
Abstract
Objective
We examine whether the recent World Health Organization (WHO) report on global mental health uses severity of illness as a criterion in priority setting for resource allocation.
Conclusions
The WHO does not prioritise severity in the recent landmark World Mental Health Report. It recommends instead the insuperable task of scaling-up interventions for broadly defined mental health conditions, including milder distress, amongst over a billion people, with the majority living in low- and middle-income countries. Schizophrenia, the most severe and disabling of all psychiatric illnesses, is relatively neglected in the WHO report, and the disability associated with bipolar disorder is underestimated. This is inconsistent with the ethical principle of vertical equity, where the most severe illnesses should receive the greatest priority. The global mental health movement must refocus on deinstitutionalisation, and ensure adequate community and general hospital treatment for severe illnesses, especially the 24 million people with schizophrenia.
Alice laughed. “…one can’t believe impossible things.” “I daresay you haven’t had much practice,” said the Queen. “When I was your age, I always did it for half-an-hour a day. Why sometimes I believed as many as six impossible things before breakfast!”
Lewis Carroll
WHO Global Health Estimates 2019 – lay descriptions and disability weights
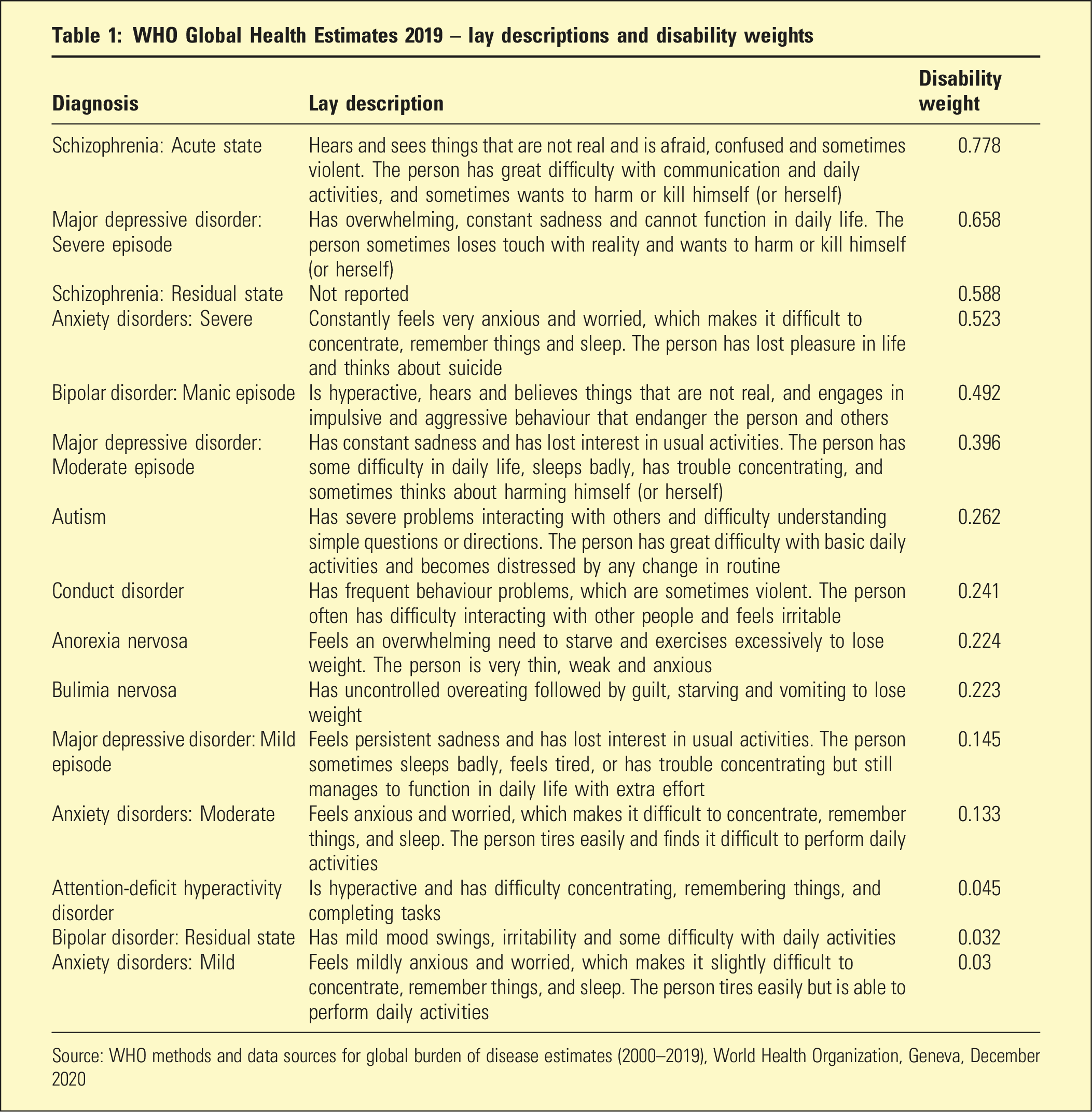
Source: WHO methods and data sources for global burden of disease estimates (2000–2019), World Health Organization, Geneva, December 2020
However, there has been a shift away from severe psychiatric illness in recent reviews of, and enquiries into Australian psychiatric care. 2 Their reports have focused instead on ‘broader, looser, and more benign’ conditions. 2 This shift in policy has been accompanied by real increases in Australian Government spending on primary care initiatives for mild-to-moderate conditions over the past decade, while spending on state and territory mental health services for the most severe illnesses has remained largely static.
A trend towards broadening the definition of mental health, and focusing on the less severe end of the spectrum might not be isolated to Australia. To assess whether it is actually a global phenomenon, we examine whether the landmark World Mental Health Report developed by the World Health Organization (hereinafter the WHO report), demonstrates a similar trend towards broader, looser and milder conditions while de-emphasising severe illnesses. 3 If so, this might increase vertical inequity in global mental health care, when people with greater needs are not be provided with more resources.
The vital few with the greatest needs
The WHO report recommends scaling-up interventions for over a billion people with broadly defined mental health conditions, most of whom live in low- and middle-income countries (LMICs). As the report explains: “To speak to the broadest group of stakeholders possible, this report generally uses the umbrella term “mental health conditions”, which covers mental disorders, psychosocial disabilities and other mental states associated with significant distress, impairment in functioning, or risk of self-harm” (p. 36).
3
Pre-pandemic in 2019, the Global Burden of Disease Study estimated that 970 million people had an International Classification of Diseases 11th Revision (ICD-11) mental health disorder, 82% of whom live in LMICs. 3 This was around 13% of the total global population. The addition of ‘other mental states associated with significant distress’ broadens the definition of mental health conditions beyond ICD-11 disorders in the WHO report, and lowers the threshold to include a larger proportion of the global population who are distressed, possibly due to social disadvantage or life stressors. Depression and anxiety are also used as umbrella terms in the WHO report to include depressive and anxiety symptoms, so the population with these conditions is greater than those with more strictly defined ICD-11 diagnoses.
The potential benefits of scaling-up mental health interventions for over a billion people worldwide remain uncertain. Rising treatment rates have not reduced the prevalence of mental health disorders, nor lowered the associated burden of disease in high-income countries (HICs) over recent decades. 3 ICD-11 mental health disorders remain considerably more prevalent (15.1%) in HICs than LMICs (11.6%). 3 There might be cultural, demographic, or methodological reasons for the disparity. However, these data do not support the effectiveness of scaling-up interventions in reducing the population burden of disease.
Concurrent with scaling-up interventions for more than a billion people, the WHO report calls for global deinstitutionalisation with the safe closure of all mental hospitals, and transfer of care to community teams, backed up by general hospital acute units. While Europe has the most mental hospital beds per capita, this reform has larger implications for LMICs, which rely to a greater extent on mental hospitals. 3 Mental health budgets in LMICs would need to approximately double during deinstitutionalisation because community teams and general hospital acute units must be developed before mental hospitals can be safely and gradually closed. 3
Despite the immense task of global deinstitutionalisation, the WHO report minimises discussion of severe psychiatric illnesses. The WHO report does not use the term ‘psychiatric illness’, and ‘mental illness’ is only mentioned in patient narratives and the reference list, as shown in the count of key terms in Figure 1. Specific diagnoses like schizophrenia, and bipolar disorder also have relatively few mentions in the WHO report. Log scaled count of key terms in the world mental health report. Source: World mental health report: transforming mental health for all. Geneva: World Health Organization; 2022.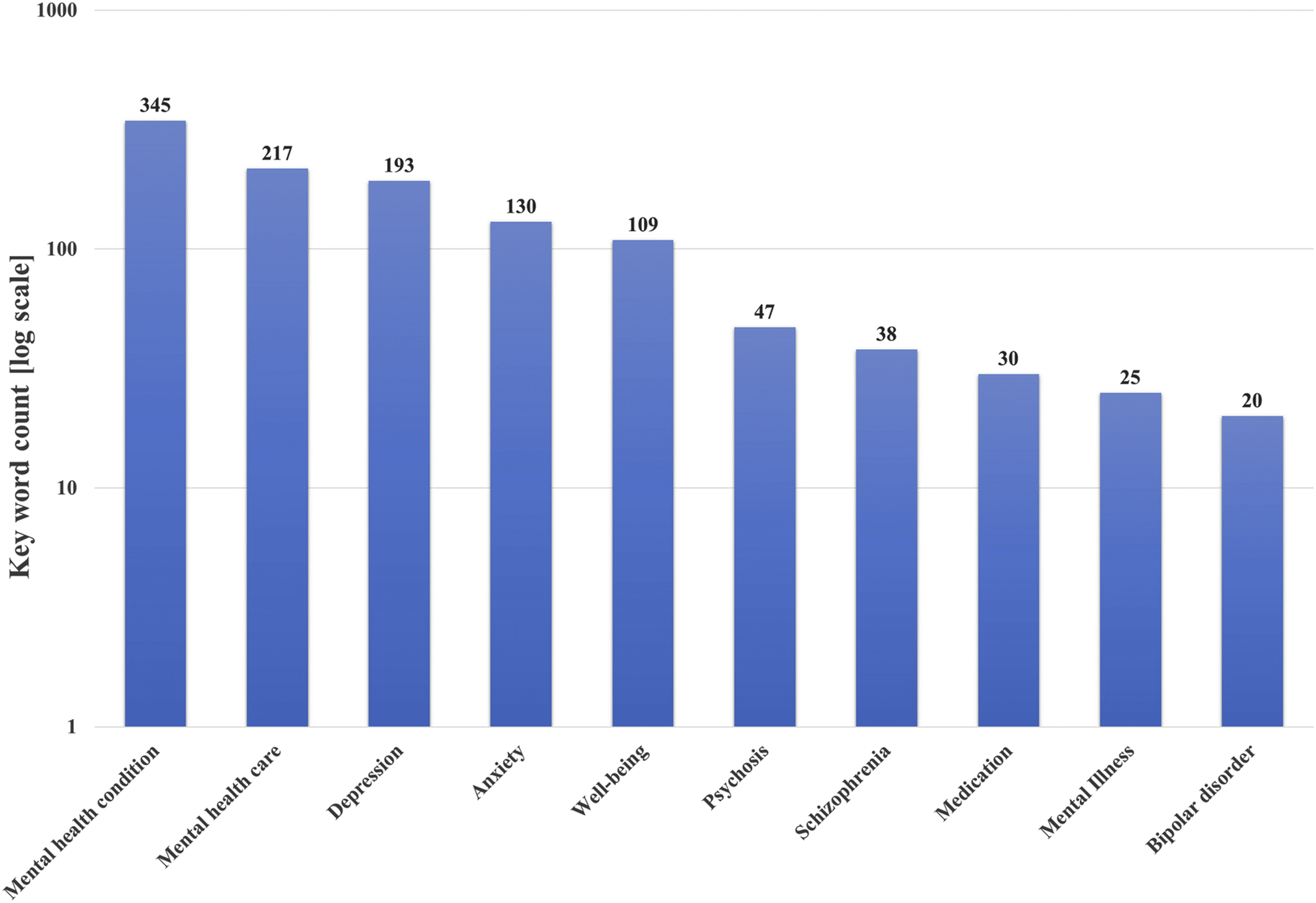
There are few references to medication, despite the poor availability and high cost of psychotropic medications for severe psychiatric illness in LMICs. 3 While most LMICs (60%) have lithium carbonate on essential medicine lists, clozapine is an essential medicine in only 25–29% of LMICs. 4 Poor access to psychiatrists and laboratory services probably limit use of these essential medicines in LMICs.
Instead of highlighting these crucial issues, the WHO report focuses more attention on care and wellbeing interventions for loosely defined, high prevalence mental health conditions (Figure 1). Thus, the report valorises ‘the many’ with less severe conditions (more than a billion people) over ‘the few’ with the most disabling illnesses especially schizophrenia (around 24 million people), 3 thereby breaching the ethical principle of vertical equity. 1 Adopting this broad definition of mental health conditions would be counterproductive for LMICs because their government services need a resolute focus on severe illnesses, particularly schizophrenia.
Prioritising severity in global mental health
A diagnosis of schizophrenia should be recognised as the driver of prioritisation in global mental health because of ‘the enormous health, economic and social hardships, including the significantly increased mortality rates and some of the worst instances of human rights abuse witnessed in modern times’. 5 At present, it is estimated that only 29% of people with psychosis receive adequate treatment. 3
An international policy focus on schizophrenia and other severe psychiatric illnesses is consistent with societal opinion. Large surveys conducted for Global Burden of Disease Study of households in Bangladesh, Indonesia, Peru, Tanzania and the USA rated acute schizophrenia as the most disabling illness amongst 220 unique health states with severe multiple sclerosis being the second most disabling illness. 6 The WHO Global Health Estimates 2019 also rated schizophrenia as the most disabling mental health condition. Table 1 shows the lay descriptions used to determine disability weights. Acute schizophrenia received a disability weighting of 0.778 on a scale from 1 (perfect health) to 0 (a state equivalent to death), so during an acute episode a person has only about a fifth of the level of the functioning of a fully healthy individual. Psychotic depression was rated as the second most disabling mental health condition (0.658). Clinicians might rate the disability associated with an acute manic episode relatively higher than the WHO Global Health Estimates (0.492).
In practical terms, LMIC must devote most of their mental health spending to the treatment of severe and disabling illnesses. Given the large treatment gap for severe illnesses in LMICs, a target of 80% cover has been proposed, which would require major increases in government spending. 7 It has also been suggested that an additional 10% of LMIC total mental health spending should be allocated to higher prevalence conditions, 7 although this might prove impossible for LMIC governments during the costliest phases of deinstitutionalisation for severe illnesses.
If funding becomes available for higher prevalence conditions, people in LMICs might prefer direct help with the basic necessities of life first – food, public safety, fresh water, electricity and family income. 8 As a respondent in rural India reported: ‘What else can a poor man have except tension [stress]? […] Money is the issue. We have no money in our home. If I had money then all of my tension would be ended (p. 555)’. 8 In an example of an intervention addressing the social determinants of a mental health condition, a young woman who was living in a slum in Mussoorie, North India responded to an innovative program that arranged for her to raise and sell chickens, which gave her purpose and a family income. 8
Conclusions
There has been a recent policy trend in Australia to de-emphasise severe psychiatric illnesses, in favour of broader, looser and milder conditions. 2 This trend appears to be global. The WHO report also highlights population distress rather than prioritising severe illnesses, concluding that more than one in eight people living in LMICs need a mental health intervention. 3 Instead of pursuing this policy, which is yet to show benefits in HICs, the WHO should emphasise the human rights of people with severe psychiatric illnesses, and advocate that those most in need have their care prioritised. The limited resources of LMICs should be directed toward the huge financial and logistic challenges of deinstitutionalisation with the creation of comprehensive care in the community, backed up with adequate numbers of general hospital acute inpatient beds, before safely phasing out mental hospitals. The WHO and HICs should not advocate for impossible targets for milder mental health conditions in LMICs. Treatment for severe illnesses must be the first and principal global priority to achieve vertical equity.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.