
Abstract
A mixture of ketamine, xylazine, and butorphanol was inadvertently injected into the right carotid artery of a 1-year-old alpaca. Injection was followed by a brief period of recumbency and seizure activity. The alpaca recovered, but was euthanatized 72 hr later because of development of progressive neurologic deficits. Pathologic findings were confined to the right cerebrum, meninges, thalamus, and hippocampus. Cerebrocortical edema with astrocytic reaction, perivascular hemorrhage and neutrophilic infiltration, and fibrinoid necrosis of vasculature within the meninges and thalamus were the most prominent lesions. Neuronal necrosis was mild. Astrocytic reaction within the right cerebral cortex was confirmed with immunohistochemistry for glial fibrillary acidic protein.
Unintentional intra-arterial injection of drugs is a recognized risk in human medicine 11 and in veterinary medicine. 1,2,4,9 The frequent administration of intravenous solutions into the jugular vein in large animals can result in inadvertent intracarotid injection. 2,4,9 Numerous studies have been made of experimental disruption of the blood–brain barrier by intracarotid injection of a variety of compounds, 8,10,13 but few reports document the pathologic consequences of inadvertent intra-arterial injection in animals. 1,2,4,9 Cerebral injury occurring within 5 min after inadvertent injection of a lipid-based antibiotic into the auricular artery of cattle was attributed to vascular occlusion. 1 Cerebral injury after intracarotid injection of other compounds in cattle and horses has been attributed to breakdown of the blood–brain barrier and includes edema, hemorrhage, status spongiosis of white matter, neuronal necrosis, vascular necrosis, and thrombosis. 2,4,9 No studies to date include evaluation of glial fibrillary acidic protein (GFAP) immunohistochemistry to detect reactive astrocytes in affected tissue. This report describes clinical and routine pathologic findings and immunohistochemical changes in GFAP expression in the brain after inadvertent intracarotid injection of a mixture of a sedative, an opioid, and an anesthetic agent in an alpaca that was euthanized 3 days later because of persistent neurologic deficits.
A 1-year-old, 45-kg, female alpaca (Vicugna pacos) required chemical restraint for tooth trimming. Jugular vein venipuncture was attempted but the vein was difficult to locate, and approximately 0.3 ml of a mixture of ketamine (83 mg/ml), xylazine (8 mg/ml), and butorphanol (0.8 mg/ml) was inadvertently injected into the right carotid artery. Injection was followed immediately by recumbency and a brief period of seizure activity. The alpaca appeared to recover and stood after approximately 30 min. Over the next 24 hr, the alpaca's attitude was considered subdued, and development of visual deficits was suspected at 24 hr postinjection. On examination, the alpaca was mildly obtunded with normal temperature, pulse, and respiration. Neurologic examination revealed normal menace response on the right but none on the left. The alpaca was treated with 5 mg of intravenous dexamethasone. Forty-eight hours after intracarotid injection, the alpaca was found in lateral recumbency. After a brief seizure, she was able to maintain sternal recumbency. There was no change in the menace deficit on the left, the head occasionally drifted to the left, and horizontal nystagmus and lip fasciculations were observed. Dexamethasone treatment was repeated, and the alpaca also received 2.5 mg of intravenous diazepam and 1 liter of lactated Ringer solution administered subcutaneously. The animal stood, but was ataxic and circled to the right. Neurologic signs persisted, and the alpaca was euthanatized 72 hr after intracarotid injection.
On postmortem examination 24 hr later, the alpaca was in good body condition. An approximately 7-cm-long area of perivascular hemorrhage was associated with the right carotid artery. The cerebral hemispheres were asymmetric, with severe meningeal congestion and more pronounced gyral definition of the right hemisphere. Cerebellar herniation was not evident, with no significant findings in any other organs. Samples of both sides of the brain at multiple levels were obtained after 4 days of immersion fixation in 10% neutral buffered formalin and were fixed in formalin for an additional 50 hr before processing to minimize fixation artifact. All sections were stained with hematoxylin and eosin. Selected sections of right and left cerebrum were immunostained with the use of an automated immunostainer a with polyclonal rabbit anti-glial fibrillary acidic protein a (GFAP, diluted 1:500), Nova Red chromogen, b and Mayer hematoxylin counterstain. c Sections incubated with nonimmune serum served as negative controls.
Histologic lesions were confined to the right cerebrum, meninges, hippocampus, and thalamus. There was severe congestion and acute perivascular hemorrhage within the meninges, with mild perivascular hemorrhage within cerebral and thalamic parenchyma. Scattered arterioles, particularly within the meninges and thalamus, exhibited focal to diffuse fibrinoid necrosis, often without obvious associated parenchymal damage (Fig. 1). Perivascular spongiosis of white matter was present surrounding necrotic vasculature in a few areas of the thalamus, with scattered intravascular fibrin thrombi. Perivascular cuffs of intact neutrophils were present in the cerebral meninges and parenchyma (Fig. 2). Parenchymal changes within the right cerebral cortex were subtle and were best appreciated when compared with findings in the left cerebral cortex. Scattered individual neutrophils were present within gray matter parenchyma on the right. Perivascular and perineuronal clear zones indicative of edema were evident in the right cerebral cortex, with smaller clear zones consistent with artifactual change detected within the left cerebral cortex (Figs. 3, 4). Astrocyte nuclei within the gray matter of the right cerebrum and thalamus were enlarged and euchromatic, and there were scattered small aggregates of pyknotic nuclear debris (Fig. 3). Astrocyte nuclei within the gray matter of the left cerebrum were small and heterochromatic (Fig. 4). Convincing neuronal necrosis, characterized by shrunken cell bodies with eosinophilic cytoplasm and pyknotic nuclei, was mild and occurred as single to small clusters of neurons within the right cerebral cortex, particularly the parahippocampal gyrus, thalamus, and hippocampus. Immunoreactivity for GFAP was similarly intense within the white matter of both cerebral hemispheres. Immunostaining of the left cerebral gray matter was either negative or revealed a very thin rim of astrocyte cytoplasm (Fig. 5). Astrocytic reaction within right cerebral gray matter was confirmed with GFAP immunostaining and was characterized by increased nuclear size and formation of branching cytoplasmic processes (Fig. 6).
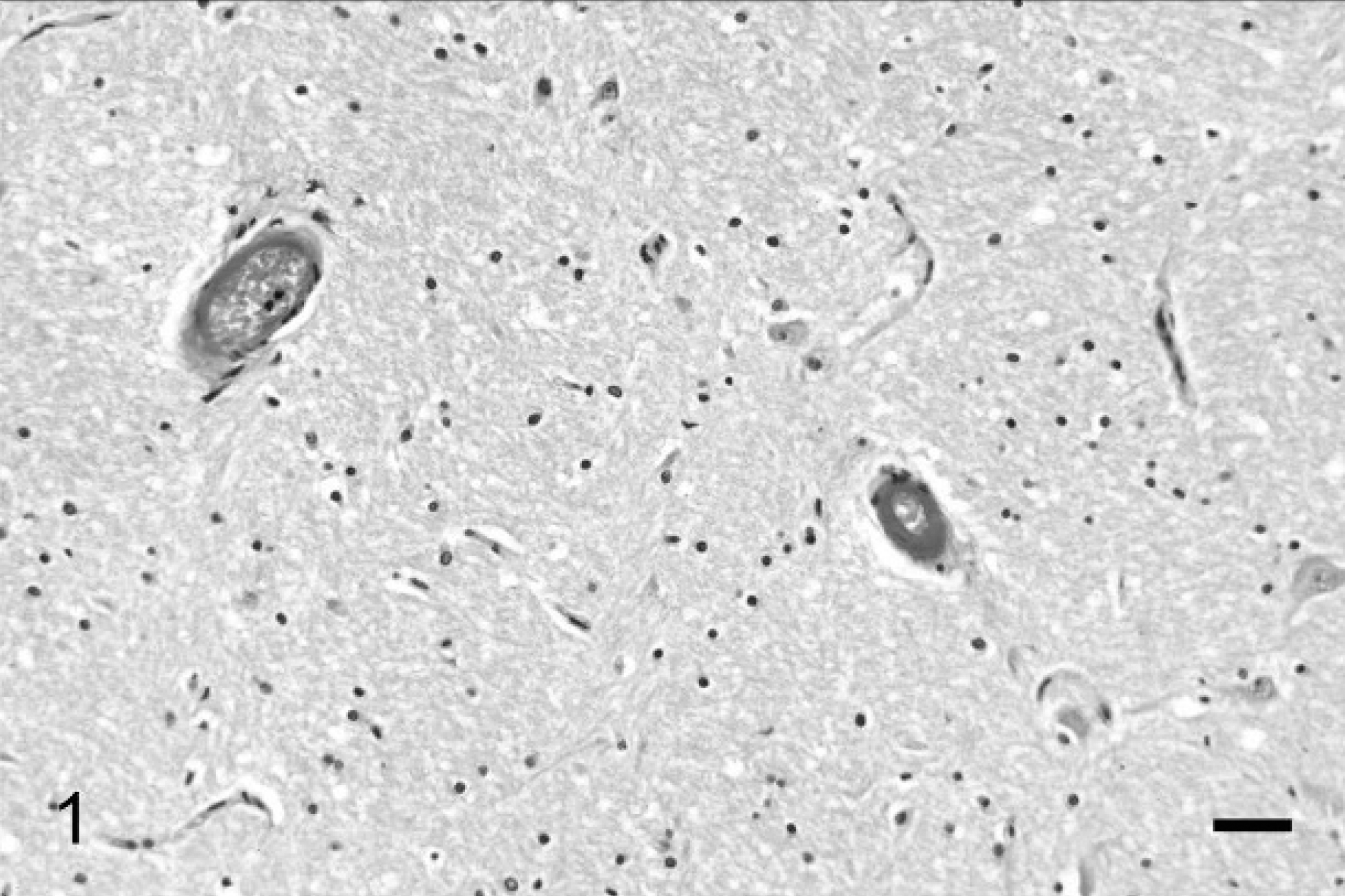
Right thalamus of a 1-year-old alpaca 72 hr after right intracarotid injection. Fibrinoid necrosis of the walls of 2 arterioles is present. Parenchymal damage is not evident. Hematoxylin and eosin. Bar = 50 μm.
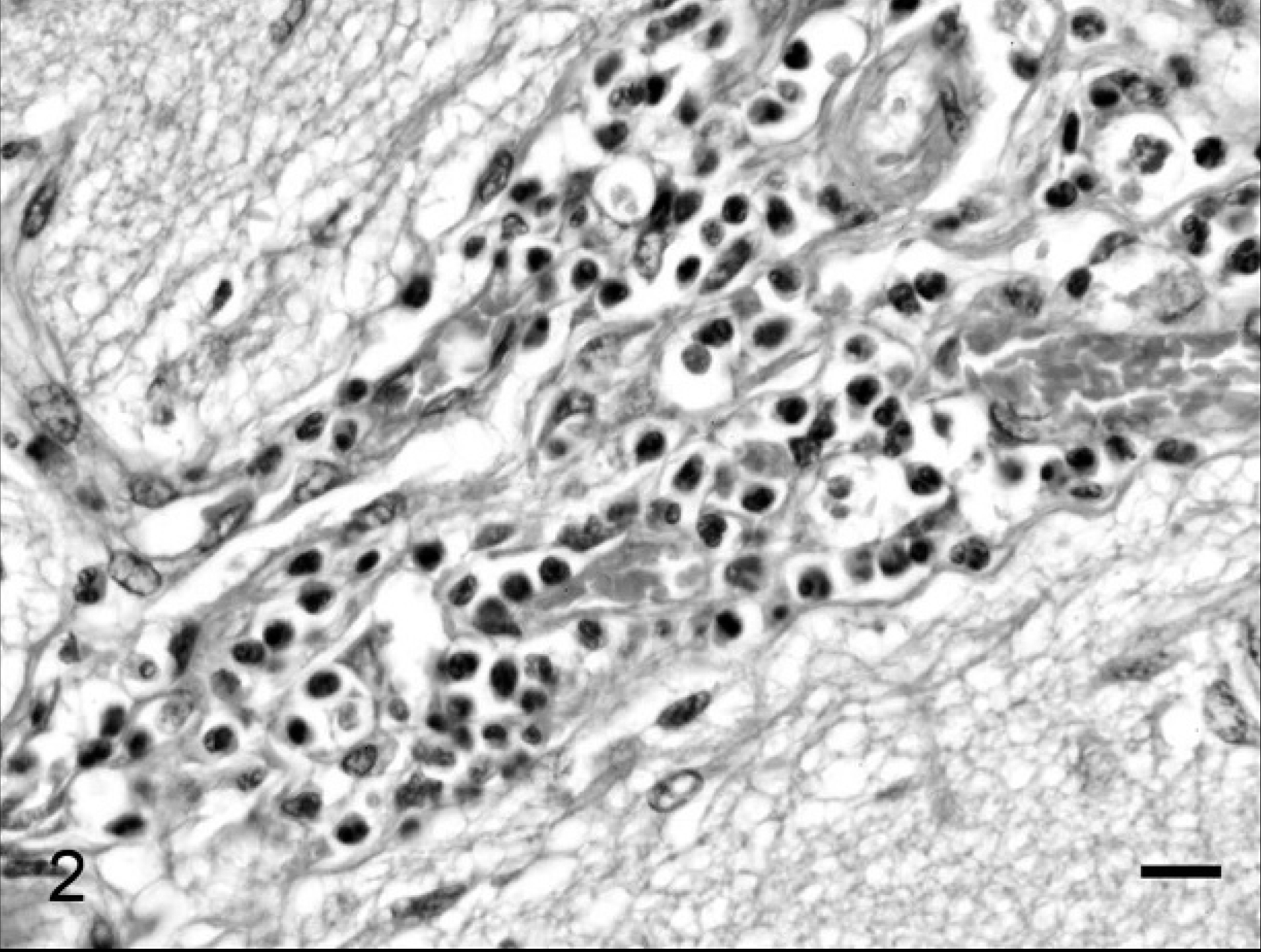
Right cerebrum of a 1-year-old alpaca 72 hr after right intracarotid injection. There are dense perivascular infiltrates of neutrophils within the meninges. Hematoxylin and eosin. Bar = 20 μm.

Right cerebrum of a 1-year-old alpaca 72 hr after right intracarotid injection. The gray matter exhibits prominent perivascular and perinuclear halos indicative of edema. Pyknotic nuclear debris is scattered within the parenchyma (arrow). Astrocyte nuclei are enlarged and euchromatic (arrowheads). Hematoxylin and eosin. Bar = 25 μm.

Left cerebrum of a 1-year-old alpaca 72 hr after right intracarotid injection. There is no evidence of injury. There are small perivascular and perinuclear halos consistent with artifactual change. Astrocyte nuclei are small and contain condensed chromatin. Hematoxylin and eosin. Bar = 25 μm.

Left cerebrum of a 1-year-old alpaca 72 hr after right intracarotid injection. Two astrocytes contain a very thin rim of glial fibrillary acidic protein (GFAP)-positive cytoplasm (arrows). Other astrocytes do not express GFAP. Immunohistochemistry, Nova Red chromogen, Mayer hematoxylin counterstain. Bar = 20 μm.
Tissue damage after unintentional intra-arterial injection of drugs can have serious consequences. 11 Possible causes of tissue injury include vasoconstriction, thrombosis, intravascular crystallization of injected compounds, endothelial inflammation, and direct cytotoxicity. 11 Intracarotid injection is used in human medicine for administration of compounds for brain imaging studies and for chemotherapy of central nervous system disease. 8,13 Breach of the blood–brain barrier is undesirable when administering imaging agents but can be valuable when administering chemotherapeutic agents. Numerous experimental studies document disruption of the blood–brain barrier by intracarotid injection of various compounds. 4,6,8,10,13 Breakdown of the blood brain barrier by material injected into the carotid artery can be due to reversible endothelial changes 8 or to vascular endothelial or mural necrosis. 6,10 Factors associated with parenchymal injury include the nature of the injected compounds, in particular high osmolality, 6,8,13 direct cytotoxicity, 13 and lipid solubility. 7 Arteriolar spasm 6,10 and thrombosis as a consequence of endothelial injury 2,4,6 contribute to the potential for parenchymal injury.
Prior studies of pathologic changes in the brain of animals after intracarotid injection of various compounds have documented perivascular edema and spongiosis of white matter, hyalinization and fibrinoid necrosis of vascular walls, 2,7,9 and neuronal necrosis. 2,4 Experimental studies indicate that the cerebrum and thalamus are the most commonly affected areas, and that neural lesions occur primarily on the same side as the injection. 6,7,13 The nature and degree of pathologic findings are also dependent on time from injection until death. Time of death following intraarterial injection in prior reports was 5 min, 1,9 6hr, 2 up to 24 hr, 4 and 3–7 days. 7 No convincing evidence of neuronal necrosis or perivascular edema was detected in the brain of cattle that died 5 min after inadvertent injection of a lipid-based antibiotic into the right auricular artery. 1 Neuronal necrosis was reported in a cow that died within 5 min of intracarotid injection of chloramphenicol, 9 although the very short time from injection to death suggests that neuronal changes might have been artifactual. Neuronal necrosis was described in a horse that died 6 hr after intracarotid injection of promazine. 2 Inflammatory cell infiltrates within the brain were not seen in horses that died within 20 hr of injection of various compounds, but perivascular infiltrates of lymphocytes were detected in the brains of horses that survived 20 to 24 hr. 4 Hemorrhagic necrosis, most prominent in white matter, and neutrophils and mononuclear cells within damaged vessel walls and in the perivascular space were present in the ipsilateral cerebrum of dogs examined 3 to 7 days after experimental intracarotid injection of a lipid-soluble nitrosourea chemotherapeutic agent. 7
Clinical signs in this case were indicative of right cerebral injury, and pathologic findings were confined to the right meninges, cerebrum, hippocampus, and thalamus. Ketamine, the primary component of the injected mixture, is hyperosmolar with an acidic pH, but a study of myotoxicity of ketamine after intramuscular injection concluded that ketamine also had a direct cytotoxic effect. 3 Direct neurotoxicity of the injected compounds after breakdown of the blood–brain barrier is possible, in that both ketamine and butorphanol are reported to be neurotoxic after intrathecal injection. 5 Results of studies of the neurotoxicity of ketamine are conflicting, however, and some attribute toxicity to the preservative benzethonium. 5
Edema causing overall swelling of the affected cerebrum is expected in cases in which death occurs within minutes to hours after intracarotid injection. 4,9 In the current case, the animal survived for approximately 72 hr after injection, and the right cerebral hemisphere appeared slightly collapsed rather than swollen. Astrocytic reaction, vascular damage, and perivascular neutrophils were the most prominent features, with only mild neuronal necrosis. Normal cerebrocortical astrocytes lack immunoreactive GFAP. 12 Increased GFAP immunoreactivity within right cerebral gray matter astrocytes in this case is characteristic of an astrocytic reaction, which is evident within 1–3 days of injury. 12 Artifactual changes in brain tissue are common, and immediate removal and prolonged fixation are important to provide optimal sections for examination. 12 In this case, the postmortem interval of approximately 24 hr likely resulted in some degree of artifact, but comparison of the left and right cerebral sections allowed detection of the right-sided cerebrocortical lesions.

Right cerebrum of a 1-year-old alpaca 72 hr after right intracarotid injection. Two astrocytes are enlarged with prominent glial fibrillary acidic protein (GFAP)–positive branching cytoplasmic processes (arrows). Immunohistochemistry, Nova Red chromogen, Mayer hematoxylin counterstain. Bar = 20 μm.
This case confirms that cerebral injury after intracarotid injection in animals occurs on the same side as the injection. This case also illustrates that prominent perivascular inflammation, most likely secondary to cellular injury, can be found in animals that survive for days after intracarotid injection. Immunostaining for GFAP proved to be valuable for detecting an astrocytic reaction in areas of cerebrocortical damage.
Footnotes
a.
Dako North America Inc., Carpinteria, CA.
b.
Vector Laboratories, Burlingame, CA.
c.
Sigma-Aldrich, St. Louis, MO.