alb = albumin (66 kDa); IgG = immunoglobulin G (150 kDa). The thick band in lane 3 is compatible with LZM based on the approximate molecular weight compared with the MWC.
Flow cytometric immunophenotyping was performed on K3–ethylenediamine tetra-acetic acid blood and bone marrow samples as previously reported. 23 The designation, specificity, and reactivity of the primary antibodies used in flow cytometry are presented in Table 2. Because cluster of differentiation (CD)45 is expressed on the surface of all hematopoietic cells, with the exception of erythroid and platelet lines, it is a useful immunologic marker to assess myeloid lineage assignment. During flow cytometry, the gate was drawn around the large neutrophil and monocyte regions in blood and bone marrow specimens. High positive reactivity to CD45 and CD34 antibodies and the failure to label with CD3 and CD79 antibodies were consistent with a diagnosis of AML. Moreover, positive reactivity to CD14 in the same regions indicated myelomonocytic differentiation. Finally, cytologic and immunologic findings, peroxidase reactivity (Fig. 3), and nuclear density analysis (PANDA) using a commercial hematology system 8 supported a diagnosis of AML-M4 according to the FAB classification. 11,14,23,24
Qualitative assessment of proteinuria was performed by sodium dodecyl sulfate–agarose gel electrophoresis d of a urine sample using a semiautomated system e and following the manufacturer's recommendations. A thick protein band with a MW of approximately 15 kDa (compared with the MW control) was compatible with LZM (Fig. 4, lane 3). Additional protein bands with LMW and a protein band of 66 kDa that was compatible with albumin were also observed. A diagnosis of renal tubular proteinuria was made. Concentrations of LZM were subsequently measured in serum and urine samples using a turbidimetric assay. f The concentration of LZM was 24.5 mg/l (reference interval: 2.5–8.0 mg/l) in serum and 274.5 mg/l (reference interval: <2 mg/l) in urine. The high serum LZM concentrations were probably the result of acute myeloid cellular proliferation with the liberation of the enzyme from monocytes and neutrophils, as previously reported. 17 The high enzymatic detection in the urine was likely associated with an impaired renal tubular absorption as expression by an overflow lysozymuria.
The presence of LZM with other LMW protein bands in urine also suggested the presence of precocious renal tubular damage without kidney failure. In fact, the accumulation of LZM inside the renal tubular cells may induce renal tubular dysfunction. 10 In addition, hypokalemia correlated with the high fractional excretion of potassium (FEK+; Table 1) could also suggest renal tubular dysfunction. In a study of 66 human patients with acute leukemia, serum potassium concentrations were found to be inversely correlated with FEK+, suggesting an important role of lysozymuria-induced kaliuresis, in producing potassium depletion in these patients. 10 However, further studies are necessary to confirm the presence of this mechanism in veterinary patients.
Interestingly, facial nerve paralysis has been seen previously in dogs with acute myelomonocytic leukemia. 7,15 In human medicine, symptomatic facial nerve involvement in AML is rare and may be due to leukemic cell infiltration at any site of facial nerve or occurrence of a granulocytic sarcoma in the temporal bone or auditory canal. 4 Thus, myelomonocytic leukemia should be considered as a differential diagnosis for facial nerve paralysis in dogs.
Acknowledgements. The authors thank Dr. Valeria Pantaleo for her support and assistance with this project.
Footnotes
a.
ADVIA 120 analyzer, Siemens Healthcare Diagnostics, Deer-field, IL.
b.
Olympus AU 2700 analyzer, Olympus diagnostics, Hamburg, Germany.
c.
Sta Compact, Diagnostica Stago, Roche, Basel, Switzerland.
d.
Hydragel 5 proteinurie, Sebia, Lisses, France.
e.
Hydrasys analyzer, Sebia, Lisses, France.
f.
Lysozyme Standard, turbidimetric assay, Paramedical, Salerno, Italy.
g.
AbD Serotec, Oxford, UK.
h.
BD Biosciences, Erembodegem, Belgium.
i.
Dako Denmark A/S, Glostrup, Denmark.