
Abstract
Objective
This study aimed to assess the adherence to guidelines in the prescription of sodium valproate (SV) to women of childbearing potential (WOCP) in Southern District Mental Health Services (SMHS) in New Zealand (NZ).
Methods
Electronic records of women aged 18–54 who were newly prescribed SV by SMHS between the 1st of January 2018 and the 31st of December 2019, were retrospectively reviewed. Documentation of the following criteria was examined: pre-commencement pregnancy test, education on the teratogenic potential of SV and/or the importance of avoiding unplanned pregnancy, information on contraception, and the rationale for prescribing SV over alternative treatments.
Results
Among the 3065 WOCP who had contact with SMHS during the study period, 51 women were newly prescribed SV and at risk of pregnancy. Twenty-one women (41%) had a recorded reason for prescribing SV over alternative treatments, four women (8%) underwent a pre-commencement pregnancy test, 10 women (20%) received information about the teratogenic potential of SV and/or the importance of avoiding unplanned pregnancy, and 21 women (41%) had documentation regarding contraception.
Conclusion
The study findings indicate heterogeneous and suboptimal documentation of specific risks associated with SV use in WOCP in SMHS. Interventions are needed to improve prescribing and documentation practices.
In New Zealand (NZ) and Australia, sodium valproate (SV) is approved for the treatment of epilepsy and acute and recurrent mania in bipolar disorder. 1 Additionally, SV is used off-label in psychiatry to manage affective symptoms or mood instability in diagnoses other than bipolar disorder. 2
Data from the United Kingdom, North America, Europe, and Australia indicate that infants exposed to SV in utero have a risk of congenital malformations ranging from 6%–12%, compared to a baseline rate of 2%–3%.3–5 Furthermore, approximately 30%–40% of children exposed to SV in utero may experience adverse neurodevelopmental outcomes, including reduced IQ, specific deficits in speech and language, and, in severe cases, global developmental delay.6–8 The prevalence of autism spectrum disorder and attention-deficit/hyperactivity disorder also appears to be higher among children exposed to SV in utero.9,10
Guidelines endorsed by the European Medicines Agency and the Medicines and Healthcare Products Regulatory Agency recommend avoiding the use of SV in women of childbearing potential (WOCP).
11
If there are no suitable alternative treatments, SV can be used if the conditions of a pregnancy prevention program (PPP) are met (see Figure 1).
11
Similar guidelines have been endorsed by the Royal Australian and NZ College of Psychiatrists (RANZCP).
12
While NZ currently does not have a national PPP, agencies such as the Medicines and Medical Devices Safety Authority (Medsafe) and The NZ Formulary (NZF) have issued similar recommendations.1,13 Summary of conditions included in the pregnancy prevention programme published by the European Medicines Agency and the Medicines and Healthcare Products Regulatory Agency.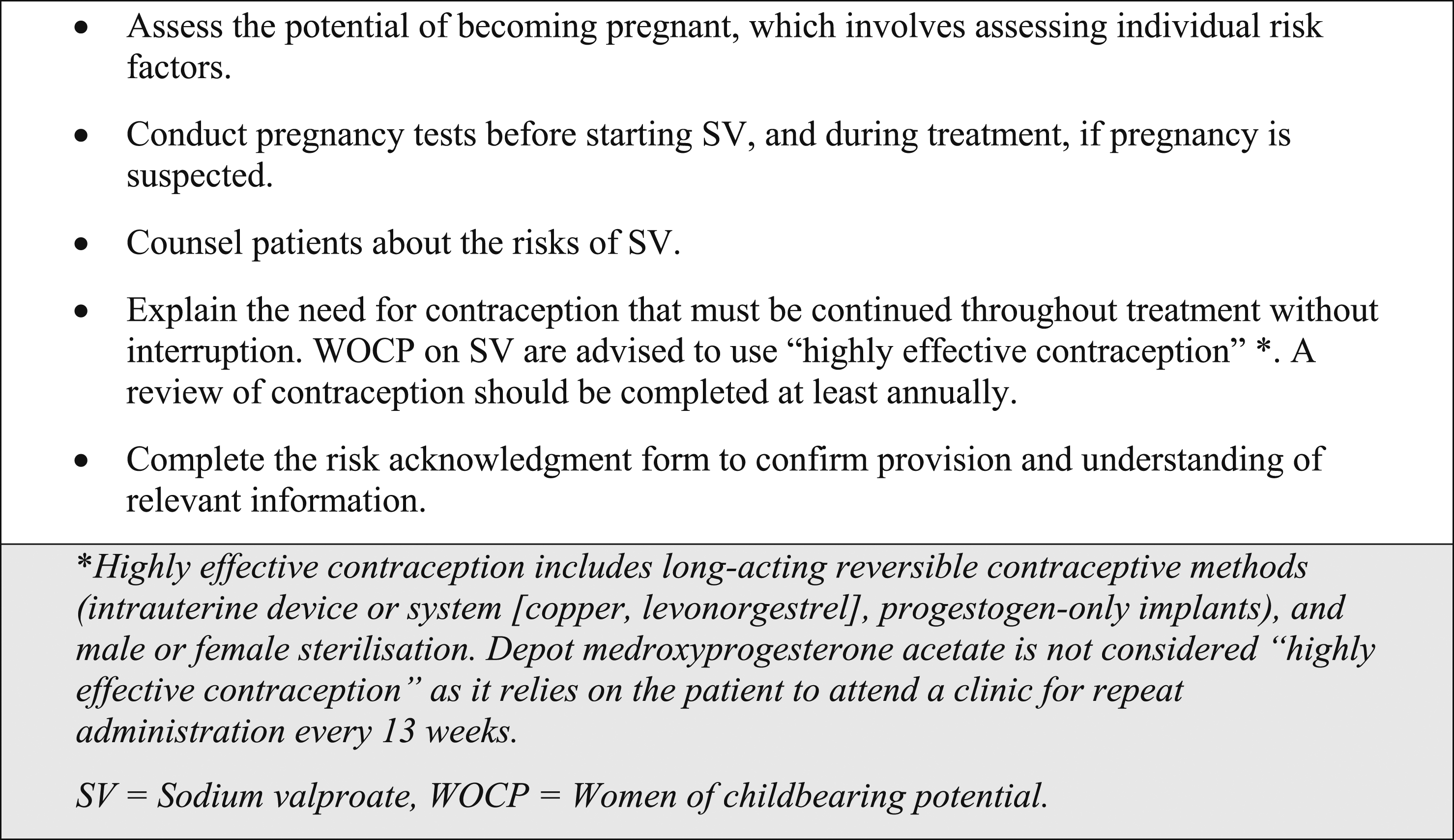
Research from international and national sources indicates suboptimal documentation of patient education regarding the specific risks of SV in WOCP in mental health services.14–17 This issue was further highlighted in a 2022 Health and Disability Commissioner Report, which involved a woman who became pregnant whilst on SV. 18
Given the significant clinical implications of non-adherence to guidelines, this study aims to assess the extent to which guidelines are followed in the prescription of SV to WOCP in Southern District Mental Health Services (SMHS).
Methods
The electronic patient management system was used to identify women aged 18–54 who were recorded as having at least one contact with inpatient or outpatient SMHS between the 1st of January 2018 and the 31st of December 2019. The upper age limit of 54 was chosen to align with the typical age range of menopause. 19 Women aged under 18 and those receiving treatment from Forensic or Intellectual Disability Services were excluded for ethical reasons.
Electronic records were reviewed for documentation of the four following criteria at the time SV was first prescribed: • Reason for prescribing SV over alternative treatments. • Negative pregnancy test or justification for minimal pregnancy risk (e.g., menopause, hysterectomy, sterilisation, not engaging in sexual contact that places them at risk). • Education provided regarding the teratogenic potential of SV and/or the importance of avoiding unplanned pregnancy while taking SV. • Information related to contraception, including contraception status, type of contraception being used, and any prescriptions or referrals for contraception.
The electronic clinical records include all medical outpatient letters, hospital discharge summaries, prescription copies, pharmacy dispensing records, and biochemistry test results. As such, it represents an accurate record of all clinical decisions. Study IDs were assigned to both patients and prescribers to maintain confidentiality. The research received Decapitalise locality authorisation from Health Research South and obtained ethics approval from the University of Otago.
Results
Sociodemographic characteristics, MHA status, and DSM-5 diagnosis of the WOCP (n = 58) newly prescribed SV by SMHS
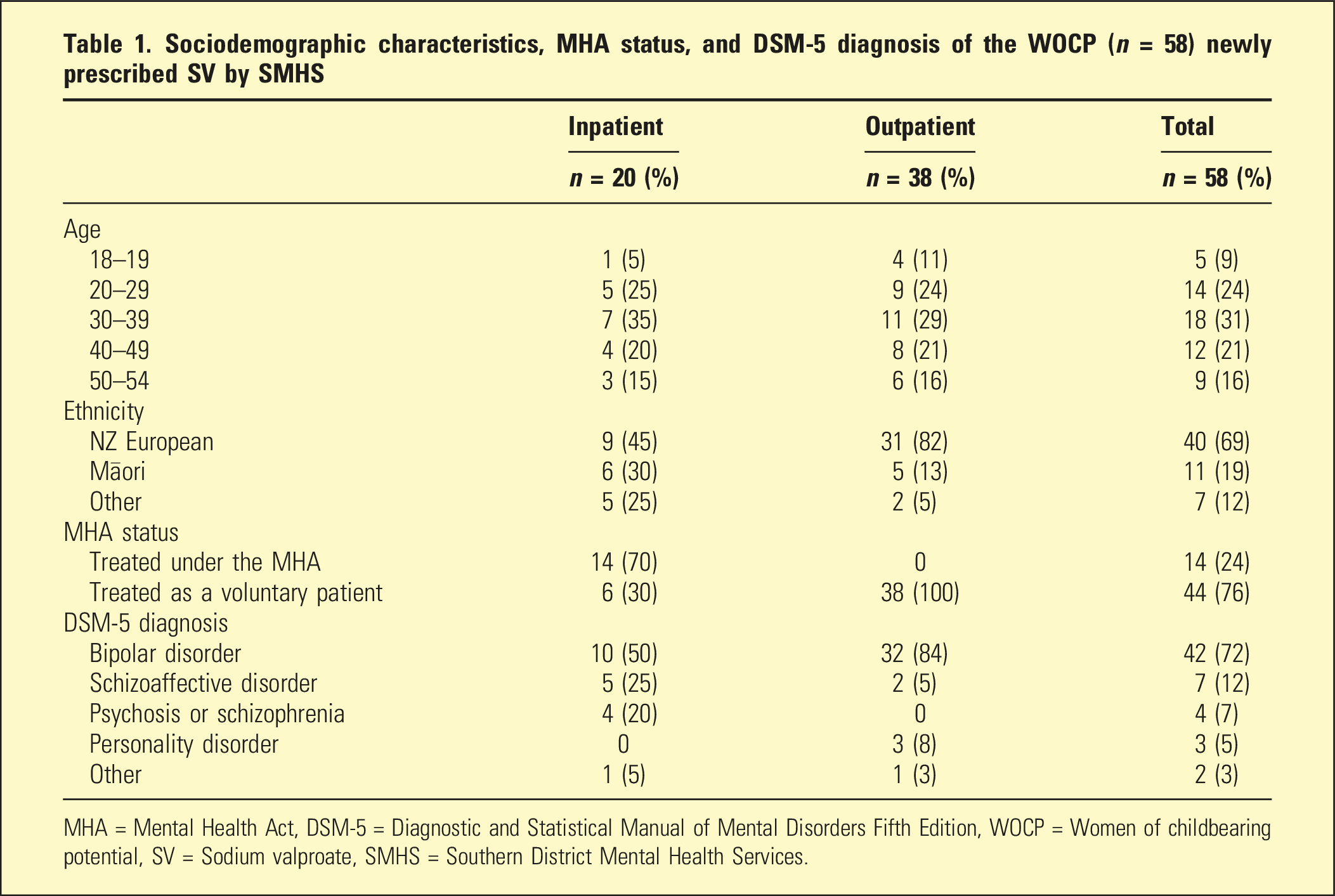
MHA = Mental Health Act, DSM-5 = Diagnostic and Statistical Manual of Mental Disorders Fifth Edition, WOCP = Women of childbearing potential, SV = Sodium valproate, SMHS = Southern District Mental Health Services.
Number of WOCP newly prescribed SV by SMHS and at risk of pregnancy (n = 51) with documentation of study criteria
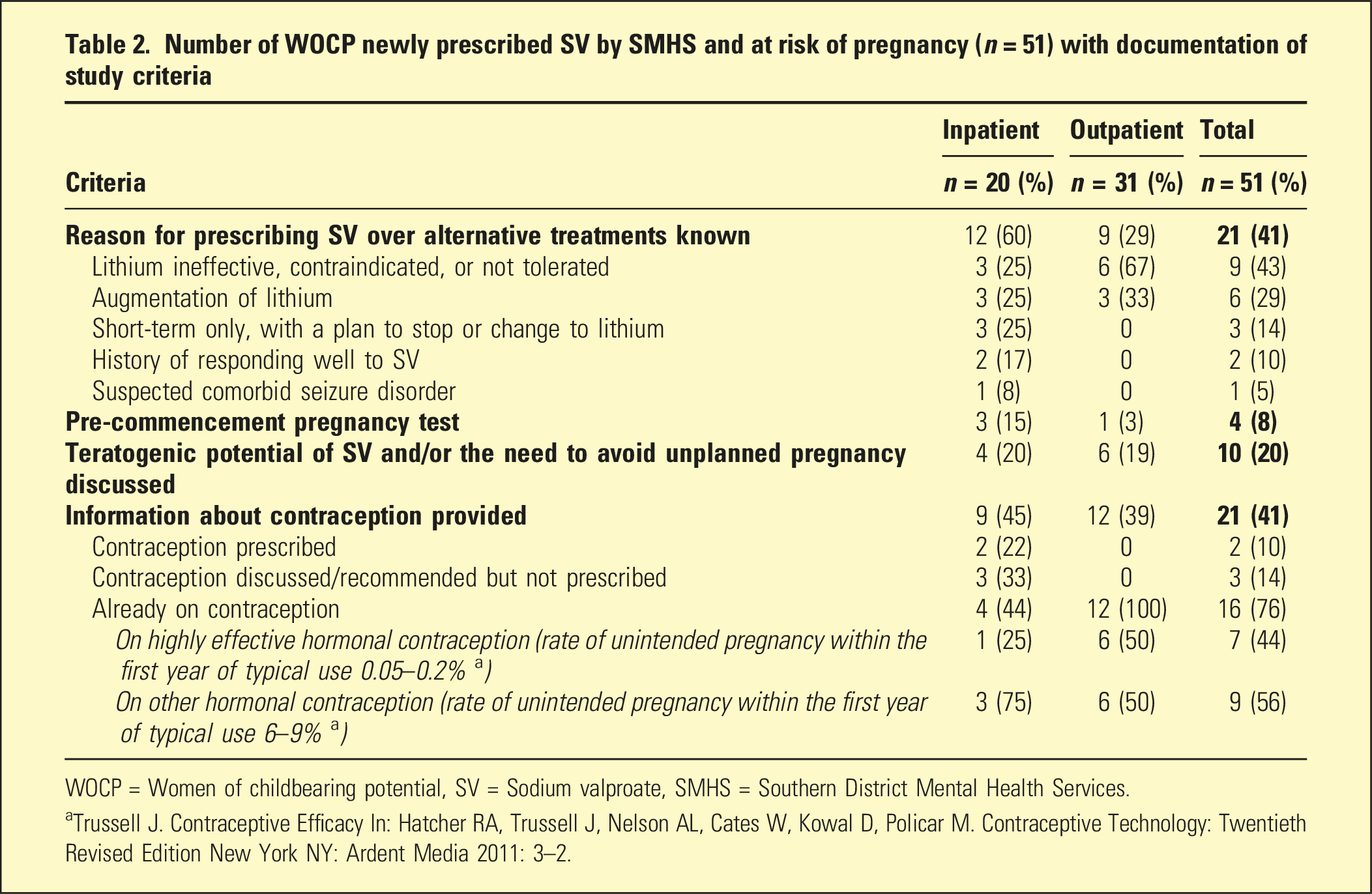
WOCP = Women of childbearing potential, SV = Sodium valproate, SMHS = Southern District Mental Health Services.
aTrussell J. Contraceptive Efficacy In: Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar M. Contraceptive Technology: Twentieth Revised Edition New York NY: Ardent Media 2011: 3–2.
Of the 21 women with documentation about contraception, only seven (44%) were on highly effective contraception. Among the two women prescribed contraception, only one was prescribed highly effective contraception.
A total of 14 women (27%) had no documentation of any of the four study criteria, 21 women (41%) had documentation of one criterion, 13 women (25%) had documentation of two criteria, and three women (6%) had documentation of three criteria. None of the patients had documentation of all four study criteria (see Figure 2). Bar graph showing the number of WOCP prescribed SV (black) and the average number of the four criteria documented (grey) by each prescriber. Consultant Psychiatrist IDs: P1-P15, P17-19, P22, P24. Psychiatry Registrar IDs: P16, P20, P21, P23. WOCP = Women of childbearing potential, SV = Sodium valproate.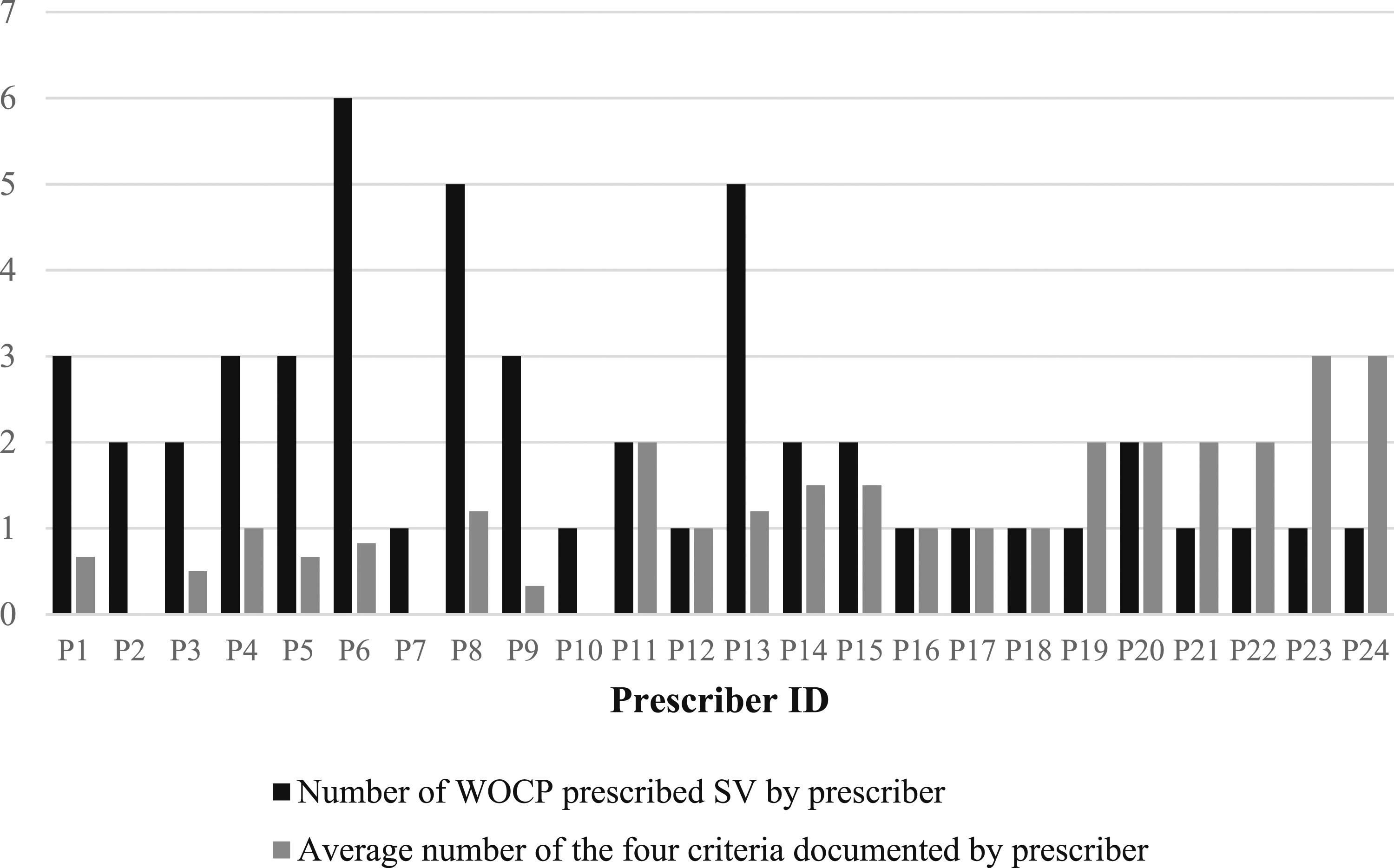
The study identified a total of 24 prescribers, including 20 consultant psychiatrists and four psychiatry registrars. Psychiatry registrars documented an average of two criteria per WOCP for whom they prescribed SV, while consultant psychiatrists documented an average of one criterion.
While variations in the documentation of individual criteria were observed, neither prescribers working in the inpatient nor outpatient setting demonstrated superiority in achieving complete documentation of all four criteria.
Documentation practices varied among prescribers and even among patients prescribed SV by the same prescriber. Notably, prescribers who used SV more frequently in WOCP did not demonstrate better adherence to guidelines.
Discussion
Given the well-established teratogenic and adverse neurodevelopmental effects of SV, all current guidelines recommend avoiding the use of SV in WOCP.1,11–13 In cases where no suitable alternative treatment exists, prescribers must take necessary steps to assess the patient’s pregnancy potential and provide comprehensive education regarding the associated risks of SV and the importance of using highly effective contraception while taking SV. Acknowledgement that this information has been provided and understood by the patient should be documented in clinical records to ensure patient safety and continuity of care. Despite the endorsement of these guidelines by reputable bodies such as RANZCP, Medsafe, and the NZF, this study found adherence to guidelines is suboptimal in SMHS. These findings are consistent with previous international and national research.14–17
None of the 51 WOCP newly prescribed SV and at risk of pregnancy had documentation that fulfilled guidelines. The absence of pregnancy testing before initiating SV is particularly worrisome, considering the elevated incidence of unplanned pregnancies among women with bipolar disorder. 20 Out of the 16 women who were already on contraception, seven were using highly effective methods when SV was prescribed. While none of the prescribers documented their rationale for omitting a pre-prescribing pregnancy test, it is possible that some refrained from conducting such tests for women who were already established on highly effective forms of contraception. If this possibility is considered, the pre-prescribing testing rate among the study population increases from 8% to 9%, which still remains inadequate.
A possible explanation for psychiatrists’ hesitancy in discussing and prescribing contraception is the practice of shared care, which assumes that patients are also registered with a general practitioner (GP) who may be better suited to provide advice on contraception options. 21 In NZ, accessing GP services can be challenging due to barriers such as cost, long wait times for appointments, and limited availability of spaces for registration with practices. Placing the responsibility solely on patients to arrange contraception with their GP puts them at risk of unplanned pregnancies without adequate follow-up and support.
One of the main findings of this study is the heterogeneity of documentation practices among prescribers, both between different prescribers and within the same prescriber for different patients initiated on SV. On average, psychiatry registrars documented two criteria per WOCP prescribed SV, whereas consultant psychiatrists documented only one criterion. The clinical and statistical significance of this finding is unclear, as neither registrars nor consultants consistently adhered to the guidelines in their documentation.
While interprescriber variation may be related to differences in training, knowledge, or experience with prescribing SV, it does not explain the intraprescriber variation. Although no discernible patterns emerged from the data to explain this intraprescriber variation, one potential explanation is that prescribers may be generally aware of the risks associated with the use of SV in WOCP but have a limited understanding of the specific information that should be discussed with patients and documented in their clinical notes. There may also be instances where these discussions have taken place but have not been adequately documented in the clinical notes. The failure to document these discussions places the prescriber at risk from a medicolegal perspective, which was highlighted in a recent report by the NZ Health and Disability Commissioner. 18 Despite the psychiatrist reporting verbal discussions about alternative options and associated risks with the patient, there was no documented evidence to support that these discussions about SV had occurred. 18 Consequently, the psychiatrist was found to have breached the Code of Health and Disability Services Consumers’ Rights. 18
Similar to the findings from Goldspink et al., 17 a large proportion of inpatients in SMHS were commenced on SV whilst being treated under the Mental Health Act. 17 Initiating SV in WOCP who are undergoing involuntary treatment puts them in a vulnerable position, as it grants the prescribing psychiatrist undue influence over decisions pertaining to their reproductive health.
Despite Māori making up 10% of the population in the Southern District, 19% of women in this cohort identified as Māori. 22 This overrepresentation of Māori aligns with the findings of Goldspink et al., 17 suggesting a systemic issue rather than a statistical anomaly. Considering the higher prevalence of bipolar disorder among Māori compared to other ethnic groups, there is a possibility that Māori WOCP with bipolar disorder face a disproportionately higher risk of being prescribed SV. 22 Further research is necessary to explore SV prescribing patterns specifically in Māori and other minority WOCP.
One limitation of this study is the exclusion of inpatient paper-based notes, which may have limited access to potentially relevant information about SV prescribing. This decision was based on the limited accessibility of these notes to other healthcare professionals and the expectation that important information should be documented in the electronic discharge summary.
Conclusion
The findings of this study indicate that the adherence to guidelines when prescribing SV to WOCP in SMHS is suboptimal. These findings, in conjunction with those from Goldspink et al., 17 highlight the need for interventions to enhance adherence to guidelines in NZ. Previous research has demonstrated that the introduction of protocols alone is insufficient to drive improvements in clinical practice.23,24 Therefore, system-based approaches that minimise cognitive burden on prescribers, such as automated inpatient prescribing alerts and community pharmacy dispensing alerts, are likely to be the most effective intervention strategies. The findings of this study have been communicated to the Southern District Leadership Group to facilitate the development of a comprehensive and collaborative district-wide management plan.
Ethical statement
This study was granted Decapitalise locality authorisation from Health Research South (ID01830) and ethics approval from the University of Otago (HD21/076).
Footnotes
Acknowledgements
We would like to thank Simon Jamieson, Amelia Needs, and The Ministry of Health Pharmaceutical Collection for assistance with data collection.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Otago Division of Health Sciences Summer Research Scholarship.
Correction (June 2024):
This article has been updated with minor grammatical or style corrections since its original publication.