
Abstract
Two quadrigeminal arachnoid cysts with different pathogenesis are described in 2 different species. A 10-week-old male Persian kitten with a progressively decreasing level of consciousness died spontaneously. At necropsy, mild internal hydrocephalus, caudal cerebellar coning, and cerebellar herniation through the foramen magnum were associated with a congenital quadrigeminal arachnoid cyst compressing the rostral cerebellum and shifting the entire cerebellum caudally. In contrast, a possibly acquired quadrigeminal cyst was observed in a 2-year-old male neutered Yorkshire Terrier in association with necrotizing encephalitis. Quadrigeminal arachnoid cysts have been rarely reported in dogs and humans.
The owner of a 0.8 kg, 10-week-old thin, male Persian cat that was purchased at a local pet shop described a 24- to 36-hr period of lethargy that progressed to decreasing levels of consciousness and death. At necropsy, there was a 4-cm wide × 1.5-cm long intrameningeal cystic cavity filled with clear fluid that was located between the cerebral hemispheres and the cerebellum and filled the quadrigeminal cistern (Fig. 1). Coning of the vermis and caudal cerebellum was also present as a result of herniation through the foramen magnum, along with dilation of the lateral ventricles to 2 to 3 times their normal volume (Fig. 2). No other significant lesions were detected grossly.
Microscopically, the cat's post-tentorial/quadrigeminal cystic space was lined by arachnoid membrane characterized by a delicate membranous row of interconnected flattened arachnoid cells along with fragmented trabeculae composed of loose connective tissue with loosely arranged fibroblasts possessing irregular branching processes (Fig. 3A, 3B). Throughout the brain, there were expanded clear to lightly eosinophilic spaces around blood vessels and neuronal cell bodies that frequently contained amorphous eosinophilic substance consistent with low-protein transudate indicating cerebral edema. No evidence of inflammatory cells was seen in the brain parenchyma or meninges, nor was there any evidence of other lesions that might predispose to the formation of a congenital arachnoid cyst. The internal hydrocephalus might also have been congenital; however, compromised cerebrospinal fluid (CSF) flow/ drainage due to the cystic mass could have resulted in increased pressure within and secondary dilation of the lateral ventricles secondary to the presence of the cyst.
In contrast to the congenital quadrigeminal arachnoid cyst (QAC) seen in the kitten, a 2.3 kg, 2-year-old male, neutered Yorkshire Terrier presented with multifocal antemortem neurologic signs, including generalized ataxia, paraparesis progressing to tetraparesis circling to the left, lack of menace response in the right eye, hyper-reflexive limb reflexes, anisocoria, and a marginally decreased level of consciousness. These signs began 1 week before presentation. Cerebrospinal fluid analysis yielded only necrotic cellular debris, which was consistent with a degenerative or necrotizing process. Seizures became increasingly refractory to treatment, and the dog was euthanatized. At necropsy, a 2.5-cm wide × 1.5-cm long thin-walled cyst between the cerebellum and cerebral hemispheres was present that filled the quadrigeminal cistern. This cyst was filled with pink fluid that compressed and displaced the cerebellum caudally and ventrally and was associated with a 5-mm-in-diameter area of hemorrhage over the left cerebellum (Fig. 4). Coning of the caudal cerebellum from herniation of the vermis through the foramen magnum also was observed. The cerebral hemispheres collapsed easily when compressed, and the lateral ventricles were mildly dilated. The white matter appeared gray and gelatinous, whereas the gray matter was tan and friable.
Microscopically, the lining of the quadrigeminal cyst was consistent with an arachnoid membrane as described in the cat but with concurrent lymphocytes, plasma cells, macrophages, and hemorrhage. Approximately 40% of the cerebrum, cerebellum, midbrain, and brainstem were totally effaced by an intense infiltrate of macrophages, lymphocytes, and plasma cells. Increased numbers of microglial cells and astrocytes (gemistocytes) were admixed with occasional multinucleated giant cells and necrotic cellular debris surrounding areas of liquefactive necrosis. The numbers of neurons and amount of neuropil were markedly decreased in affected areas. Blood vessels had
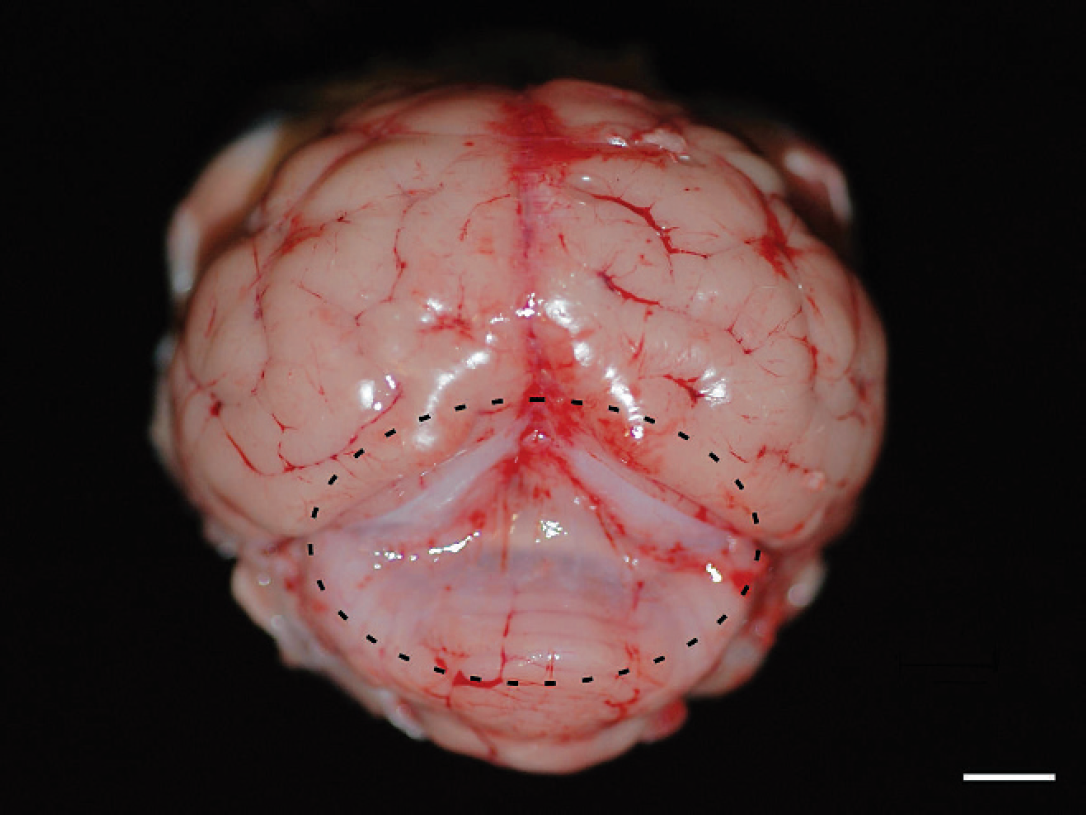
Persian kitten. Gross image of a brain with meninges in the area of the quadrigeminal cyst. The fluid filling the cyst cavity was lost during removal of the brain from the skull. The margins of the cyst are indicated with a dashed line. Bar = 1 cm.
marked, densely cellular cuffs of lymphocytes and plasma cells.
In humans, small arachnoid cysts are usually considered benign. Similarly, in dogs, there is some question regarding the significance of many such lesions. 5 In both of the cases in the current report, the cysts were thought to be clinically relevant. The mass effect from the cyst in the cat and subsequent cerebellar herniation into the foramen magnum was fatal. In the Yorkshire Terrier, the cyst may have contributed to the progression of the neurologic signs and the decision to euthanatize the animal, but a clinically silent congenital cyst could not be excluded given the presence of severe necrotizing encephalitis.
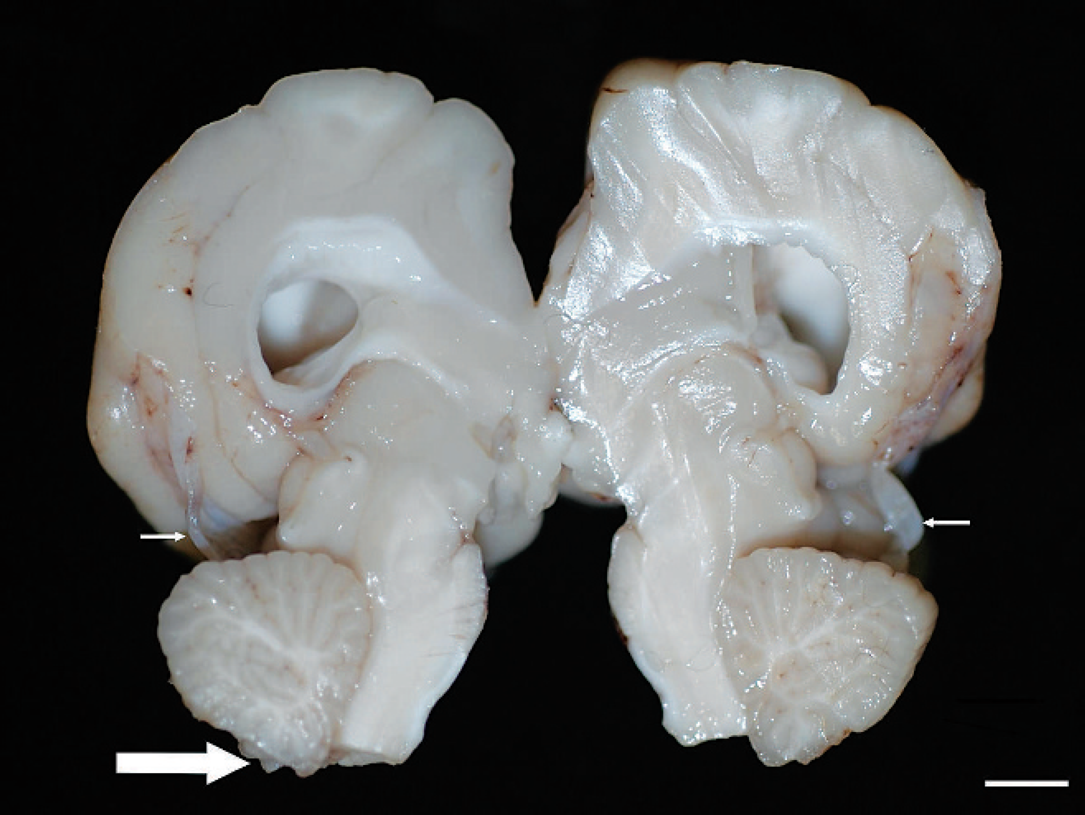
Persian kitten. Midline section of a brain demonstrating mild dilation of the lateral ventricles, the area of the quadrigeminal cyst (small white arrows) with caudal displacement of cerebellum, and coning of the caudal cerebellum from herniation into the foramen magnum (large white arrow). Bar = 1 cm.
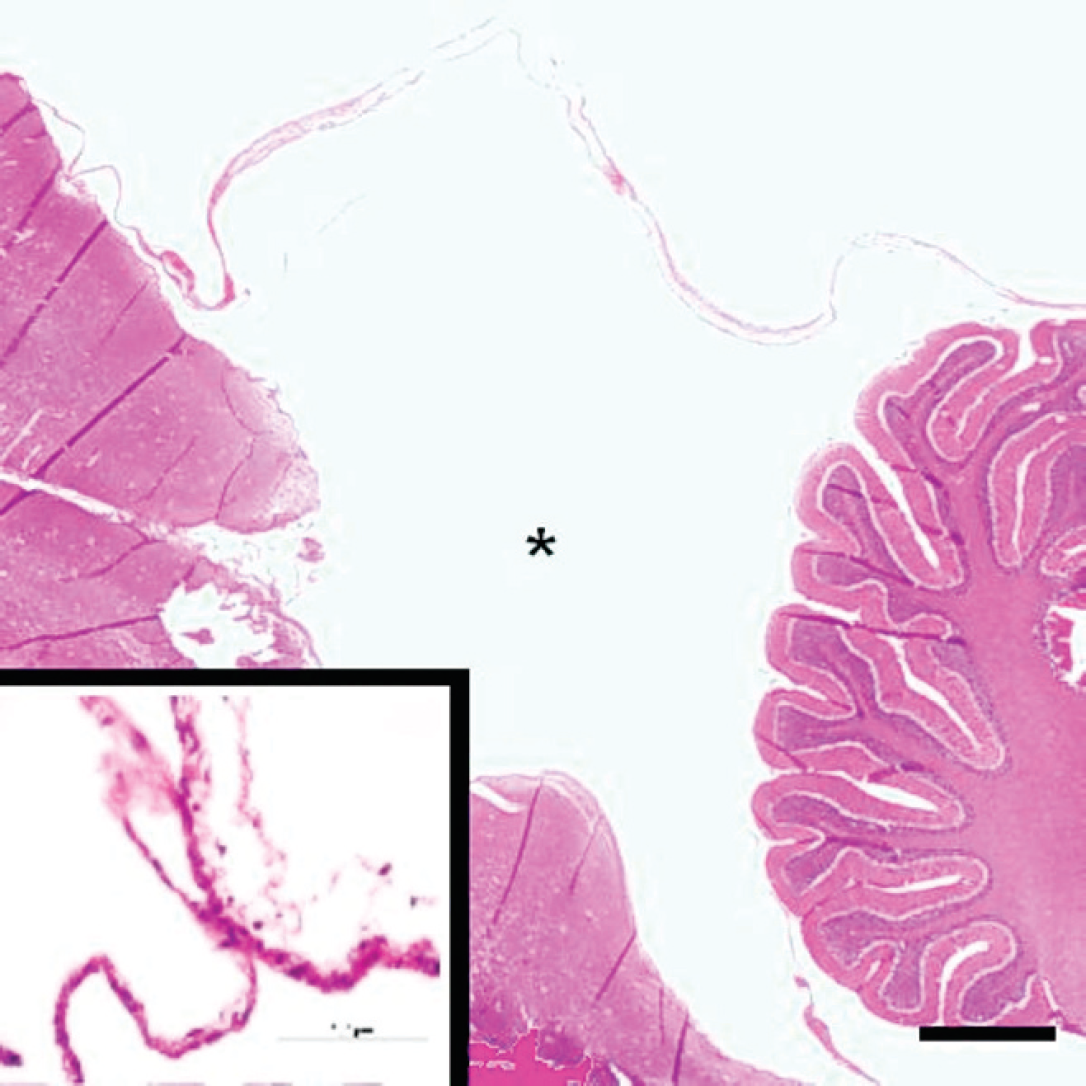
Persian kitten. Subgross sagittal section through the quadrigeminal cyst. Hematoxylin and eosin stain. Bar = 0.5 cm. Asterisk indicates cyst lumen. Inset: higher magnification view of the cyst lining consistent with a split arachnoid membrane. Bar = 100 μm.
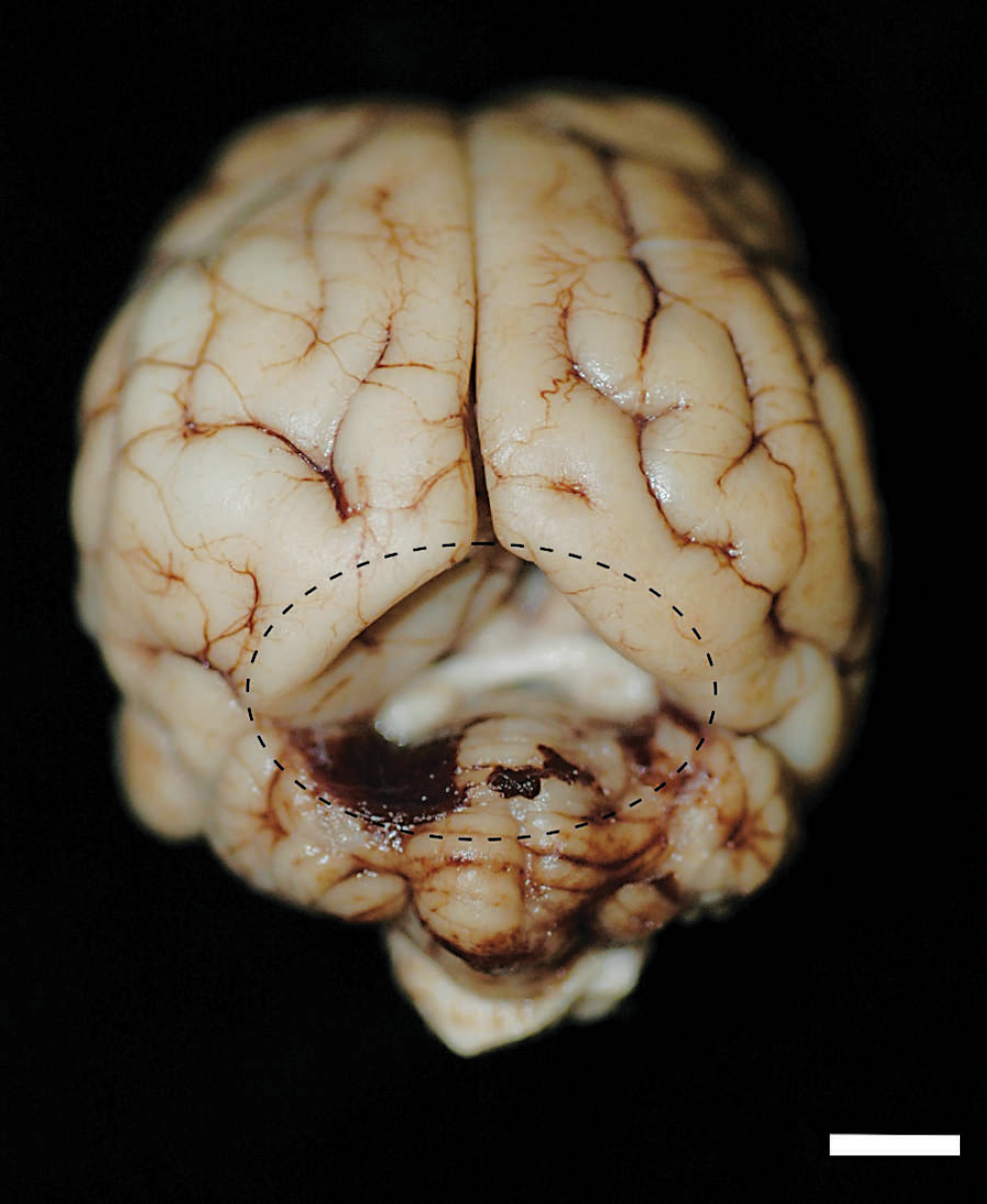
Yorkshire Terrier. Gross image of the brain showing dilation of the quadrigeminal cistern and compressive effect of the quadrigeminal cyst. The meninges and cyst were removed before photography. A focally extensive area of hemorrhage is also apparent over the left cerebellar hemisphere. The dashed line indicates the margins of the quadrigeminal cyst. Bar = 1 cm.
In both cases, the anatomic location and arachnoid lining were consistent with previous descriptions of QACs in humans and dogs. 2,4,5,10,16–18 Arachnoid cysts occur in the central nervous system within the arachnoid membrane, arise on the midline of the neural axis, contain pellucid fluid that is rarely xanthochromic, and do not communicate with the ventricular system. 7 Arachnoid cysts can be classified according to location along the neural axis and may occur within the spinal canal where they are located subdurally or in the epidural space. When classified histologically, arachnoid cysts are composed of either arachnoid connective tissue or glioependymal tissue and designated as arachnoid or glioependymal cysts. Glioependymal cysts are composed of a layer of glial fibrillary acidic protein-positive glial cells covered multifocally by epithelial cells, some of which have apical cilia consistent with their ependymal origin, and overlaid by arachnoid membrane. Glioependymal cysts are considered rare in humans and have been reported only once in animals. 20 Histologically, the walls of arachnoid cysts are formed from the splitting of the arachnoid membrane, with an inner and outer leaflet surrounding the cyst cavity. The outer wall of the cyst adheres loosely to the dura. The cyst wall is devoid of blood vessels, and inflammatory changes or hemorrhage seldom occurs. 1,7,9,14 The histologic composition of the cysts in the kitten and dog of the current report is consistent with arachnoid cysts. The inflammatory changes and hemorrhage seen in the Yorkshire Terrier were most likely a consequence of the concurrent necrotizing encephalitis. Given the location of the cysts, both would be categorized as QACs, an uncommonly reported lesion in veterinary medicine. Aside from one large case series of 28 dogs, 9 most reports of QACs in dogs have involved a few individuals. 6,8,10–12,18,19 Most of the previous reports, including the series of 28 cases, have characterized the cysts based on computed tomography or magnetic resonance imaging in live patients, and detailed descriptions of morphologic changes associated with QAC are lacking in veterinary medicine.
Human arachnoid cysts are usually thought to be congenital. 7 Microscopically, their walls are formed from splitting of the arachnoid membrane, with an inner and outer leaflet surrounding the cyst cavity, and may be secondary to a congenital deficiency within the arachnoidal trabeculae. 4,7,9,14 The fluid within the cysts is thought to be normal CSF. 3,4,6,7,9,14 Given the kitten's age and lack of contributing lesions, its QAC was thought to be congenital. The only previously published feline case of intra-arachnoid cyst formation was an extracranial spinal cyst that was thought to be congenital. 13
It is thought that the mechanism of acquired cyst formation often involves adhesion formation, rheologic disturbances in CSF flow, and/or abrupt changes in local CSF pressures. 3,9,14,21 Acquired arachnoid cysts have been seen in association with neoplasms, postsurgical adhesions, leptomeningitis, and hemorrhage. 3,9,14 Arachnoid cyst expansion most likely occurs because of intracranial pulsation pushing CSF through defects, which behave like valves. Intracranial tumors exemplify such a mechanism in which cysts develop as a consequence of CSF loculation surrounded by arachnoid scarring, with expansion due to osmotic filtration or via a ball-valve mechanism. 21 In some cases in humans and dogs, as well as in the canine case described herein, the cysts have been associated with concurrent necrotizing meningoencephalitides. 9 Although the meninges were not found to be affected, as is usually the case in Yorkshire Terriers with necrotizing encephalitis, 15 cyst formation may occur without direct inflammation of the meninges. Given the degree of brain parenchymal inflammation and necrosis, any or all of the aforementioned processes were likely in this patient.
In summary, the present report adds to the pathologic description of QAC associated with necrotizing encephalitis in dogs. The QAC in the kitten was thought to be congenital, and progressive accumulation of fluid led to expansion of the cyst and death. Conversely, the dog provided a classic example of a presumably acquired QAC, arising secondary to necrotizing encephalitis.