
Abstract
Canine respiratory coronavirus (CRCoV) has been detected in dogs suffering from respiratory disease and is thought to be involved in canine infectious respiratory disease (CIRD) complex. Canine enteric coronavirus (CECoV) is a widespread pathogen of dogs, responsible for mild to severe diarrhea in pups. The purpose of this study was to establish the seroprevalence of CRCoV in Italy and its relationship to CECoV type II seroprevalence. The age and year of sample collection from seropositive dogs was also assessed. Of adult domestic dogs, 23.3% had antibodies to CRCoV, compared with 86.1% with antibodies to CECoV. Amongst a population of kenneled pups, 4.0% had antibodies to CRCoV, and 97.0% had antibodies to CECoV.
Canine respiratory coronavirus (CRCoV) has been identified in the respiratory tract of dogs from a large humane-adoption facility with a high prevalence of canine infectious respiratory disease (CIRD). It has been hypothesized that CRCoV may have a role in canine respiratory disease. 9 CIRD is a common contagious disease characterized by acute onset of a dry, hacking and paroxysmal cough. The disease is often mild and recovery rapid; however, in some cases interstitial pneumonia or severe bronchopneumonia develop and can be fatal. 1 A number of pathogens have been associated with CIRD, including canine adenovirus 2 (CAV-2), canine parainfluenza virus (CPIV), Bordetella bronchiseptica, canine herpesvirus (CHV), and mycoplasmas, and disease may result from one or a combination of these agents. 3,5,6,12
CIRD is usually only a problem when groups of dogs are kept together under crowded conditions, such as in animal shelters, laboratory animal units, and training kennels. Despite widespread vaccination, CIRD remains a persistent global problem. In addition to the obvious welfare implications and costs of treatment, the disease also delays and disrupts re-homing and training schedules of kennels and shelters.
The seroprevalence of CRCoV in the domestic canine population has been shown to be 59.1% in Canada, 54.5% in the United States, 36.0% in the United Kingdom, 30.3% in the Republic of Ireland, and 17.8% in Japan. 11,18 The seroprevalence rate of CRCoV has been shown to increase with age in both UK and US canine populations and to decline following a plateau phase between 2 and 11 years. 18
The other coronavirus of dogs, canine enteric coronavirus (CECoV) is known to be widespread in the dog population. CECoV is divided into 2 genotypes: CECoV type I is genetically similar to feline coronavirus (FCoV) type I and CECoV type II to FCoV type II. 16 Antibodies have been detected in 54% of a population of healthy and diarrheic pet dogs in the United Kingdom, 19 while CECoV seroprevalence ranged from 76% in a rescue kennel to 100% in a commercial breeding colony. 20 These studies demonstrate that seroprevalence rates depend on the population of dogs tested with generally higher rates in endemically infected kennels, where population densities are high and there is a continuous influx of susceptible animals and pathogens as a result of high dog turnover. In the United States, the seroprevalence of CECoV was 26% for pet dogs and up to 87% for kenneled dogs. 10
A low genetic similarity has already been demonstrated between CRCoV and CECoV. The 2 canine coronaviruses have sequence identity of 68.5%, based on the polymerase gene, and only 21.1%, based on the spike gene, which is considered to be the primary immunologic determinant of the virus. 9 Erles et al. have shown that, in a population of dogs entering a humane-adoption facility, there was no correlation between antibodies to CRCoV and CECoV or between the presence of antibodies to CECoV and the development of respiratory disease. 9
This study aimed to establish serologic evidence of CRCoV in Italy in both kenneled and domestic dog populations, to compare the seroprevalence of CRCoV and CECoV type II, and to examine the influence of age and year of serum collection on seroprevalence.
This study used 590 heat-inactivated canine sera from the Department of Animal Health and Well-being, Faculty of Veterinary Medicine, Bari, Italy. The sera were all collected from southern Italy. One hundred sera were collected from young pups in various kennels in the Apulia region, where CECoV was a particular problem. Four hundred and ninety adult dog sera, submitted for diagnostic purposes, were obtained from several small animal clinics in southern Italy.
CRCoV enzyme-linked immunosorbent assay (ELISA) was performed as described by Priestnall et al. with minor modifications. 18 In brief, 96-well ELISA plates a were coated with 20 μg/ml of CRCoV antigen and uninfected cell control diluted in phosphate-buffered saline (PBS). CRCoV UK isolate 4182 multiplicity of infection (MOI) = 0.1 obtained from a clinical case of CIRD (Erles, K. et al., Isolation and sequence analysis of canine respiratory coronavirus, Virus Res. (2006), doi:10.1016/j.viruses.2006.10.004) was used to infect human rectal tumor (HRT-18) cells and the whole cell lysate used as CRCoV antigen. The plates were incubated overnight at 37°C, and then washed 3 times with PBS containing 0.05% Tween-20 (PBS-T). Sera were diluted 1/100 in PBS-T and added to each of the CRCoV antigen-coated and control wells (50 μl per well). The sensitivity and specificity of the ELISA were previously determined to be 95.6% and 96.7%, respectively, at this serum dilution when compared with immunofluorescence assay. 18 Plates were incubated at 37°C for 60 minutes, and then washed 4 times with PBS-T. All incubation stages were performed in a humid atmosphere to prevent drying of the wells. Peroxidase-labeled rabbit anti-dog IgG b was diluted 1:5000 in PBS-T and 50 μl added to each well, followed by incubation for 60 minutes at 37°C. Plates were washed 3 times with PBS-T and shaken dry. OPD (o-phenylenediamine) peroxidase substrate b was prepared according to the manufacturer's instructions and 100 μL added to each well. The plates were incubated in the dark at room temperature for 10 minutes. To stop the reaction, 50 μL of 2MH2SO4 was added to each well. The optical density (OD) was measured at 405 nm using a microplate reader. c The cut-off value was defined as mean OD plus 3 standard deviations calculated from a panel of 28 canine control sera (negative for CRCoV antibodies). The adjusted OD values of each sample were obtained by subtracting the absorbance of the mock antigen-coated well from that of the corresponding virus antigen-coated well.
CECoV type II ELISA was performed as described by Pratelli et al. with minor modifications. 14 CECoV type II antigen was prepared from Crandell feline kidney (CrFK) cells infected with CECoV strain 45/93, or mock infected to produce control antigen. In brief, 96-well microtiter plates were coated with 25 μg/ml of CECoV antigen diluted in coating buffer (15 mM Na2CO3, 35 mM NaHCO3, 0.02% NaN3 [pH 9.6]) and incubated overnight at 4°C with shaking to ensure adequate antigen adsorption. Plates were then washed 4 times with PBS-T and treated with blocking solution (0.2% gelatin in coating buffer) for 90 minutes at 37°C. After a further 4 washes, 100 μl of each dog serum diluted 1/50 in PBS-T was added in duplicate, and the plates were incubated for 90 minutes at 37°C. In a previous study, sensitivity and specificity for the assay were determined comparing ELISA with virus neutralization (VN) test. 14 Considering VN as a “gold standard” test, ELISA showed a sensitivity of 100% and a specificity of 34.5%, with an overall agreement of 82.6%. The wash cycle was repeated 4 times, then goat anti-dog IgG labeled with peroxidase b was added to each well, and the plates were incubated for 60 minutes at 37°C. After an additional 4 wash cycles, 100 μl/well of freshly-prepared substrate ABTS [2,2′-Azino-bis (3-ethylbenzothiazoline-6-sulfonic acid)] b in 50 ml phosphate citrate buffer 0.05 M, pH 5.0, containing 0.025% H2O2, was added and the plates were incubated for 25 minutes at room temperature. After adding the stop buffer solution (1% sodium dodecyl sulfate), the OD was measured at 405 nm using an automatic ELISA reader. d The cut-off value was defined as the mean OD plus 3 standard deviations calculated from 10 negative dog sera used as control. The adjusted OD value of each sample was obtained by subtracting the OD of the mock antigen-coated well from that of the corresponding virus antigen-coated well.
The Fisher's exact test was used to evaluate the statistical significance of differences among seroprevalence values, including the influence of age on the seropresence of CRCoV and the relationship between the seroprevalence of CECoV and CRCoV at a particular age. Differences in seroprevalence values between years of sample collection were also examined using the Fisher's exact test.
In order to extend the data on the epidemiology of CRCoV, the present study investigated the presence of canine antibodies to CRCoV in Italy. Twenty percent (118/ 590) of all dogs sampled were found to be seropositive for CRCoV compared with 89.2% (313/351) for CECoV type II. This difference was most marked in the dogs less than 1 year old; 4% (4/100) of pups had antibodies to CRCoV, while 97% (97/100) had antibodies to CECoV (P < 0.0001).
Amongst adult domestic dogs (>1 year old), the seroprevalence of CRCoV was lower than previously reported in other countries. In Italy, 23.3% (114/490) of adult dogs were seropositive for CRCoV, which is less than in the United Kingdom (36.0%) and just over half of the 54.7% seroprevalence in North America. In the United Kingdom and Ireland, CRCoV antibody prevalence among pet dogs appeared to correlate to some degree with population density. 18 The difference in seroprevalence observed between southern Italy and the United Kingdom may therefore be explained by the lower population density (and possibly domestic dog density) in southern Italy. The low seroprevalence of CRCoV noted in the kenneled pups suggests that the premises studied were either naïve to CRCoV or had a very low incidence of the virus at the time of the sampling. Previous work on kenneled dogs found that antibody responses to CRCoV coincided with outbreaks of respiratory disease and that the virus may have a seasonal occurrence. 8
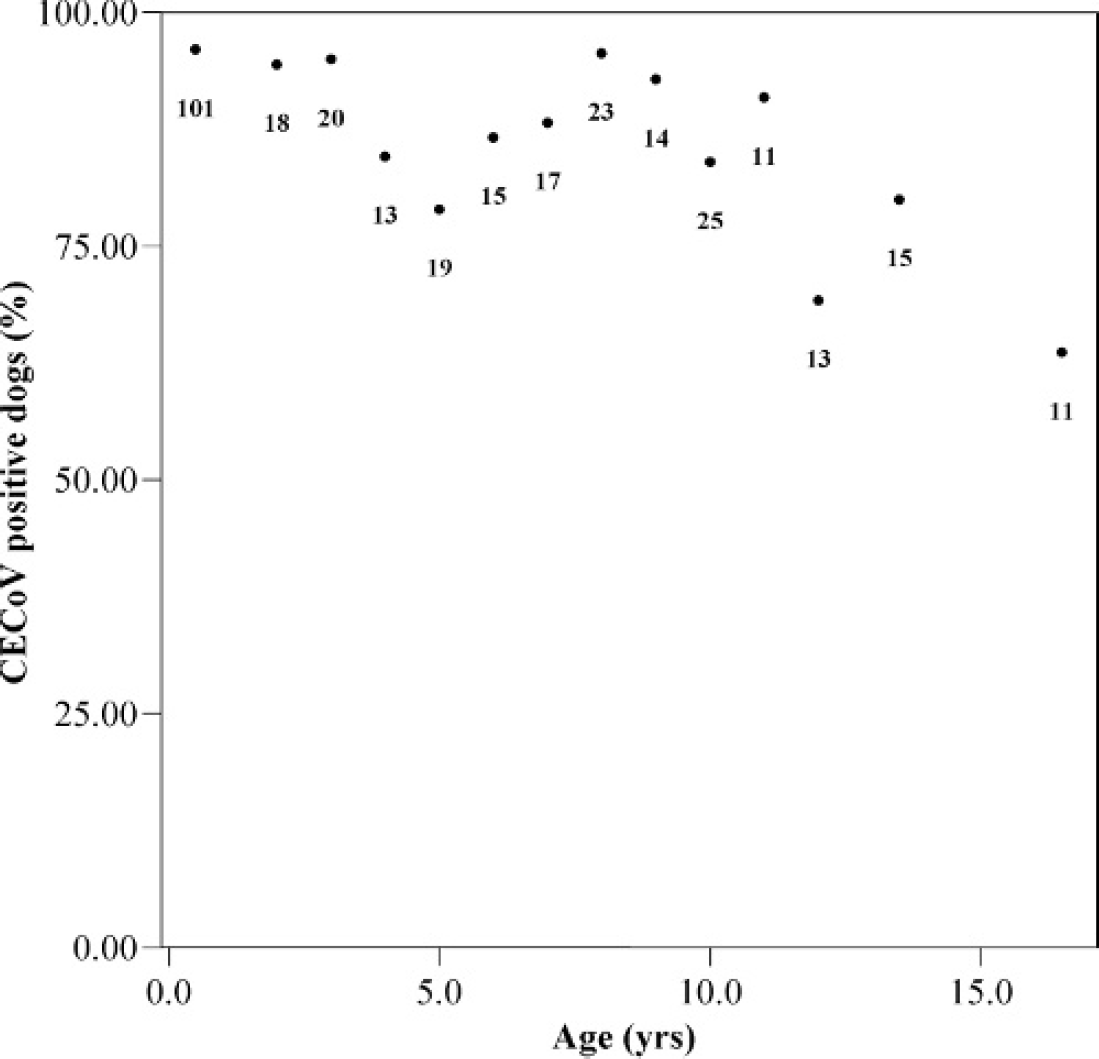
The relationship between age of dog and the presence of CRCoV or CECoV type II antibodies was examined (Figs. 1, 2). The percentage of dogs with antibodies to CRCoV increased with age to a peak seroprevalence of 40.0% (12/30) at 9 years and appeared to decline after 9 to 11 years of age. This finding is in agreement with previously demonstrated age distributions in the United Kingdom and United States. 18 Age appeared to influence the prevalence of antibodies to CRCoV, with dogs less than 1 year of age more likely to be seronegative for CRCoV compared with older dogs (P < 0.0001). Analysis of the percentage of CECoV type II seropositive dogs by age revealed an overall stable seroprevalence with 86.1% (216/ 251) of adult dogs seropositive. This high rate of seropositivity was maintained until 12 years of age, when a gradual decline was seen, possibly because of reduced immune efficiency and antibody production with age. A smaller decline in seropositivity rates was also seen between 3 and 8 years. The difference in seroprevalence between CECoV and CRCoV and was found to be statistically significant for the following age groups: 0.5 and 3 years (P < 0.0001); 2 and 7 years (P < 0.01); and 4, 5, 6, 8, and 10 years (P < 0.05).
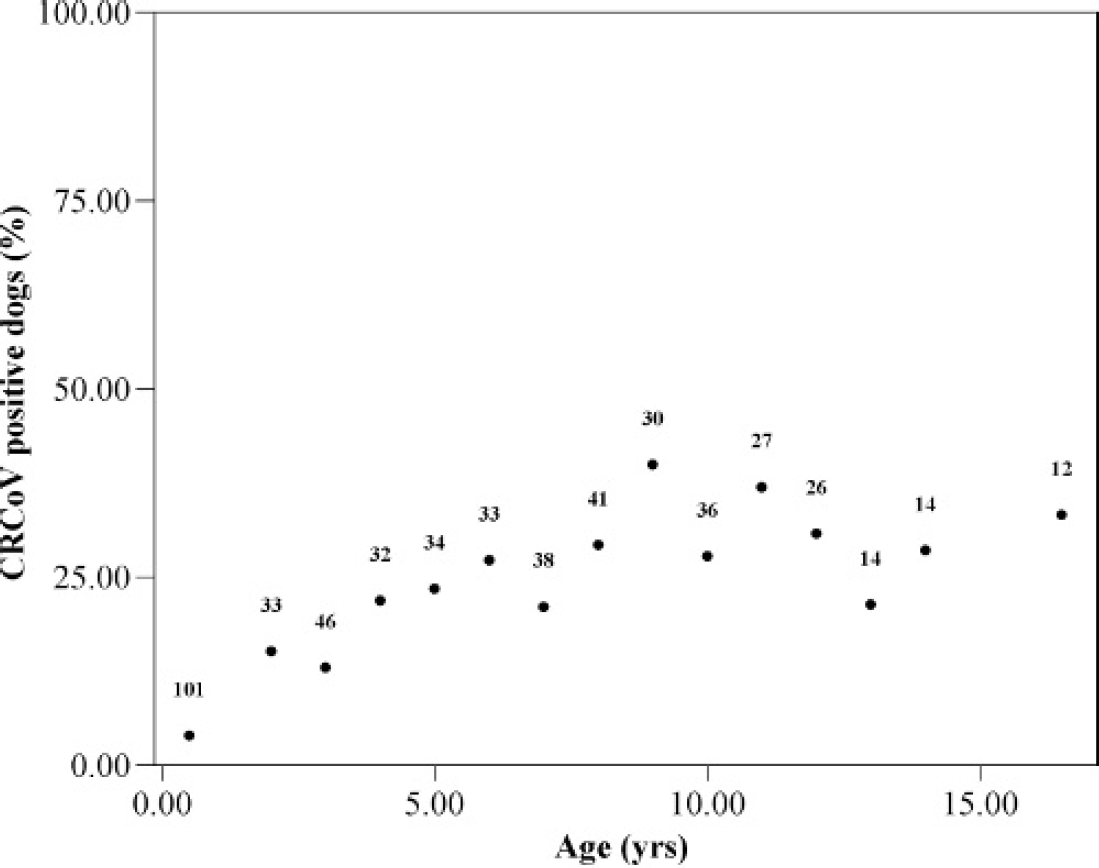
Relationship of CRCoV antibody status to age in canine serum samples (n = 517) from southern Italy. Labels indicate the number of samples associated with each data point.
Seroprevalence of CECoV seems to depend on the environment of the population of dogs sampled; animal shelter or breeding colony dogs have a larger number of social interactions and a greater opportunity for exposure to virus. The seroprevalence of CECoV type II in 100 pups from shelters with outbreaks of enteric disease was found to be 97.0%. This high seropositivity rate is in accordance with other reports from different researchers around the world. 2,14,21 In a previous study of adult domestic Italian dogs, 73.4% were found to be seropositive for CECoV type II by ELISA compared with 86.1% of adult dogs in the present study. 14 These differences in seroprevalence were almost certainly due to the presence of active CECoV infections in the animal shelter studied. This was an “open” shelter with a high turnover of susceptible animals (young dogs). The infection also appeared to be endemic because CECoV was detected in the shelter on several occasions (data not shown). Moreover, it is known that the virus may become established in the population either by continuous reinfection from the environment, other dogs, or both, or by the development of chronic infections in some animals. 15,17 CECoV type II is thought to have arisen from a recombination event between FCoV and CECoV, resulting in FCoV-like CECoV strains, based on sequencing of the M gene; thus interspecies spread between cats and dogs may be important. 4,15 The virus has a low stability in normal environmental conditions and appears to be labile in the feces, thus frequent virus shedding from infected animals would be required to maintain the virus in the environment. 13 Considering the close confines and the overcrowding of the shelter, constant reinfection from infected feces and recycling around the premises may maintain high levels of the virus and cause the high seropositivity observed. Of interest >90% of 8- to 9-year-old domestic dogs had antibodies to CECoV type II, approaching the seroprevalence in young pups housed in a shelter where CECoV was endemic. This finding suggests that environment may have less of an effect on the seroprevalence of CECoV in Italy. Tennant et al. 20 examined the age of seroconversion in different environments and found that in an animal shelter, there was no difference in the seroprevalence of CECoV between dogs less than or more than 4 months of age.
The year of sample collection was evaluated with respect to CRCoV seroprevalence; however, no significant differences in CRCoV seroprevalence were found (Fig. 3). The year 2001 appeared to have the lowest CRCoV seroprevalence (7.7%); however, the sample number was small. The year 1999 also had a low seroprevalence (10.1%) despite a high sample number; however, the mean age was lower (2.19 years) than the other years for which samples were available (6.7 to 8.0 years), indicating a possible age influence. The highest seroprevalence was detected in 2005 (29.4%). These data do however show that CRCoV seroprevalence does appear to be stable in the canine population of southern Italy.
CECoV may have been present within the worldwide canine population for longer than CRCoV. The earliest evidence of CRCoV to date is from 1996 in 2 Canadian pups with respiratory disease. 7 Circulation of CECoV for longer would lead to an increased chance of infection and the establishment of a higher seroprevalence from a younger age. Chronic infections and long-term shedding could also explain an overall higher seroprevalence of CECoV. To examine these theories, further work needs to be performed to look at the potential for the development of long-term shedding states during CRCoV infection and establish whether CRCoV is a true emergent infection or whether simply being overlooked, precluded earlier discovery.
Acknowledgement. This study was supported by a PhD scholarship (S. L. Priestnall) from The Royal Veterinary College, North Mymms, Hatfield, Hertfordshire, UK.
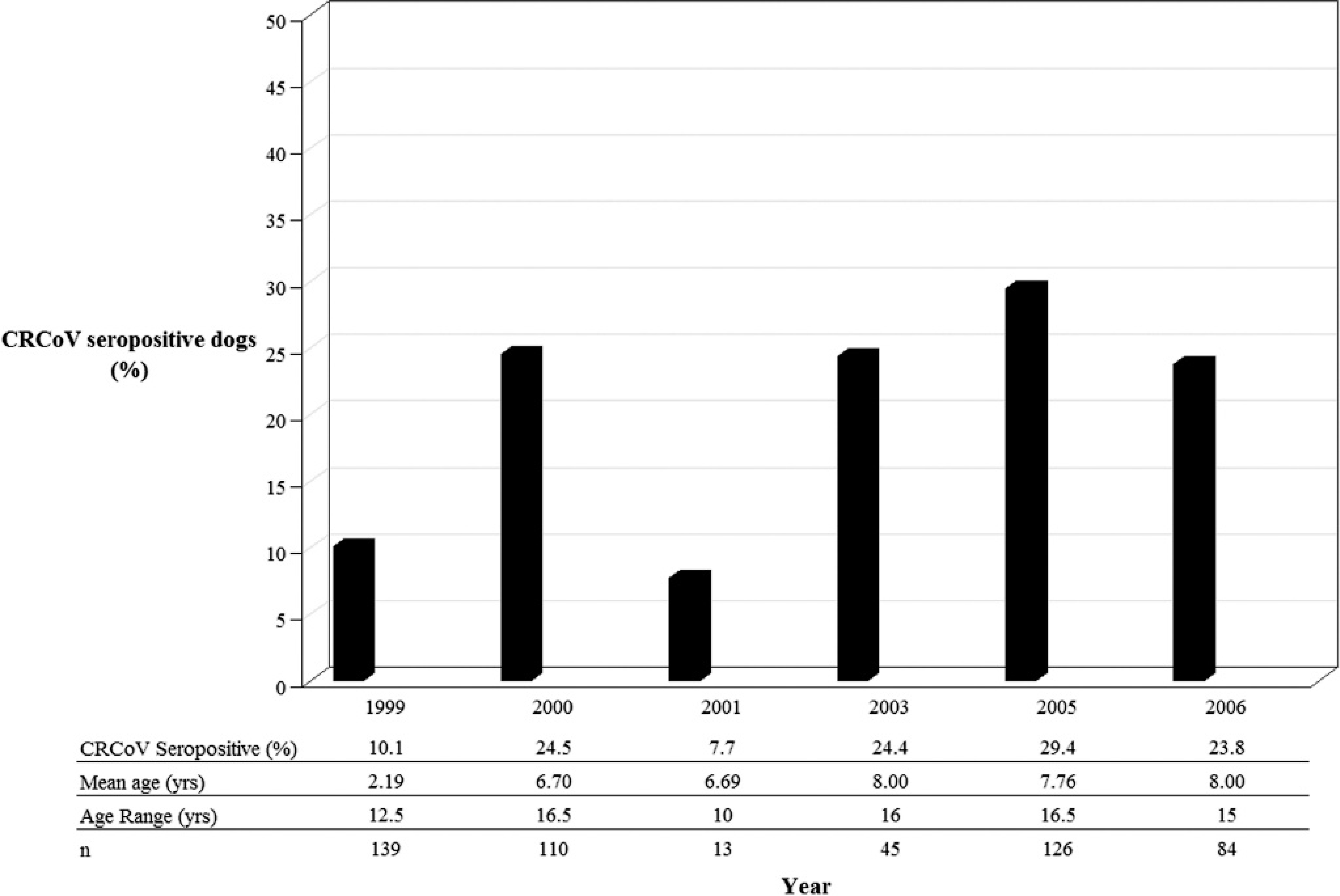
Relationship of CRCoV antibody status to year of sampling (n = 517).
Footnotes
a.
Maxisorp, Nunc, Roskilde, Denmark.
b.
Sigma-Aldrich Co., Poole, Dorset, UK.
c.
SpectraMax M2, Molecular Devices, Ltd., Wokingham, Berkshire, UK.
d.
Bio-Rad, Hemel Hempstead, Hertfordshire, UK.