
Abstract
Hair follicle neoplasms occur in many different species, including humans. In domestic animals, they are most common in dogs. Most hair follicle tumors are benign, but malignant neoplasms can also occur. To diagnose hair follicle neoplasms, a thorough knowledge of follicular anatomy is important, given that follicular tumors are classified according to the differentiation pattern seen in the corresponding part of the normal hair follicle. This review focuses on the key diagnostic features of hair follicle tumors and follicular cysts in dogs and cats.
Introduction
Hair follicle (HF) tumors are common in dogs and cats and are frequently submitted to diagnostic laboratories. However, these cases rarely get transferred to teaching hospitals, and anatomic pathology residents may not be able to routinely diagnose hair follicle tumors and cysts. The diagnosis of HF neoplasms can be challenging given that some of these tumors have histologic features in common. This review focuses on the key diagnostic features of HF neoplasms and cysts to facilitate the diagnosis of these lesions. In cats, basal cell tumors are the most frequent skin tumors (~25%), of which the majority are apocrine ductular adenomas and trichoblastomas.1,22 Trichoepitheliomas and pilomatricomas are much rarer in cats (~4%). 1 In dogs, the frequency of hair follicle tumors is ~10%.18,27 Trichoblastomas are the most common HF tumors in dogs, followed by infundibular keratinizing acanthomas (IKAs), pilomatricomas, and trichoepitheliomas. 1 Tricholemmomas are rare in both dogs and cats. 1
Most HF tumors are benign, and surgical excision is curative. Rarely, HF neoplasms (i.e., trichoepithelioma and pilomatricoma) can be malignant and may metastasize. 16 To diagnose HF neoplasms and cysts, a thorough knowledge of follicular anatomy is important because these lesions are classified according to the differentiation pattern seen in the corresponding part of the normal HF.
Anatomy of the hair follicle
The HF is a mini-organ that goes through lifelong cycles of growth (anagen), regression (catagen), and rest (telogen). Two additional hair cycle stages are exogen (active shedding of the club hair) 32 and kenogen (hairless telogen). 37 Kenogen is increased in non-inflammatory alopecic disorders. 34 Anagen and telogen are the phases that are seen most commonly in healthy skin.
Anagen hair follicle
The anagen HF consists of 8 concentric layers, the outer root sheath (ORS), companion layer, inner root sheath (IRS; consisting of the Huxley layer, Henle layer, and IRS cuticle), and hair shaft (comprised of the hair cuticle, the cortex, and the medulla). 47 The anagen HF can be categorized into 3 major anatomic regions.
The
The
The
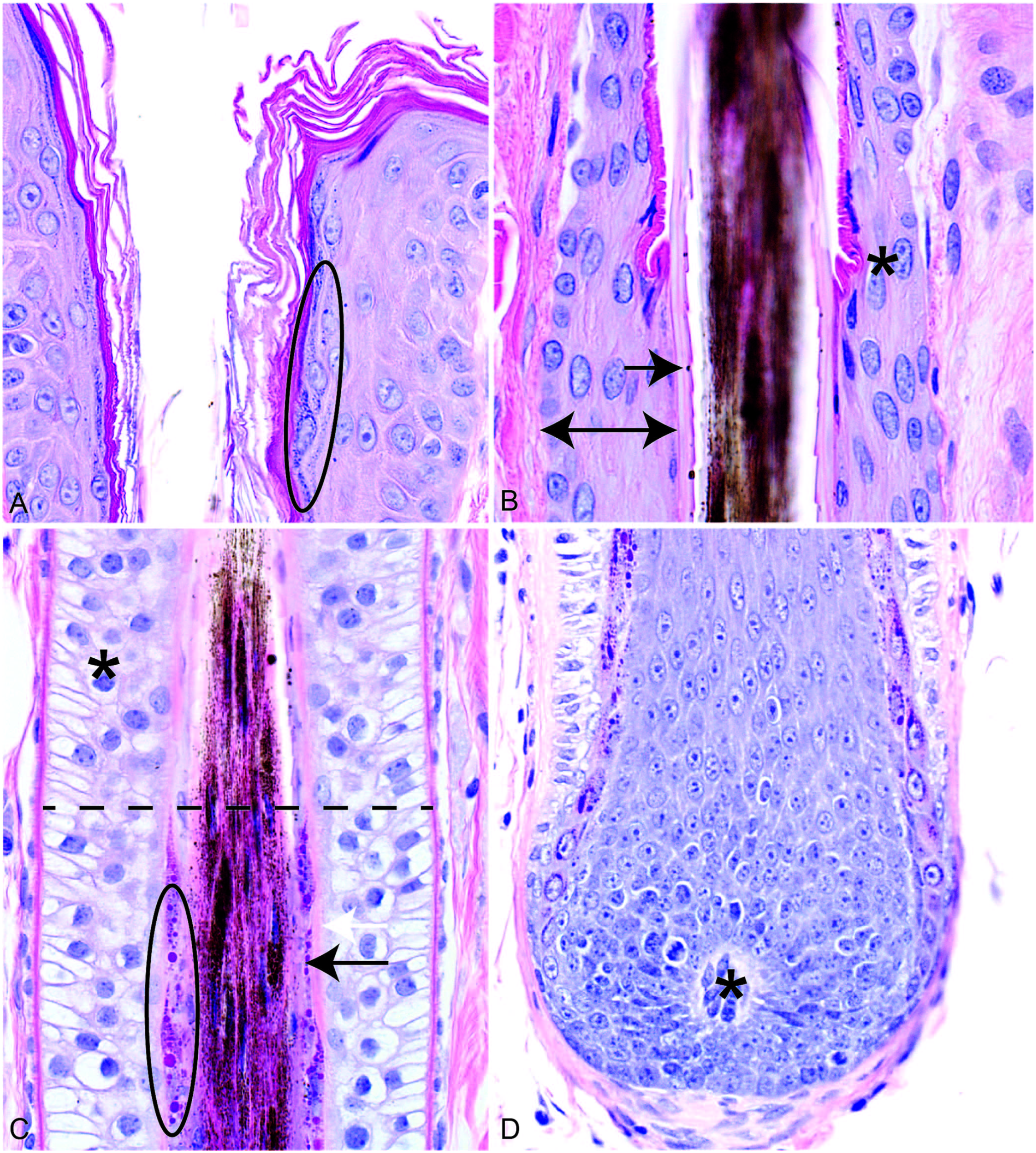
Anatomy of a canine anagen hair follicle.
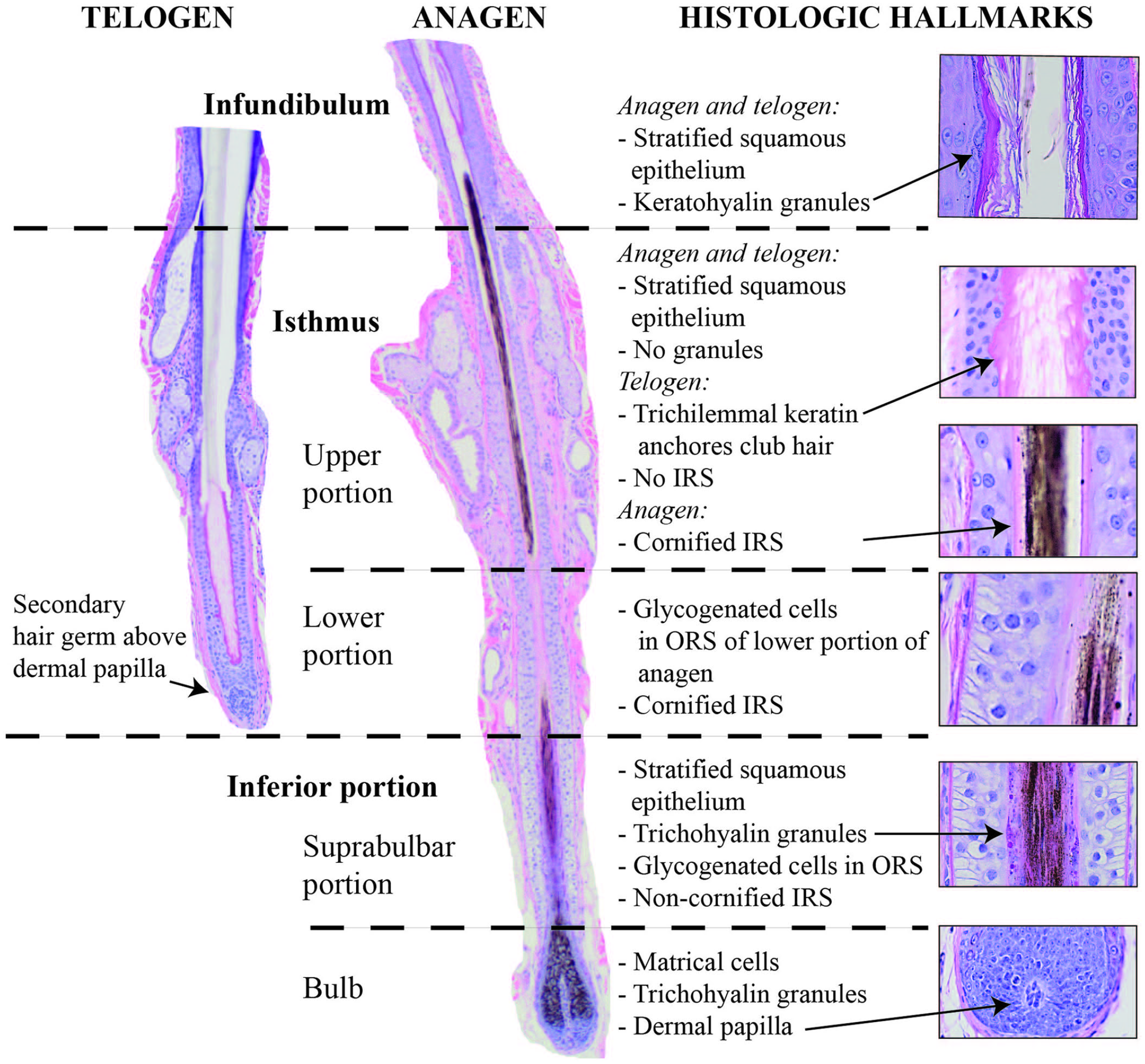
Summary of histologic hallmarks in canine telogen and anagen hair follicles. Note the opening of the sebaceous gland duct at the junction of the infundibulum and isthmus of both the telogen and anagen hair follicle. H&E. 10× (telogen) and 4× (anagen), respectively.
The infundibulum and isthmus constitute the permanent portion of the HF, whereas the inferior segment is transitory and undergoes regression during catagen and is absent during telogen.
Telogen hair follicle
The telogen HF consists of 2 main parts: the infundibulum and the isthmus. As mentioned above, in contrast to the anagen HF, the telogen HF does not have an inferior portion, and the telogen isthmus does not have an IRS. Instead, the club hair is anchored by trichilemmal keratin, protruding into the ORS (Fig. 2).
At the lower end of the telogen HF, there are epithelial cells called the secondary hair germ (Fig. 2), which serves as a repository for “primed,” short-term stem cells. The secondary hair germ is biologically and morphologically different from the cells forming the bulge in the isthmus. The cells are quiescent, but they start to proliferate at the beginning of anagen and give rise to transit-amplifying cells that surround the dermal papilla to form the bulb of the anagen HF.19,47
The dermal papilla, which is much less prominent in telogen compared to anagen, is located beneath the secondary germ.
Hair follicle neoplasms and stem cells
HF stem cells, which are present mainly in the bulge region in the isthmus, seem to play a role in the tumorigenesis of certain canine HF tumors.4 –6 Expression of cytokeratin (CK)15, a common stem cell marker expressed in the basal cell layer of the epidermis and the isthmic ORS, was compared in the most common HF neoplasms. 6 CK15 was expressed mainly in trichoblastomas, suggesting that these tumors originate from follicular stem cells or hair germ. Other tumors that expressed CK15 were trichoepitheliomas (mostly in areas with deep follicular differentiation and in basal cells in areas with squamous differentiation) and some tricholemmomas. 6
Interestingly, survivin, a member of the inhibitor of apoptosis proteins associated with tumor initiation and progression and maintenance of stem cells, 41 showed partial co-localization with CK15 in trichoepitheliomas and trichoblastomas, suggesting a role for survivin in the maintenance of cancer stem cells in these HF tumors. 5
Other common stem cell markers, namely LGR6, LGR5, and SOX9, had significantly higher mRNA expression levels in trichoblastomas compared to basal cell carcinomas (BCCs). These stem cell markers, especially LGR5, may therefore be useful in differentiating between these 2 tumors. 4 Furthermore, LGR6 and SOX9 mRNA seem to be more strongly expressed in malignant trichoepitheliomas, indicating that these stem cell markers may be used as markers of malignancy. 4 SOX9 is reported to be expressed in variable levels in all HF tumors, but was expressed most strongly in trichoblastomas. 14
In a 2018 study, all HF tumors could be characterized and differentiated with an isthmic and inferior stem cell marker panel (CK8, CK15, CK19, and CD34), except pilomatricomas, in which most tumor cells had a strong expression of p63. 26 In a hierarchical cluster analysis, HF tumors clustered in 3 distinct groups. One cluster included tumors derived from the inferior or lower isthmic segment (inferior tricholemmoma, malignant trichoepithelioma, trichoepithelioma, and pilomatricoma) and another cluster had tumors derived from the middle isthmic segment (IKA and isthmic tricholemmoma). Trichoblastomas did not cluster with any of these groups and formed a separate cluster, composed of undifferentiated, germinative epithelial cells that strongly expressed all evaluated stem cell markers (CK8, CK15, CK19, and CD34), further corroborating the stem cell or hair germ origin of trichoblastomas. 26 However, in routine diagnostic work, all of the above-mentioned markers are not commonly used to differentiate between the different HF tumor types, and diagnoses are based mainly on histologic features.
Hair follicle neoplasms
Most HF tumors are considered benign, and metastases have not been reported. In rare cases, trichoepitheliomas and pilomatricomas can be malignant with metastases to various organs. In the following, tumors are grouped based on their location of origin in the HF (Table 1).
Summary of the main histologic features of the most common presentation of hair follicle tumors. Note that epidermal contiguity may be affected by plane of section.
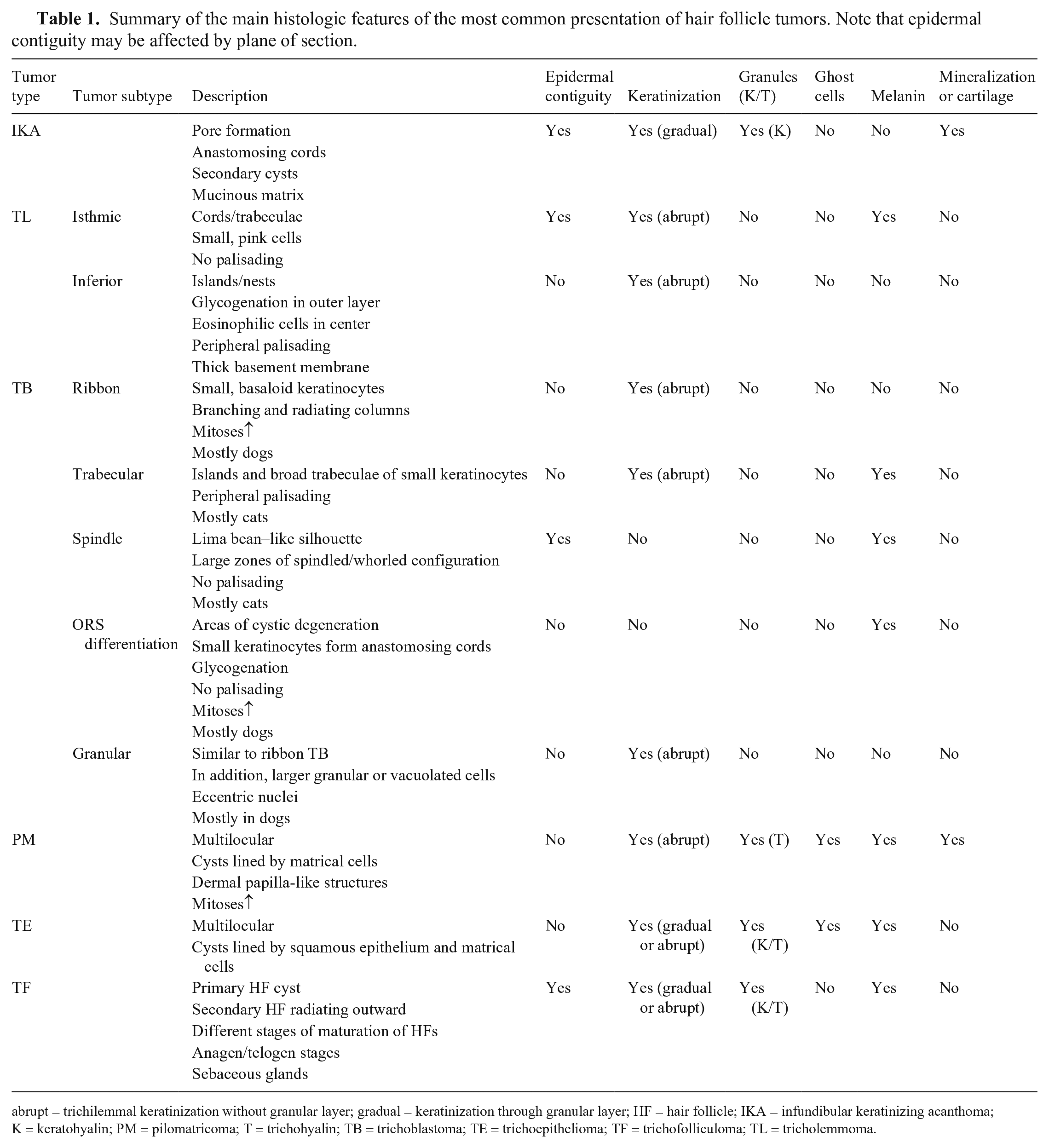
abrupt = trichilemmal keratinization without granular layer; gradual = keratinization through granular layer; HF = hair follicle; IKA = infundibular keratinizing acanthoma; K = keratohyalin; PM = pilomatricoma; T = trichohyalin; TB = trichoblastoma; TE = trichoepithelioma; TF = trichofolliculoma; TL = tricholemmoma.
Infundibulum
Infundibular keratinizing acanthoma (intracutaneous cornifying epithelioma)
Clinical findings
The dog is the only species affected. 16 IKAs appear as partially alopecic, variably sized nodules that usually have a central pore from which keratinaceous material can be expressed. Larger nodules may form a cutaneous horn.16,20,28,30 Spontaneous regression does not occur. 20
Breed and age predilection
Norwegian Elkhounds have a marked predilection, but other commonly affected breeds include the Tibetan Terrier, Bedlington Terrier, Kerry Blue Terrier, and Pekingese.16,28 Young, male Norwegian Elkhounds and Keeshonds are predisposed to having numerous nodules (in some cases, there may be 40–50 nodules). Multiple IKAs are also reported in German Shepherds, Lhasa Apsos, and Old English Sheepdogs.16,28 A peak incidence is reported at 4–10 y. 16
Location
The most common locations of IKAs are dorsal neck, back, and tail, but these tumors may occur anywhere.28,30 Subungual lesions may also occur. 30
Histopathologic findings
IKAs are well-demarcated, dermal, cup-shaped lesions, consisting of a cyst that is filled with lamellar, concentric keratin, and has a central pore opening to the epidermal surface (Fig. 3A). When located within the deeper dermis and subcutis, IKAs may not have a pore opening. Trabecular, anastomosing projections of the epithelium extend downward from the cyst wall and form small keratinaceous cysts in later lesions (Fig. 3B). These secondary cysts may interconnect with anastomosing trabeculae, either in a double row of basaloid cells or in broader trabeculae with squamous epithelium in the center and basaloid cells in the periphery (Fig. 3B, 3C). Cellular and nuclear polymorphism is minimal. The surrounding stroma is mucinous, giving a pale blue background (Fig. 3C). The cyst wall consists of squamous, stratified, glassy epithelium with keratohyalin granules (infundibular differentiation; Fig. 3D). The outline of the cyst compresses adjacent collagen, forming a pseudocapsule, but there is no invasion into the surrounding tissue. Occasionally, there is cartilaginous or osseous metaplasia, which may be marked in some cases resulting in atrophy of the epithelial component (Fig. 3E, 3F).17,20 The cysts may rupture, resulting in a secondary pyogranulomatous inflammation, which may give the owner the impression that the nodule is growing rapidly.16,20,30 Subungual IKAs should not be confused with nailbed keratoacanthomas, given that these tumors have a different morphology and biological behavior. 21 In contrast to IKAs, nailbed keratoacanthomas do not have a granular cell layer, usually have large zones of parakeratin, and apoptosis may be a prominent feature. Nailbed keratoacanthomas are usually associated with lysis of the third phalanx, but the tumor does not infiltrate into the underlying bone.16,21
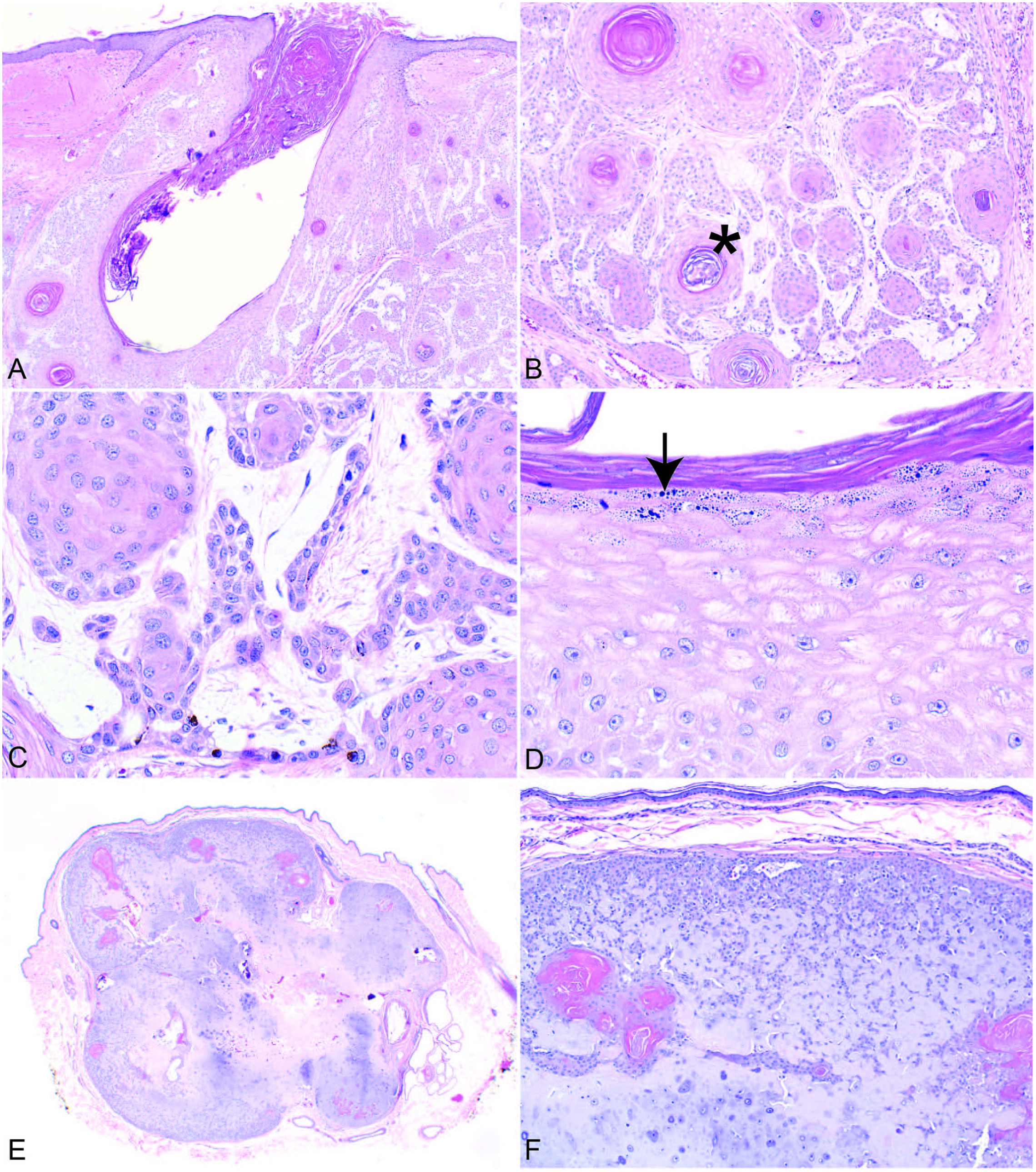
Canine infundibular keratinizing acanthoma.
Differential diagnosis
The main differential diagnosis for IKAs is an inverted papilloma. Inverted papillomas have papillary projections from the cyst wall as opposed to small keratinaceous cysts of IKAs. Also, there are no intranuclear viral inclusion bodies in IKAs, and testing for papilloma virus is consistently negative. 20
IKAs without a pore-opening to the epidermis may need to be differentiated from trichoepitheliomas and tricholemmomas. Trichoepitheliomas usually have both squamous and matrical epithelial cells, and may show ghost cells. Tricholemmomas have only a few cysts, epithelial cells are eosinophilic, and there are no granules.
IKAs may look similar to squamous cell carcinomas (SCCs), especially when the tumors are small and only the edge of the tumor is available for evaluation. SCCs typically are less well demarcated, and they are invasive and have increased cellular pleomorphism. Assessment of cellular proliferation may aid to differentiate well-differentiated SCCs from IKAs, given that these tumors have different proliferative behavior, which may be assessed by methods such as MIB1 immunohistochemistry and AgNOR staining. 13
Isthmus
Tricholemmoma
Clinical findings
Tricholemmomas are rare HF tumors in dogs and even more rare in cats, in which only isthmic types are reported. 30 The tumor usually appears as a firm, circumscribed, dome-shaped, alopecic nodule, of variable size.20,28
Breed and age predilection
Afghan Hounds may be predisposed, 28 and the tumor tends to occur in animals 5–13 y old (average 10 y old),20,28 although too few cases have been reported to establish age, breed, or sex predilections.
Location
Tricholemmomas seem to occur most often on the head and neck. 28 However, too few cases have been described to establish a clear site predilection.
Histopathologic findings
Tricholemmomas are well-demarcated, non-encapsulated tumors with a low mitotic rate. There are 2 types, the isthmic and the inferior or bulb type. Neither type has keratohyalin or trichohyalin granules. The histopathologic findings of the inferior tricholemmoma are described under inferior portion below.
Isthmic tricholemmoma
The isthmic tricholemmoma shows differentiation to the ORS of the isthmus segment and is composed of small, eosinophilic keratinocytes with slightly glassy cytoplasm. Cords and trabeculae of epithelial cells radiate outward from large epithelial islands and often interconnect. Peripheral palisading is not a prominent feature. There may be large keratinaceous cysts or areas forming pseudocysts as a result of drop-out of central keratin. 20 The stroma may be mildly mucinous. There is usually contiguity with the epidermis. The center of the islands may have small foci of tricholemmal keratinization. Melanization may be present and can be heavy.16,20,30 A case of a desmoplastic tricholemmoma with an intense stromal reaction and multifocal acantholytic cells has been reported. 25
Differential diagnosis
Isthmic tricholemmomas may have features similar to IKAs; however, there is no pore-forming opening, multiple secondary keratinaceous cysts, or abundant mucinous stroma. IKAs have larger keratinocytes with a paler cytoplasm, and there are keratohyalin granules, whereas isthmic tricholemmomas have trichilemmal keratinization without a granular cell layer.
Trabecular trichoblastomas can be differentiated from isthmic tricholemmomas by prominent palisading of cells and multifocal spindling of cells. 20
Hair germ
Trichoblastoma
Trichoblastomas are derived from the primitive hair germ of embryonal follicular development.6,16,20,28,30 In cats, they were previously called basal cell tumors, a category that also included benign and malignant apocrine gland ductular tumors and BCCs. 20
Clinical findings
Trichoblastomas are common tumors of variable size in dogs and cats. The lesions are frequently pigmented and can be difficult to differentiate from melanocytic tumors clinically. 20 In dogs, they usually appear as solitary, dome-shaped, or polypoid alopecic nodules.
A case of multiple trichoblastomas was reported in a dog, which was successfully treated with surgical excision and chemotherapy (doxorubicin). 8 In cats, polypoid tumors are uncommon. 20
Breed and age predilection
Poodles, Cocker Spaniels, and mixed-breed dogs appear to be predisposed. 20 Increased occurrence of trichoblastomas has also been reported in Kerry Blue Terriers, Siberian Huskies, Shetland Sheepdogs, Bichon Frisés, Pulis, Bedlington Terriers, and Cockapoos.16,20
Peak incidence is reported in dogs 4–10 y old.16,20 Male dogs seem to be slightly predisposed. 16 In cats, there is no known breed or age predilection. 20
Location
Trichoblastomas are reported to occur most commonly on the head and neck, especially at the base of the ear. In cats, the most common location is on the head and the cranial half of the trunk.16,20
Histopathologic findings
Trichoblastomas are well-demarcated, non-encapsulated, benign tumors (Fig. 4A, 4C, 4E, 4G). Five subtypes are described. In all of the subtypes, small clusters of mesenchymal cells may be seen in the stroma close to the epithelial neoplastic cells, resembling dermal papillae (follicular papillary mesenchymal bodies).7,20 A solid trichoblastoma is described by some pathologists. 16
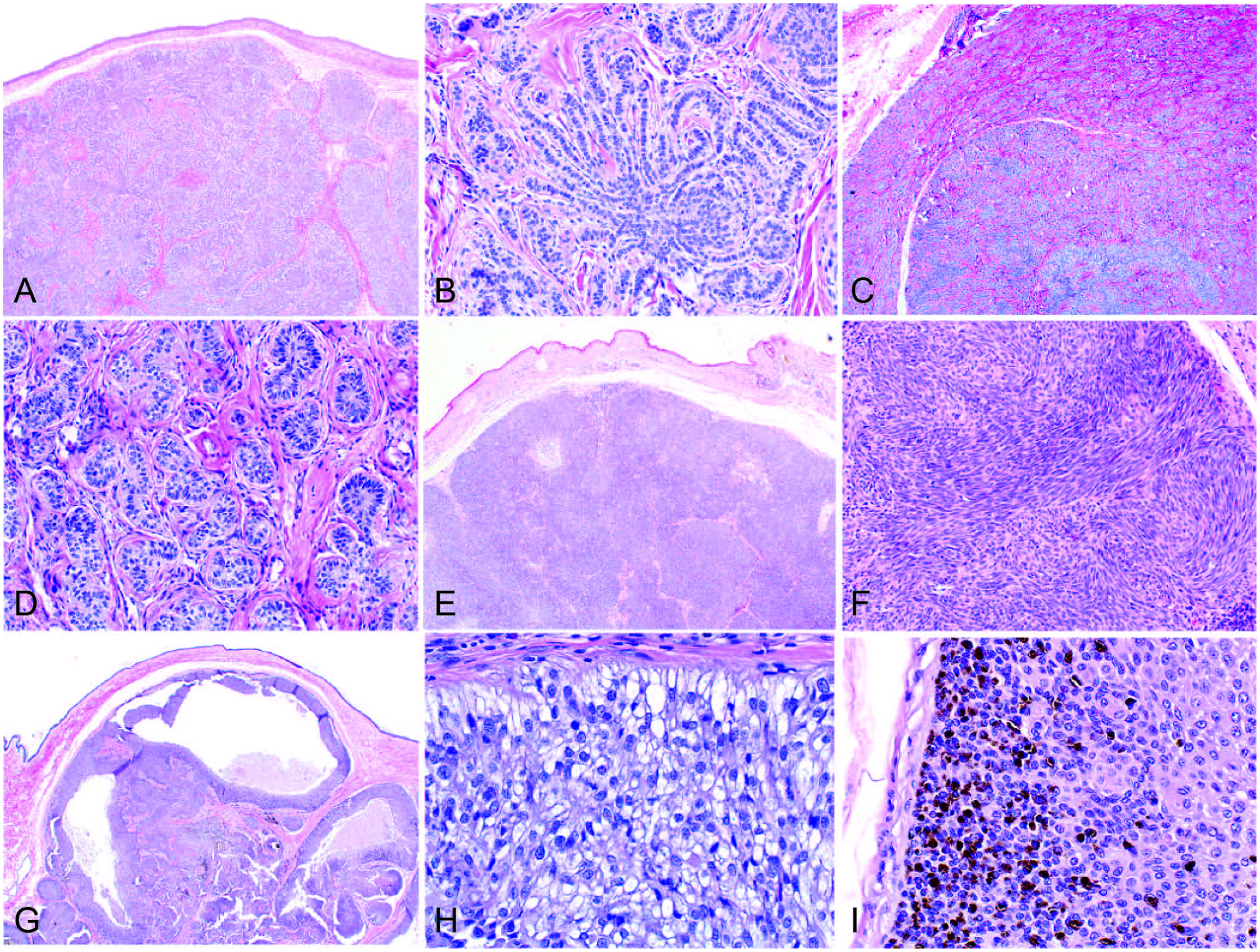
Trichoblastoma.
Ribbon or medusoid trichoblastoma
This is the most common subtype in dogs and is composed of small, basaloid keratinocytes arranged in branching and radiating columns, usually 2–3 cells in width (ribbon trichoblastoma).16,20 Nests of epithelial cells with radiating columns give the impression of a medusoid arrangement (medusoid trichoblastoma; Fig. 4B). Neoplastic cells have a small amount of eosinophilic cytoplasm with a nucleus that is perpendicular to the columnar structure of the tumor. Mitotic figures may be infrequent to numerous.16,20 In dogs, the tumor is supported by abundant stroma that ranges from fibrous to hyalinized to mucinous, whereas, in cats, the stromal component is sparse. 20 One case report describes a trichoblastoma with a proliferation of plump peritumoral stromal cells. 33 Melanization is uncommon. Occasionally, hair shafts can be seen within small HF structures in the periphery of the tumor, and there may be areas of keratinization. No contiguity with the epidermis is present. 20 Feline ribbon trichoblastomas are rare.
Differential diagnosis
Some canine ribbon trichoblastomas have nests of glycogenated cells resembling the inferior tricholemmoma, but this feature does not compromise most of the tumor. Merkel cell carcinoma may have a cord-like pattern resembling ribbon trichoblastomas. Merkel cell carcinomas can be differentiated from trichoblastomas by positive immunolabeling of tumor cells with CK20, chromogranin A, synaptophysin, and neuron-specific enolase.20,24
Trabecular trichoblastoma
This is the most common subtype in cats, and it occurs occasionally in dogs. This subtype is composed of islands and broad trabeculae of small keratinocytes with prominent peripheral palisading (Fig. 4D). Cells in the center of epithelial nests usually have a slightly larger amount of cytoplasm. The surrounding stroma is usually sparse with few cells, and may be mucinous.20,30 Keratinized microcysts may be seen, but trichogenesis, as seen in the ribbon subtype, is not a prominent feature. Spindling of keratinocytes is a common feature in cats. Melanization can be present with a patchy distribution. 20 Epidermal contiguity is minimal.20,30
Differential diagnosis
Trabecular trichoblastomas can be differentiated from isthmic tricholemmomas by peripheral palisading and lack of glassy keratinocytes with an eosinophilic cytoplasm. Trabecular trichoblastomas can be differentiated from inferior tricholemmoma by lack of small, clear cells. Merkel cell carcinoma may have a trabecular and cord-like pattern resembling trabecular trichoblastomas. Merkel cell carcinomas can be differentiated from trichoblastomas by lack of peripheral palisading and by positive immunolabeling of tumor cells with CK20, chromogranin A, synaptophysin, and neuron-specific enolase.20,24
Spindle trichoblastoma
This subtype occurs most commonly in cats. The tumor frequently has a lima bean–like silhouette with a central indentation, a broad epidermal connection, and ulceration. 20 The tumor consists of basaloid epithelial cells arranged in islands, nests, and short trabeculae. Peripheral palisading is not a prominent feature. There are large zones of cells with elongated cytoplasm in an interwoven pattern, giving the impression of a spindled and whorled configuration (Fig. 4F). Cells have a small amount of cytoplasm and a round-to-oval nucleus with inconspicuous nucleoli. Larger cell aggregates may have central necrosis. Mitotic figures are few. The surrounding stroma is scant and paucicellular, and mucin is present occasionally in the center of the neoplasm. Melanization can be present. Squamous differentiation or keratinization is rare.
Differential diagnosis
Given the broad connection of spindle trichoblastoma with the epidermis, BCC must be included in the differential diagnosis. BCC is more plaque-like with an irregular silhouette, spindling is less extensive, and the mitotic rate is higher. Additionally, the stroma of BCCs is more cellular and abundant and reaches beyond the epithelial component of the tumor. 20
Trichoblastomas with ORS differentiation
This subtype of trichoblastoma is composed of multiple lobules, trabeculae, and areas of cystic degeneration as a result of acantholysis and drop-out of keratinocytes (Fig. 4G). Keratinization is not a feature. Similar to ribbon trichoblastoma, small keratinocytes form anastomosing cords. These cords merge into small islands of cells with glycogenated cytoplasm and no peripheral palisading (Fig. 4H) or into trabeculae consisting of small cells with eosinophilic cytoplasm lining the cystic zones, similar to isthmic tricholemmoma cells. The nuclei of neoplastic cells are larger and more vesicular than the cells in the ribbon trichoblastoma. The mitotic rate can vary from low to fairly high. The surrounding stroma is sparse, paucicellular, and may be mucinous. Epidermal connection and ulceration are not present. Melanization is common (Fig. 4I). 20
Differential diagnosis
The main differential diagnosis is a solid-cystic apocrine ductular adenoma, which has a similar silhouette with cystic centers. This tumor has tubular structures lined by a double row of cells and foci of squamous differentiation with keratinization and keratohyalin granules, features that are lacking in trichoblastoma with ORS differentiation. 20
Granular cell trichoblastoma
This subtype is rare and seen most commonly in the dog. Granular cell trichoblastomas are similar to ribbon trichoblastomas, but some epithelial aggregates are composed of larger cells with abundant finely granular or vacuolated cytoplasm and small eccentric nuclei. 20 Mitotic figures are infrequent, and the amount of surrounding stroma may vary. 16 A report describes the absence of A1/A3 cytokeratin immunolabeling in the granular cells and positive labeling in the surrounding epithelial cells. 2
Differential diagnosis
The main differential diagnosis is granular-cell BCC. 44 Unlike granular cell trichoblastoma, granular-cell BCCs lack a ribbon-like configuration, have an epidermal connection, and display features of malignancy. Granular cell trichoblastomas may have clear cells, similar to bulb tricholemmomas; however, bulb tricholemmomas lack the eccentric nuclei seen in granular cell trichoblastomas. 20
Inferior portion
Tricholemmoma
Inferior tricholemmoma
For clinical findings, breed predilection and location, please see above under isthmic tricholemmoma. The inferior tricholemmoma has lobular groupings with small cells arranged in islands, nests, and delicate trabeculae (Fig. 5A, 5B). Cells in the outer layer of tumor nests have clear cytoplasm, and there is prominent peripheral palisading. The pallor of these cells is the result of cytoplasmic, periodic acid-Schiff–positive glycogen storage that represents differentiation to the ORS cells of the hair bulb. Toward the center, cells have more intensely eosinophilic cytoplasm. Each tumor aggregate is surrounded by a thick, eosinophilic, glassy basement membrane, similar to the vitreous sheath of the normal HF (Fig. 5B, arrow). Small foci of trichilemmal keratinization may be seen. Similar to the isthmic tricholemmoma, the surrounding matrix may be mildly mucinous. There is no contiguity with the overlying epidermis.
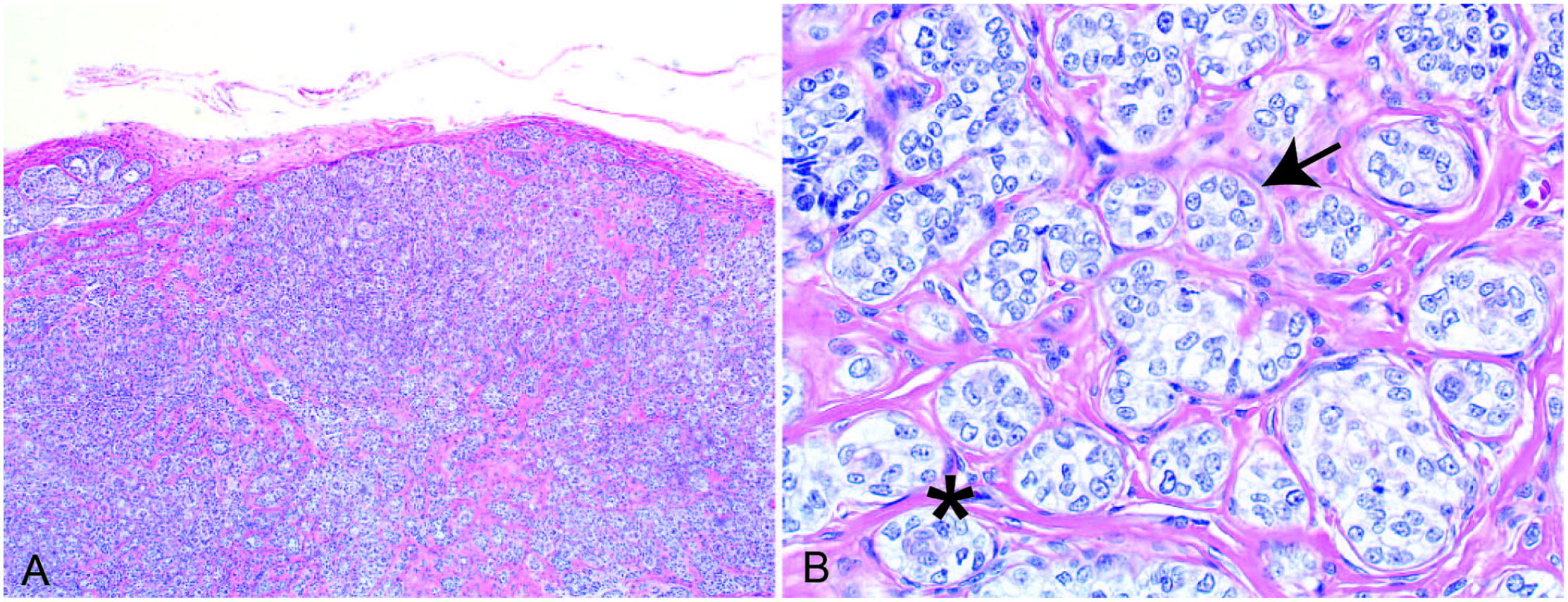
Canine inferior tricholemmoma.
Differential diagnosis
Inferior tricholemmomas can have morphologic features similar to granular trichoblastomas and clear-cell BCCs. Unlike inferior tricholemmomas, granular trichoblastomas form cords rather than islands, and the nuclei are peripherally displaced. Clear-cell BCCs generally have larger tumor cell aggregates than inferior tricholemmomas. Additionally, they have larger cells with features of malignancy and an association with the epidermis.20,30 Inferior tricholemmomas can be differentiated from trabecular trichoblastomas by the presence of small cells with clear cytoplasm.
Pilomatricoma
Clinical findings
Pilomatricomas are benign neoplasms that arise from the hair matrix of the hair bulb, and are uncommon in the dog and rare in the cat. They usually appear as solitary, firm, often alopecic and sometimes ulcerated, dome-shaped to plaque-like nodules of variable size. Some are cystic or pigmented. Mineralization within the lesion may make pilomatricomas difficult to cut.16,20
Breed and age predilection
Kerry Blue Terriers are highly predisposed. 16 Higher incidence is also reported in Old English Sheepdogs, Standard Poodles, Soft-coated Wheaten Terriers, Airedale Terriers, Bouvier des Flandres, Bichon Frisés, Standard Schnauzers, and Basset Hounds.16,20 Breeds with a continuously growing hair coat and anagen predominance seem to be more affected.20,30 Most occur in dogs 5–10 y old.20,28 No sex-predilection is reported.
Location
Pilomatricomas most commonly occur on the proximal pelvic limbs, thorax, dorsal trunk, neck, and tail.16,20,28 The tumors may be difficult to transect because osseous metaplasia is frequently present.
Histopathologic findings
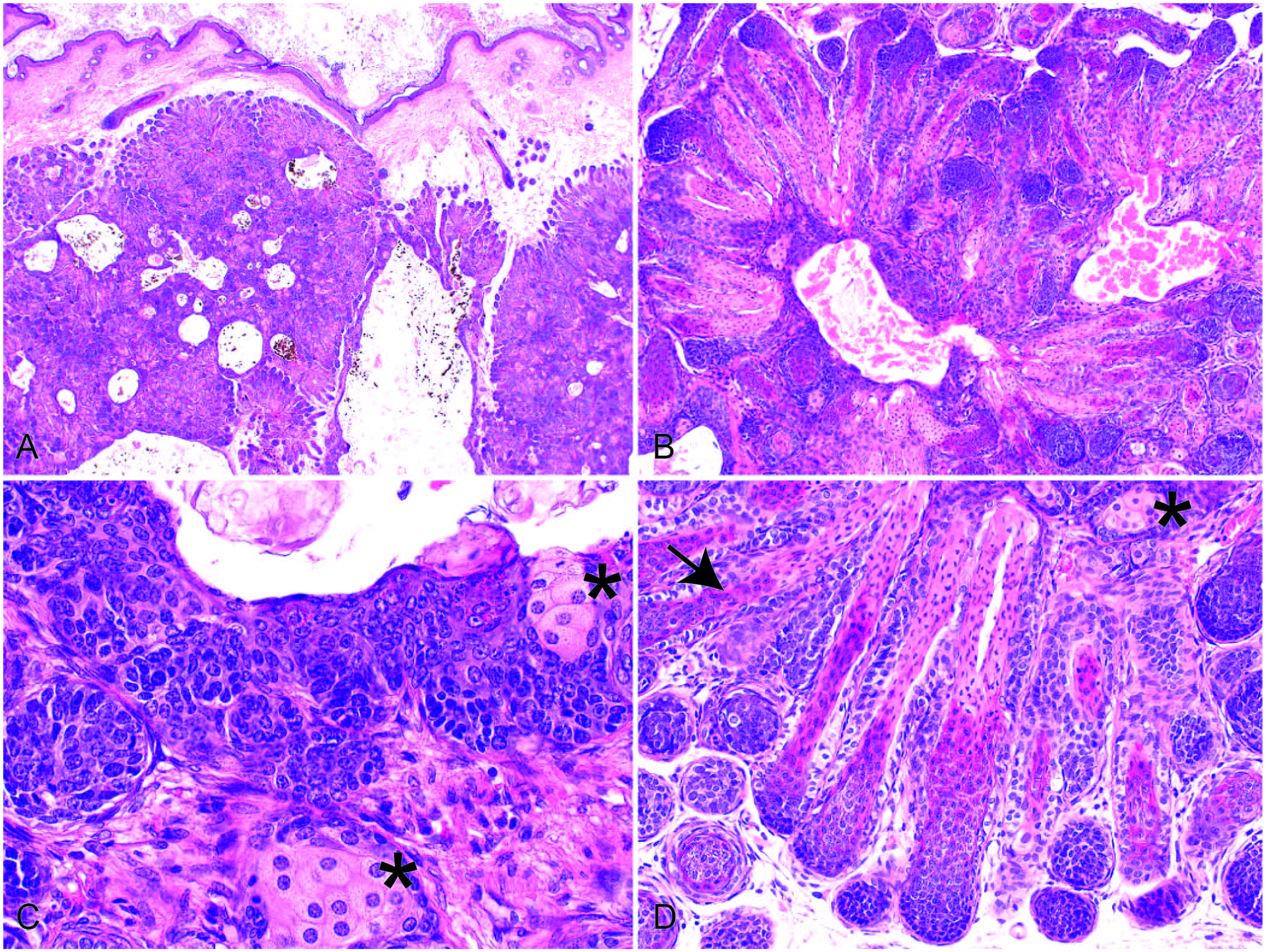
Pilomatricoma is a well-circumscribed dermal and/or subcutaneous tumor composed of multiple cystic structures of variable size, lined by small, basaloid cells resembling matrical cells of the anagen bulb (Fig. 6A). Nuclei are large and hyperchromatic with inconspicuous nucleoli. Small dermal papilla-like structures may be present within the cyst wall. Trichohyalin granules, indicating IRS differentiation, are usually present. The cells frequently exhibit high mitotic activity, but the tumor is considered benign with rare exceptions. The cyst-like structures show abrupt keratinization without a granular cell layer (Fig. 6B). Within cyst lumina, there are frequent ghost cells (or shadow cells), characterized by large amounts of eosinophilic cytoplasm and a central empty space instead of a nucleus, representing matrical differentiation (Fig. 6B). 16 Frequently, ghost cells undergo dystrophic mineralization within the cyst lumina and some progress to osseous metaplasia, particularly in later stages. Amyloid may be found in the center of lobules. Melanization may be present and can be striking. Small areas of squamous epithelium with a granular cell layer may be seen, but cysts are not primarily lined by squamous epithelium. The surrounding stroma is sparse and paucicellular, and may be mucinous. 20 At the periphery of the tumor, there may be a rim of small, basophilic cells with an increased mitotic rate, but the tumor is still considered benign. 16 Long-standing tumors may consist mainly of ghost cells and mineralization or osseous metaplasia with only a small rim of basaloid cells.16,20 There is no contiguity with the overlying epidermis.
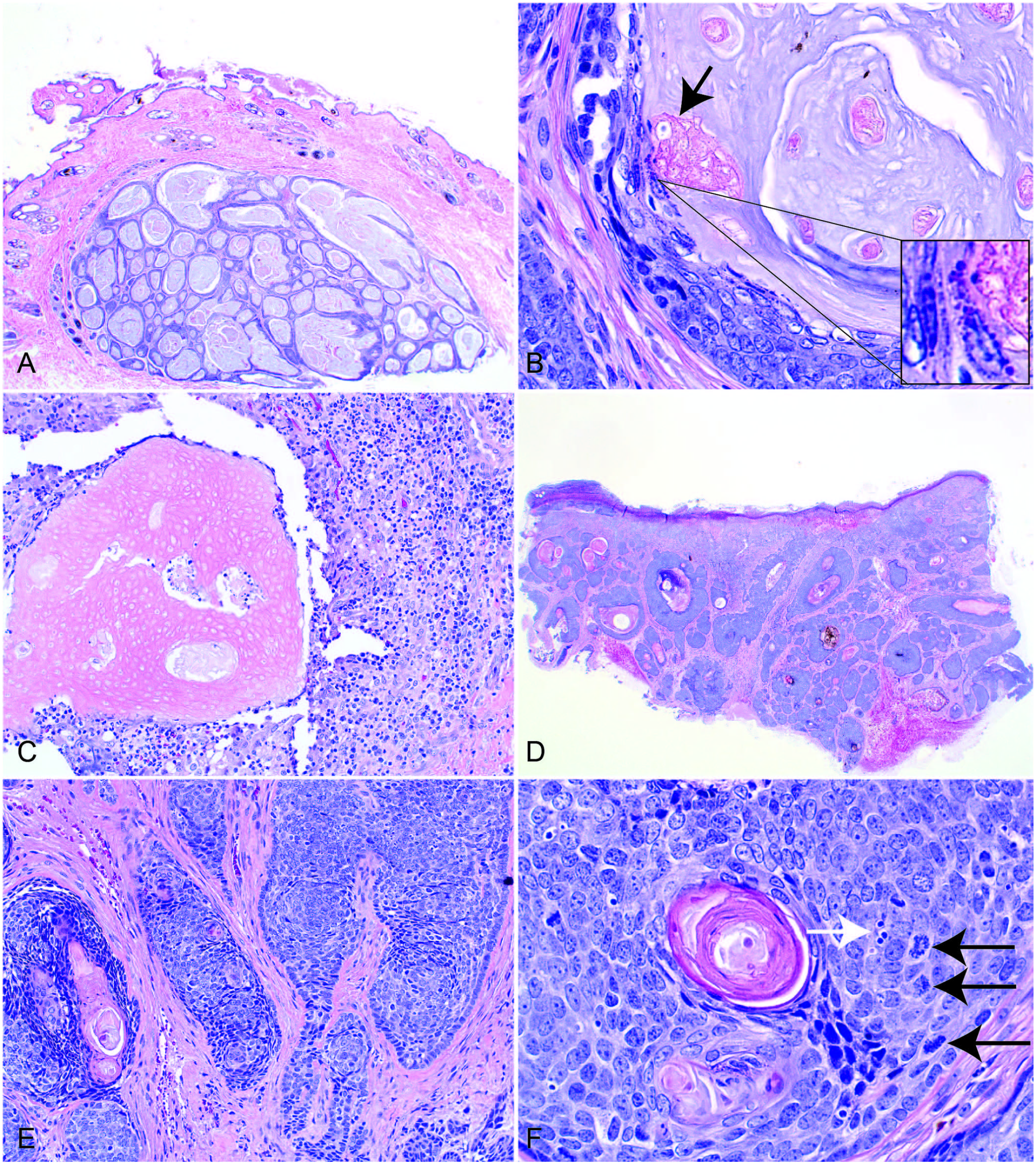
Canine pilomatricoma.
Rupture of the pilomatricoma frequently evokes a granulomatous inflammatory response, and the only indication of a tumor in some cases is an accumulation of ghost cells surrounded by granulomatous inflammation with fibrosis (Fig. 6C).20,30
One report describes a tumor with a similar cell population as pilomatricoma (basaloid and ghost cells) but with an additional melanocytic cell population, and this lesion was termed melanocytic matricoma. 42
Differential diagnosis
The main differential diagnosis for pilomatricomas are trichoepitheliomas, keratinizing BCCs, and matrical cysts.
Trichoepitheliomas generally have smaller cysts, which are frequently lined by squamous epithelium with keratohyalin granules, whereas pilomatricomas have only rare foci of squamous epithelium with a granular layer. Mineralization is rare in trichoepitheliomas but frequent in pilomatricomas.
Keratinizing BCCs have a broad connection to the epidermis, which is lacking in pilomatricomas. Furthermore, BCCs have higher cellularity and exhibit signs of malignancy with nuclear and mitotic atypia and invasive borders.
Matrical cysts are unilocular as opposed to the often multilocular appearance of pilomatricomas.
Rare malignant forms of pilomatricomas (matrical carcinoma, pilomatrix carcinoma) are described in dogs. These tumors have histologic features similar to their benign counterpart, but they are poorly circumscribed and frequently invade the dermis and subcutis (Fig. 6D, 6E). Other features include an increased ratio of basaloid cells to keratinized ghost cells, nuclear and cellular pleomorphism, mitotic atypia, increased mitotic rate, and desmoplasia (Fig. 6E, 6F). Nuclei may be less basophilic. 17 Lymphatic invasion may also occur. Some of these neoplasms are contiguous with the epidermis. Ulceration and areas of necrosis are common. Reported cases had distant metastasis to a variety of organs, including bone, lung, liver, spleen, kidney, and the central nervous system.3,9,12,23,29,31,39,40,46 Too few cases are reported to determine if there is a breed or sex predilection.16,20,30
A rare subset of malignant pilomatricoma, cutaneous pilomatrical carcinosarcoma, has been described in a dog. This tumor consisted of 2 malignant cell populations, sarcomatous and pilomatrical. 38
Differential diagnosis
Differentiation between malignant pilomatricoma and malignant trichoepithelioma may be impossible. Mineralization or ossification is not a feature of malignant trichoepitheliomas. 20
All 3 segments of the hair follicle
Trichoepithelioma
Clinical findings
Trichoepitheliomas are common neoplasms in the dog and uncommon in cats.16,20,45 Most commonly, trichoepitheliomas appear as alopecic, firm, white-to-gray, multilobulated masses that may become ulcerated. The location of the tumor varies from superficial to deep dermal or subcutaneous. Superficial tumors are often dome-shaped. The masses are usually <2 cm in diameter, but occasional lesions are large and ulcerated.16,20,30 Trichoepitheliomas are usually single tumors but ~7.5% are multicentric, especially in Basset Hounds. 16
Breed and age predilection
Among dogs, Basset Hounds are the most predisposed breed. Predisposition is also reported in the Golden Retriever, Soft-coated Wheaten Terrier, Bull Mastiff, English Springer Spaniel, Gordon Setter, Irish Setter, German Shepherd, Miniature Schnauzer, and Standard Poodle.16,20,28 Most dogs are 5–11 y old. Spayed female dogs seem to be predisposed.16,20
Among cats, Persians may be predisposed, and animals are usually 4–11 y old.16,28
Location
In dogs, tumors are often located on the dorsal trunk, thorax, neck, tail, and limbs, but they may occur anywhere.16,20 In cats, lesions are more common on the head, tail, and limbs. 28
Histopathologic findings
At low magnification, trichoepitheliomas may be impossible to differentiate from pilomatricomas. Trichoepitheliomas are well-circumscribed, usually non-infiltrative, unencapsulated tumors consisting of epithelial islands and cystic structures of variable size that show differentiation toward all 3 of the follicular segments (Fig. 7A). Accordingly, they have specific structures such as keratohyalin and trichohyalin granules (as features for infundibular differentiation and IRS of the inferior portion, respectively) as well as epithelium with squamous and matrical differentiation. The cysts are lined by either squamous epithelium that may show keratohyalin granules and/or by small, basaloid cells resembling matrical cells with multifocal trichohyalin granules (Fig. 7B–D). The outer layer of basaloid cells is usually palisaded. There may be transitional zones with larger cells with vacuolated, glycogenated cytoplasm (lower isthmic and inferior ORS differentiation). Keratinization may be gradual or abrupt with lamellar, infundibular, or amorphous trichilemmal keratinization, respectively. In the lumina of the cyst-like structures, ghost cells are present, indicating matrical keratinization (Fig. 7D). Islands of epithelial cells and cystic structures may be surrounded by a thick, eosinophilic, hyalinized basement membrane, representing the vitreous sheath. Similar to pilomatricomas, matrical and ghost cells may be melanized. Mitotic activity is variable in the matrical cell population, ranging from low to fairly high and absent in the non-basaloid areas. Inflamed trichoepitheliomas may have a higher mitotic rate. 20 The surrounding stroma is sparsely cellular, can be abundant, and may be collagenous or mucinous. Recognizable hair shafts and papillary mesenchymal bodies are uncommon. Contiguity with the epidermis is focal or not present.
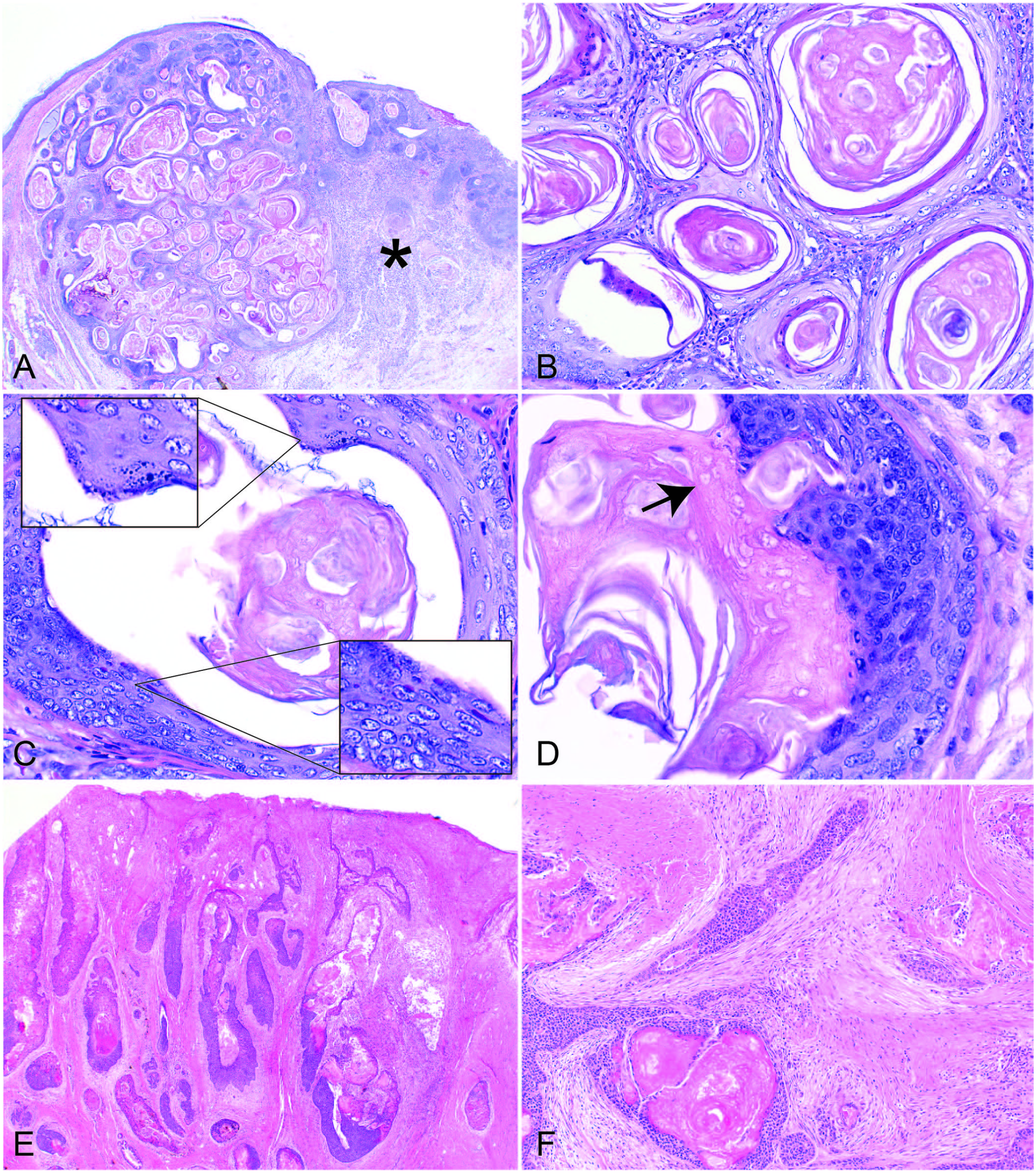
Canine trichoepithelioma.
Rupture of the tumor can evoke a granulomatous inflammatory response, and dystrophic mineralization may occur occasionally in these foci, but mineralization and osseous metaplasia are not prominent features.16,20,30
Differential diagnosis
The main differential diagnosis is benign pilomatricoma, which usually has larger, but fewer, cystic structures. Mineralization and osseous metaplasia are frequent in pilomatricomas, whereas they are rare in trichoepitheliomas. Areas with squamous epithelium with keratohyalin granules are rare in pilomatricomas and will not primarily line cystic structures as in trichoepitheliomas.
IKAs have a predominance of keratinocytes with glassy, pale cytoplasm, a feature not seen in trichoepitheliomas.
Predominantly basaloid trichoepitheliomas may have to be differentiated from malignant pilomatricomas and keratinizing BCCs. The nuclear and mitotic atypia, invasive behavior, and desmoplasia of these malignant tumors usually allow differentiation from trichoepithelioma. Keratinizing BCC has broad contiguity with the epidermis, is plaque-like, and lacks large cystic structures.
Rare malignant forms of trichoepitheliomas are described in dogs. Spayed females and the Basset Hound and Airedale Terrier breeds may be predisposed. Older dogs 8–12 y old are affected most often. 16
Malignant trichoepitheliomas have a morphology similar to their benign counterparts, but they are generally larger, asymmetrical, poorly circumscribed, and invasive (Fig. 7E). Epithelial necrosis, nuclear and cellular pleomorphism, atypical mitoses, and lymphatic invasion may be seen. 17 Desmoplastic stroma is present at the periphery of the tumor (Fig. 7F). Ulcerated, benign trichoepitheliomas may have fibrosis as a result of ulceration, which can be difficult to differentiate from desmoplasia caused by a malignant tumor. However, benign trichoepitheliomas do not have features of malignancy as described above. Focal and multifocal contiguity with the epidermis is often observed. 20 Metastasis to regional lymph nodes and lungs has been described. 16
Differential diagnosis
Differentiation between malignant trichoepithelioma and malignant pilomatricoma may be impossible. The epithelial aggregates are usually larger in malignant pilomatricoma.
Inflamed benign trichoepitheliomas have a more distinct silhouette, epidermal connection is rare, and areas of proliferative activity and reactive squamous metaplasia are always associated with areas of inflammation.
Differentiation between keratinizing BCC and malignant trichoepithelioma may be challenging. Keratinizing BCC has broad contiguity with the epidermis, is plaque-like, and lacks large cystic structures. 20 In addition, keratinizing BCCs lack trichohyalin granules or IRS differentiation, and matrical differentiation with presence of ghost cells is limited.
Trichofolliculoma
Trichofolliculomas are more likely non-neoplastic, hamartoma-like lesions rather than true neoplasms.
Clinical findings
Trichofolliculomas are uncommon in dogs and rare in cats.20,30 Trichofolliculomas are <2 cm diameter, solitary, dome-shaped nodules that may have a central depression or pore-like opening that contains hair or sebaceous material.20,28,30
Breed, age, and site predisposition
There are no known breed, age, or site predilections.
Histopathologic findings
Trichofolliculoma usually appears as a well-circumscribed, unencapsulated dermal nodule composed of one or several, large, dilated primary HFs filled with keratin and hair shafts (Fig. 8A). There is gradual keratinization through a granular cell layer with keratohyalin granules. The primary follicles may open onto the skin surface (creating the clinically apparent pore) and are surrounded by secondary HFs radiating outward from the primary follicles in an arborizing pattern (Fig. 8B). The secondary HFs vary in number and exhibit various stages of maturation, ranging from primitive hair germ (Fig. 8C) to fully developed HFs with hair shafts. Different hair cycle stages may be present. Anagen HFs may have well-differentiated hair bulbs (Fig. 8D) and dermal papillae. The follicular epithelium may be heavily melanized. 20 The surrounding stroma is paucicellular and separates the lesion from the adjacent dermis. Sebaceous glands may be associated with the primary follicles. A lesion with large, prominent sebaceous glands is called sebaceous trichofolliculoma.20,30
Trichofolliculoma in a guinea pig.
Differential diagnosis
The main differential diagnosis for trichofolliculoma is a dermoid cyst. Dermoid cysts have fewer secondary hair structures radiating from the primary HF, and the central cyst in the primary HF is lined entirely by squamous epithelium. Trichoepitheliomas have more cystic structures, less trichogenesis, and may have differentiation toward the isthmus and lower segments. 20
Cutaneous cysts
True neoplastic lesions of HFs must be histologically distinguished from cysts. Clinically, cysts are often difficult to distinguish from true neoplasms.
Dermoid cysts
Dermoid cysts are focal reduplications of the skin resulting from a developmental anomaly, and they include epidermis, dermis, and adnexal structures. Such cysts are formed because of incomplete separation of the cutaneous ectoderm and neuroectoderm during embryogenesis.
Clinical findings
Dermoid cysts occur in dogs and less commonly in cats, and they are clinically similar to follicular cysts. Lesions are usually solitary and <2 cm in diameter. Commonly, the cysts include a small pore from which hair may protrude. 20
Breed and age predilection
Rhodesian Ridgebacks and Boxers are predisposed and often have multiple cysts on the dorsal midline.20,30 Other breeds with an increased incidence include the Kerry Blue Terrier, English Bulldog, Shi Tzu, Chow Chow, Boerboel, Yorkshire Terrier, Great Pyrenees, Siberian Husky, English Springer Spaniel, and St. Bernard.10,20,36 There is no breed predisposition in cats. Given that dermoid cysts are developmental anomalies, young animals (<2 y old) are affected primarily. 16
Location
As a result of the defect in embryogenesis, lesions are located most commonly on the dorsal midline and occasionally may extend to the spinal canal and attach to the dura mater. Cysts can also be found in other locations such as the lateral neck or shoulder, particularly in cats. 20
Histopathologic findings
Dermoid cysts can be either dermal or subcutaneous. The cysts are lined by squamous epithelium with prominent keratohyalin granules, and they contain lamellar keratin, hair fragments, and sometimes sebaceous secretions. Dense collagen usually surrounds the cysts, and collagen bundles are often parallel to the cyst wall. Evenly spaced adnexal structures, including well-differentiated HFs, sebaceous glands, and occasional apocrine glands, are attached to the cyst wall and radiate downward. Hair shafts are frequently present. 20
Differential diagnosis
The differential diagnosis for dermoid cysts includes trichofolliculomas and infundibular cysts. Trichofolliculomas usually have more HFs radiating from the central cyst, and the lining epithelium may also contain features of the isthmic and inferior segment, whereas dermoid cysts are lined entirely by squamous epithelium with infundibular differentiation (with keratohyalin granules). Differentiation between dermoid cysts and infundibular cysts may therefore be problematic, but dermoid cysts usually have more adnexal structures radiating from the cyst. Infundibular cysts typically have only a few sebaceous glands and lack the concentric arrangement of collagen seen in dermoid cysts. 20
Follicular cysts
Follicular cysts are non-neoplastic, benign lesions. Progression of follicular cysts to SCC has been reported, 43 but this is considered to be exceptionally rare. Follicular cysts may develop on pressure points and in the vicinity of surgical scars or trauma as a result of follicular entrapment, or they may develop from dilated and occluded HFs.
Clinical findings
Infundibular cysts are common in dogs and fairly common in cats. Isthmic and hybrid or panfollicular cysts are quite common in dogs and rare in cats. Matrical cysts are rare in both dogs and cats. 20 Follicular cysts are firm, usually <2 cm diameter, and may be dermal or subcutaneous. The cysts may have a white, blue, or yellow tinge. Partial or complete alopecia is common. A pore on the surface may be present, and keratin and secretory material may protrude. Follicular cysts are usually solitary, but multiple cysts (mainly of infundibular origin) have been described in both dogs and cats, including perianal cysts and cysts within the ear canal.15,35,48 Surgical excision is usually curative for follicular cysts, but complete excision may be difficult with multiple or disseminated cysts.
Breed and age predisposition
Boxers, Shi Tzus, Miniature Schnauzers, Basset Hounds, and Old English Sheepdogs have increased incidence.20,28 Dogs usually are 4–8 y old.16,28 There is no apparent breed or age predilection in cats.
Location
Lesions are found most commonly on the head, trunk, and proximal limbs in dogs16,28 and on the head, neck, and trunk in cats, 28 but lesions may occur anywhere on the body.
Histopathologic findings
Similar to HF tumors, HF cysts are grouped based on the location of origin in the HF, and identification of the cysts depends on the type of epithelium that is lining the cyst, type of keratinization, and features specific to the individual HF segments (such as ghost cells and trichohyalin granules for the inferior portion, and keratohyalin granules for the infundibular segment).
Rupture of cysts may result in severe pyogranulomatous inflammation with fibrosis and ulceration.
Infundibular cyst
Infundibular cysts are lined by squamous epithelium with keratohyalin granules, and are filled by lamellar, often concentric keratin (Fig. 9A, 9B). Occasionally, a few sebaceous glands are attached to the cyst wall. 20
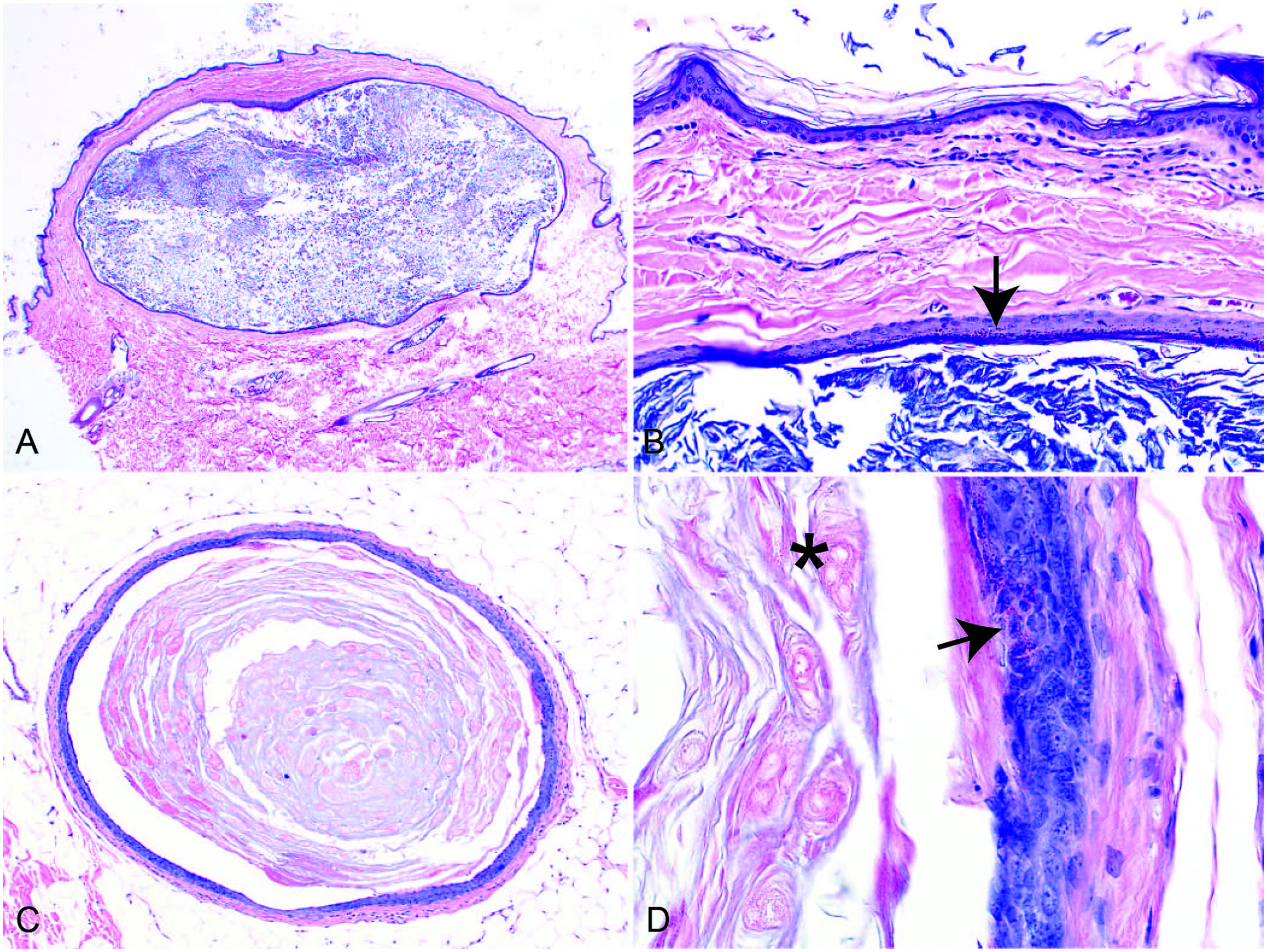
Follicular cysts in a dog.
Differential diagnosis
Differentiation between dermoid cysts and infundibular cysts may be problematic. Dermoid cysts usually have more adnexal structures radiating from the cyst; infundibular cysts usually have only a few sebaceous glands. Also, infundibular cysts lack the concentric arrangement of collagen that surrounds dermoid cysts. 20
Isthmus cyst (tricholemmal cyst)
The lining epithelium and keratinization pattern of the isthmus cyst closely resembles the isthmus ORS, with granules absent. Keratinocytes are often glassy and pale. The cyst is filled with amorphous, trichilemmal keratin.20,30
A rare isthmus cyst subtype has a large amount of trichilemmal, eosinophilic, amorphous keratin with a spiked outline that seems to protrude into the wall of the cyst (flame follicle–like). These cysts are relatively small, have a wrinkled contour, and are surrounded by a prominent, vitreous membrane. This type of cyst occurs only in Siberian Huskies and may be multiple. 20
Differential diagnosis
A rare subtype of isthmus cysts has a proliferation of squamous epithelium into short trabecular projections at the base of the cyst that, with time, form secondary keratinaceous cysts. This rare “proliferating isthmus cyst” has features similar to IKA but lacks the pore opening to the surface. 20
Matrical cyst
Matrical cysts are derived solely from the inferior portion of the HF and are lined by small, basaloid epithelial or matrical cells with scant cytoplasm and hyperchromatic nuclei (Fig. 9C, 9D). Occasionally, cells are glycogenated and have trichohyalin granules, indicating differentiation toward the IRS. There is abrupt keratinization without a granular layer, and the cysts are filled with amorphous keratin that may contain ghost cells (Fig. 9D).
Similar to proliferating isthmus cysts described above, matrical cysts rarely have proliferative, smaller, cystic structures adjacent to the primary cyst. These lesions may represent precursors to trichoepitheliomas or pilomatricomas. 20
Differential diagnosis
A possible differential diagnosis of matrical cysts is the benign pilomatricoma. Matrical cysts usually are unilocular as opposed to the often multilocular appearance of pilomatricomas.
Hybrid and panfollicular cysts
Hybrid cysts are derived from 2 HF segments; panfollicular cysts have differentiation to all 3 parts of the HF. Accordingly, these cysts are lined by epithelium with features of 2 (hybrid) or 3 (panfollicular) of the above-mentioned types of follicular cysts.
The most common type in dogs seems to be the infundibular-isthmus cyst, which is characterized by squamous epithelium with keratohyalin granules, most commonly in the upper part, and a lack of granules in the rest of the cyst. The keratin within the cyst has both lamellated and amorphous features. 20 If the cyst is also lined by matrical cells and/or there are trichohyalin granules and/or ghost cells, the diagnosis is a panfollicular cyst.
Follicular cysts are benign in the vast majority of cases, so differentiation of cyst types may not be clinically relevant.
Differential diagnosis
Similar to the proliferating types of isthmus and matrical cysts, panfollicular cysts may proliferate and progress to trichoepitheliomas. 20 A possible differential diagnosis of panfollicular cysts is therefore benign trichoepithelioma. Panfollicular cysts usually are unilocular as opposed to the often multilocular appearance of trichoepitheliomas.
Footnotes
Acknowledgements
I thank Dr. Monika Welle for her mentorship, Drs. Aline Rodrigues Hoffmann and Chiara Brachelente for their advice, and Dr. Raquel Rech for her support in my writing of this review. I thank Dr. Brian Porter for critically reviewing this paper. Images are from cases from the archive of the Texas A&M Dermatopathology Specialty Service.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.