
Abstract
Squamous cell carcinoma of the mammary gland is rare in both veterinary and human medicine. Whereas human metaplastic and squamous variants are known, the objectives of the current study were to ascertain the presence of such entities in canine mammary tumors and to distinguish them from other (epidermal, sweat gland) squamous tumors that may develop in the same area. A panel of antibodies (anticytokeratin [CK] 19, CK 14, CK 5/6, pancytokeratin, and vimentin) was used on 18 mammary gland malignancies with squamous features and 16 malignant skin tumors (11 squamous cell carcinomas of the skin and 5 sweat glands). Fifteen of the 18 mammary carcinomas were classified as metaplastic carcinomas, and the remaining 3 were classified as squamous cell carcinomas. The 2 most useful markers to establish the histogenesis of mammary tumors were pancytokeratin and CK 19. All other antibodies were equally expressed (CK 14 and 5/6) in all histotypes. The antibody panel discriminated primary epidermal squamous tumors (pancytokeratin positive and CK 19 negative) from gland-derived squamous neoplasms (pancytokeratin positive and CK 19 positive) but failed to distinguish primary mammary tumors from other squamous tumors of glandular origin.
Introduction
Current terminology distinguishing squamous cell carcinoma of the breast from metaplastic (squamous) carcinoma is confusing. More than 90% of human carcinomas are squamous and are classified under the heading “squamous cell carcinoma,” whereas the remainder are classified as “mammary carcinoma with squamous metaplasia” 25 or metaplastic carcinoma. Squamous cells in carcinomas of the breast may have either an epithelial (most frequently) or stromal (less frequently) origin. 24
Squamous metaplasia is observed in both hyperplastic and neoplastic breast lesions in humans. Fibroadenomas and papillomas are benign neoplasms commonly associated with squamous metaplasia. 22 , 26 The frequency of squamous metaplasia in breast carcinoma is probably underestimated, with only about a 100 cases reported to date. 4 The extent of metaplasia varies from isolated microscopic foci in an otherwise typical mammary carcinoma to complete replacement of glandular growth by the metaplastic phenotype. 24
In human medicine, strong consideration is given to the differentiation between squamous cell carcinoma of the breast and its skin counterpart. A series of criteria must be fulfilled to establish a diagnosis of primary breast squamous cell carcinoma: 1) absence of ductal or mesenchymal neoplastic elements; 2) absence of relationship to mammary skin or areolarnipple complex; and 3) absence of extramammary primary squamous cell tumors. 3 When all these criteria are met, the differentiation of mammary squamous cell carcinoma from well-differentiated squamous cell carcinoma of the skin is clear, but this is not the case with poorly differentiated neoplasms, as they lose intercellular bridges, lose the capacity to form horny pearls, and may mimic the glandular structure of the mammary gland.
Veterinary medicine includes squamous cell carcinoma among the classifications of mammary and skin tumors. Specifically, the World Health Organization (WHO) classifies squamous cell neoplasms among mammary tumors 20 and defines them as “a carcinoma composed of solid sheets and cord of cells with areas of squamous differentiation,” whereas squamous cell carcinoma of the skin is defined as “a malignant tumor of epidermal cells with varying degrees of keratinocyte (squamous cell) differentiation.” 10 Neither definition specifies the amount of squamous tissue necessary to discriminate between squamous cell carcinoma and carcinoma with squamous metaplasia, as in human medicine. Therefore, tumors with squamous differentiation may be found in the mammary region, originating either from the skin (epidermis or adnexa) or the mammary gland. Squamous cell carcinomas arising in the mammary gland are usually highly infiltrative and frequently invade the lymphatics. 9 The periphery of the tumor has predominantly basal cells with cellular atypia. Care must be taken to distinguish these neoplasms from cutaneous squamous cell carcinomas, as mammary tumors are more aggressive. 9
Primary antibodies used for immunohistochemistry in the current study.

Most commercially available antibodies are raised against keratins of human origin. Since cytokeratins are largely retained, even when cells undergo neoplastic transformation, these monoclonal antibodies have been successfully used for cell typing and tumor classification. 1 Pancytokeratin clone AE1/AE3 is a cocktail of 2 monoclonal antibodies that identifies most human cytokeratins 30 and thus may be used to identify cells of simple and stratified epithelial origin. 28–30 Antibody AE1 immunoreacts with an antigenic determinant present on most of subfamily A cytokeratins, including cytokeratins (CK) 10, 13, 14, 15, 16, and 19 (from 56.5 to 40 kD). 28 Antibody AE3 reacts with an antigenic determinant shared by the subfamily B cytokeratins, including CK 1, 2, 3, 4, 5, 6, 7, and 8 (from 65 to 52 kD). 6 This antibody has already been used in canine tissue sections to identify the luminal epithelium of the normal mammary gland and the epithelial component of mammary tumors, 8 as well as epithelial micrometastases in the regional lymph nodes. 19
Cytokeratin 19 is a useful tool for the differentiation and identification of human epithelial tumors and may be especially useful in identifying ductal and glandular neoplastic epithelia. 2 In canine mammary tumors, CK 19 has been found to detect glandular epithelial cells. 5 Cytokeratin 14 is known to immunoreact with myoepithelial cells, both in human breast tissue and in the canine mammary gland. 8 Cytokeratins 5 and 6 are closely related and are found in human nonkeratinizing stratified squamous epithelia, tracheal epithelia, and apocrine sweat glands of the skin, hair follicles, and mammary glands. 15 These antibodies bind to basal cells and part of the stratum spinosum in normal squamous epithelium. 15 In the dog, CK 5 has been used to detect lens epithelial cells. 16 The objectives of this investigation were 1) to differentiate squamous cell carcinoma of the skin from mammary gland squamous cell carcinoma using a panel of antibodies and 2) to discriminate between mammary squamous cell carcinoma and mammary metaplastic carcinoma in the dog, as has been done for human breast neoplasms.
Materials and methods
Cases
Eighteen mammary carcinomas with squamous metaplasia, 11 squamous cell carcinomas of skin, and 5 apocrine carcinomas of sweat glands were identified for study from the database of the Anatomopathological Service of the Department of Veterinary Public Health and Animal Pathology of the University of Bologna (Bologna, Italy). The histological diagnosis was achieved for each case based on microscopic evaluation of formalin-fixed, paraffin-embedded tumor sections that were stained with hematoxylin and eosin (HE).
Immunohistochemistry
Five-micron-thick paraffin tissue sections were dewaxed. Endogenous peroxidase was blocked by treatment with 3% hydrogen peroxide for 30 min. For antigen retrieval, the slides were immersed in 200 ml of citrate buffer and exposed to microwaves at 750 W for 10 min (5 min per cycle). The tissue sections were allowed to cool for 20 min, and the slides were then washed with Tris-buffered saline (pH 7.6) 3 times for 5 min each. For immunostaining, the sections were treated with protein block a for 20 min. The primary monoclonal antibodies are summarized in Table 1. All antibodies were incubated with the tissue sections overnight at 4°C.
Sites of primary antibody binding were identified using a commercial streptavidin-biotin-peroxidase kit b and diaminobenzidine as the chromogen (0.04% for 7 min). The sections were then counterstained with Papanicolaou hematoxylin, rinsed in tap water, dehydrated, and coverslipped. Sections of skin, normal mammary gland, and tendon were used as positive controls for anti-pancytokeratin, anti-CK 19 and 14, and anti-vimentin antibodies, respectively. Negative controls were achieved by incubating the slides with a nonspecific antibody of the same isotype.
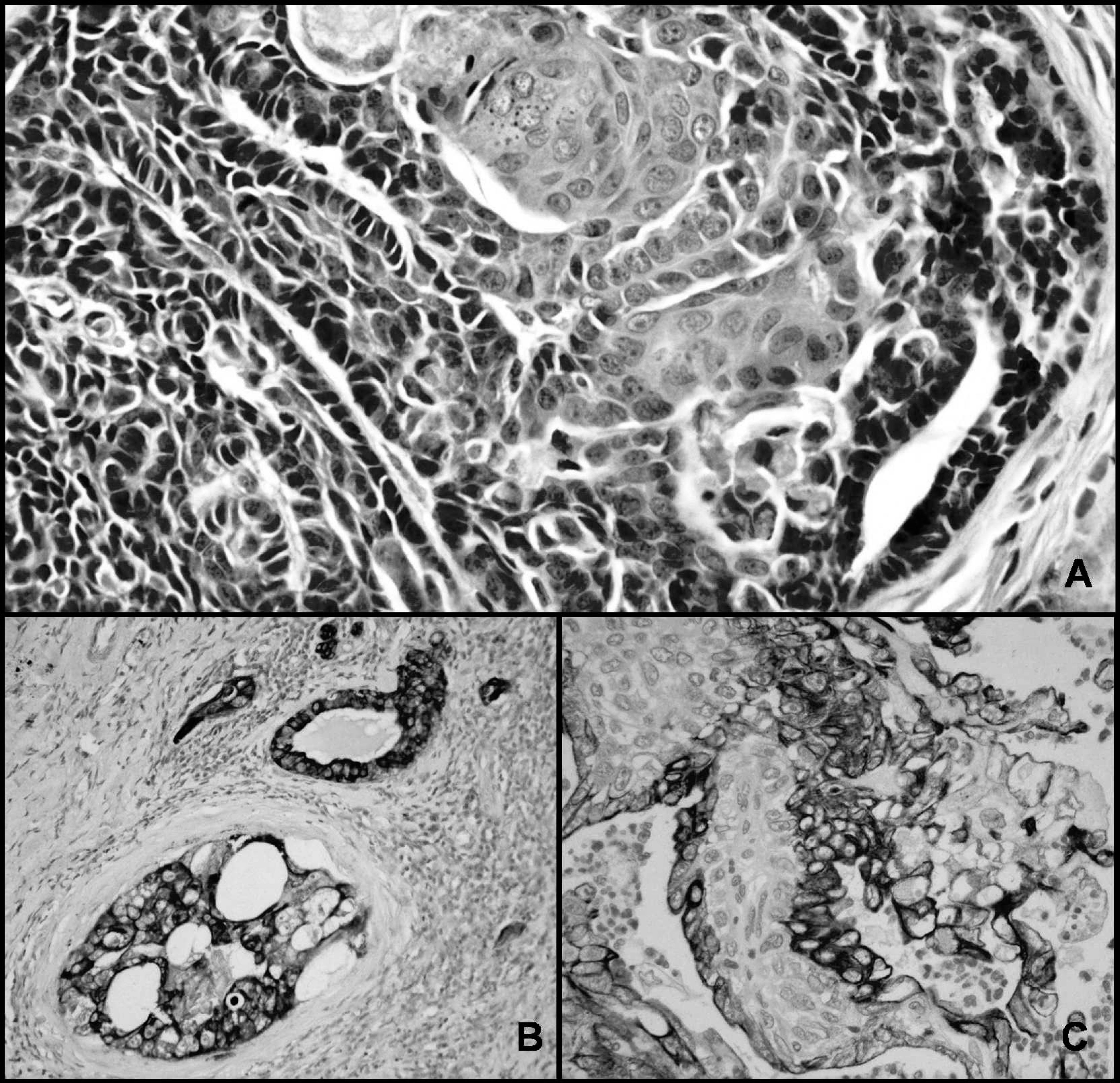
Mammary metaplastic carcinoma.
Results
Histology
Following the criteria used in human medicine, 24, 25 the 18 cases of mammary tumors were diagnosed as 15 metaplastic carcinomas and 3 squamous cell carcinomas. In the HE-stained sections, metaplastic carcinomas showed a typical simple glandular pattern of tubulopapillary or solid type. The squamous component was always minimal, but varied in distribution throughout the neoplasms (Fig. 1A). Squamous cells were mixed with adenocarcinoma as single cells or circumscribed cell clusters. These individual squamous cells had abundant hyaline eosinophilic cytoplasm; a centrally located, moderately atypical nucleus with irregular heterochromatin aggregates; and large central nucleoli. In some areas, the squamous component had a multilayered malpighian arrangement, with evidence of basal cell, prickle cell, and keratin layers containing flattened keratinocytes and thin layers of keratin. Basophilic keratohyaline granules were sometimes present in the cytoplasm of squamous cells of both metaplastic and squamous cell carcinomas. When present, the infiltrating component of these tumors did not necessarily exhibit a squamous pattern.
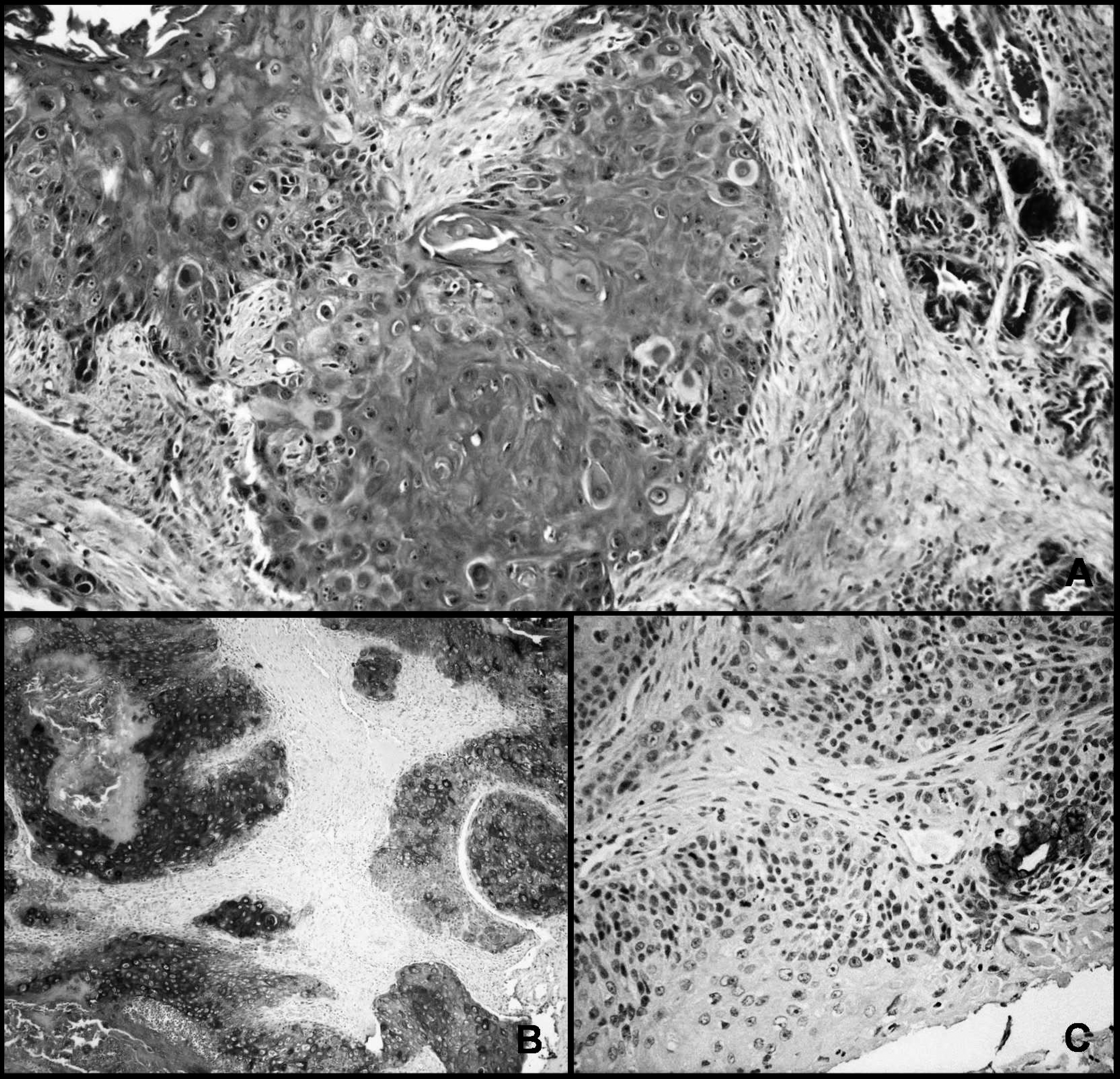
Mammary squamous cell carcinoma.
Three out of 18 cases of squamous cell carcinoma of the mammary gland had a prevalent squamous component, with a multilayered malpighian arrangement similar to squamous cell carcinomas of skin (Fig. 2A). Prickle cells were prevalent, but basal cells were sparse. The amount of keratin covering the surface varied and sometimes was organized in concentric layers (horny pearls). The infiltrating component of all 3 tumors had a consistent squamous pattern. Only a few microscopic fields of view had a tubulopapillary or solid-type glandular pattern.
The 11 cases of squamous cell carcinoma of the skin were well differentiated. These neoplasms had malpighian organization that lacked polarization to the skin surface or had a more atypical appearance, with solid cords of squamous cells or single squamous cells infiltrating the dermis, which incited desmoplasia. When not strictly connected to the epidermis basal layer or tumor areas with malpighian arrangement, most atypical areas formed by solid cords appeared to have a glandular or trabecular epithelial pattern. The infiltrating tissue of these tumors constantly had a squamous component.
Results of immunohistochemical staining in the epithelial (malignant) component of the mammary gland group.*
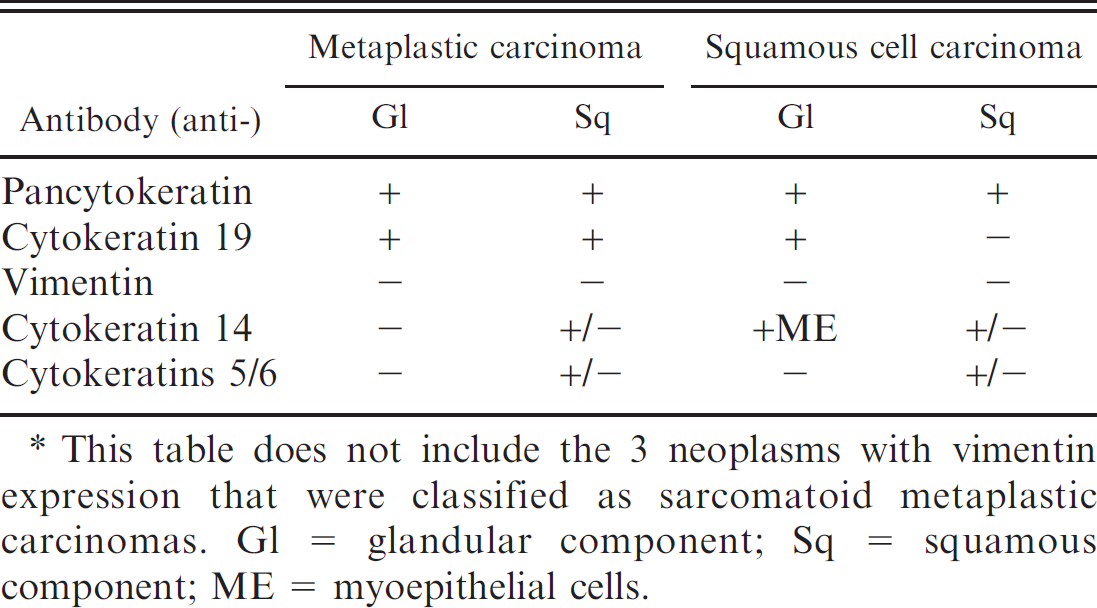
This table does not include the 3 neoplasms with vimentin expression that were classified as sarcomatoid metaplastic carcinomas. Gl = glandular component; Sq = squamous component; ME = myoepithelial cells.
The 5 cases of apocrine carcinoma of the sweat glands appeared histologically as solid or tubular tumors that were lobulated by fibrous trabeculae. The tumor cells had abundant eosinophilic cytoplasm, which rarely showed the apical blebs characteristic of apocrine glandular cells. The tumors infiltrated the deep dermis and subcutis in association with desmoplasia. The neoplastic cells in 2 of these tumors had squamous metaplasia in single cells or small cell clusters, similar to the squamous pattern described for mammary carcinomas.
Immunohistochemistry
Mammary carcinomas. The metaplastic carcinomas stained positively for pancytokeratin (Fig. 1B) and CK 19 (Fig. 1C). These 2 antibodies were constantly expressed in both the glandular and the squamous components in all but 3 neoplasms, which expressed only vimentin. Cytokeratin 14 expression varied. Strong staining of myoepithelial cells of carcinomas was observed. There was greater expression but weaker staining intensity for CK 14 in the squamous portion compared to the glandular component. Cytokeratins 5/6 were inconsistent and were expressed more frequently in squamous than in glandular cells.
In squamous cell carcinoma of the mammary gland, there was no concordance of pancytokeratin and CK 19 immunoreactivity. Pancytokeratin was expressed in the glandular and squamous components (Fig. 2B), whereas CK 19 was always expressed in the glandular cells and never in the squamous portion (Fig. 2C). Both the glandular and squamous components failed to express vimentin. Cytokeratin 14 and CK 5/6 were expressed more consistently in the squamous than in the glandular component of these neoplasms. Results are summarized in Table 2.
Results of the immunohistochemical staining in the malignant epithelial component of the skin tumor group.
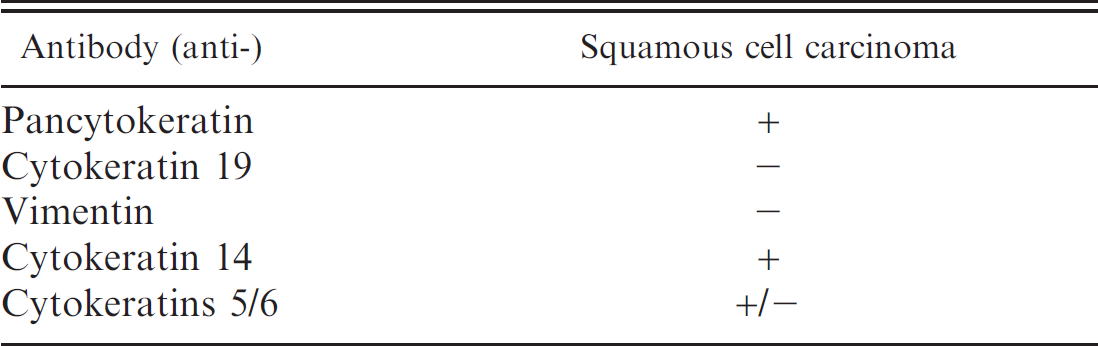
Squamous cell carcinoma of the skin. All 11 cases of squamous cell carcinoma of the skin were positive in the epithelial and squamous components for pancytokeratin. Furthermore, 10 of 11 squamous cell carcinomas of the skin were negative for CK 19. A glandular phenotype was only observed in 1 skin neoplasm located in the neck, wherein the nonsquamous glandular cells had likely originated from sweat glands. The squamous epithelial components of the skin squamous cell carcinomas also were negative for vimentin, positive for CK 14, and slightly positive for CK 5/6. Results are summarized in Table 3.
Apocrine carcinoma of the sweat glands. Two of the 5 cases of apocrine carcinoma of the sweat glands had squamous metaplasia. All neoplasms were positive for pancytokeratin and CK 19, confirming their glandular origin. Vimentin was always negative in both glandular and squamous epithelial components, whereas CK 14 and CK 5/6 were weakly positive. In particular, CK 5 and CK 6 were prevalently located in the myoepithelial component in 3 out of 5 neoplasms. Results are summarized in Table 4. Immunohistochemical results for all tumor groups are found in Table 5.
Results of immunohistochemical staining in the malignant epithelial component of the sweat gland tumor group.*
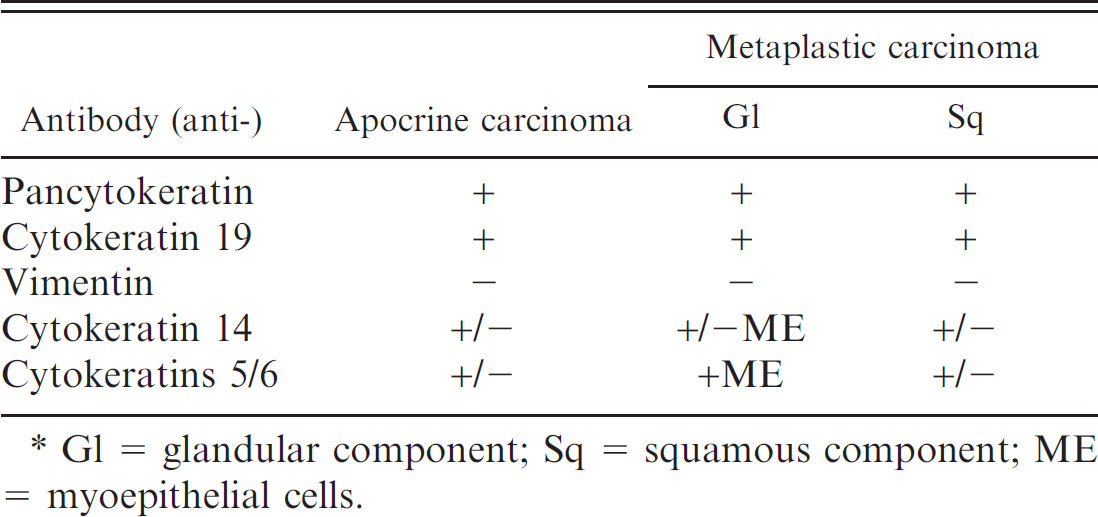
Gl = glandular component; Sq = squamous component; ME = myoepithelial cells.
Results of immunohistochemical staining in the malignant epithelial component of the various tumor groups.*
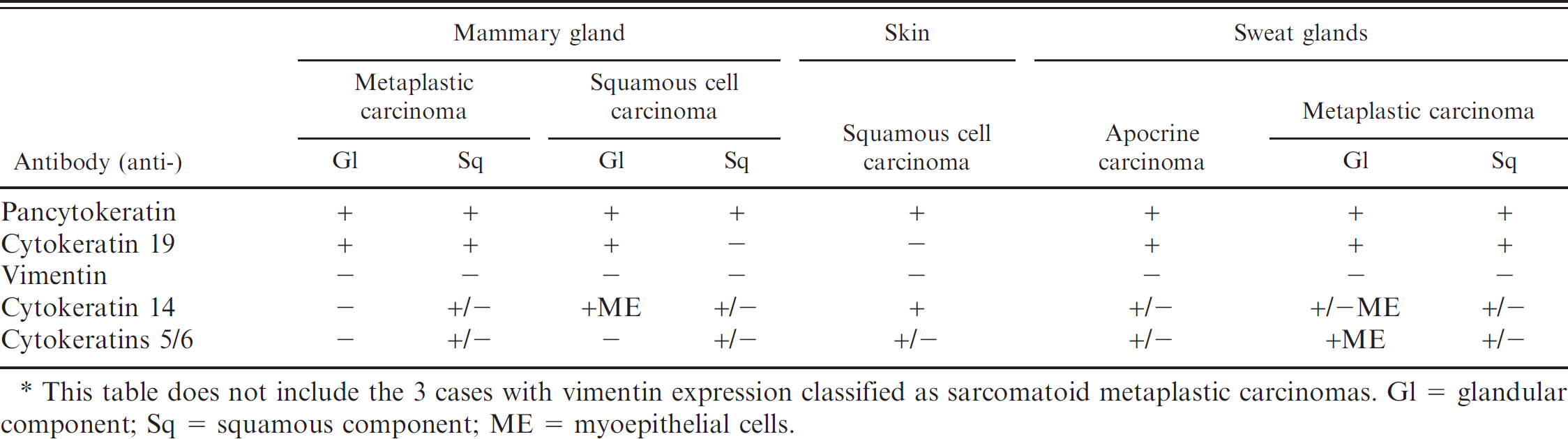
This table does not include the 3 cases with vimentin expression classified as sarcomatoid metaplastic carcinomas. Gl = glandular component; Sq = squamous component; ME = myoepithelial cells.
Discussion
No clear distinction exists in veterinary medicine between mammary squamous cell carcinoma and mammary carcinoma with squamous metaplasia (metaplastic carcinoma). The current classification for feline and canine mammary tumors, adopted by the WHO, combines the 2 neoplasms under the term squamous cell carcinoma. The amount of squamous metaplasia necessary to diagnose a carcinoma as squamous or adenosquamous is a subjective decision. 21 The term adenocarcinoma is used for neoplasms in which the cells have maintained their capacity to form ducts or alveoli. 27 This feature was present in all 18 canine mammary tumors investigated. Based on histological pattern and the diagnostic criteria for the classification of human neoplasms, the 18 canine mammary carcinomas with squamous cells were grouped into 2 types: metaplastic carcinoma (15 out of 18 cases) and squamous cell carcinoma (3 out of 18 cases). Most authors place squamous cell carcinoma in the heterogeneous group of the so-called metaplastic carcinomas of the breast. 22 Squamous cell carcinomas are divided into high and low grades of differentiation. 9 Well-differentiated (high-grade) squamous cell carcinoma is an uncommon tumor made up of glandular structures with variable areas of squamous differentiation and proliferation of dense collagenous stroma. 7 Poorly differentiated (low-grade) squamous cell carcinomas are characterized by nuclear atypia, frequent metastases to the regional lymph nodes, and poor prognosis. The presence of both epidermoid and nonepidermoid organized squamous components in the canine tumors emphasizes the analogies between human and canine neoplasms.
Some pathologists believe that an additional criterion is of primary diagnostic importance. Histologically, more than 90% of the tumor consists of squamous cells. 12 Other pathologists consider squamous cell carcinoma as an adenocarcinoma with a particularly high grade of squamous metaplasia. 13 , 18 Even if classified differently, these tumors share a particularly high degree of squamous metaplasia (>90%) and are defined as squamous cell carcinomas. Three of the canine tumors that were classified as squamous cell carcinoma of the mammary gland were characterized by a greater extension of the metaplastic component that was always mixed with a limited adenocarcinomatous pattern of cellular arrangement.
The histologic findings of mammary neoplasms in the dog are in line with human medicine, in which metaplastic carcinoma is more common than squamous cell carcinoma. 24 , 25 Lack of vimentin immunoreactivity (a marker for the mesenchymal component) in all but 3 tumors confirmed the epithelial phenotype of metaplastic carcinomas.
Three of the 15 mammary carcinomas with squamous metaplasia were vimentin positive and were proved to possess a malignant mesenchymal component. Since metaplastic carcinoma of the human breast can have squamous and sarcomatoid metaplasia, 24 these 3 canine neoplasms may be analogous to sarcomatoid metaplastic carcinomas. Thus, they may be designated as mammary carcinosarcomas according to the classification of mammary tumors. 21
Several monoclonal antibodies against keratin of different molecular weights can recognize epithelial cells in formalin-fixed specimens. It has been observed that so-called simple epithelia express keratins of a lower molecular weight, whereas stratified epithelia express high-molecular weight keratins. 23 The most useful markers for objective histogenesis of mammary tumors in the current study were pancytokeratin and CK 19, because CK 14 and CK 5/6 were expressed equally in all histotypes. Pancytokeratin and CK 19 immunoreactivity apparently distinguished mammary and sweat glandular tumors (pancytokeratin and CK 19 positive) from squamous cell carcinoma of the skin (pancytokeratin positive and CK 19 negative). In human medicine, squamous cell carcinoma of the breast cannot be distinguished histologically from a variant neoplasm developing in the skin above the mammary gland or from skin metastases that originate from other primary sites, including lung, esophagus, uterine cervix, and urinary bladder.
In human medicine, clinical symptoms and diagnostic imaging are helpful in tumor diagnosis because histology and immunohistochemistry offer little help in differentiating squamous cell carcinoma of the breast from mammary squamous metaplasia. 11 In the dog, it is also important to differentiate squamous neoplasms originating from the mammary parenchyma from those derived from the skin or cutaneous adnexa. The morphology of these 2 tumors is similar, 17 but the prognosis is worse for mammary tumors. 9 Cytokeratin 14, a well-known myoepithelial marker in the mammary gland, 30 was always expressed, albeit weakly, in the squamous component of mammary carcinomas in these canine tissues. Because this result was also obtained for the squamous variants of human breast carcinoma, 14 it may indicate the presence of a common metaplastic cell. The human literature has been identified this metaplastic cell as a nonglandular epithelial cell, most likely the myoepithelial cell. 22
The immunohistochemical panel allowed the reclassification of 4 canine tumors: 3 as mammary sarcomatoid metaplastic carcinomas and 1 as a squamous variant of apocrine carcinoma. The latter neoplasm was positive for pancytokeratin and CK 19. This staining pattern is typical of glandular epithelium, but this neoplasm on the neck was unlikely to have arisen from the mammary gland, unless it was a distant metastasis from a primary mammary neoplasm.
The antibodies employed in immunohistochemistry demonstrated their usefulness to differentiate between well-differentiated and poorly differentiated mammary and apocrine glandular squamous tumors versus those neoplasms of epidermal origin. Unfortunately, the antibodies did not distinguish the squamous variants of different glandular histogenesis. In particular, they failed to differentiate a squamous tumor of the mammary parenchyma from a squamous variant of apocrine carcinoma, which remains an entity to consider in the differential diagnosis.
Footnotes
a.
Dako Netherlands BV, Heverlee, Belgium.
b.
LSAB kit, Dako Netherlands BV, Heverlee, Belgium.