
Abstract
Collaboration was established in 2001 to evaluate a commercially available immunohistochemistry assay kit for the detection of bovine spongiform encephalopathy (BSE) disease-associated prion protein in formic acid-treated formalin-fixed samples of bovine brain. The kit protocol was evaluated at the National Centre for Foreign Animal Diseases (Winnipeg, Canada) and the Veterinary Laboratories Agency (Weybridge, U.K.). The U.K. laboratory provided paraffin-embedded blocks of brainstem (medulla oblongata at the level of the obex) from 100 positive cases defined by clinical signs and histopathology, and 100 clinically suspect but BSE-negative samples defined by histopathology and immunohistochemistry with anti-PrP monoclonal antibody R145. The Canadian laboratory provided 400 blocks from surveillance cases defined as clinically suspect but negative by histopathology and immunohistochemistry with anti-PrP antibody 6H4. Consecutive sections from each block were cut and coded. Each set of 600 slides was immunolabeled and read in each laboratory. Evaluation parameters included estimates of diagnostic sensitivity and specificity and reproducibility of the results. The kit performed with 100% sensitivity, specificity, and reproducibility in spite of minor differences between the laboratories in brain sample areas, fixation and processing, and in the immunolabeling protocol. Although enzyme linked immunosorbent assays are widely used in high throughput surveillance programs, standardized protocols and reagents for manual immunohistochemistry provide a useful adjunct to surveillance efforts, particularly in laboratories testing small numbers of samples or using immunohistochemistry for confirmation and characterization of BSE cases.
Bovine spongiform encephalopathy (BSE) is a fatal neurological disease of adult cattle that was first recognized in Great Britain in 1986,
16
and is one of the subacute spongiform encephalopathies associated with unconventional transmissible agents or prions.
9
The agent of BSE is considered the cause of variant Creutzfeldt-Jakob disease (vCJD) in humans.
2,4,12
The rapid and accurate diagnosis of BSE is therefore of critical importance to control measures for human and animal health protection. When BSE surveillance was implemented in 1992 in Canada, it was based on testing mature cattle with clinical signs compatible with BSE collected at provincial and federally inspected abattoirs, from rabies-negative submissions, and from private practitioners' submissions. At the initiation of the current study (2001), the U.K. BSE surveillance program comprised passive surveillance of all cattle presenting with clinical signs compatible with BSE, irrespective of age, together with active surveillance that targeted all cattle aged 30 months or over at death or slaughter (fallen animals, on-farm casualties, and healthy slaughtered). The surveillance program later included cattle aged 24–30 months slaughtered for human consumption but presenting as casualty animals or as animals segregated at antemortem inspection as unfit. The principal diagnostic approach for confirmation of BSE was originally neuropathological examination for morphological changes of spongiform encephalopathy.
18
After recognition of the diagnostic importance of the disease-associated form of the prion protein (PrPSc), immunochemical methods using polyclonal or monoclonal antibodies became standard approaches. For screening purposes these have evolved principally as high throughput ELISA or Western blot formats, but immunohistochemistry (IHC) provides a confirmatory and complementary approach that characterizes PrPSc distribution in brain to inform on disease phenotype. Because the antibodies used for IHC cannot distinguish between the cellular form of prion protein (PrP
Samples of brain were collected over a 3-year period (1998–2001) from cattle that exhibited neurological signs at the time of slaughter or death. The diagnosis of all cases included in this evaluation was based initially on histological examination in the laboratory of origin. The study included 100 cases considered BSE positive and 500 cases considered BSE negative. Positive cases demonstrated histological evidence of spongiform changes suggestive of BSE. 18 The negative cases showed no histologic evidence of spongiform encephalopathy and no evidence of PrP-Sc when screened by immunohistochemistry using MAb R145 (U.K. samples), a C-terminal specific anti-PrP rat monoclonal antibody produced at the VLA and raised against a bovine PrP peptide sequence, residues 221–233 15 or 6H4 (Canadian samples), a murine monoclonal antibody raised against recombinant bovine PrP and recognizing an epitope corresponding to residues 156–164. 6 Four hundred of the 500 negative samples were provided by NCFAD and 100 by the VLA. All VLA samples represented the medulla oblongata at the level of the obex. Of the 400 Canadian samples, 35% were from the medulla at obex, 46% from the medulla oblongata (nonobex), and the remaining 19% were from other areas of the brain, including the cerebellum. Samples were fixed and processed with minor protocol differences between the NCFAD and VLA laboratories, including fixation (10% neutral buffered formalin overnight vs. 10% formol saline for 48 hr), formic acid decontamination (2 hr vs. 1 hr), and embedding medium (paraffin b or paraffin/plastic c ). Four consecutive 5-μm sections from each block were mounted on positively charged d or treated e slides. Sections were coded and exchanged between laboratories. Each laboratory immunolabeled 1 set of 600 slides. All test kits were from the same lot number and were supplied to each laboratory by the manufacturer. The kit includes: a citrate buffer for antigen retrieval by hydrated autoclaving, 3 a proprietary proteinase K (PK) reagent of undisclosed concentration, primary monoclonal antibody F99/97.6.1 8 (a murine IgG1 binding the epitope QYQRES, residues 220–225 of the bovine PrP 5-octapeptide repeat molecule), antibody diluent, antimouse-IgG-biotinylated secondary antibody, peroxidase-labeled streptavidin, and diaminobenzidine (DAB) as the substrate-chromogen. Each laboratory independently selected a single BSE case as a positive control and a single non-BSE case as a negative control; both controls were included in each run with 38 test samples. Both laboratories immunolabeled the sections using the same generic protocol, including pretreatment with 3% (v/v) hydrogen peroxide in methanol to quench endogenous peroxidase, antigen retrieval with acid (undiluted 98% formic acid) for 5 min followed by 3 rinses with Tris buffered saline (TBS, pH 7.6) and hydrated autoclaving (121°C for 20 min with the kit-supplied citrate buffer). Slides were cooled, placed onto facing plastic coverplates, f which provide a constant 100-μl volume incubation chamber at the slide surface and a 2-ml reservoir above the slide for wash solution, and transferred to a slide rack g designed to hold the assembly vertically. Care was taken to remove air bubbles from the assembly before application of reagents. Wash buffer h was added to the reservoir and the sections were washed by gravity flow of the solution. The kit-supplied PK solution was added to the sections and incubated for 60 (VLA) or 90 (NCFAD) sec. Preliminary optimization assays demonstrated that this step was time and temperature dependent and performed most reliably if the solution was removed from the refrigerator within 5–10 min of use. The PK pretreatment caused partial digestion of the tissue sections in some cases, although this did not affect the final observations. Sections were immunolabeled with sequential 10-min incubations at room temperature with primary antibody at 1 or 10 μg/ml, antimouse-IgG-biotin, and streptavidin-horseradish peroxidase complex with intervening wash buffer rinses. Five hundred microliters of DAB was added as the enzyme substrate for 3–5 min (endpoint determined macroscopically by NCFAD) or 10 min (standardized by VLA). Deionized water was added and the coverplates were removed. The slides were washed for 2 min in running tap water, counterstained with Mayer's hematoxylin, and blued in Scott's Tap Water i (NCFAD) or tap water (VLA). After thoroughly washing in running tap water for 4 min, the slides were dehydrated and placed into xylene, then permanently mounted with mounting media.
Two pathologists and 2 technicians evaluated each coded slide using brightfield light microscopy. Samples were considered positive if there was evidence of chromogen deposits conforming to disease-associated patterns of labeling 17,18 in the dorsal nucleus of the vagus nerve and the solitary tract nucleus, the regions previously described as target areas for PrPSc accumulation. 18 Disease-specific labeling in samples immunolabeled with this protocol was as described previously for BSE using other antibodies 3,17,18 and corresponds to some, but not all, forms of immunolabeling reported in sheep with scrapie 5,7,11 using polyclonal antisera and other antibodies and in deer and elk with chronic wasting disease, 13,14 in a variety of manual and automated protocols. Multifocal particulate labeling (also termed “punctate” 5 or “synapse-like” 18 ) predominated, with variably sized, irregular particles distributed in a random fashion through the neuropil without obvious association with morphologically defined cells or structures. This labeling was most commonly evident as separate fine particles but was sometimes also aggregated (Fig. 1A). Perineuronal labeling appeared similar to the particulate labeling, but was clearly distributed in close association with the neuronal membrane around the perikaryon (Fig. 1B) and bordering neurites. Throughout the sections there was glial-associated labeling (Fig. 1C). The most obvious cell-associated disease-specific labeling was a granular labeling of the perikaryonal cytoplasm of neurons. This labeling was either diffusely distributed throughout the cytoplasm or localized, sometimes with a perinuclear location. Labeled granules were usually round and variable in size (Fig. 1D). The specific labeling patterns observed in the hypoglossal nucleus were predominantly neuronal with some perineuronal particulate labeling. The dorsal nucleus of the vagus nerve demonstrated mainly coarse granular neuropil labeling and occasional intraneuronal labeling. In the reticular formation, linear particulate and coalescing labeling patterns were evident. Samples were considered negative if no chromogen deposits were observed or if the disease-associated patterns of labeling were absent.
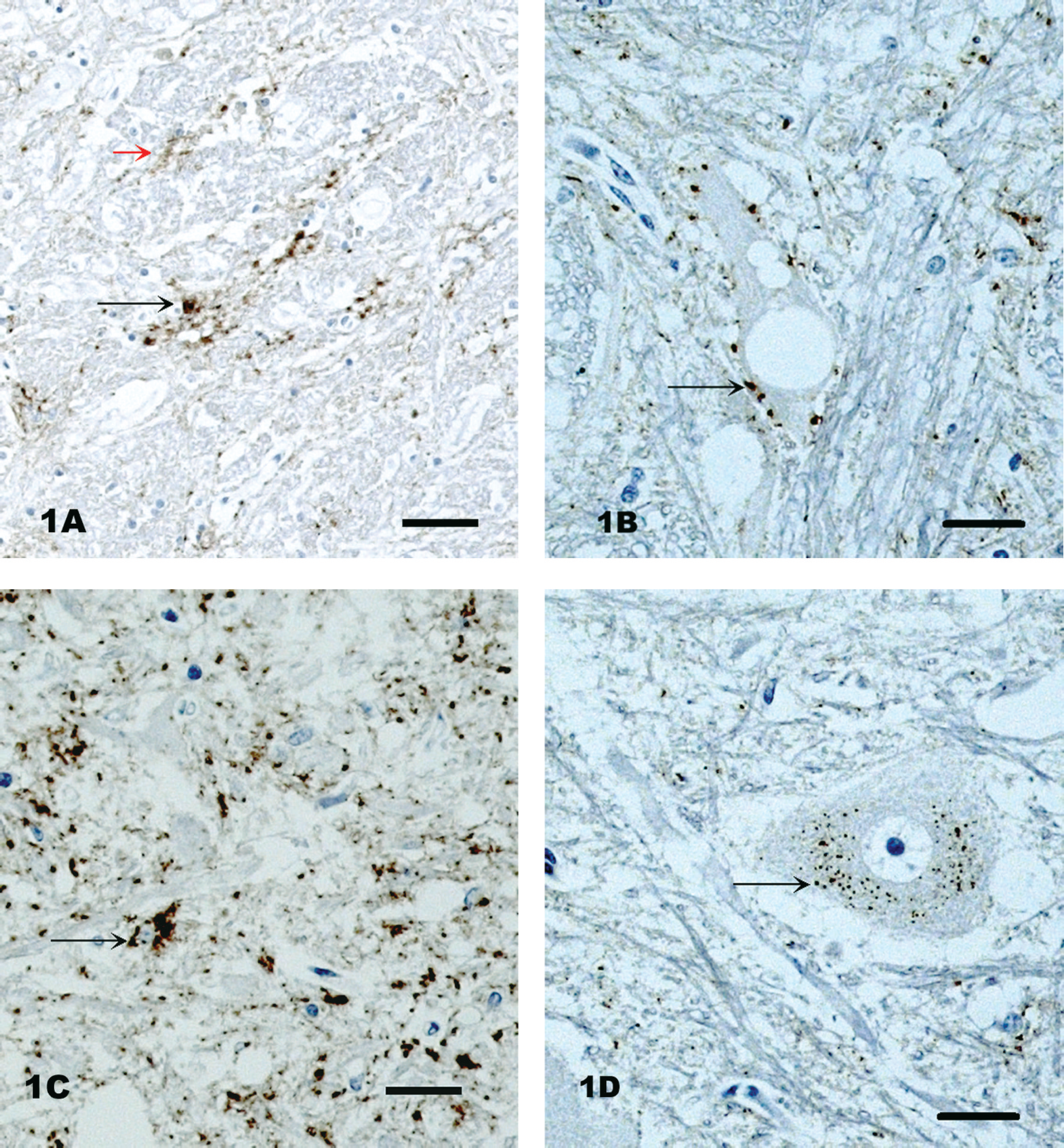
Immunohistochemical detection of bovine spongiform encephalopathy in various bovine brainstem regions.
Results from both laboratories were tabulated at NCFAD. The performance of each immunohistochemistry (IHC) run was monitored by using BSE-positive control tissue sections and documented as 100% repeatable within each laboratory. All 100 positive and 500 negative cases were correctly identified by both laboratories, yielding 100% sensitivity, specificity, and reproducibility. 19 These findings were derived in spite of minor variation between the laboratories in neuroanatomic sample site selection, fixation and processing, and immunolabeling protocols, as well as inherent differences in local water supply and laboratory room temperatures. The results obtained by the 2 national reference laboratories confirm the robustness and validity of these procedures for the detection of BSE field cases. Subsequent to this study, mAb F99/97.6.1 was included in the panel of antibodies used in the confirmatory IHC testing schedule for BSE diagnosis at the NCFAD. Eight Canadian BSE cases and 2 U.S. BSE cases were confirmed with this antibody, including atypical BSE cases in the United States 10 and Canada (unpublished data). The availability of a standardized, complete IHC kit for the detection of PrP is useful to laboratories that perform primary screening and/or confirmatory testing of small numbers of cattle by manual IHC. The kit procedure is easily adapted to automated staining systems 1 with minor modifications to the heat induced epitope retrieval timings. The NCFAD laboratory subjected their slides to 25 min of hydrated autoclaving greatly enhanced the specific staining signals in their automated staining processes. Since its initial use, individual laboratories have introduced modifications to the generic protocol which, in common with other commercial immunodetection systems, should be subject to proficiency testing controlled by the appropriate BSE reference laboratory. 19
Acknowledgements. The authors thank Yves Robinson (NCFAD) and Peter Wright (Deputy Director, Canadian Food Inspection Agency) for providing invaluable input into this study. Case selection and technical assistance provided by staff of Pathology Department of the VLA are gratefully acknowledged. Mention of trade names or commercial products in this article is solely for the purpose of providing specific information and does not imply recommendation or endorsement by the U.S. Department of Agriculture.
Footnotes
a.
Bovine Spongiform Encephalopathy Antigen Test Kit, Immunohistochemistry, VMRD Inc., Pullman, WA.
b.
Paraplast
c.
FibroWax, Van Loenen Instruments, Zaandam, The Netherlands.
d.
ProbeOn Plus Slides, Fisher Scientific Company, Ottawa, Ontario, Canada.
e.
VECTABOND
f.
Shandon Coverplate
g.
Shandon Sequenza® Slide Rack, Thermo Fisher Scientific Inc., Waltham, MA.
h.
Tris-Buffered NaCl Solution with Tween 20, pH 7.6, Dako Canada Inc., Mississauga, Ontario, Canada.
i.
Surgipath Medical Industries, Richmond, IL.