
Abstract
Objective:
To identify distinct trajectories of antipsychotic use prior to and during pregnancy and describe the associated maternal and birth characteristics.
Methods:
We conducted a population-based cohort study of births (2005–2012) using linked administrative data in New South Wales, Australia. We used group-based trajectory modelling to classify trajectories of antipsychotic use in the 450 days prior to pregnancy and during pregnancy. We characterised women with different trajectories according to maternal sociodemographic characteristics, mental health diagnoses and hospitalisations, use of psychotropic medicines and birth outcomes.
Results:
Of 137,993 women who gave birth, 2741 (2.0%) were exposed to antipsychotics prior to or during pregnancy. We identified six trajectories of antipsychotic use: two involved short-term use of low daily doses prior to pregnancy (51.1%), while three involved long-term use of low (20.9%), moderate (11.0%) and high (2.0%) daily doses throughout pregnancy. One trajectory (15.0%) involved increasing use during pregnancy. Women with long-term use were more likely to have a schizophrenia or bipolar disorder diagnosis, to have used multiple psychotropics and to have a mental health hospitalisation during pregnancy. Overall, women using antipsychotics had elevated rates of adverse birth outcomes compared to unexposed women. Women with the greatest antipsychotic exposure had the highest rates of gestational diabetes and gestational hypertension.
Conclusion:
Women using antipsychotics around pregnancy are heterogeneous, with varying patterns of use and associated birth outcomes, reflecting underlying differences in the indications for treatment and/or severity of illness. This diversity should be considered when developing clinical guidelines and designing safety studies.
Introduction
The prevalence of mental health disorders in pregnant women is high (Andersson et al., 2003; Bennett et al., 2004) with 1 in 10 women dispensed a psychotropic medicine and 1 in 100 an antipsychotic during pregnancy (Hanley and Mintzes, 2014; Leong et al., 2017). While antipsychotics are primarily indicated for schizophrenia and bipolar disorder, they are increasingly being used off-label to treat other conditions such as depression, anxiety, insomnia and substance abuse (Alexander et al., 2011; Citrome et al., 2013; Gjerden et al., 2017). Consequently, the characteristics of antipsychotic users and the patterns of use have been changing over time (Alexander et al., 2011; Gjerden et al., 2017).
Antipsychotic use in pregnancy has increased in recent years (Park et al., 2017; Toh et al., 2013), yet the risks and benefits are not clear. While some studies have found an increased risk of congenital malformations (Coughlin et al., 2015; Habermann et al., 2013), most robustly designed studies have found little evidence of an increased risk (Chisolm and Payne, 2016; Cohen et al., 2018; Huybrechts et al., 2016; Petersen et al., 2016). However, abrupt discontinuation of antipsychotic treatment can lead to relapse during pregnancy or the postpartum period (Taylor et al., 2018; Viguera et al., 2011). Moreover, typical (first generation) antipsychotics have been linked to low birth weight and preterm delivery (Habermann et al., 2013), and atypical (second generation) antipsychotics are associated with maternal weight gain, gestational diabetes and increased infant size (Chisolm and Payne, 2016; Cohen et al., 2018). Establishing a causal association between antipsychotic use and poor birth outcomes is challenging, as bipolar disorder and schizophrenia are both associated with an increased risk of adverse birth outcomes regardless of treatment (Boden et al., 2012b; Kang-Yi et al., 2017; Tosato et al., 2017) and pregnant women with mental illness have high rates of smoking, substance abuse, use of multiple psychotropic medicines and obesity, all important risk factors for pregnancy complications (Chisolm and Payne, 2016). Not properly accounting for these potentially confounding factors may result in false associations, and several studies have found that the increased risk of certain poor birth outcomes observed in women using antipsychotics during pregnancy attenuate or disappear after adjusting for relevant health and lifestyle factors (Boden et al., 2012a; Petersen et al., 2016).
Despite the limited evidence, the use of antipsychotics in pregnancy is generally recommended in women with severe mental illness, due to the risks associated with untreated mental illness (Galletly et al., 2016; McAllister-Williams et al., 2017; Malhi et al., 2015). Given the increasing diversity of indications for antipsychotic treatment, there is great variability among people using antipsychotics, which to date has not been described in detail among women using antipsychotics prior to and during pregnancy. Many studies on the use of antipsychotics in pregnancy have found that reduced adherence and discontinuation is common (Leong et al., 2017; Margulis et al., 2014; Petersen et al., 2014); yet, most studies have been based on relatively crude measures of use, with limited consideration of duration of use and dosage. Thus, the objectives of this study were to (1) identify trajectories of antipsychotic use prior to and during pregnancy according to duration and dose, (2) describe the sociodemographic and mental health characteristics of women by trajectories of antipsychotic use and (3) describe the birth outcomes according to different trajectories of antipsychotic use.
Methods
Data sources
We conducted a population-based cohort study, using data linked for the Maternal Use of Medications and Safety (MUMS) Study (Havard et al., 2013). Specifically, we used linked records from the New South Wales (NSW) Perinatal Data Collection, the NSW Admitted Patient Data Collection, the Pharmaceutical Benefits Scheme (PBS) data and the NSW Registry of Births, Deaths and Marriages. The Perinatal Data Collection is a legislated and whole-of-population surveillance system of all live and stillbirths of ⩾20 weeks or ⩾400 g birth weight in NSW, Australia’s most populous state, and contains information on mothers and babies collected at the time of birth. The Admitted Patients Data Collection is a statutory data collection of discharges from public and private hospitals in NSW. The PBS dispensings claims data contain records for pharmaceuticals dispensed to Australian residents for which a government subsidy was paid. Australia has a publicly funded universal health care system which subsidises prescribed medicines; eligible patients pay a co-payment that varies depending on their beneficiary status (general or concessional), and the government subsidises the remaining cost (Mellish et al., 2015).
Study population
We included all women who gave birth from 1 January 2005 to 31 December 2012. We estimated the date of conception as the date of birth – (gestational age in weeks) × 7 + 14 days. For each pregnancy, we defined the study period as 450 days prior to conception to the date of birth. A pre-conception period of 450 days was chosen as most women actively trying to conceive do so within 1 year (Joffe and Li, 1994). We excluded pregnancies among women who had a previous birth in the pre-conception period, as a pregnancy or birth during this time period may affect antipsychotic use. All eligible pregnancies were included in the study regardless of the mother’s parity. Thus, multiparous women may have one or more of their pregnancies included in the study, as long as they met the inclusion criteria described above.
Medicines priced below the co-payment threshold are not subsidised and were not captured prior to July 2012. As some medicines of interest were priced below the co-payment threshold for general beneficiaries, we restricted the analysis to women who were concessional beneficiaries to ensure complete capture of medicines dispensing. We defined concessional beneficiaries as women with only dispensings attracting a concessional subsidy, and who had at least one dispensing for any medicine, during the study period. Approximately 19% of people aged 16–44 years in NSW are concessional beneficiaries (Australian Government Department of Social Services, 2018) and are primarily people with a low income or chronic disability. In a survey of Australians with psychotic illness, 87% received a government pension as their primary income (Morgan et al., 2012).
After data were cleaned as described previously (Tran et al., 2017), there were 632,542 eligible pregnancies in NSW from 2005 to 2012. We excluded 82,776 pregnancies among women who had a birth in the 450 days before conception. Of the remaining 549,766 pregnancies, 137,993 (25.1%) were among concessional beneficiaries. While the unit of analysis is pregnancies, to simplify the text we will henceforth refer to distinct pregnancies as women. Compared with general beneficiary mothers, concessional beneficiaries were younger, less likely to be married, living in an area with a lower socioeconomic status and more likely to have smoked during pregnancy (Supplementary Table S1).
Measurement of antipsychotic utilisation
We identified all women where the estimated duration of use of an antipsychotic overlapped with the study period (the ‘exposed’ group). All other women were considered ‘unexposed’. We included all PBS-listed antipsychotics (World Health Organization [WHO] ATC code N05A) available during the study period, including: typical antipsychotics (chlorpromazine, flupentixol, fluphenazine, haloperidol, periciazine, thioridazine, trifluoperazine, zuclopenthixol) and atypical antipsychotics (amisulpride, aripiprazole, asenapine, clozapine, olanzapine, paliperidone, quetiapine, risperidone, ziprasidone) with the exclusion of lithium (N05AN01) and prochlorperazine, the latter of which is listed and used as an antiemetic (A04AD) in Australia. We analysed lithium separately as it has a different mechanism of action and is more commonly used as a mood stabiliser.
As prescribed daily dose was not available, we estimated the duration of each antipsychotic dispensing using the median time between dispensings by formulation; this was 30 days for oral formulations and 14 days for injections. We measured the daily dose using the defined daily dose (DDD) to allow comparison across medicines. We determined the total DDDs available in each 30-day interval during the study period and calculated the average daily DDD in each interval. If, after accounting for all complete 30-day intervals, 20–29 days remained until the end of pregnancy, we calculated the average daily DDD for this time interval. If <20 days remained, we merged data from this brief period with the prior 30-day interval and calculated the average daily DDD for the combined interval.
Maternal and baby characteristics
From the perinatal data, we obtained sociodemographic information (age, Index of Relative Socio-Economic Disadvantage [IRSD] of residential area) (Australian Bureau of Statistics, 2011), and pregnancy and birth characteristics (parity, timing of antenatal care, plural birth, birthweight, gestational age, admission to neonatal intensive care unit [NICU] or special care nursery). Marital status was defined using the hospital data. We defined smoking during pregnancy, Caesarean section, pre-existing diabetes, gestational diabetes, chronic hypertension and gestational hypertension using the perinatal data supplemented with the mother’s hospital records (coded with ICD-10-AM; see Supplementary Table S2) (Tran et al., 2014). The presence of diabetes was supplemented using dispensing of diabetes medicines, excluding metformin, which can be used to treat polycystic ovary syndrome. We identified perinatal death (stillbirth or death within 28 days of birth) from the perinatal data supplemented with the deaths registry data. Neonatal abstinence syndrome is a collection of symptoms that a baby may experience when withdrawing from in utero exposure to drugs of dependence, most commonly opiates (Hudak et al., 2012) and was identified using diagnostic information from the baby’s hospital birth record. We calculated whether the baby’s weight was small for gestational age (<10th percentile) or large for gestational age (>90th percentile) using published Australian birth weight percentiles (Dobbins et al., 2012).
When describing mental health characteristics, we searched for mental health or behavioural disorder diagnoses in all hospital admission diagnosis fields during the entire study period (ICD-10-AM codes F00-F99). In contrast, we defined a mental health hospitalisation as an admission with a principal diagnosis only of a mental health or behavioural disorder, or with any diagnosis of intentional self-harm (ICD-10-AM codes X60-X84). We also identified dispensing of other psychotropic medicines, including antidepressants (N06A), benzodiazepines (N05BA, N05CD) and mood stabilisers (carbamazepine, lamotrigine, valproate, lithium). A woman was considered to have used one of these three psychotropic types before or during pregnancy if she had two or more dispensings in at least two separate 90-day periods either in the pre-conception period or during pregnancy, respectively.
Statistical analysis
We used group-based trajectory models to classify patterns of antipsychotic use prior to and during pregnancy. The most appropriate number of trajectories was selected using the Bayesian Information Criterion and clinical judgement. We considered a model adequate if it had good correspondence between the estimated and observed membership probabilities, high average posterior membership probabilities and high odds of correct group classification (Nagin and Odgers, 2010). In the trajectory model, we also included a time-dependent variable representing pregnancy. Trajectories stopped at 9 months due to the small number of pregnancies with a completed gestational age ⩾10 months; for pregnancies shorter than 9 months, the final month(s) were set as missing. We compared the distribution of all mother and baby characteristics described above by trajectory of antipsychotic use, using the chi-square test for categorical variables, and the Wilcoxon rank-sum test for continuous variables; both were adjusted for correlation between pregnancies from the same mother.
All analyses were performed with SAS 9.4, Stata 14.2 and R 3.5.1.
Results
The final cohort comprised 137,993 women; of these, 2741 (2.0%) were exposed to antipsychotics prior to or during pregnancy; this doubled over the study period from 1.4% in 2005/2006 to 2.8% in 2011/2012.
Trajectories of antipsychotic use
We identified six trajectories of antipsychotic use (Figure 1). Women in the two most common trajectories (1 and 2) had short-term use of low daily doses: 26.6% (95% confidence interval [CI]: [24.5%, 28.6%]) with use commencing and ending well before pregnancy, and 24.5% (95% CI: [22.6%, 26.5%]) with use immediately preceding pregnancy. Women in three trajectories (3, 5, 6) had long-term use of antipsychotics prior to pregnancy that continued during pregnancy, with a low daily dose (20.9%, 95% CI: [19.2%, 22.7%]), moderate daily dose (11.0%, 95% CI: [9.6%, 12.4%]) or high daily dose (2.0%, 95% CI: [1.4%, 2.5%]). Finally, 15.0% of women had increased antipsychotic doses during pregnancy (trajectory 4; 95% CI: [13.4%, 16.6%]).
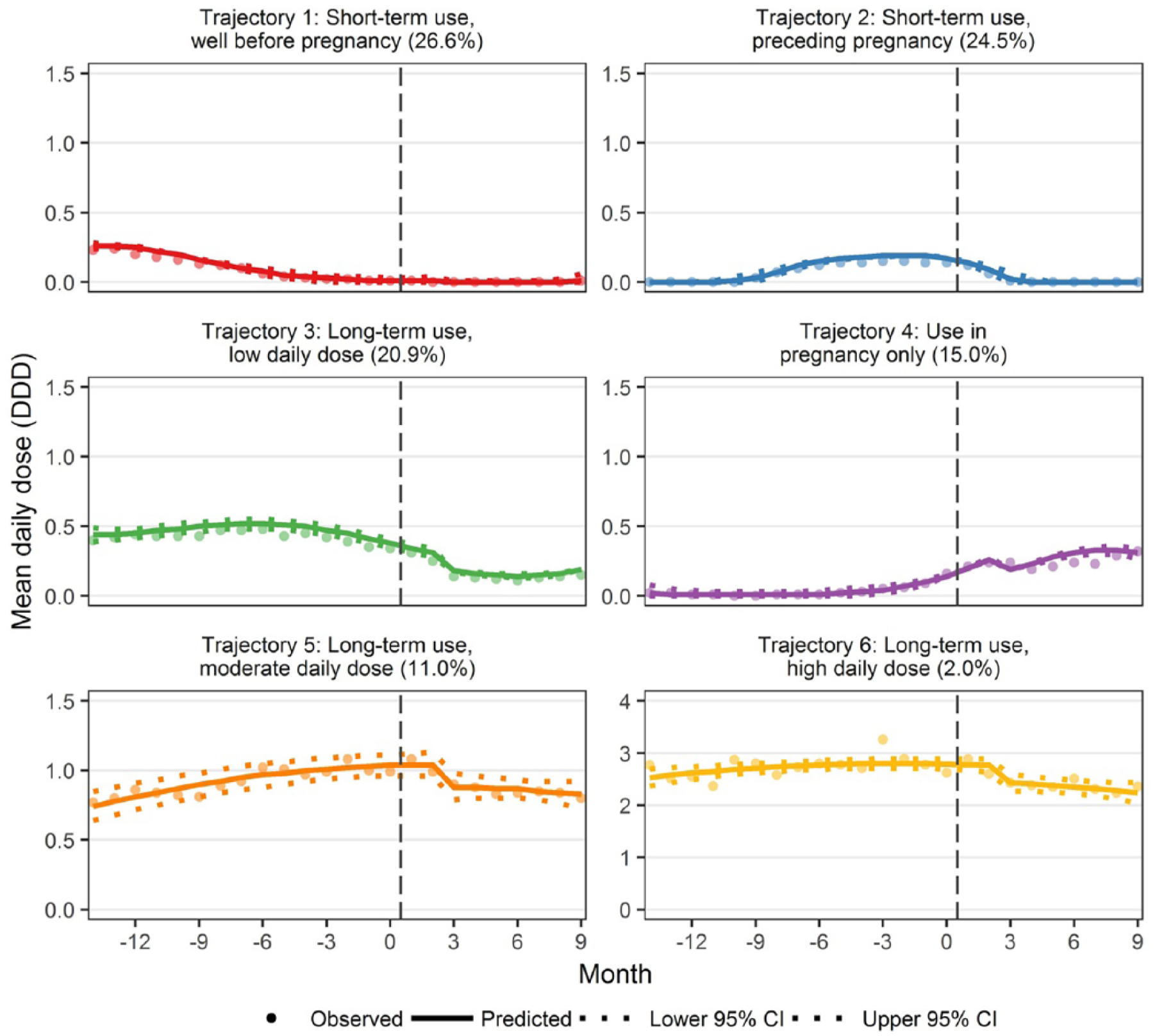
Antipsychotic use trajectories of mean defined daily dose by 30-day periods.
Overall, 86.8% and 23.2% of exposed women were dispensed atypical and typical antipsychotics, respectively; quetiapine and olanzapine were the most commonly dispensed (Table 1). Women with long-term use (trajectories 3, 5, 6) were more likely than women in other trajectories to be dispensed aripiprazole (ranging from 1.5% in trajectory 4 to 22.2% in trajectory 6), be dispensed multiple antipsychotics throughout the study period (from 10.5% in trajectory 2 to 57.4% in trajectory 6) and receive a depot injection (from 1.0% in trajectory 2 to 18.5% in trajectory 6). Women with increased antipsychotic use during pregnancy (trajectory 4) had the highest rate of haloperidol use (10.1%).
Treatment characteristics, mental health diagnoses and mental health hospitalisations by antipsychotic trajectory.
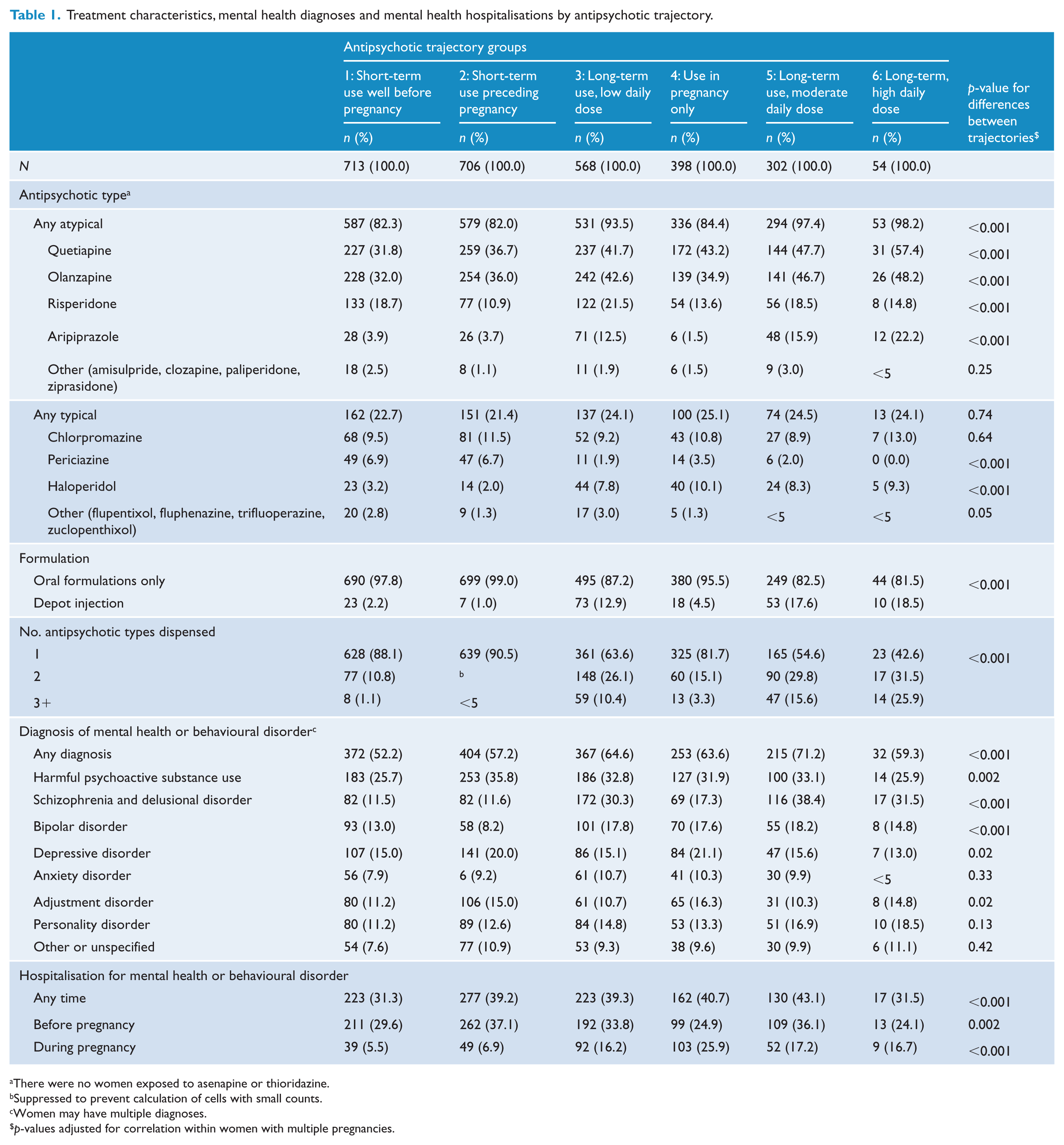
There were no women exposed to asenapine or thioridazine.
Suppressed to prevent calculation of cells with small counts.
Women may have multiple diagnoses.
p-values adjusted for correlation within women with multiple pregnancies.
Maternal characteristics
Compared with unexposed women, women exposed to antipsychotics were more likely to be single (from 46.3% to 55.2% vs 36.3%), smoke during pregnancy (57.7% to 69.4% vs 31.8%) and less likely to reside in the lowest socioeconomic quintile areas (19.7% to 24.1% vs 30.5%) (Table 2). Among exposed women, those with long-term use (trajectories 3, 5, 6) were older and more likely to be primiparous than women with short-term use.
Maternal sociodemographic and health characteristics by antipsychotic exposure and trajectory.
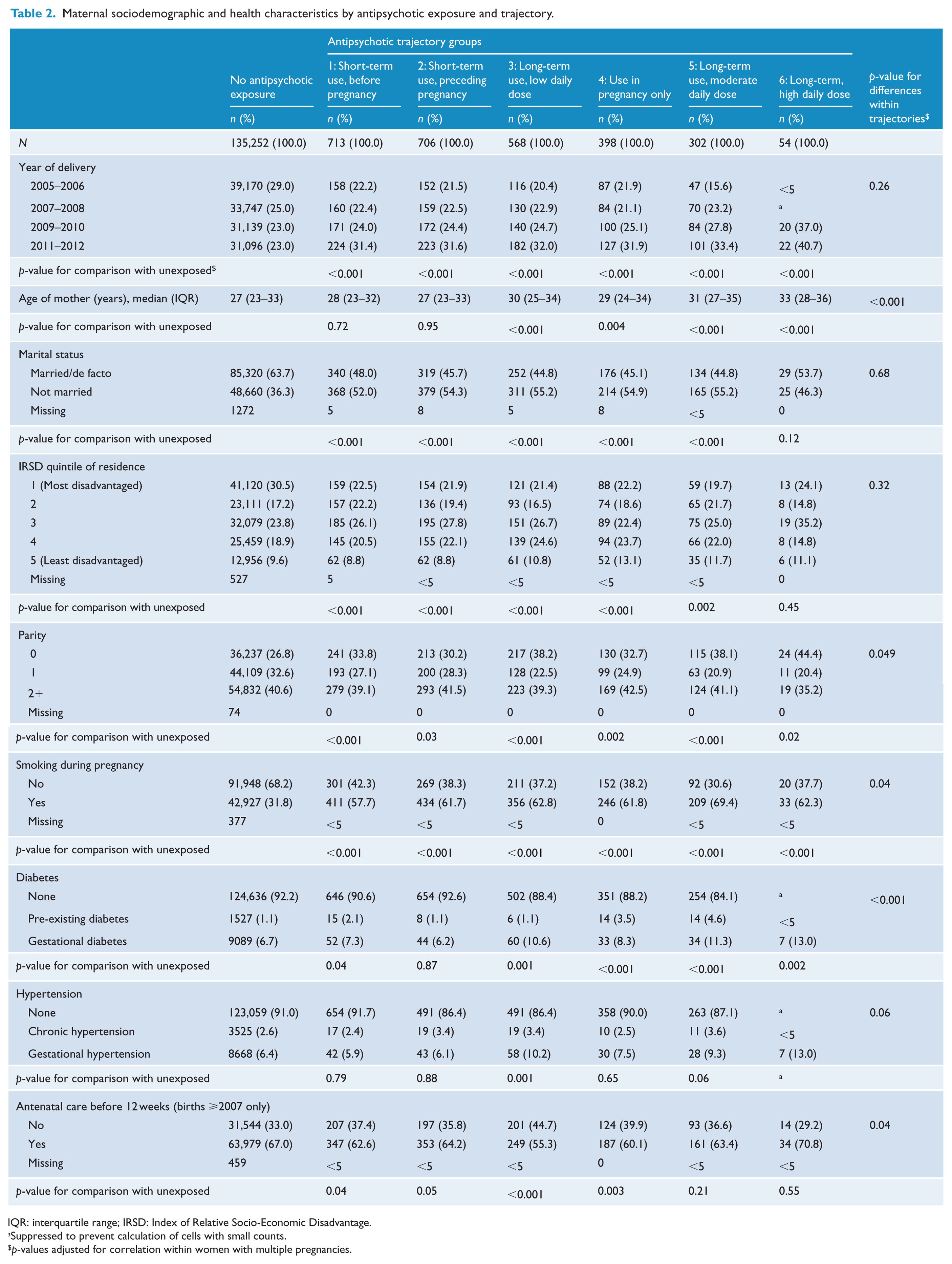
IQR: interquartile range; IRSD: Index of Relative Socio-Economic Disadvantage.
Suppressed to prevent calculation of cells with small counts.
p-values adjusted for correlation within women with multiple pregnancies.
A majority of women exposed to antipsychotics had at least one recorded diagnosis of a mental health disorder (from 52.2% to 71.2%), the most common being harmful substance use (25.9% to 35.8%), schizophrenia (11.5% to 38.4%), depressive disorder (13.0% to 21.1%) and bipolar disorder (8.2% to 18.2%) (Table 1). The most common reasons for a harmful substance use diagnosis were cannabis (57.8%), opioids (29.3%) and alcohol (27.1%). Schizophrenia or bipolar disorder diagnoses were most common among women with long-term antipsychotic use (trajectories 3, 5, 6), and least common in women with short-term use (trajectories 1, 2). Women with increased use during pregnancy (trajectory 4) had the highest rates of depressive disorder (21.1%) and adjustment disorder (16.3%). Among all exposed women, hospitalisation for a mental health disorder was common prior to pregnancy (ranging from 24.9% to 37.1%), but less so during pregnancy (5.5% to 25.9%); the highest rate of hospitalisation during pregnancy was in women with increased antipsychotic use during pregnancy (trajectory 4). Rates of hospitalisation for mental health disorders before and during pregnancy mimicked the observed antipsychotic use trajectories (Supplementary Figure S1).
Antidepressants were commonly dispensed to women across all trajectories (Figure 2), and women with short-term use of antipsychotics prior to pregnancy (trajectories 1 and 2) were most likely to discontinue their antidepressant medicines during pregnancy. Women with long-term use in moderate to high daily doses (trajectories 5 and 6) were most likely to continue. 10.8% of women with increased use of antipsychotics during pregnancy (trajectory 4) initiated antidepressants in pregnancy. While use of mood stabilisers was common in women with long-term antipsychotic use (trajectories 3, 5, 6), few continued their use in pregnancy.
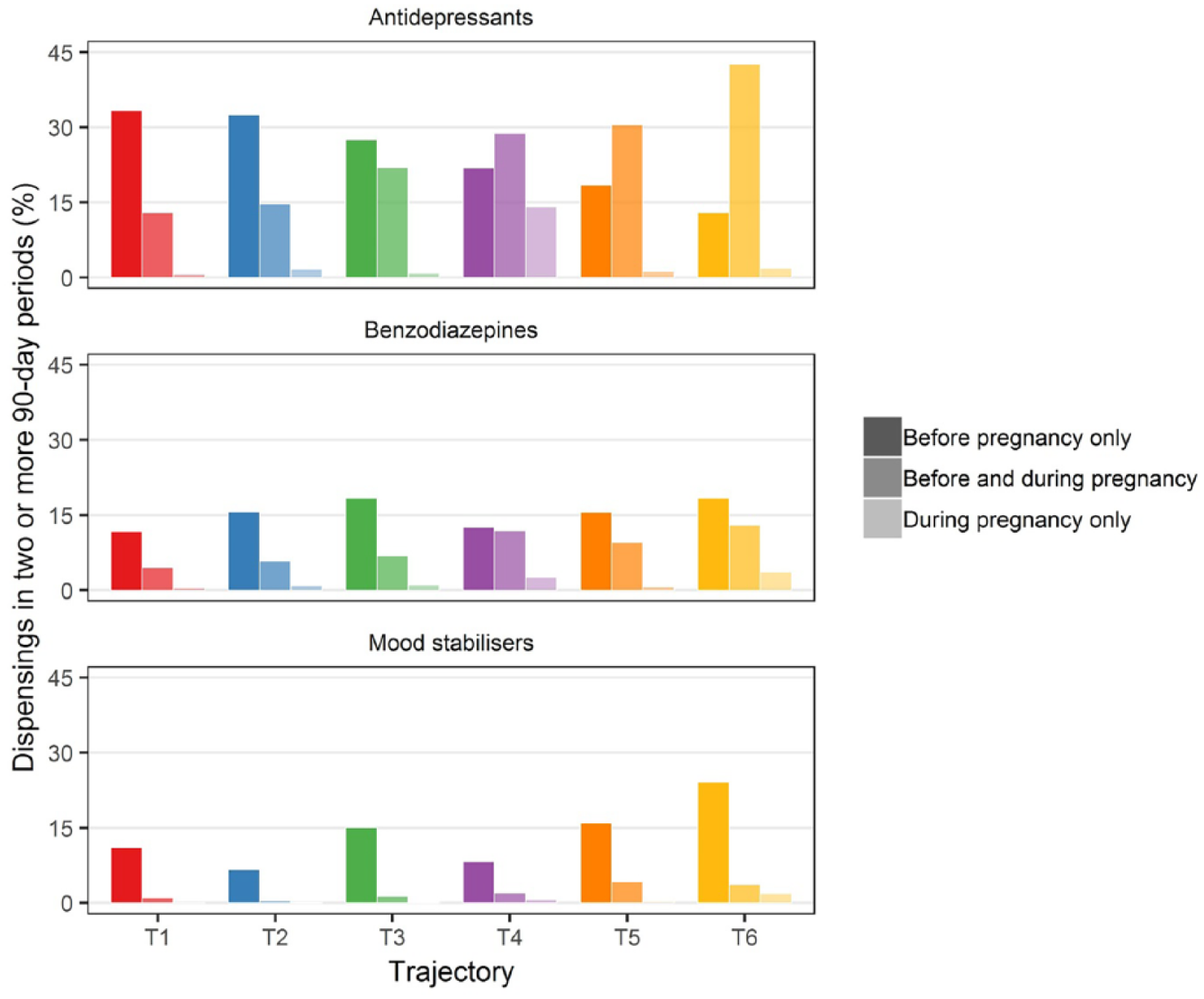
Dispensing of other psychotropic medicines in at least two 90-day periods by antipsychotic trajectory.
Pregnancy and birth outcomes
Among women exposed to antipsychotics, women with the highest daily dose (trajectory 6) had the highest rates of gestational diabetes (13.0%), gestational hypertension (13.0%) and a large baby for gestational age (16.7%). Among women in all other trajectories, a small baby for gestational age was more common (from 16.4% to 21.4%) than among unexposed women (12.6%). Compared with unexposed women, women in all trajectories were more likely to have a preterm birth (from 13.1% to 18.8% vs 7.9%), have a baby admitted to the NICU or special care nursery (29.3% to 44.4% vs 17.3%) and have a baby with a diagnosis of neonatal abstinence syndrome (6.4% to 12.2% vs 1.2%) (Table 3). Perinatal death was more common among babies born to women with increased antipsychotic use during pregnancy (trajectory 4) than babies of unexposed women (2.0% vs 1.0%).
Pregnancy and birth characteristics by antipsychotic exposure and trajectory.
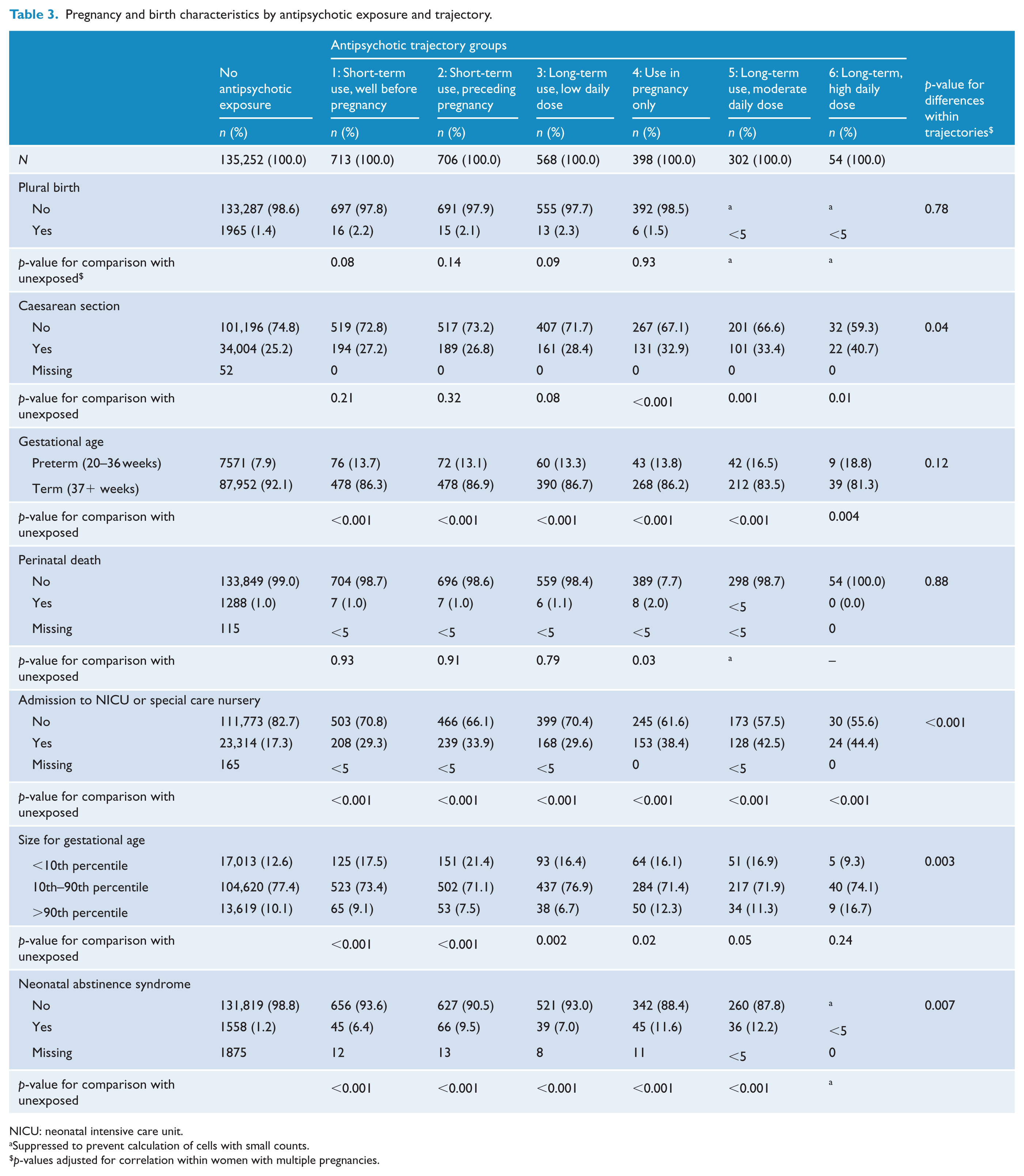
NICU: neonatal intensive care unit.
Suppressed to prevent calculation of cells with small counts.
p-values adjusted for correlation within women with multiple pregnancies.
Discussion
In our analysis of women exposed to antipsychotics prior to or during pregnancy, we identified substantial variation in maternal mental health characteristics, pregnancy complications and birth outcomes by treatment trajectory, likely reflecting differences in the underlying indication. Only a minority of women had a recorded diagnosis of schizophrenia or bipolar disorder, with diagnoses for conditions for which use of antipsychotics is considered off-label common, such as anxiety disorders, personality disorders and harmful substance use (Maher and Theodore, 2012). Similar to other studies, we found the two most common trajectories involved antipsychotic discontinuation prior to or in early pregnancy (Leong et al., 2017; Margulis et al., 2014; Park et al., 2017; Petersen et al., 2014). While treatment discontinuation carries the risk of relapse, women who discontinued were primarily using very low doses in the short term, with the lowest rates of schizophrenia and bipolar disorder, further suggesting off-label use. In contrast, one-third of women were using antipsychotics long-term and continued throughout pregnancy, with a small proportion using very high daily doses (>2 DDDs).
A UK study (Petersen et al., 2014) also found that continued use in pregnancy was more common in long-term users of higher doses; in our study, these women were more likely to have schizophrenia or bipolar disorder diagnosis and a high rate of mental health service utilisation, likely indicating more severe illness. This is a group at high risk of relapse in the antenatal and postnatal periods, which may justify use of antipsychotics through pregnancy. Only one in seven women in our study had increased doses of antipsychotics during pregnancy. Most medicines have increased or unchanged clearance during pregnancy (Ansari et al., 2016); while there are few data on antipsychotic kinetics in pregnancy, it is nonetheless surprising that we did not observe higher rates of dose increases, particularly among women who had been using antipsychotics long term. In addition, while we could not distinguish whether pregnancies were planned, unplanned pregnancy is associated with high stress and an increase in depressive episodes (Gariepy et al., 2016), consistent with our observation that this group had the highest rates of both depression and adjustment disorders.
We observed that women with long-term use of high daily doses had the highest rates of preterm birth, admission of the baby to the NICU and a baby with a diagnosis of neonatal abstinence syndrome, as well as gestational diabetes and gestational hypertension. While our study is purely descriptive and highlights associations only, long-term antipsychotic use increases the risk of obesity, metabolic syndrome and weight gain in pregnancy, all risk factors for gestational diabetes and other complications (Boden et al., 2012b; John et al., 2009; Mitchell et al., 2013). We also found that women exposed to antipsychotics had high rates of smoking and harmful substance use. Substance use disorders are common in people with psychotic illness (Moore et al., 2012) and other mental illness (Hunt et al., 2016; Lai et al., 2015), and antipsychotics are commonly misused in combination with illicit drugs (Malekshahi et al., 2015). The high rates we observed are troubling given the association between maternal use of alcohol, certain illicit drugs and adverse outcomes, such as poor neurodevelopment in children exposed to cannabis in utero (Jaques et al., 2014). Our findings also underscore the challenges in establishing a causal relationship between antipsychotic use and adverse birth outcomes, and future studies should give care to choosing an appropriate comparison group, and adequately accounting for all co-occurring risk factors, use of multiple antipsychotics and other medications, and underlying indications for treatment.
One limitation of our study is the restriction to concessional beneficiaries. The prevalence of antipsychotic use in our population (2.0%) was higher than reported in other studies (Engeland et al., 2018; Margulis et al., 2014; Petersen et al., 2014), which might be in part due to this restriction and the long pre-conception period. However, while only one-quarter of pregnant women are concessional beneficiaries, the vast majority of people living with psychosis receive government benefits and thus our population almost certainly represents the majority of pregnant women exposed to antipsychotics (Morgan et al., 2012). Furthermore, we may have underestimated some mental health diagnoses, as we relied on diagnoses recorded during hospital admissions only. While all women in our cohort were admitted to hospital at least once to give birth, some conditions for which off-label uses of antipsychotics is common, such as attention-deficit hyperactivity disorder, anxiety, sleep problems or autism may not be recorded if they did not impact on care received in hospital. Some conditions, such as harmful substance use, may also be more likely to be recorded than other mental health diagnoses as they may have more direct impact on care, particularly in pregnant women. Despite these limitations, our study has several strengths. We had access to rich data for all births in Australia’s most populous state. Moreover, most previous studies have used crude measures of antipsychotic use, such as defining antipsychotic use based on one dispensing only, and/or as a dichotomous variable. We took a big picture view of antipsychotic use over time, using trajectory models to capture patterns sometimes missed using single measures (such as persistence) (Hurault-Delarue et al., 2016).
In this study, we have identified six distinct trajectories of antipsychotic dosing and treatment durations around the time of pregnancy. Pregnant women treated with antipsychotics are heterogeneous, with varying mental health needs and complexity of treatment, reflecting the diversity of indications for antipsychotic use. Continuation of antipsychotics through pregnancy appears to be correlated with the underlying indication and severity of psychiatric illness. The use of antipsychotics through pregnancy is advised in women at high risk of relapse; however, this is also a group with high rates of pregnancy complications and poor birth outcomes. This diversity should be considered not only when developing clinical guidance about the use of antipsychotics in pregnancy but also when designing safety studies.
Supplemental Material
Supplementary_Files – Supplemental material for Trajectories of antipsychotic use before and during pregnancy and associated maternal and birth characteristics
Supplemental material, Supplementary_Files for Trajectories of antipsychotic use before and during pregnancy and associated maternal and birth characteristics by Andrea L Schaffer, Helga Zoega, Duong T Tran, Nicholas A Buckley, Sallie Pearson and Alys Havard in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the NSW Ministry of Health, the Australian Government Department of Health and Ageing, the Department of Human Services as well as data custodians of the NSW Perinatal Data Collection, the NSW Admitted Patient Data Collection, and the NSW Registry of Births, Deaths and Marriages. The authors also thank the Centre for Health Record Linkage (CHeReL) and the Australian Institute for Health and Welfare for conducting the linkage of records. A.L.S. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. A.L.S. conducted the analysis of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the Australian National Health and Medical Research Council (NHMRC) Centre of Research Excellence in Medicines and Ageing (#1060407); an Australian Government Department of Industry, Innovation and Science Cooperative Research Centre Project Grant (CRC-P-439); a NHMRC Project Grant (#1028543); a NHMRC Early Career Fellowship (#1158763 to A.L.S.); a National Heart Foundation of Australia Future Leader Fellowship (#100411 to A.H.); and a UNSW Scientia Fellowship (to H.Z.).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.