
Abstract
A 6-year-old male elk presented in August with a 4-month history of weight loss and a 1-day history of being recumbent and unable to rise. The elk's body condition score was 1.5/5. Hematology and blood chemistry showed an inflammatory leukogram, mild electrolyte abnormalities, and elevated liver enzyme activities. Because of poor prognosis, the owner elected euthanasia. On necropsy, 8 diverticula were in the duodenum distal to the common bile duct, which was dilated and filled with feed material. Many intrahepatic bile ducts were dilated up to 5 cm, were filled with ingesta and gritty material, and had walls thickened up to 1.5 mm. On histologic examination, mural thickening of dilated bile ducts was because of increased fibrous connective tissue with inflammatory cell infiltration and hyperplastic and hypertrophic epithelial lining. Portal tracts diffusely contained hyperplastic bile ducts and had increased amounts of fibrous connective tissue. Abscesses that contained bacteria were scattered throughout the liver. Duodenal diverticula lacked the tunica muscularis, and the muscularis mucosa was hypertrophied. Caudal to some diverticula, the duodenal lumen was narrowed. An additional finding was embolic pneumonia with fungi morphologically and immunohistochemically consistent with Aspergillus spp.
A 6-year-old male elk presented to the Purdue University Veterinary Teaching Hospital (PUVTH; West Lafayette, IN) in August 2007 with a history of weight loss of approximately 4 months' duration. Reportedly, this elk was always slower to gain weight in the spring and summer than the other males on the farm. When the elk first showed signs of ill thrift, the referring veterinarian treated the elk for digestive problems. There was no improvement in the body condition with treatment. The elk was pastured with 11 adult females. The pasture was supplemented with clover hay round bales produced on the farm, and each elk was fed 2.7 kg of sweet feed per day. All elk received anthelmintic therapy 4 times a year with Ivomec plus, a with the most recent dose given 2 months before presentation. No routine vaccinations were given. No other elk were showing weight loss. The farm had no history of chronic wasting disease.
The day before presentation to PUVTH, the elk was recumbent, unable to rise, and anorexic. On presentation, the elk was depressed and unable to rise. The body condition score was 1.5/5, and the body weight was estimated at 450 kg. Vital parameters were within normal limits. Patchy multifocal alopecia was present. Rumen contractions were weak but were present at 2 per min, and there was no diarrhea. No cranial nerve deficits were noted. The elk was estimated to be 5–8% dehydrated based on prolonged skin tent and tacky mucus membranes. Hematology and serum chemistry were nonspecific and showed an inflammatory leukogram, mild electrolyte abnormalities, and elevated liver enzyme activities (Table 1). Fecal flotation and egg count yielded trichostrongyle-type ova (<100/g feces) and Eimeria spp. (200 oocysts/g feces). No parasite eggs were seen on Baermann sedimentation. Serum enzyme-linked immunosorbent assay (ELISA) as well as fecal culture and polymerase chain reaction (PCR) for Mycobacterium avium sp. paratuberculosis were negative. Bacterial culture of the tissues at a postmortem was not performed because of the chronicity of lesions, chronic use of antibiotics, and the unlikelihood that the primary lesions were caused by bacterial infection. Because clinical signs and laboratory findings were nonspecific, the elk was treated empirically with fluids, antibiotics, and parasiticides. Over several days, the elk did not improve substantially, and the owners elected euthanasia.
At the necropsy, the elk had minimal body-fat stores and marked subcutaneous edema. The liver had a red and brown mottled appearance, rounded edges, and multiple firm adhesions to the diaphragm. The caudal surface of the liver was firmly adhered to parts of the duodenum and jejunum. The common bile duct was dilated and communicated with dilated (up to 5 cm) confluent areas within the liver (intrahepatic bile ducts), with 1.5-mm-thick walls filled with ingesta that contained corn and sandy material (Fig. 1). Portal tracts throughout the liver were prominent (Fig. 2). Occasional, 1–3-mm, tan-white, granular, friable foci (abscesses) were in the parenchyma. Eight round diverticula were on the mesenteric border of the duodenum and ranged from 1 to 3 cm in diameter (Fig. 3). These were immediately distal to the area of the bile-duct ampulla (papilla of Vater) and extended 25 cm distally. The lumen of the intestine was narrowed caudal to some of these diverticula. The lungs contained many 0.3–1.5 cm in diameter, tan, firm abscesses. Multiple firm adhesions were present between the lungs and the diaphragm and between lung lobes and the pericardial sac.
Hematology and serum biochemistry at the time of submission.
Unless otherwise indicated, elk reference values for hematology and serum biochemistries were taken from a previous study. 5
Bovine reference value supplied by the Purdue University Veterinary Teaching Hospital Clinical Pathology Laboratory.
Samples of selected tissues (lung, liver, intestine, rumen, omasum, abomasum, lymph nodes, tonsils, and pericardium) were fixed in formalin and routinely processed for histopathology. On microscopic examination, sections of liver had greatly dilated bile ducts that were lined by columnar-to-flattened epithelium and very thick (up to 1.5 mm) fibrous walls. Sometimes dilated bile ducts contained food material. Many lymphocytes, plasma cells, and macrophages infiltrated the thickened subepithelial connective tissue. Portal areas contained increased numbers of disorganized bile ductules and increased amounts of fibrous connective tissue. Abscesses in the liver contained necrotic debris, amorphous basophilic material, and scattered bacterial bacilli, and were surrounded by a thin zone of degenerate neutrophils, lymphocytes, plasma cells, and macrophages.
The lamina propria and serosa of the small intestines were multifocally edematous. The tunica muscularis (muscularis externa) in normal-appearing intestine ranged from 1- to 2-mm thick and was composed of 2 muscle layers. The walls of the diverticula were composed of a single, thickened layer of smooth muscle, approximately 0.25-mm thick, which was continuous with the muscularis mucosa in more normal areas of the small intestine. The submucosa and serosa in diverticula had increased amounts of fibrous connective tissue and were contiguous because of a lack of a tunica muscularis (Fig. 4).
The lungs contained multifocal hemorrhages and numerous necrotic foci, which contained neutrophils, cellular debris, and amorphous basophilic material surrounded by scant fibrous connective tissue and few macrophages and fewer lymphocytes, plasma cells, and granulocytes. Numerous, 6–8-μm-wide, refractile, basophilic or nonstaining, septate fungal hypha within the foci had parallel walls and dichotomous, acute-angle branching. Sometimes the fungi were surrounded by spicules of bright eosinophilic material (Splendore-Hoeppli material). Some adjacent alveoli contained fibrillar eosinophilic material (fibrin) and proteinaceous fluid, and few adjacent vessels were occluded by fibrin (thrombosis). Fungal hyphae stained positively with Grocott-Gomori methenamine silver stain, and immunohistochemistry for Aspergillus spp. was positive when using a mouse monoclonal antibody (Mab-WF-AF-1). b Samples of obex, lymph nodes, and tonsils, submitted to the National Veterinary Services Laboratory (Ames, IA) were negative for chronic wasting disease.
The final diagnosis was duodenal diverticulosis with dilatation of the extrahepatic and intrahepatic bile ducts (cholangiectasis) with intraductal accumulation of ingesta. In addition, there was an embolic fungal pneumonia because of Aspergillus spp. It is suggested that a previous obstruction led to herniation of the submucosa and mucosa of the duodenum through the tunica muscularis, which resulted in partial narrowing of the duodenal lumen and retrograde flow of feed into the bile duct and liver. Continued flow into the liver led to ectasia of the intrahepatic and extrahepatic bile ducts.
Intestinal diverticula may be congenital but will include all intestinal layers, which was not the case in this animal. Acquired diverticula (pseudodiverticulosis) have a loss of the tunica muscularis because of herniation of the mucosa and submucosa through the tunica muscularis. 6 A lack of the tunica muscularis in the diverticula of this elk indicates the diverticula were acquired.
Cholangiectasis in animals and man was reported with congenital anomalies, postsurgical intervention, and bile-flow obstruction because of parasites, a foreign body, choleliths, and intestinal atresias. 2,3,8,9,14,16 In this elk, bile-duct obstructions were not found, but partial intestinal obstruction was suspected as the cause of cholangiectasis. Intestinal obstructions and diverticula have been associated with biliary-tract disease, most often reported in humans. 5,11,14,17 Intestinal diverticula have only rarely been reported in animals and are more often described in farm animals. 1 In humans, diverticula adjacent to the duodenal papilla (juxtapapillary diverticula) have been associated with biliary-tract disease, dilatation of the extrahepatic bile duct, and formation of choleliths. 17 Similarly, this elk had diverticula adjacent to the papilla of Vater and concurrent biliary-tract disease.
In humans, it is believed that juxtapapillary diverticula are partially caused by an inherent weakness in the muscle layers of the duodenum at the area where the blood vessels enter along the mesentery. 6 The diverticula then may occur secondary to increased intraluminal pressure, such as with constipation or increased peristalsis. These acquired diverticula usually occur in elderly individuals, because this region of the muscle layers might progressively weaken. In this elk, increased intraluminal pressure may have occurred because of a foreign body or perhaps because of another cause, such as congenital duodenal stenosis. The increased intraluminal pressure and, rarely, foreign-body obstruction of the diverticula are believed to cause a weakness in the sphincter of Oddi, which predisposes to bacterial overgrowth in the biliary tract. 17 This results in the aforementioned association with biliary-tract diseases. 17 Duodenal stenosis has been associated with hepatic-duct obstruction and dilatation of the biliary and pancreatic ducts in 2 foals; some bile-duct proliferation was evident in these foals. 11 It seems plausible that, without surgical intervention, the foals may have acquired similar hepatic lesions as this elk. Interestingly, in humans, studies have often shown that biliary-tract disease is associated with juxtapapillary diverticula, but pancreatic disease is not, although some reports disagree with this assertion. 17 Other reports of diverticula in animals, including multiple duodenal diverticula in sheep, have not reported concurrent biliary-tract disease. 4 In the sheep, these diverticula were sometimes considered incidental, but, in some cases, there was also diarrhea or peritonitis. 4 Diverticula in animals are sometimes associated with smooth-muscle hyperplasia and/or hypertrophy of the intestinal wall, particularly in horses and ponies. 4 An important potential complication of diverticula in animals is rupture that results in peritonitis. 4
Liver; elk. Intrahepatic bile ducts (i) were dilated up to 5 cm, and the extrahepatic bile duct (e) was similarly dilated. Most of the ingesta were removed from the bile ducts, but some corn remained. Bar = 10 cm.
Liver; elk. Bile ducts were dilated (asterisk). Prominent portal areas are easily visible throughout the parenchyma on cut surface. An abscess (arrowhead) was in the parenchyma.

Duodenum; elk. Diverticula (asterisk) in the duodenum were outpouchings on the mesenteric side. The intestinal lumen was narrowed between 2 diverticula (arrowhead).
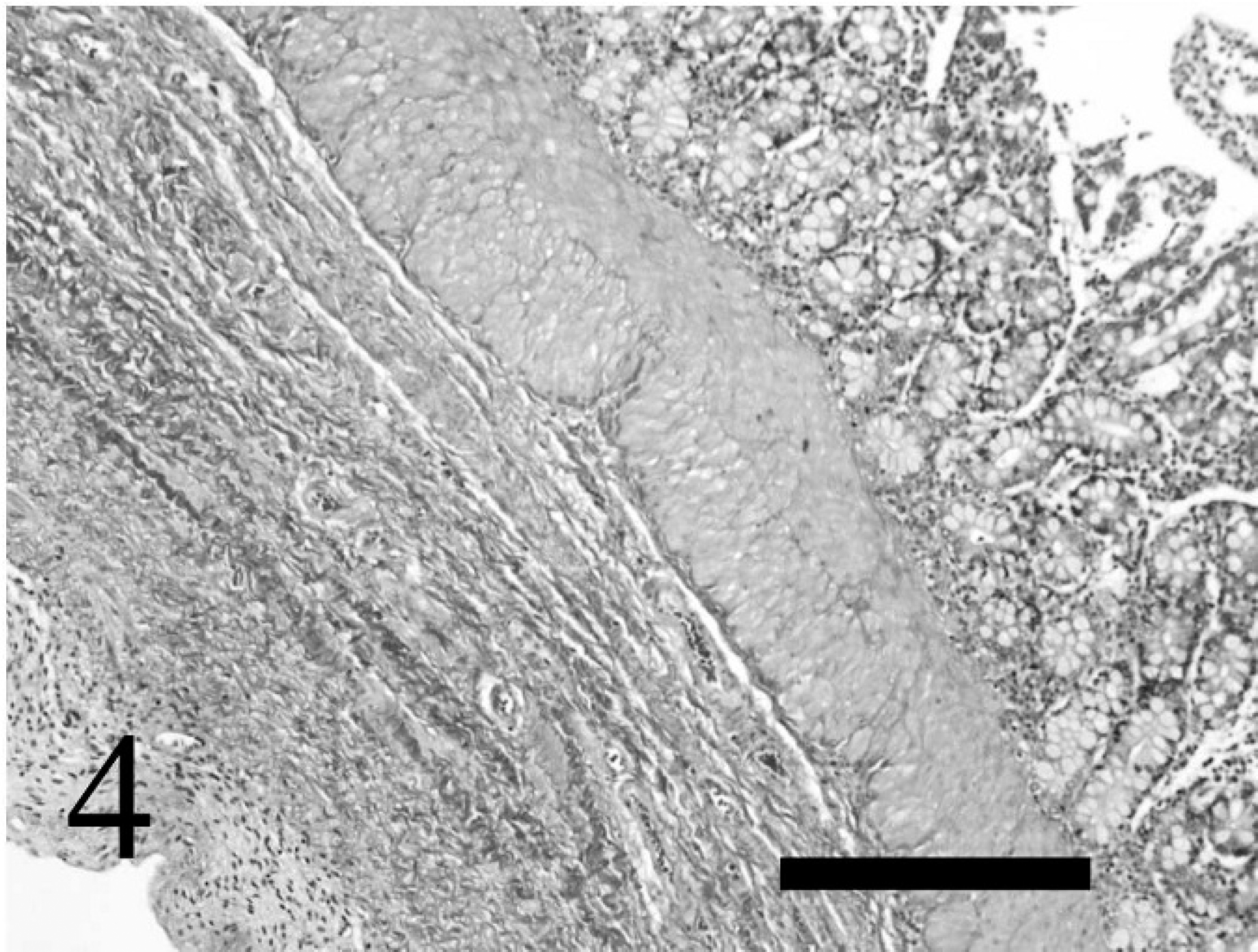
Duodenum; elk. The diverticulum had a mucosa and submucosa without a tunica muscularis. The muscularis mucosa was thickened and the tunica muscularis was absent. Masson trichrome stain. Bar = 300 μm.
Disseminated fungal infections, and fungal pneumonia in particular, have been associated with a loss of integrity of the gastrointestinal tract in different species, including cattle, horses, and llamas. These infections have also been associated with antibiotic and corticosteroid use, poor management, and poor hay quality. 10,12,13,15 The hepatic and intestinal lesions, with the loss of the mucosal barrier; immunosuppression because of emaciation; and antibiotic therapy likely contributed to fungal pneumonia in this animal.
In conclusion, this was an unusual presentation of liver disease in an elk. The authors are not aware of a report that describes a similar presentation of severe intrahepatic cholangiectasis with accumulation of intraductal ingesta in any species. Obstruction or narrowing of the duodenum distal to the opening to the bile duct could produce similar changes in other animals, but early surgical intervention may prevent this sequela.
Footnotes
a.
Ivomec plus, Merial Ltd., Duluth, GA.
b.
Mab-WF-AF-1, Dako North America Inc., Carpinteria, CA.