
Abstract
The Alexander Technique (AT) is a somatic method often employed by musicians, including pianists, which teaches its students to become consciously aware of their own postural behavior while carrying out various tasks. Little research has been conducted as to whether, and if so, how the AT affects the posture of pianists while they are playing the piano, and quantitative measurements of their postural angles have not yet been taken. The purpose of this study was to determine the effects of an intervention consisting of 10 AT lessons on pianists’ postural angles while playing, and to find out if the effects were still evident 4 weeks later. The following postural angles were measured before and after the intervention: craniovertebral angle, head tilt, head–neck–trunk angle, trunk angle, thoracic angle, thoracolumbar angle, and lumbar angle. There were significant effects of the intervention such that the craniovertebral and head–neck–trunk angles were found to have increased, and trunk, thoracic, and thoracolumbar angles were found to have decreased both immediately post-intervention and 4 weeks later. The AT appears to be a viable method of altering postural behavior while playing the piano, as seen in an overall pattern of spinal extension.
The Alexander Technique (AT) is a somatic method that is often used by musicians as it is thought to enhance performance by “improving ease and freedom of movement, balance, support, flexibility, and coordination” (Conable & Conable, 1995, p. 1). This is achieved by teaching students of the AT to recognize and alter counterproductive postural behavior (Cacciatore, Gurfinkel, Horak, Cordo, & Ames 2011; Cacciatore et al., 2020; Macdonald, 2015). Students learn to evaluate whether behavior is beneficial for completing tasks and to change that behavior if necessary. The postures and movements of musicians can affect the sounds they make (Klein et al., 2014; Shoebridge et al., 2017). The AT can help change their usual postures, which, in turn, could improve their music making. In AT terminology, the word use describes changes in posture over time throughout tasks, albeit in a very narrow sense as the AT deals not only with the body, but also with the mind (Barlow, 1990; Jones, 1997). The definition of use has been narrowed for the purposes of this article. Behavior that “[distorts] . . . the muscular and bony framework” (Barlow, 2005, p. 46) is termed misuse, while behavior that involves “a coordinated and balanced distribution of muscle tension throughout the body” is termed good use (Valentine, 2004, p. 179). To change the use of the body, students are taught a set of verbal directions that bring their awareness and/or attention to the amount of tension in their body. This sequence of instructions also helps them to return to a balanced muscular state (Barlow, 1990). In conjunction with these directions, the Alexander teacher provides the physical sensation accompanying this sequence through touch
Although learning the AT may improve musical performance, it does not work directly on music-making skills. Instead, its focus is to teach students the principles of the AT and how to apply them practically in daily life. One of the core principles of the AT is the primary control. This is defined as the relationship between the head, neck, and trunk/spine (Alexander, 1946; Conable & Conable, 1995), and it is essential in determining the quality of movement, or how well the body functions (Jain et al., 2004). Pianists in particular focus a great deal on their upper extremities. However, from an AT perspective, the movement of these parts are a by-product of the behavior of the head, neck, and trunk (Bosanquet, 1987). According to Brandes and colleagues (2020), “it is not well understood [by piano teachers] that a collapsed spine may cause shoulder tension and thereby poor coordination in the hands and arms” (p. 17). Attention should primarily be given to learning the AT before applying it to piano performance.
To date, little specific research has been conducted on the AT and pianists concerning changes in posture. Some studies (e.g., Armstrong, 1975) have looked at the effects of the AT on anxiety while providing only a cursory glance at posture. Kaplan (1994) conducted an exploratory study of six pianists’ experiences of the AT. She conducted two to three in-depth interviews with each participant, each one lasting approximately 1.5–2hr. Having identified “major themes and patterns” (p. 32), she found that pianists initially sought lessons in the AT because they experienced pain, discomfort, or excessive muscular tension while playing. Pianists also stated that the AT “[allowed] for continuous improvement and change” (p. 178) in their posture through the application of AT principles and was a helpful tool in identifying and changing habits in various activities, as well as in releasing excessive muscular tension.
Santiago (2004) examined the extent to which the AT helped young piano students improve their performance, specifically in relation to musical quality (e.g., tone) and posture. Twenty students between the ages of 10 and 14 participated and were randomly assigned to the control or experimental group. The experimental group received 8 weeks of 15–20-min lessons in the AT, while the control group attended sessions about mythology. Video recordings taken after the intervention period were assessed by the piano teachers who taught the students in the study, piano teachers who did not teach the students, three doctors, and four AT teachers. The results of these evaluations revealed that the AT appeared to be able to influence posture and tension although the tone quality of both groups had improved post-intervention.
Loo et al. (2015) investigated the effects of the AT on muscular tension in 15 undergraduate piano performance students, all of whom reported feeling excessive muscular tension prior to the beginning of the study. Participants used a 5-point Likert-type scale to rate the amount of tension they experienced in their fingers, hands, arms, wrists, shoulders, back, legs, and neck before and after receiving 14 weekly group lessons in the AT, each session lasting for 3 hr. During each session, participants received one-to-one instruction for 10 min, while the others observed. Post-intervention, participants reported a statistically significant reduction in muscular tension, suggesting that the AT has the potential to help relieve excessive tension in pianists.
Brandes et al. (2020) examined how the AT can be applied by a piano teacher in the context of teaching a lesson. This case study was conducted by video recording six piano lessons with a 7-year-old student who played at the skill level of Royal Conservatory of Music Level 2. Four piano teachers and AT teachers watched, coded, and commented on what they observed in the videos. The authors concluded that it is possible to integrate the AT into piano lessons by using it as a tool to observe and assess students as they play. However, the piano teacher who wishes to use the AT in their lessons must have had experience with it for AT concepts to be used during lessons.
Most research to date on the AT and pianists has mentioned posture only briefly and has not quantified differences before and after lessons in the AT using quasi-experimental or experimental methods. Rather, studies have utilized self-report rating scales (Loo et al., 2015) and qualitative methods (Brandes et al., 2020; Kaplan, 1994; Santiago, 2004). Muscular tension is a common theme in the papers reviewed, although in most cases it is not the main focus. However, from the perspective of the AT, tension is an outcome resulting from the use of the body, and use is affected by the primary control. This can be measured to a certain degree by examining spinal angles to determine the shape of the spine in various tasks. Very little research has been conducted concerning spinal angles while sitting or carrying out tasks while employing the AT. However, Cacciatore et al. (2005) conducted a detailed case study in which they followed a 49-year-old woman with low back pain through her experience with the AT. Lateral curvature in her trunk at the level of L3 was one of the variables that was examined during a quiet standing task. Before she started taking AT lessons she had a more leftward curvature, but when they measured the curvature after the lessons had ended they found that it had shifted toward the right, indicating a more symmetrical lumbar spine. In a subsequent study Cacciatore, Gurfinkel, Horak, and Day (2011) asked AT teachers and healthy adults who did not have training in the AT to carry out a sit-stand task (i.e., they were asked to stand from a sitting position) and examined the two groups’ patterns of spinal coordination. There was less movement in the cervical, thoracic, and lumbar spine of the AT teachers than the non-AT participants throughout the task.
Wong et al. (2022a) conducted a study to determine which angles were most likely to change and how they would change following AT lessons. Teachers and students training to be teachers of the AT performed a series of tasks twice, once while applying the principles of the AT and once while not applying them. The results suggested that the craniovertebral angle, head tilt, and head–neck–trunk angle could be expected to increase after a period of studying the AT while trunk, thoracic, and thoracolumbar angles could be expected to decrease, both sets of changes representing spinal extension. This study showed that it is possible to find out if the AT can be used to alter postural behavior by measuring changes in spinal angles, as such changes represent changes in posture. In general, most research on the AT and pianists is anecdotal. Little quantitative research has been reported, and objective measurements of change are lacking, as are studies of its lasting effects. Klein et al. (2014) have argued that research on the effects of the AT on musicians should be better designed. The purpose of the present study was therefore twofold, to determine (1) the potential effects of an intervention consisting of 10 AT lessons, such that there would be quantifiable changes, post-intervention, on pianists’ postural angles while playing and (2) whether these effects persisted 4 weeks later.
Method
Participants
A total of 15 pianists (12 female, 3 male) with a mean age of 35.33 ± 18.16 years volunteered to take part in the study. To ensure that they were all capable of playing at approximately the same skill level, they were all playing at Level 9 or higher as determined by the Royal Conservatory of Music, studying piano as their major instrument at a university, or had studied piano as their major instrument at a university. None had previously taken more than two one-to-one (private) AT lessons. Ethical approval was granted by the Research Ethics Board of the University of Ottawa. All participants gave their informed consent.
Design
This intervention study included a pre-test consisting of three baseline measurements, a post-test following participants’ final AT lesson, and a 4-week follow-up.
Apparatus
As shown in Figure 1, reflective markers were placed on the following anatomical locations: the tragus of the right ear, the spinous processes of C7, T5, T10, and L3, the sacrum, the left and right greater trochanters of the femur, and the posterior side of participants’ left and right forearms (i.e., palm facing down) approximately 7–10 centimeters above the wrist joint. A headband with four reflective markers was placed on their heads. Two markers at the front indicated the glabella and two markers at the back indicated the external occipital protuberance. After the markers had been attached, participants sat in front of a digital piano (Yamaha Digital Piano P-255) on an adjustable-height bench. They were permitted to change the height of the bench as well as the distance from the keyboard. The position data of each reflective marker was recorded using a 7-camera VICON Nexus motion capture system (Oxford Metrics) at 100 Hz. Video recordings were also taken in case there were anomalies in the data that would need to be explained.
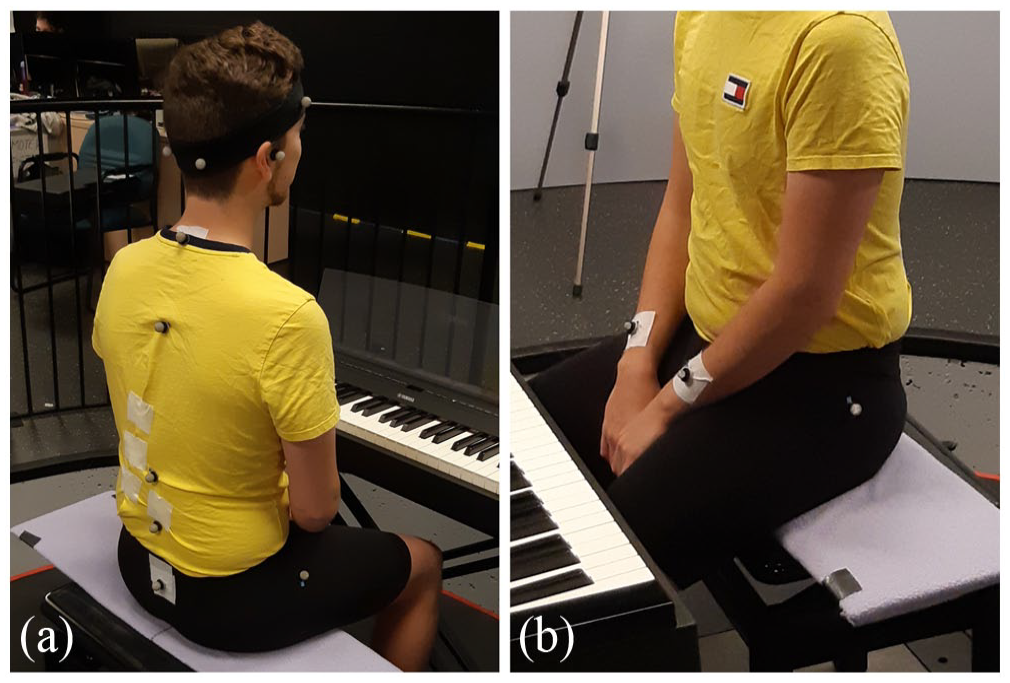
(a) Marker placement on head, spinous processes, and trochanter. (b) Marker placement on forearms and trochanter.
Procedure
Before taking part in the first of three baseline measurement sessions and the intervention itself, participants completed a questionnaire gathering demographic information (i.e., age, sex), playing history (i.e., number of years playing piano, highest level of playing achieved, post-secondary education, number of hours of practice per day, number of days of practice per week), and any previous experience they may have had with the AT or any other somatic method (e.g., Feldenkrais Method, Body Mapping). They were instructed not to begin any new activity (e.g., yoga) other than the AT for the duration of the intervention and not to continue AT lessons between the fourth measurement session, which took place within a week of the participant’s last AT lesson, and the fifth measurement session, which took place 4 weeks later.
In the first baseline measurement session, participants performed five tasks, described below, in a randomized order. The same procedure was followed in the second baseline measurement session 1 hr later, and the third session 1 week after the second session.
After the baseline measurements had been taken, all participants received 10 private AT lessons over the course of a 2-week period from eight teachers certified by the Canadian Society of Teachers of the Alexander Technique or the Society of Teachers of the Alexander Technique. Each participant was assigned to one teacher who taught them for the duration of the intervention, the number of lessons and their spacing having been discussed with and recommended by the director of the local school of AT. The post-intervention and 4-week follow-up measurement sessions followed the same procedure used in the baseline measurement sessions.
Tasks and data collection
Participants completed the following tasks: quiet-sitting, raising-hands, scale-playing, sight-reading, and playing in three different conditions (i.e., deadpan, projected, and exaggerated).
Participants’ typical sitting postures were measured in the quiet-sitting task, whereby participants sat facing the keyboard while the researcher stood in front of them reviewing the protocol for the session. Participants were not told that measurements were being taken, so as to reduce the possibility that they might consciously or unconsciously alter their posture. Ten seconds of data taken from the middle to the end of the task were analyzed.
In the raising-hands task, participants lifted both hands simultaneously from their laps onto the keyboard in front of them where they were asked to leave their hands until told to return them to their laps. The data analyzed were taken from the point when the forearm markers began to rise from participants’ laps to when they had been returned.
In the scale-playing task, participants played an ascending and descending C major scale with both hands in 16th notes at a tempo of 104 bpm. They started from the lowest C on the keyboard and played to the highest C, pausing with their hands on the keyboard until told to play the descending portion of the scale. Again, they left their hands on the keyboard until asked to remove their hands. The data analyzed were taken from the beginning of the task (i.e., when the forearm markers began to move toward the right side of the keyboard) to the end (i.e., when the hands rested on the left side of the keyboard).
In the sight-reading task, participants played an excerpt from a musical score they had never seen before. All the participants played the same excerpt, but different excerpts were used in each session.
In the playing task, participants played the first 12 measures of the first movement of Muzio Clementi’s Sonatina in C Major, op. 36, no. 3. They had received the musical score before taking part in the first baseline measurement session so that they could familiarize themselves with it. To ensure that any changes in spinal angles were not the result of playing expressively (Thompson & Luck, 2011), participants were asked to play the excerpt three times in each session, in three expressive conditions: deadpan, projected, and with exaggerated musical expression. In the deadpan condition, participants were to play with little to no variation in expressive features (e.g., tempo, dynamics). In the projected condition, they were to play as they usually would for a colleague, a teacher, or in a performance. In the exaggerated condition, they were to exaggerate all expressive features. The data analyzed in both sight-reading and playing tasks were taken for the duration of the entire excerpt from the moment the pianists placed their hands onto the keyboard to the point where they began to move their hands back onto their laps, as indicated by the forearm markers.
Data collected
The following angles were calculated using the data showing the position of each marker recorded by the motion-capture cameras. Measurements were taken from the right side of the body in the sagittal plane: craniovertebral angle, formed by connecting the tragus and C7, relative to the horizontal; head tilt, formed by connecting the glabella and external occipital protuberance, relative to the horizontal; head–neck–trunk angle, formed by connecting the tragus, C7, and the greater trochanter of the right femur; trunk angle, formed by connecting C7, T10, and the greater trochanter of the right femur; thoracic angle, formed by connecting C7, T5, and T10; thoracolumbar angle, formed by connecting T5, T10, and L3; lumbar angle, formed by connecting T10, L3, and the sacrum. Kyphosis in the thoracic, thoracolumbar, and lumbar areas were indicated by positive angles, while lordosis was indicated by negative angles.
Data analysis
Data were exported into MATLAB to calculate the postural angles. The mean of each participant’s angles in each measurement session was calculated across time points in 100ths of a second. Values with a z-score greater than 1.96 or less than −1.96 were considered outliers and Winsorized. Expectation maximization was used to impute missing data points. As Wong et al. (2022b) had shown that it is possible to obtain an overview of a participant’s typical posture from the mean of multiple baseline measurements, the angles were averaged across the three sessions to provide a single pre-intervention score. Repeated-measures analyses of variance (ANOVAs) were conducted using SPSS (v. 27) to explore the effects of AT lessons by comparing measurements taken at baseline, post-intervention, and follow-up. A Huynh–Feldt correction was applied if sphericity was violated and a value of p ⩽ .05 was considered statistically significant. Holm–Bonferroni corrections were applied to the results of all post hoc tests, assuming three analyses.
Results
The results of the repeated-measures ANOVAs and the comparisons of postural angles measured during the quiet-sitting task at baseline, post-test, and follow-up are presented in Table 1 (means and standard deviations refer to degrees). First, there was a significant main effect of AT lessons on the craniovertebral angle. Post hoc tests revealed that the angles were significantly larger at post-test than at baseline, while differences between the angles at post-test and follow-up, and at baseline and follow-up, were non-significant. Second, there was a significant main effect of AT lessons on the head–neck–trunk angle such that the angles were significantly larger at post-test and follow-up than baseline, while differences between the angles at post-test and follow-up were non-significant. Third, there was a significant main effect of AT lessons on the trunk angle although post hoc tests yielded no significant differences between the angles at baseline, post-test, and follow-up. Finally, there was a significant main effect of AT lessons on the thoracic angle such that the angles were significantly smaller at post-test than at baseline and follow-up, while differences between the angles at baseline and follow-up were non-significant. There were no significant effects of AT lessons on head tilt, thoracolumbar angle, or lumbar angle during the quiet-sitting task.
Postural angles during quiet-sitting task at baseline, post-test, and follow-up.
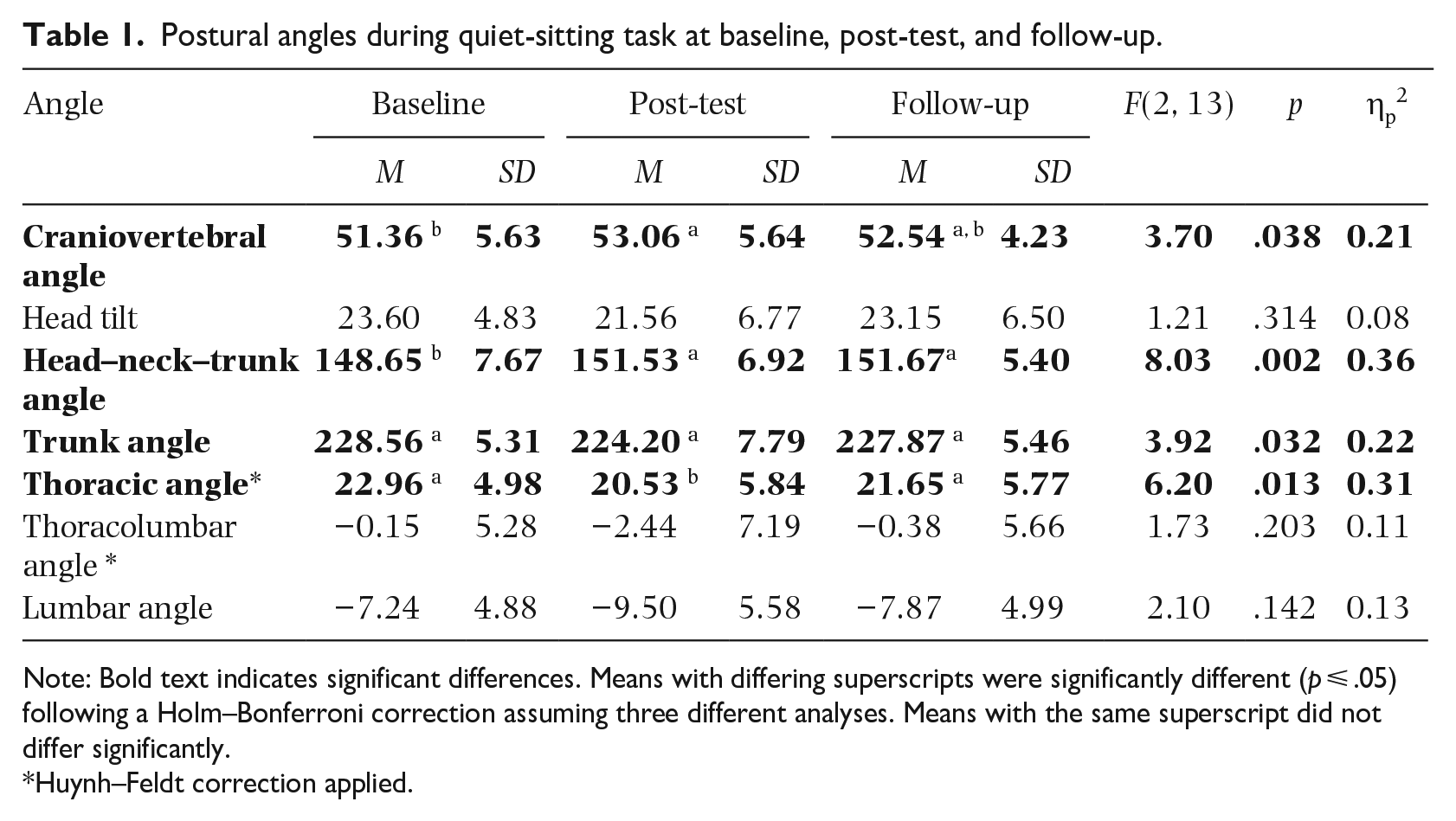
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ significantly.
Huynh–Feldt correction applied.
The results for the raising-hands task are shown in Table 2. First, there was a significant main effect of AT lessons on the head–neck–trunk angle. Post hoc tests yielded no significant differences between the angles at baseline, post-test, and follow-up. Second, there was a significant main effect of AT lessons on the trunk angle but no significant differences between the angles at baseline, post-test, and follow-up. Third, there was a significant main effect of AT lessons on the thoracic angle but no significant differences between the angles at baseline, post-test, and follow-up. There were no significant effects of AT lessons on the craniovertebral angle, head tilt, thoracolumbar angle, or lumbar angle during the raising-hands task.
Postural angles during raising-hands task at baseline, post-test, and follow-up.
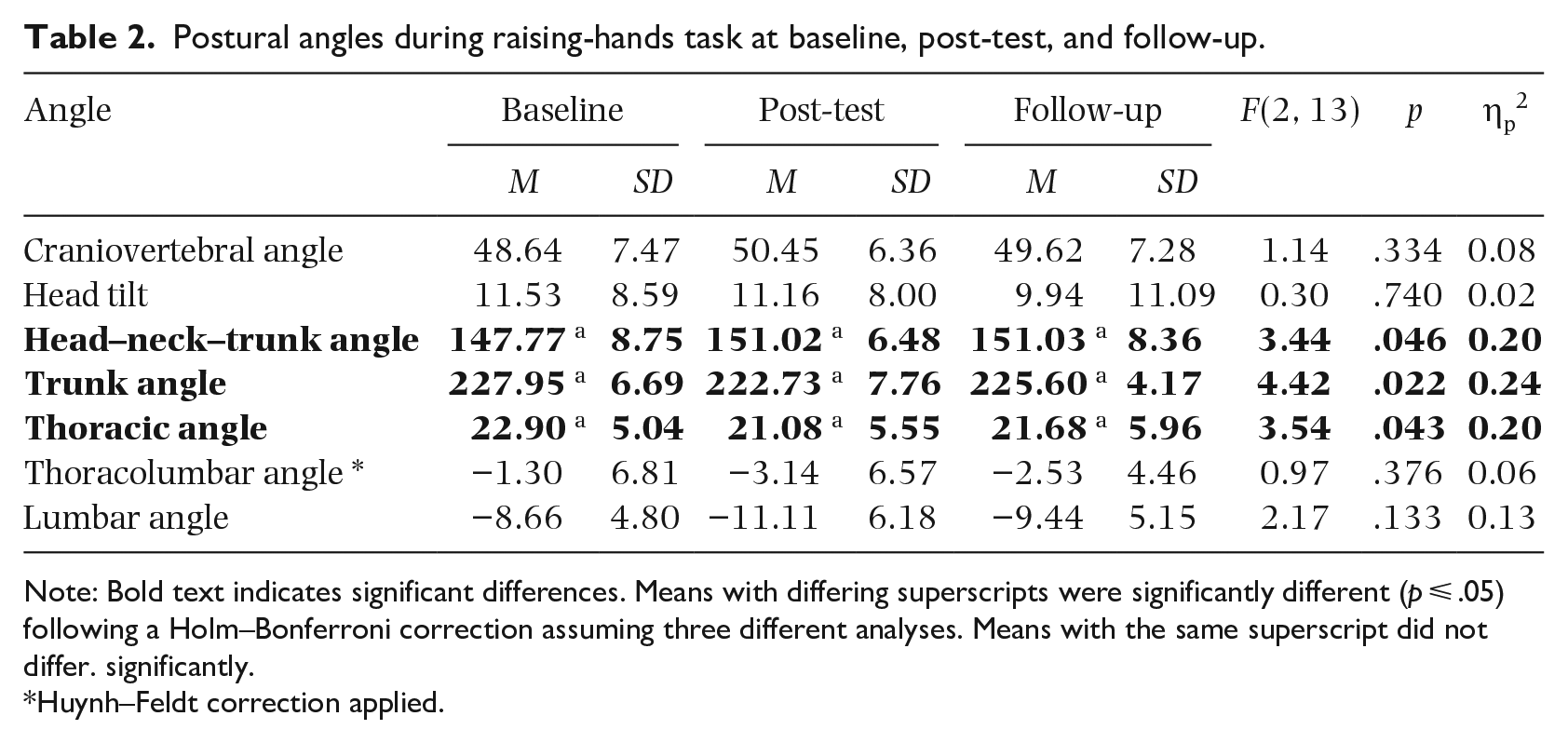
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ. significantly.
Huynh–Feldt correction applied.
There were significant main effects of AT lessons on all angles with the exception of the head tilt during the scale-playing task, as shown in Table 3. First, there was a significant main effect of AT lessons on the craniovertebral angle. Post hoc tests revealed that the craniovertebral angle was significantly larger at post-test than baseline, and at follow-up than baseline. Second, there was a significant main effect of AT lessons on the head–neck–trunk angle such that the head–neck–trunk angle was significantly larger at post-test than at baseline, and at follow-up than at baseline. Third, there was a significant main effect of AT lessons on the trunk angle such that the angle was significantly smaller at post-test than at baseline, and at follow-up than at baseline. Fourth, there was a significant main effect of AT lessons on the thoracic angle such that the angle was significantly smaller at post-test than at baseline, and at follow-up than at baseline. Fifth, there was a significant main effect of AT lessons on the thoracolumbar angle such that the angle was significantly smaller at post-test than at baseline, and at follow-up than at baseline. Sixth, there was a significant main effect of AT lessons on the lumbar angle such that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. For the scale-playing task, there were no significant differences between the post-test and follow-up for any of these six angles.
Postural angles during scale-playing task at baseline, post-test, and follow-up.
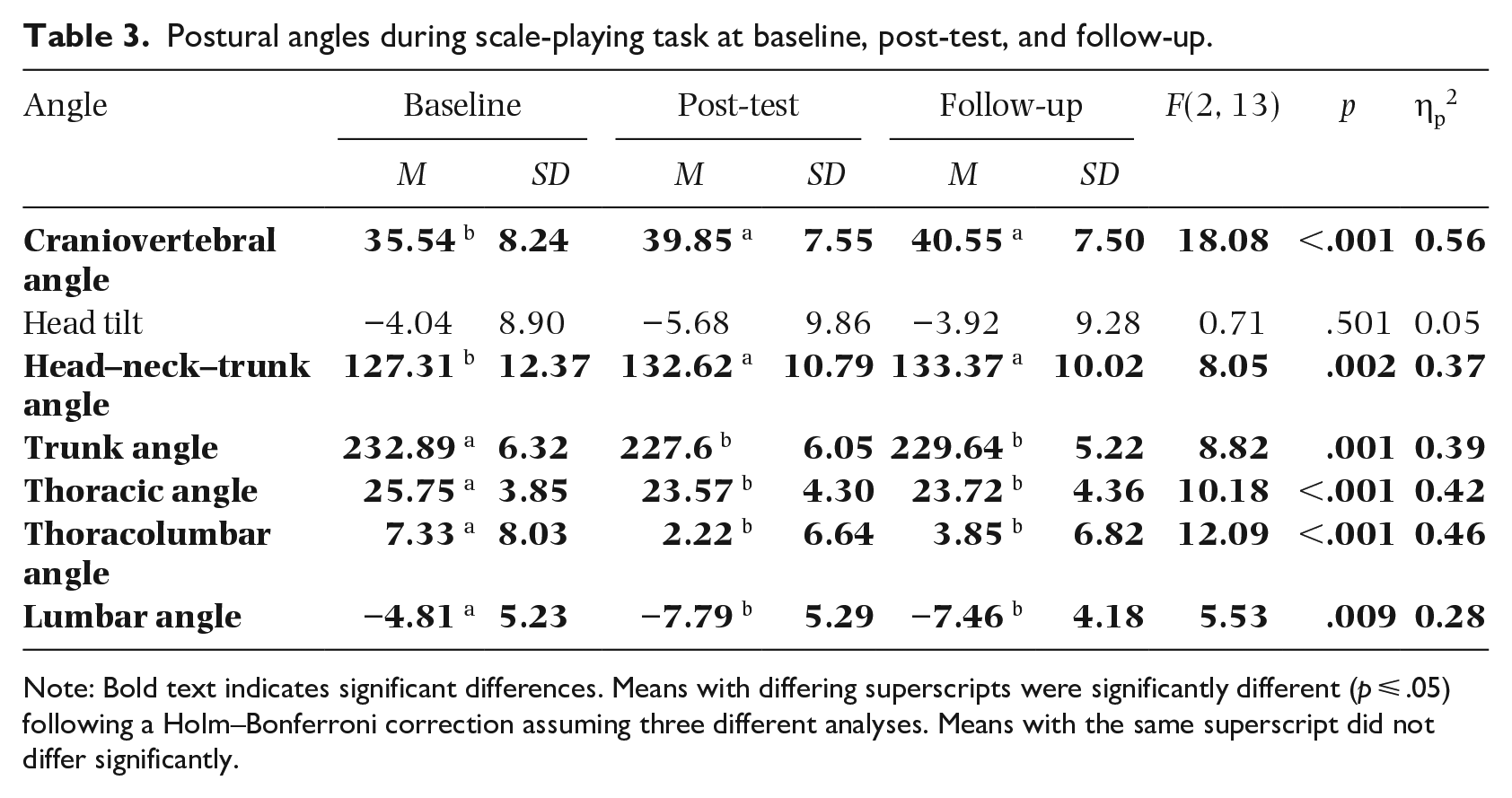
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ significantly.
There were significant differences between the three measurements of all angles except the thoracic angle during the sight-reading task, as shown in Table 4. First, there was a significant main effect of AT lessons on the craniovertebral angle. Post hoc tests revealed that the craniovertebral angles were significantly larger at follow-up than at post-test and baseline, and at post-test than at baseline. Second, there was a significant main effect of AT lessons on head tilt such that the angle was significantly larger at follow-up than at baseline. There were no significant differences between the angles at baseline and post-test or at post-test and follow-up. Third, there was a significant main effect of AT lessons on the head–neck–trunk angle such that the angles were significantly larger at post-test than at baseline, and at follow-up than at baseline. Fourth, there was a significant main effect of AT lessons on the trunk angle such that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. Fifth, there was a significant main effect of AT lessons on the thoracolumbar angle such that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. Sixth, there was a significant main effect of AT lessons on the lumbar angle such that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. For the sight-reading task, in addition to the results reported above, there were no significant differences between the head–neck–trunk, trunk, thoracolumbar, and lumbar angles measured at post-test and follow-up.
Postural angles during sight-reading task at baseline, post-test, and follow-up.
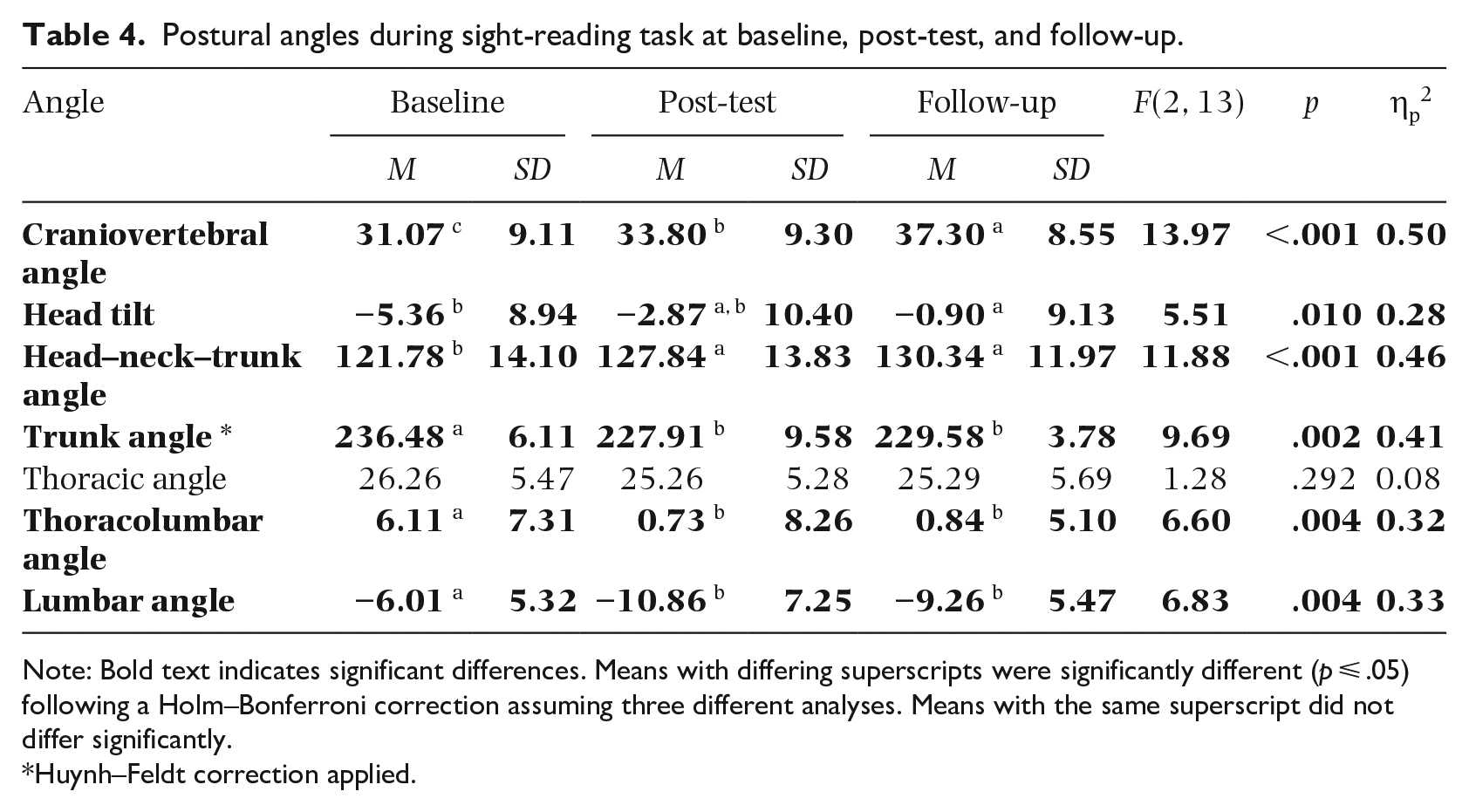
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ significantly.
Huynh–Feldt correction applied.
The results for the deadpan-playing task are presented in Table 5. First, there was a significant effect of AT lessons on the craniovertebral angle. Post hoc tests revealed that the angles were significantly larger at follow-up than at post-test and baseline, and at post-test than baseline. Second, there was a significant effect of AT lessons on the head–neck–trunk angle such that the angles were significantly larger at follow-up than at post-test and baseline, and at post-test than baseline. Third, there was a significant effect of AT lessons on the trunk angle such that the that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. There was no significant difference between the angles at post-test and follow-up. Fourth, there was a significant effect of AT lessons on the thoracolumbar angle but post hoc tests yielded no significant differences between the angles at baseline, post-test, or follow-up. Fifth, there was a significant effect of AT lessons on the lumbar angle but post hoc tests yielded no significant differences between the angles at baseline, post-test, or follow-up. For the deadpan-playing task there were no significant effects of AT lessons on head tilt and thoracic angle.
Postural angles during deadpan-playing task at baseline, post-test, and follow-up.
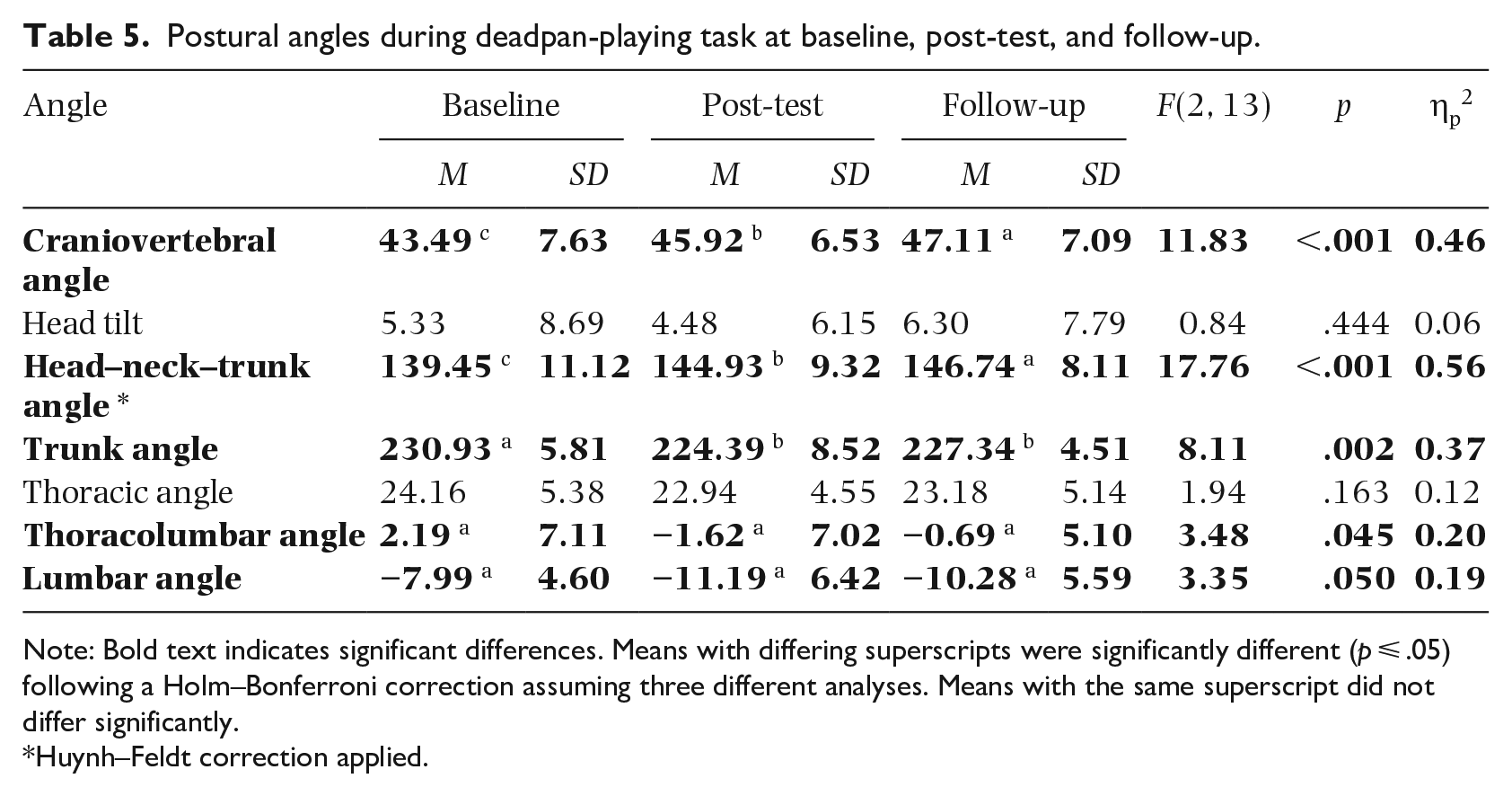
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ significantly.
Huynh–Feldt correction applied.
Results for the projected-playing task are shown in Table 6. First, there was a significant effect of AT lessons on the craniovertebral angle. Post hoc tests revealed that the angles at post-test were significantly larger than at baseline, and at follow-up than at baseline. Second, there was a significant effect of AT lessons on the head–neck–trunk angle such that the angles at post-test were significantly larger than at baseline, and at follow-up than at baseline. Third, there was a significant effect of AT lessons on the trunk angle such that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. Fourth, there was a significant effect of AT lessons on the thoracolumbar angle such that the angles were significantly smaller at post-test than at baseline, and at follow-up than at baseline. Fifth, there was a significant effect of AT lessons on the lumbar angle such that the angles at post-test were significantly smaller than at baseline, and at follow-up than at baseline. For the projected-playing task there were no significant effects of AT lessons on head tilt and thoracic angle, nor were there significant differences between any of the angles measured at post-test and follow-up.
Postural angles during projected-playing task at baseline, post-test, and follow-up.
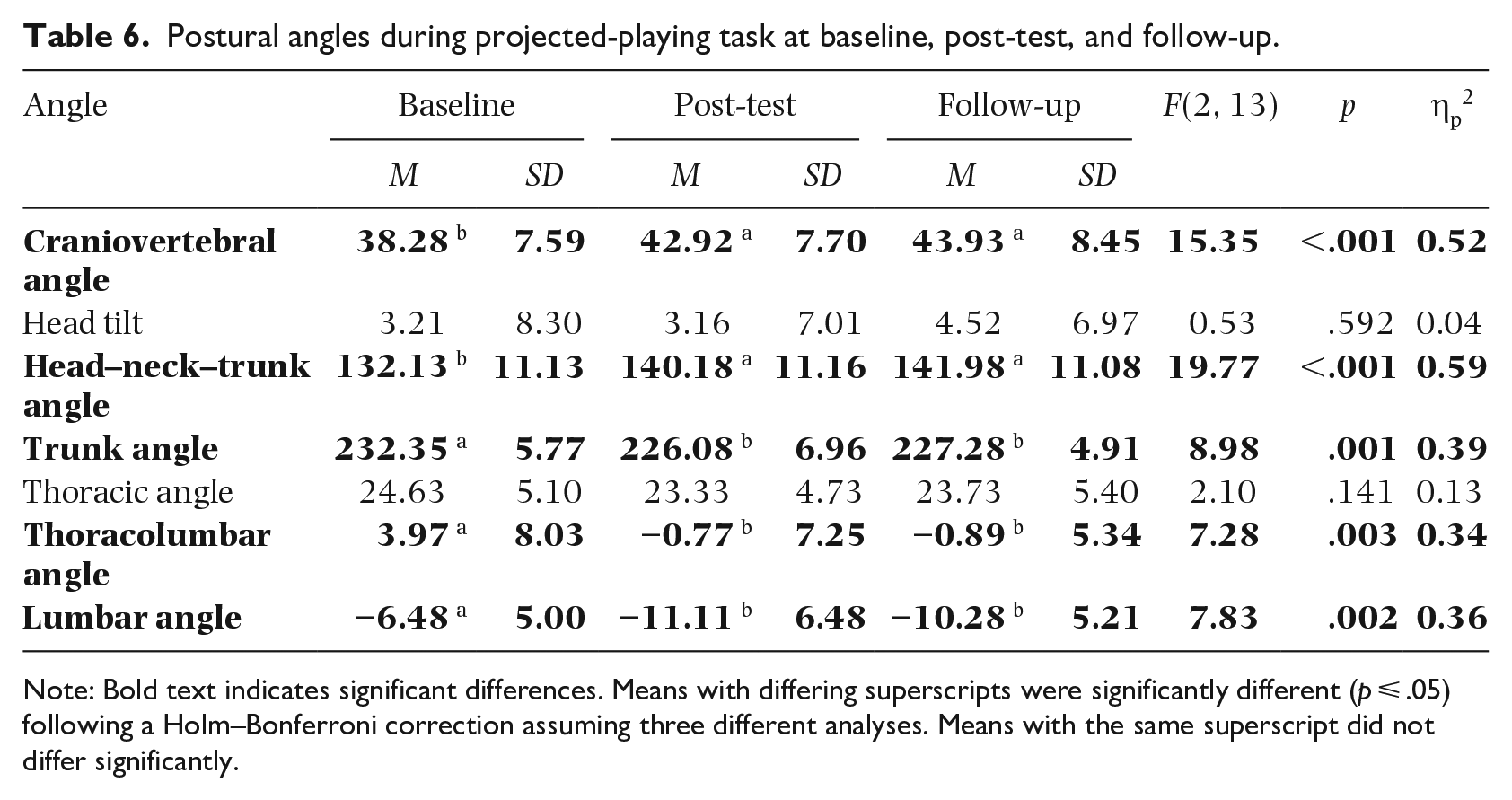
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ significantly.
Table 7 shows the results for the exaggerated-playing task. First, there was a significant effect of AT lessons on the craniovertebral angle. Post hoc tests revealed that the angles were significantly larger at post-test than at baseline, and at follow-up than at baseline. Second, there was a significant effect of AT lessons on the head–neck–trunk angle such that the angles were significantly larger at post-test than at baseline, and at follow-up than at baseline. Third, there was a significant effect of AT lessons on the trunk angle such that the angles at post-test were significantly smaller than at baseline, and at follow-up than at baseline. Fourth, there was a significant effect of AT lessons on the thoracolumbar angle such that the angles at post-test were significantly smaller than at baseline, and at follow-up than at baseline. Fifth, there was a significant effect of AT lessons on the lumbar angle such that the angle at follow-up was significantly smaller than at baseline, but there were no significant differences between angles at post-test and at baseline. For the exaggerated-playing task there were no significant effects of AT lessons on head tilt and thoracic angle, nor were there significant differences between any of the angles measured at post-test and follow-up.
Postural angles during exaggerated-playing task at baseline, post-test, and follow-up.
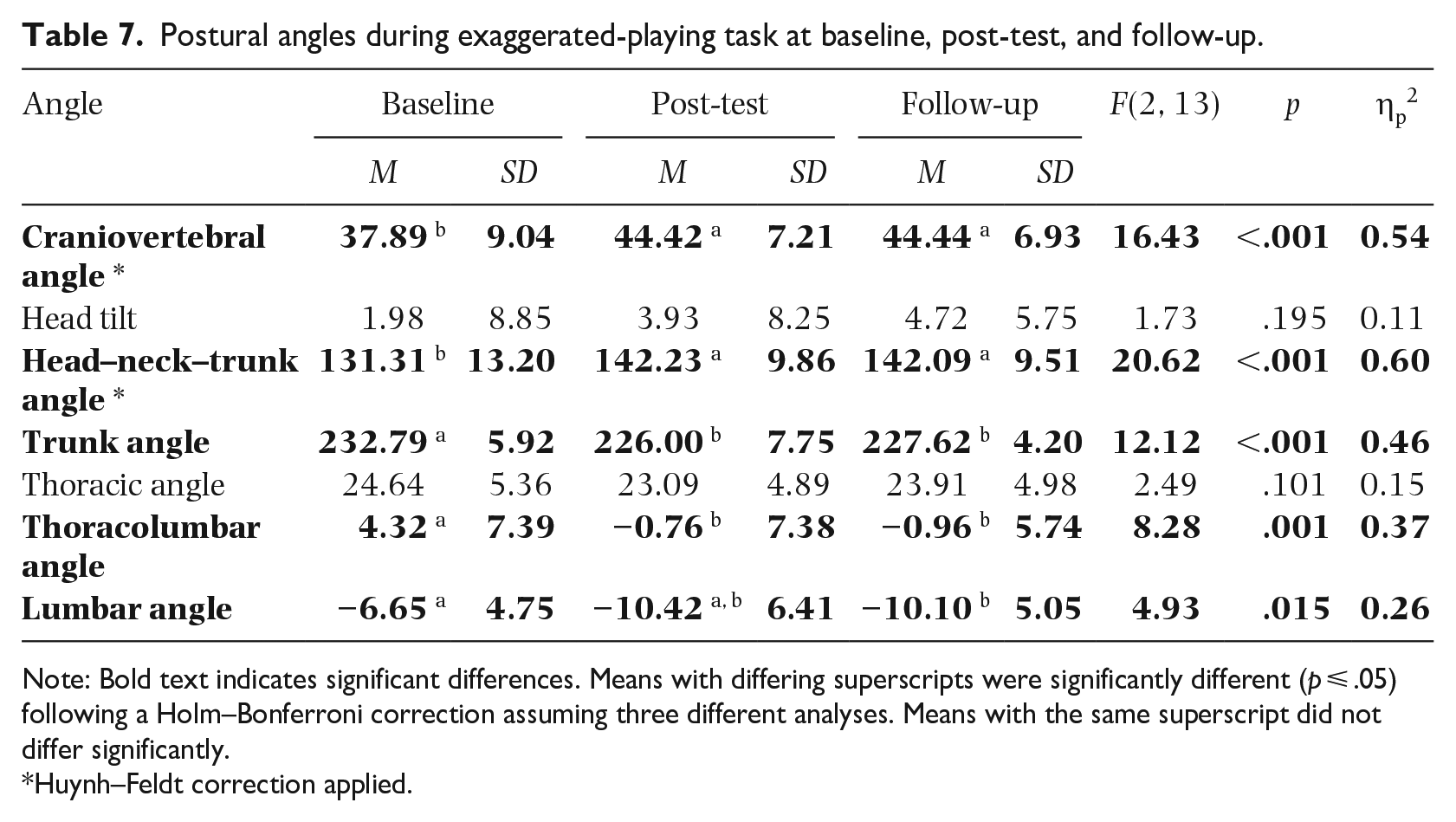
Note: Bold text indicates significant differences. Means with differing superscripts were significantly different (p ⩽ .05) following a Holm–Bonferroni correction assuming three different analyses. Means with the same superscript did not differ significantly.
Huynh–Feldt correction applied.
Trends in postural angles between measurements
Craniovertebral and head–neck–trunk angles measured in all the tasks increased from baseline to post-test and again to follow-up. Trunk, thoracic, thoracolumbar, and lumbar angles decreased, albeit to a lesser extent, from baseline to post-test and follow-up. As shown in Figure 2, participants exhibited similar postural angles between post-test and follow-up or reverted to baseline. For example, if they exhibited a larger angle at baseline, before they started taking AT lessons, the angle at follow-up was larger than at post-test but not as large as at baseline.
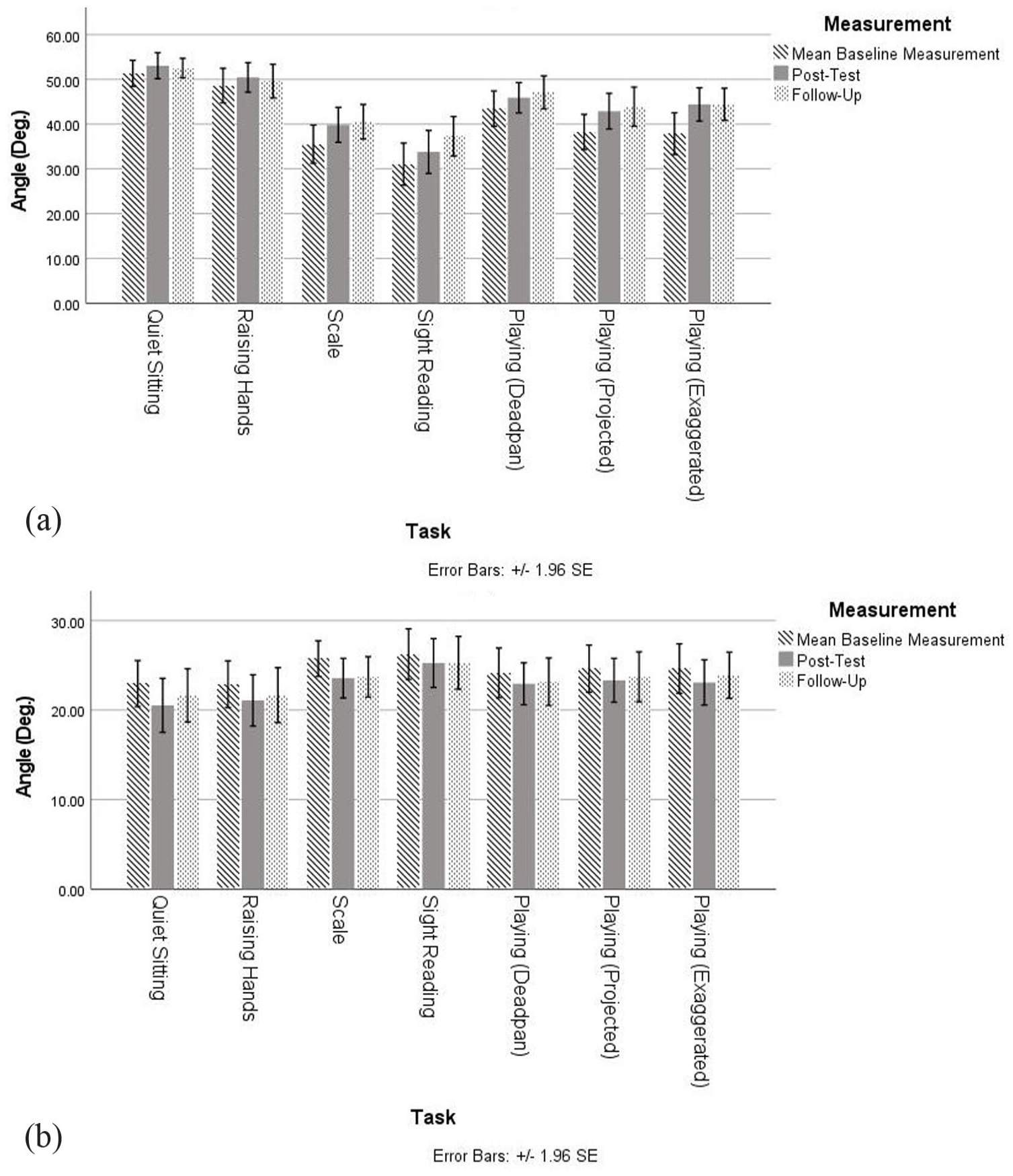
(a) Mean craniovertebral angle, pre- and post-intervention. (b) Mean thoracic angle, pre- and post-intervention.
Discussion
Musicians study the AT for various reasons, including the desire to change their postural behavior. In this study, we showed the effects of 10 AT lessons on pianists’ postural angles and the differences between them at baseline, post-test, and follow-up. The largest changes, measured in the largest number of tasks, were the craniovertebral, head–neck–trunk, and trunk angles. The AT principle of primary control focuses on the relationship between the head, neck, and back, illustrated in the motion-capture data. The changes in these angles suggest a pattern reflecting the AT notion of lengthening the spine. Participants appeared to be more kyphotic at baseline but demonstrated spinal extension at post-test and at follow-up. The results of the present study confirmed those of the authors’ exploratory research (Wong et al., 2022a) in which AT teachers and students performed a series of tasks either applying or not applying AT principles. The same postural angles were measured and the same differences were observed as in the present study, with the exception of the head-tilt measurements. This finding suggests that, over the course of the 10 AT lessons, participants in the present study integrated AT principles into their playing. Where there were significant effects of AT lessons on postural angles, there were usually differences between the angles at baseline and post-test, and/or baseline and follow-up, but fewer differences between the angles at post-test and follow-up. Even so, the effects of the AT were found not only as soon as the course of 10 lessons had ended, but also a month later. This implies that pianists would be able to change their playing posture if they were to continue practicing the AT even in the absence of lessons.
In Davies’ (2019, 2020) studies, musicians, including pianists and their teachers, agreed that the AT had helped them alter their playing posture, describing it as “more easy and upright” (Davies, 2019, p. 8). The AT’s idea of lengthening may account for this and may be explained by the post-intervention changes in angles found in the present study.
Limitations
The limitations of this study include the small size of the sample and its nature; the results may have been affected by expectation bias, as participants were volunteers, perhaps already interested in the AT and hoping that lessons would help them change their playing posture. Data were collected over a relatively short period of time; in future research it would be better to explore the long-term effects of AT lessons on posture by following participants up to a year, rather than a month, after the course of lessons has ended. Additionally, this study involved only pianists and further research is needed to confirm if these findings can be found in other musicians as well.
Conclusion
In the first study of its kind, a course of 10 AT lessons was shown to be effective in altering pianists’ postural angles from baseline to post-test and/or follow-up, demonstrating an overall pattern of spinal extension in line with the findings of Wong et al. (2022a) and the claims of the AT. There were significant increases in the craniovertebral, head-tilt, and head–neck–trunk angles and significant decreases in the trunk, thoracic, and thoracolumbar angles. The study validates the method of measuring postural angles and confirms the finding that the angles measured are appropriate for research on the AT. Finally, the measurements should be tested in the exploration of the potentially long-lasting effects of extended AT practice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.